
Abstract
Study Design
A systematic review and meta-analysis.
Objectives
To estimate reoperation rate after lumbar disc herniation surgery and identify associated risk factors.
Methods
We searched PubMed, Cochrane Central Register of Controlled Trials (CENTRAL), Web of Science, Scopus, and Embase to April 2025 for English-language randomized controlled trials and observational studies reporting risk factors and reoperation rates. Two reviewers independently screened studies, extracted data, and assessed quality using the Newcastle–Ottawa Scale and Cochrane Risk of Bias 2.0 tool. Meta-analysis used fixed-effect model.
Results
Twenty-five studies (1,031,348 patients) met the inclusion criteria. The pooled reoperation rate was 8.5% (95% CI: 6.2%-11.6%), rising with follow-up: 4% at ≤1 year, 11.1% at 1-5 years, and 8.8% beyond 5 years (P < 0.0001 for subgroup differences). Smoking (OR 1.39; 95% CI: 1.09-1.78), older age (OR 1.52; 95% CI: 1.25-1.85), and large annular defect size (OR 2.19; 95% CI: 1.07-4.48) were significant risk factors; sex was not (OR 1.22; 95% CI: 0.96-1.55). Diabetes and certain surgical techniques were also linked to higher risk in individual studies. Adjustment for publication bias increased the overall pooled rate to 10.3% (95% CI: 7.6%-14.0%).
Conclusions
Reoperation rates after lumbar disc herniation surgery differ by follow-up duration: 4% at ≤1 year, 11.1% at 1-5 years, and 8.8% beyond 5 years. Smoking, older age, diabetes, and large annular defects were significant risk factors. Recognizing high-risk patients can support decisions for extended conservative care or closer follow-up. Further studies should compare revision techniques to improve long-term outcomes.
Introduction
Lumbar disc herniation (LDH) is one of the most common spinal disorders worldwide and a leading cause of low back pain with or without radiculopathy, imposing a substantial personal and socioeconomic burden.1,2 It primarily affects adults aged 30-50 years, with higher incidence in males, and most often occurs at the L4-L5 and L5-S1 levels due to greater biomechanical stress. 2
Conservative management—including rest, physiotherapy, and pharmacological treatment—relieves symptoms in 85-90% of patients within 6-12 weeks.1-3 Surgery is indicated for cauda equina syndrome, progressive neurological deficits, or persistent pain despite conservative therapy. 2 Discectomy, whether open, microdiscectomy, or percutaneous endoscopic lumbar discectomy (PELD), generally provides faster symptom relief than non-operative care.3,4 with primary surgery success rates of 70-90%.3-5
Despite these outcomes, 5-11% of patients require revision surgery for recurrent LDH or other complications.5,6 Revision procedures are technically more challenging due to altered anatomy and scar tissue, with higher rates of dural tears and potentially less favorable results than primary surgery. 6 Identifying patients at higher risk for reoperation is essential to improve surgical decision-making, refine techniques, and optimize follow-up.
Studies have proposed multiple predictors of revision, including Modic changes, 7 diabetes with poor glycemic control,5,8 incomplete disc removal, 8 type of herniated disc material, degree of degeneration, facet joint arthropathy, and specific surgical techniques.3,5,7-9
However, existing evidence is limited by inconsistent definitions of rLDH, variable indications for revision, and heterogeneity in study designs. 6 The interplay between patient-related factors, comorbidities, lifestyle habits.4,6 Similarly, a more definitive understanding of how specific surgical techniques and intraoperative decisions influence the risk of revision is needed.1,8 The long-term impact of identified risk factors and the role of radiological parameters as predictors for the necessity of revision surgery.1,5 Although numerous studies and reviews have examined predictors of reoperation after lumbar disc herniation surgery, the evidence remains fragmented and inconsistent. Despite this, revision surgery rates remain substantial, and the risk factors are unclear. An updated and comprehensive synthesis is valuable for guiding daily surgical practice and improving patient outcomes.
While meta-analyses have addressed recurrence after specific procedures, 9 no comprehensive synthesis has examined risk factors for revision surgery across different primary surgical techniques. This systematic review and meta-analysis aim to estimate reoperation rates and identify health-related risk factors for revision after primary LDH surgery to help guide treatment planning and reduce the need for subsequent procedures.
Methods
The methodological approach and reporting of the results followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guidelines.10,11 The protocol was registered in the PROSPERO database (Registration number CRD420251035279).
Search Strategy and Study Selection
A comprehensive literature search was conducted using PubMed, Scopus, Cochrane Central Register of Clinical Trials, Web of Science, and Embase databases, to identify studies published up to April 2025. The search strategy employed the following combination: (Reoperation OR “Revision surgery” OR “Revision operation” OR “secondary surgery” OR “Repeat surgery” OR “surgical revision” OR “Second Look Surgery”) AND (“Risk factor*” OR risk OR Determinant* OR “Risk”) AND (“lumbar Degenerative Disc Disease” OR “DDD” OR “lumbar Disk Degeneration disorder” “lumbar intervertebral Disc Degeneration” OR “lumbar intervertebral Disk Degeneration” OR “Lumbar Disc Disease” OR “Lumbar Disk Disease” OR “Herniated Disc” OR “Disk Herniation” OR “Disk Protrusion” OR “Protruded Disc” OR “Disk Prolapse” OR “Prolapsed Disc” OR “Slipped Disc” OR “Slipped Disk” OR “Disk Displacement” OR “Disc Displacement”) (Supplemental Appendix 2).
To screen the studies from the databases, two authors independently assessed the titles, abstracts, and full texts using Rayyan software according to the selection criteria. In case of any disagreements, we resolved them through consensus and the primary investigator’s opinion. Duplications were removed by Rayyan. 12
Eligibility Criteria
Included studies were eligible if they enrolled participants aged 18 years or older with lumbar disc herniation (with or without lower limb symptoms) who underwent primary surgery, followed by revision at either the index or an adjacent segment. Studies were required to report not only reoperation rates but also potential risk factors associated with revision.
We included published English-language randomized controlled trials (RCTs) and observational studies. All other study types were excluded, as well as studies that lacked sufficient data on risk factors.
Data Extraction
Data extracted independently by at least two authors independently, with subsequent verification resolve differences. Extracted data included author name, year of publication, country of origin, study design, sample size, reoperation cause, reoperation method, follow up and risk factors for reoperation.
Quality Assessment
The Newcastle–Ottawa Scale (NOS) was employed to assess study quality of included observational studies. 13 The NOS awards stars across three domains: Selection, Comparability, and Outcome. Each subcategory within these domains can receive up to one star, except Comparability, which allows a maximum of two stars. The total score ranges from 0 to 9, with higher scores indicating lower risk of bias. The NOS scores were categorized into AHRQ quality categories: Good (7-9 stars), Fair (5-6 stars), and Poor (0-4 stars). 14
The Cochrane Risk of Bias tool version 2.0 was used to assess RCTs. This tool evaluates five specific domains: (1) bias arising from the randomization process; (2) bias due to deviations from intended interventions; (3) bias due to missing outcome data; (4) bias in outcome measurement; and (5) bias in the selection of reported results. Each review author applied the tool to each included study and recorded supporting information and justifications for their risk of bias judgments (low, high, or some concerns). Two reviewers independently assessed each study, with discrepancies resolved through discussion.
Data Synthesis and Statistical Analysis
A pairwise meta-analysis was performed for the eligible studies. For dichotomous outcomes, odds ratios (ORs) were used as the effect measure, with 95% confidence intervals (CIs) pooled using a fixed-effects model. Reoperation rates were synthesized separately using rate as the effect measure and analyzed under a random-effects model. The level of statistical significance for the overall effect was set at P < 0.05.15,16 Heterogeneity was assessed using the I2 statistic and classified as not important (<40%), moderate (40-60%), substantial (60-75%), or considerable (75-100%). 17 If heterogeneity was not important, a fixed-effects model was used. To ensure the robustness of our findings, Sensitivity analyses were conducted by omitting individual studies with high weights if available or by model of meta-analysis if heterogeneity greater than 40%. 18 For meta-analyses comprising ten or more studies, publication bias was assessed and addressed using the trim-and-fill method. 19
Eligible studies comparing reoperation vs no reoperation based on health risk factors were included in the quantitative synthesis. Studies without an odds ratio or sufficient data to calculate one were excluded from the meta-analysis. The reoperation rate was determined based on data from the last available follow-up in each study and was subgrouped by follow-up period: Short-term: ≤1 year Mid-term: >1 to ≤5 years Long-term: >5 years.
Meta-analysis related to health risk factors were conducted using RevMan Web 9.6.0,16,20 while analysis of reoperation rates were performed using R statistical software (version 4.5.0). 20
Studies that did not meet the eligibility criteria for quantitative synthesis were included in a narrative synthesis, which served to complement the meta-analytic findings.
Results
Study Selection
Our systematic search identified 711 potential studies from various databases; among these, 176 were excluded as duplicates. A screening of titles and abstracts of the remaining 535 records led to the exclusion of 482 records, and 3 records not retrieved, leaving 50 for full-text review. Upon full-text assessment, 25 records were excluded due to reasons such as non-English language articles, irrelevant population, irrelevant study design, no reoperation and inadequate.21-45 Ultimately, 25 studies were included for quantitative and qualitative analysis. Figure 1 illustrates the Prisma flow diagram. PRISMA Flow Diagram 2020. *Consider, If Feasible to Do So, Reporting the Number of Records Identified From Each Database or Register Searched (Rather Than the Total Number Across All Databases/Registers). **If Automation Tools Were Used, Indicate How Many Records Were Excluded by a Human and How Many Were Excluded by Automation Tools. Source: Page MJ, et al. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. This Work is Licensed Under CC BY 4.0. To View a Copy of This License, Visit https://creativecommons.org/licenses/by/4.0/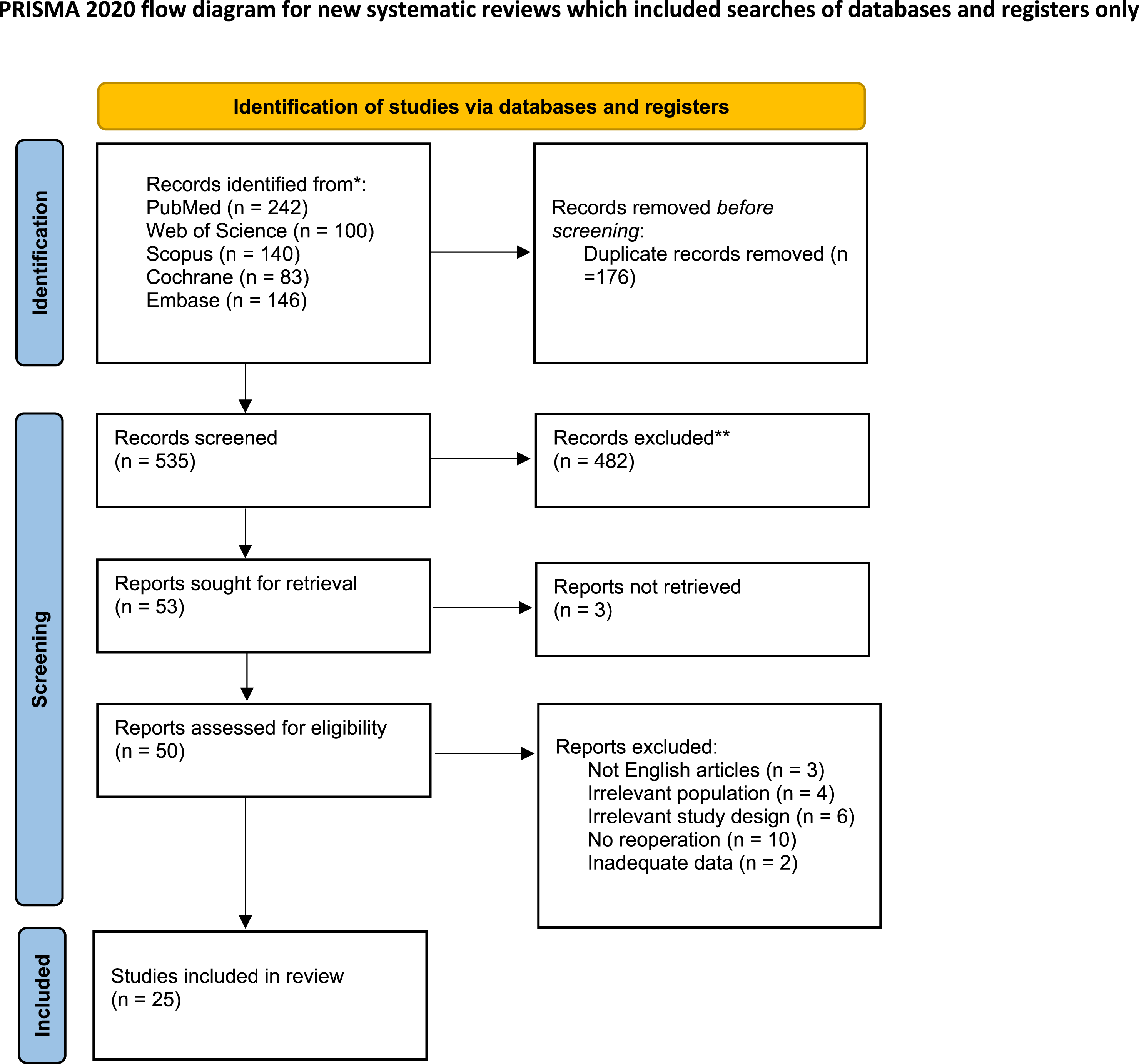
Characteristics of Included Studies
This review included 25 studies published between 2000 and 2025, encompassing 1,031,348 participants. No date restrictions were applied in the search strategy.46-70 These studies were primarily retrospective cohort studies, with some prospective cohorts and three randomized controlled trials. The studies originated from various countries, including the USA,47-49,51,56,65,68,69 Japan,46,63 Taiwan,52,53,70 Finland,57,60 Turkey,50,62 the United Kingdom,55,66 China, 58 South Korea, 59 and two multinational.61,64
The total number of patients across these studies varied significantly. For example, Kang et al. (2021) analyzed a large cohort of 549,531 patients undergoing single-level lumbar discectomy. Other studies had sample sizes ranging from 75 (Meredith et al., 2010) to 308,979 (Etigunta et al., 2025).
The types of primary surgery performed included lumbar discectomy (microscopic, open, or unspecified), percutaneous endoscopic lumbar discectomy (PELD/FELD). The causes for reoperation were diverse, commonly including recurrent disc herniation at the same or different level, contralateral herniation, and persistent symptoms. Reoperation methods also varied, encompassing revision discectomy, laminectomy, and fusion.
The mean interval between index surgery and reoperation ranged from as short as 0.11 years to as long as 8.51 years, with several studies did not reporting the exact duration. Reherniation occurred at the same level in most studies, although some reported involvement of both same and different levels.
Follow-up durations varied from 6 months to up to 20 years, providing a broad range of temporal data for assessing recurrence and reoperation rates.
Summary of Characteristics of Included Studies
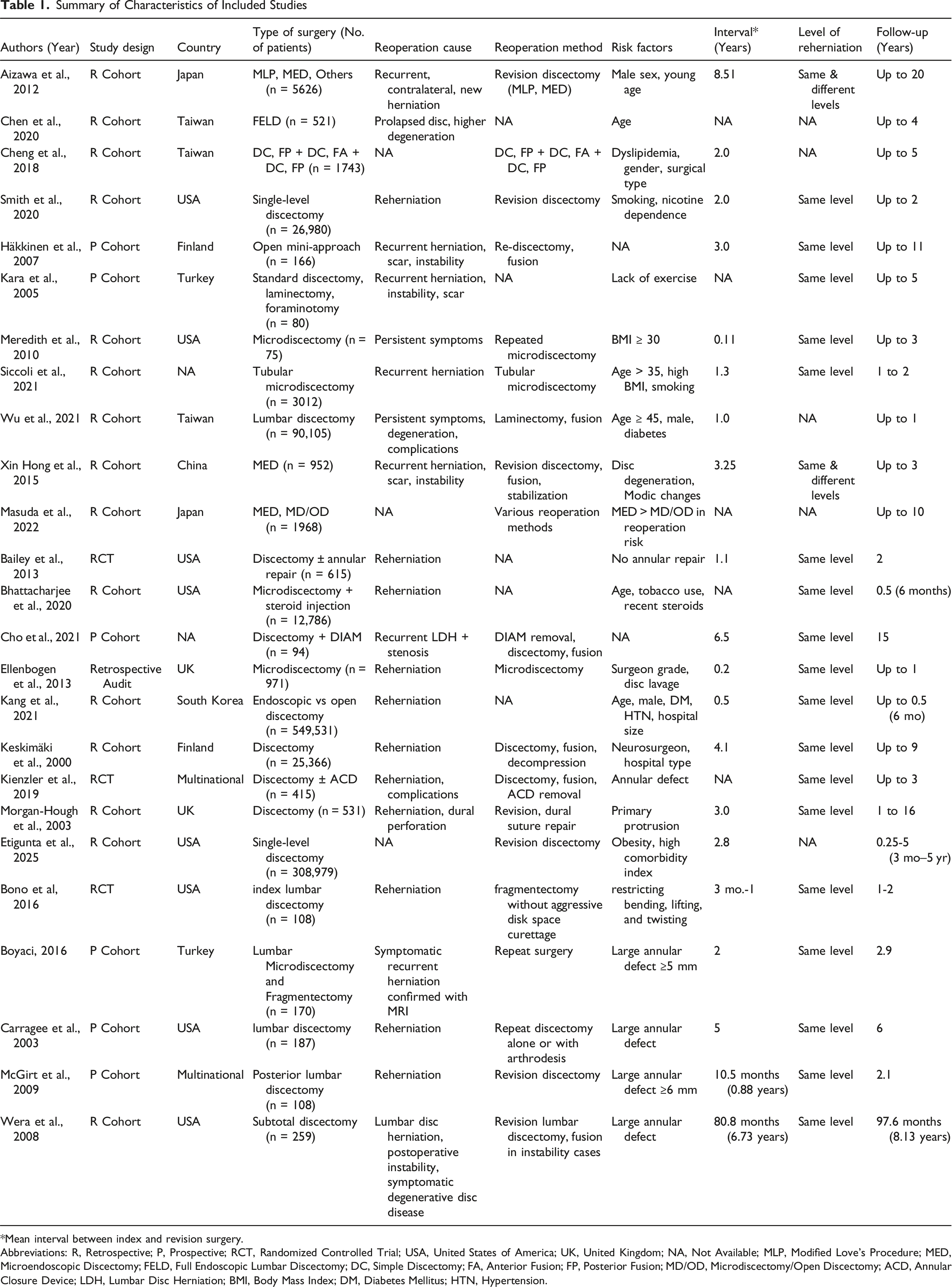
*Mean interval between index and revision surgery.
Abbreviations: R, Retrospective; P, Prospective; RCT, Randomized Controlled Trial; USA, United States of America; UK, United Kingdom; NA, Not Available; MLP, Modified Love’s Procedure; MED, Microendoscopic Discectomy; FELD, Full Endoscopic Lumbar Discectomy; DC, Simple Discectomy; FA, Anterior Fusion; FP, Posterior Fusion; MD/OD, Microdiscectomy/Open Discectomy; ACD, Annular Closure Device; LDH, Lumbar Disc Herniation; BMI, Body Mass Index; DM, Diabetes Mellitus; HTN, Hypertension.
Quality Assessment and Risk of Bias
The methodological quality of the included studies was assessed using the Newcastle-Ottawa Scale (NOS) and the AHRQ criteria. Out of the 22 observational study studies included in the systematic review, the majority (18 studies) were rated as “good” quality, receiving scores of 7 to 9 stars.46,50-53,64,67,69,71,72 and others—fulfilled most or all domains of selection, comparability, and outcome assessment.
Results of Quality Assessment for Cohort Studies
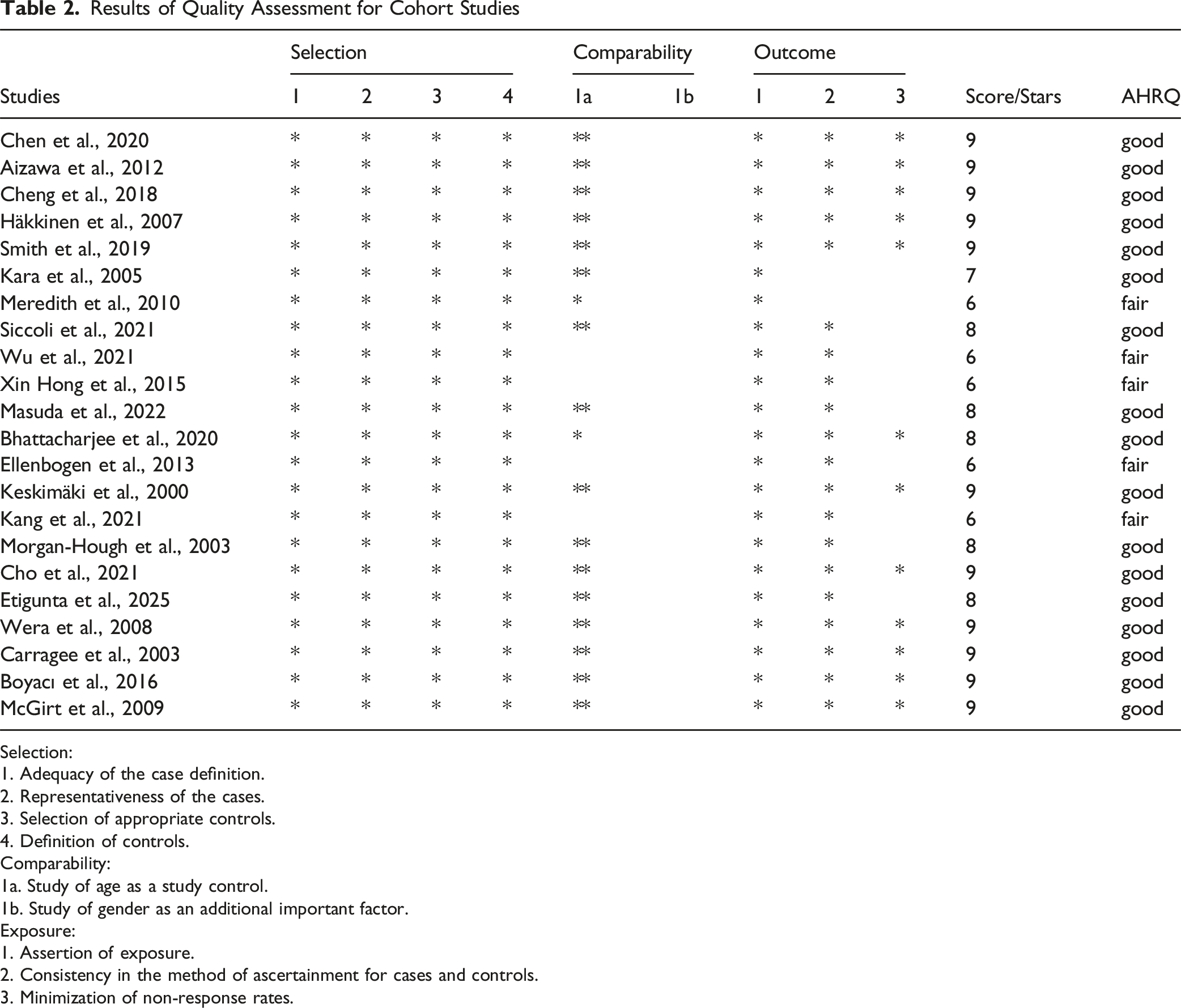
Selection:
1. Adequacy of the case definition.
2. Representativeness of the cases.
3. Selection of appropriate controls.
4. Definition of controls.
Comparability:
1a. Study of age as a study control.
1b. Study of gender as an additional important factor.
Exposure:
1. Assertion of exposure.
2. Consistency in the method of ascertainment for cases and controls.
3. Minimization of non-response rates.
Risk of Bias Assessment
Using the Cochrane Risk of Bias (RoB) 2.0 tool, which evaluates five key domains, the risk of bias was assessed for the three randomized controlled trials (RCTs) included in this review.47,49,61 Two were classified as having some concerns,47,61 and one as a high risk of bias.
49
See Figure 2. Risk of Bias Assessment of Included Studies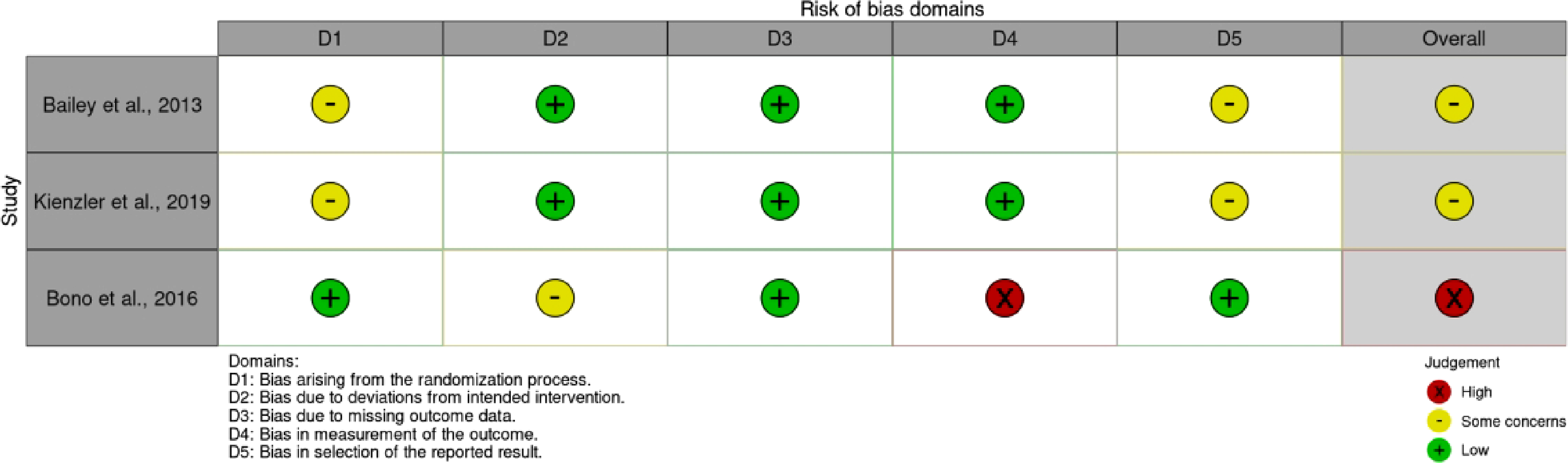
Outcomes
The following sections detail the meta-analysis findings for specific risk factors identified.
Smoking
The association between smoking and the risk of revision surgery was assessed using data from three studies,48,58,65 as demonstrated in the forest plot (Figure 3A). The pooled analysis, using a fixed-effects model, yielded an Odds Ratio (OR) of 1.39 (95% Confidence Interval [CI] 1.09 - 1.78). There was no evidence of heterogeneity between the studies (I2 = 0%; Chi
2
= 1.03, df = 2, P = 0.60). The test for overall effect was statistically significant (Z = 2.64, P = 0.008), suggesting that there is an increased risk of reoperation with smoking. Sensitivity analysis revealed removing the study with the largest weight (Bhattarajee et al., 2020) would alter the results, as this study contributes 89.9% of the weight to the pooled estimate (P = 0.94). (A) Forest Plot for the Association Between Smoking and the Odds of Revision Surgery (B) Forest Plot for the Association Between Sex and the Odds of Revision Surgery (C) Forest Plot for the Association Between Age and the Odds of Revision Surgery (D) Forest Plot for the Association Between Annular Defect Size and the Odds of Revision Surgery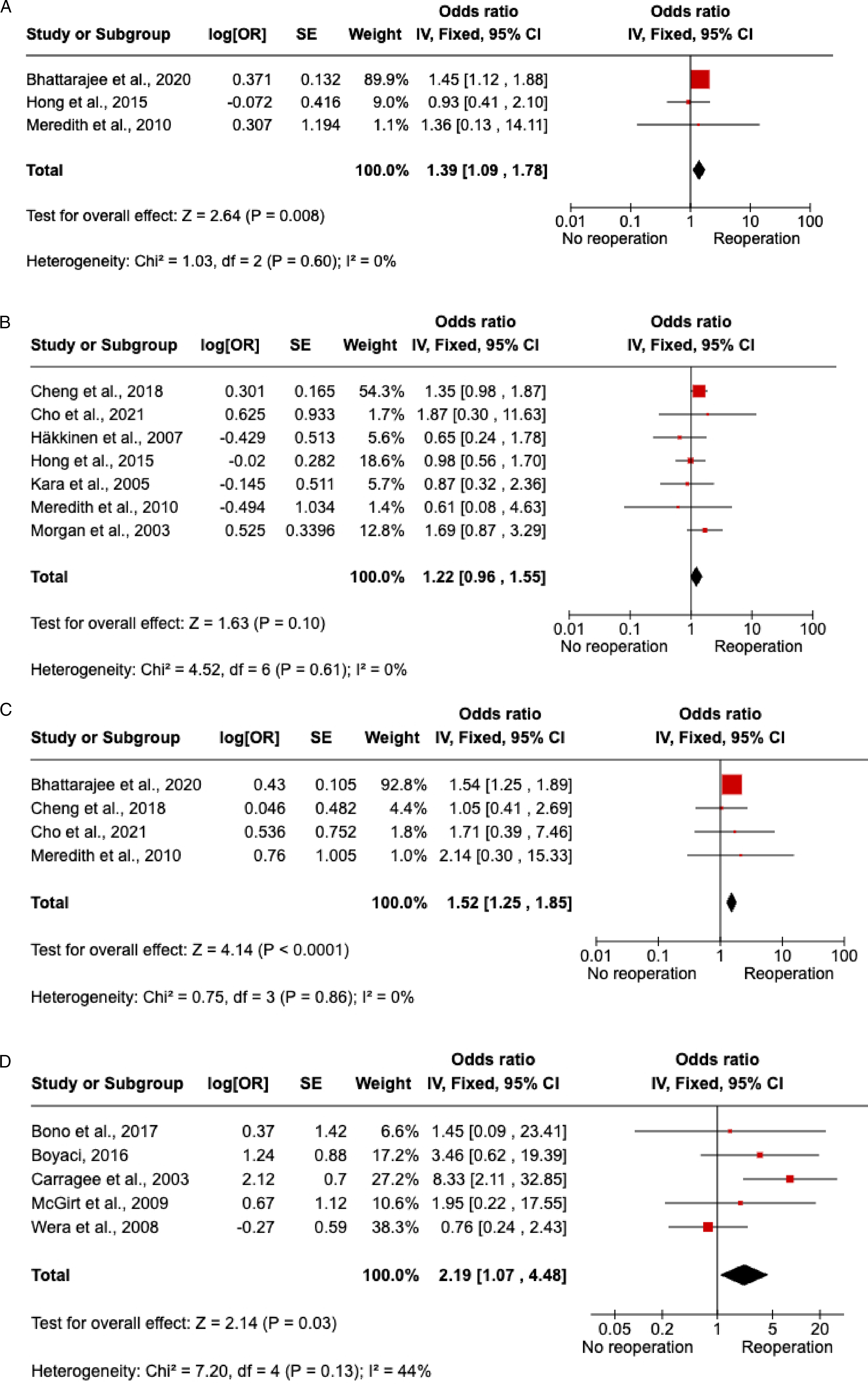
Sex
Seven studies53,54,58,62,65,66,71 provided data for the meta-analysis on sex as a risk factor for revision surgery (Figure 3B). The pooled OR, calculated using a fixed-effects model, was 1.22 (95% CI 0.96 - 1.55). There was no important heterogeneity observed (I2 = 0%; Chi 2 = 4.52, df = 6, P = 0.61). The overall effect did not reach statistical significance (Z = 1.63, P = 0.10), indicating that sex was not identified as a significant predictor of revision surgery in this meta-analysis. Sensitivity analysis revealed a non-significant difference after removing the study with the largest weight (Cheng et al., 2018).
Age
Data from four studies48,52,54,65 were pooled to assess age as a risk factor (Figure 3C). The fixed-effects meta-analysis showed a pooled OR of 1.52 (95% CI 1.25 - 1.85). There was no heterogeneity among the studies (I2 = 0%; Chi2 = 0.75, df = 3, P = 0.86). The test for overall effect was statistically significant (Z = 4.14, P < 0.0001), suggesting that age is a significant risk factor for revision surgery, with increasing age associated with higher odds of reoperation. Sensitivity analysis revealed removing the study with the largest weight (Bhattarajee et al., 2020) would alter the results, as this study contributes 89.9% of the weight to the pooled estimate (P = 0.48) (Figure 3C).
Annular Defect Size
Data from five studies49-51,64,69 were pooled to assess annular defect size as a risk factor for reoperation. The fixed-effects meta-analysis showed a pooled odds ratio (OR) of 2.19 (95% CI, 1.07-4.48). The test for overall effect was statistically significant (Z = 2.14, P = 0.03), suggesting that annular defect size is a significant risk factor for reoperation, with an increase in defect size associated with higher odds of reoperation. Sensitivity analysis revealed non-significant results (P = 0.14) based on a random effect model (Figure 3D).
Reoperation Rate
Overall Results Reoperation Rate
This meta-analysis showed a pooled reoperation rate for all included studies was 8.5% (95% CI: 6.2%-11.6%), estimated using a random-effects model. The heterogeneity across studies was substantial and highly significant (I2 = 99%, P < 0.0001), indicating that the observed variability was not due to chance alone.
Subgroup Analysis by Follow-up Duration
To investigate potential sources of this high heterogeneity, a pre-specified subgroup analysis was performed based on the duration of follow-up: Short-term follow-up (≤ 1 year): Eight studies contributed to this subgroup. The pooled reoperation rate was 4% (95% CI: 2.8%-5.5%). Substantial heterogeneity was also evident within this subgroup (I2 = 99.6%, P < 0.0001). Mid-term follow-up (1 to 5 years): Ten studies provided data for this subgroup. The pooled reoperation rate was 11.1% (95% CI: 6.4%-18.5%), with significant heterogeneity observed (I2 = 99.6%, P < 0.0001). Long-term follow-up (> 5 years): Seven studies were included in this subgroup. The pooled reoperation rate was 8.8% (95% CI: 6.5%-13.2%), again with considerable heterogeneity (I2 = 99.2%, P < 0.0001).
The test for subgroup differences was statistically significant (Chi2 = 23.23, df = 2, P < 0.0001), confirming that the reoperation rates differ significantly across the follow-up periods.
Adjustment for Publication Bias Using the Trim and Fill Method
Visual inspection of the funnel plot (Figure 4C) suggested asymmetry, indicating a potential for publication bias. The trim and fill method was utilized to adjust for this bias. After adjustment, the overall pooled reoperation rate was estimated to be 10.3% (95% CI: 7.6%-14.0%) (Figure 4B). This adjusted estimate continued to exhibit substantial heterogeneity (I2 = 99.5%, P < 0.0001). The prediction interval for the reoperation rate, which accounts for both sampling error and between-study heterogeneity, was notably broad, ranging from 0.8% to 42.7%. (A) Forest Plot of Pooled Reoperation Rates by Follow-up Duration (Before Adjustment) (B) Forest Plot of Pooled Reoperation Rate (After Adjustment) (C) Funnel Plot for Assessment of Publication Bias (After Adjustment)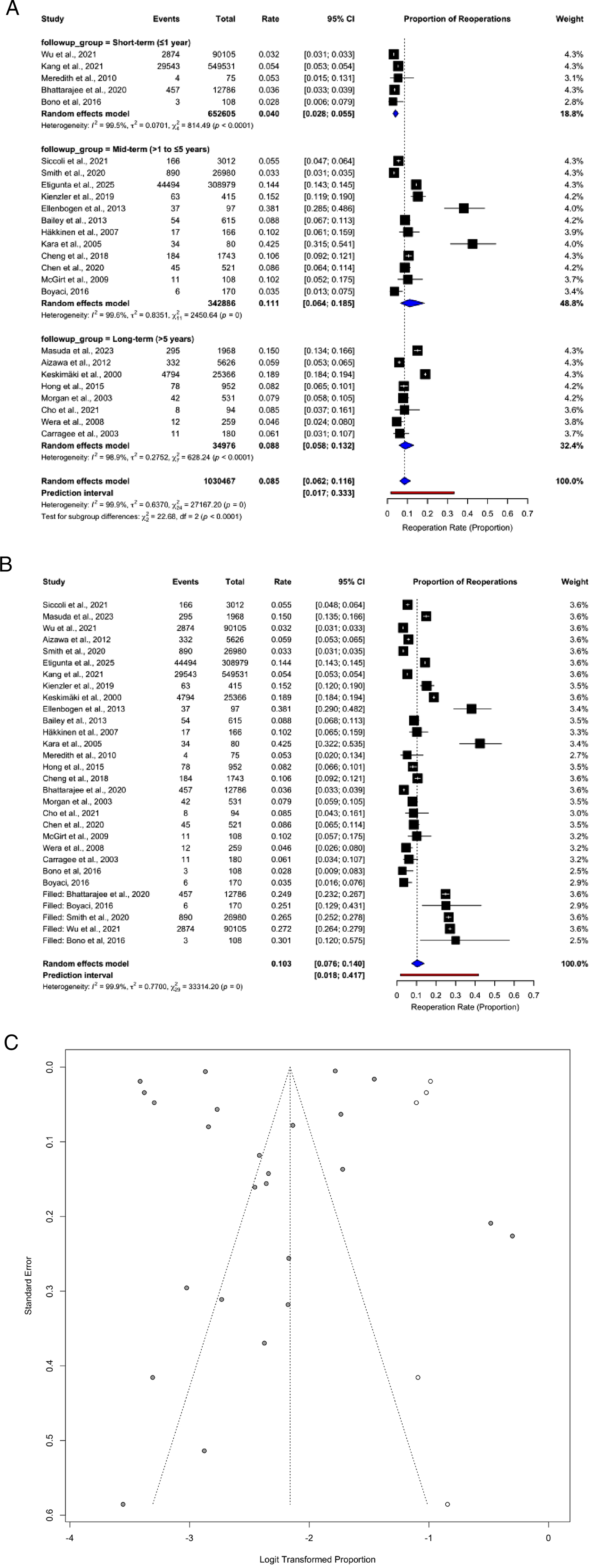
Narrative Synthesis
In addition to the pooled analyses, several other risk factors were inconsistently reported across studies, precluding meta-analysis. Diabetes mellitus, adjacent segment degeneration, and Pfirrmann disc degeneration grading were reported as potential contributors to reoperation risk.58,70 Certain socioeconomic and hospital-related factors (treatment in smaller hospitals, university vs regional centers, or by surgeon grade) were also linked to higher reoperation rates.59,60 Surgical factors such as prior steroid injections, use of annular closure devices, and disc morphology (protrusion vs extrusion/sequestration) showed associations with recurrence in single studies. Regarding the type of reoperation, revision discectomy was more frequently reported than fusion procedures; however, few studies provided sufficient detail to allow pooled analysis. Similarly, studies with longer follow-up durations reported a progressive increase in cumulative reoperation rates, with indications that later reoperations more often involved fusion procedures or adjacent-level disease, whereas earlier reoperations tended to involve revision discectomy at the index level. Detailed descriptive findings are presented in Supplemental Appendix 1.
Discussion
This systematic review, including 25 studies with a total of 1,031,348 patients, found an overall reoperation rate after LDH surgery of 8.5%, with 4% occurring within the first year, 11.1% within five years, and 8.8% after more than five years. Risk was higher in older patients, smokers, and those with diabetes, larger annular defects, or adjacent vertebral degeneration. Other factors—such as type of surgery, kidney disease, peripheral neuropathy, and hypertension—may also contribute to increased reoperation rates.
Animal studies have shown that the annulus fibrosus has a limited intrinsic healing capacity.73,74 Larger annular defects after surgery are therefore associated with higher reoperation rates compared with smaller defects. 75 Aging further reduces healing potential through loss of collagen and proteoglycans, diminished blood supply, and reduced regenerative capacity.76,77 Smoking compounds these effects by causing vasoconstriction around the annulus fibrosus, 78 increasing infection risk, and accelerating degeneration. 79 Comorbidities such as diabetes, hypertension, peripheral neuropathy, and kidney disease may similarly impair healing, elevate risk of infection, and raise the likelihood of reoperation.80-82
Most reoperations occur at the same spinal level as the primary surgery,with higher rates observed when the adjacent vertebrae are degenerated. Fusion and discectomy are the most common revision procedures. While two systematic reviews reported comparable functional outcomes for fusion and discectomy,83,84 more recent evidence suggests that fusion may yield better functional outcomes and reduce re-recurrence rates for recurrent LDH. 85 Our analysis demonstrates that reoperation rates increase with longer follow-up, which is in line with previous observations. Early reoperations, usually within the first two years, were predominantly revision discectomies at the same level.43,68,86 These procedures generally address recurrent herniation or persistent symptoms shortly after the index surgery. 41
In contrast, later reoperations more frequently involved fusion procedures or surgeries addressing adjacent segment disease. For instance, Häkkinen et al. (2007), Keskimäki et al. (2000) and s Ambrossi et al. (2009) reported fusion as a common reoperation method during extended follow-up up to 9-11 years.57,60,87 Similarly, Hong et al. (2015) found that advanced disc degeneration and instability contributed to the need for stabilization procedures in longer-term cohorts. 58 These findings support the concept that while early recurrences are technical or biological failures at the operated level, long-term failures often reflect the natural progression of spinal degeneration. 88
Moreover, the site of reoperation appears to shift over time. Aizawa et al. (2012) observed that reherniations occurred both at the same and different levels during 20 years of follow-up, with same-level recurrences predominating in the early years and adjacent-level disease contributing increasingly with time. 46 This temporal pattern suggests that different mechanisms drive early and late failures: recurrent herniation vs progressive segmental degeneration.
Together, these findings explain why reoperation risk rises with follow-up duration. Revision discectomy remains the most common early reoperation, whereas fusion procedures and adjacent-level surgeries account for a growing proportion of late reoperations.
Our findings also parallel those from studies on other lumbar spine conditions. For instance, the reoperation rate after surgery for degenerative lumbar spondylolisthesis is approximately 10%, with smoking, obesity, and diabetes identified as major risk factors. 89 Similarly, decompression-only surgery has a reported reoperation rate of 6.9% at one year, increasing to 11.9% at five years. 90
This study has several strengths, including a comprehensive search strategy, the inclusion of a large patient population, and evaluation of diverse patient, surgery, and anatomically related risk factors. Potential sources of bias, heterogeneity, and sensitivity were thoroughly assessed. However, limitations must be acknowledged. Sensitivity analysis revealed no statistically significant association between reoperation rate and either age, smoking, or annular defect; nevertheless, integration of the qualitative synthesis with meta-analytic data supports a likely link. Additionally, several risk factors—such as annular defect size, patients’ comorbidities, and hospital type—were only qualitatively assessed, underscoring the need for further high-quality studies. Finally, future primary studies should stratify reoperation rates by location (index vs adjacent level) across short-, mid-, and long-term follow-up to better clarify temporal and anatomical patterns of failure.
In summary, reoperation after LDH surgery remains an important clinical concern, with identifiable modifiable and non-modifiable risk factors. These findings should inform surgical decision-making, patient counseling, and the design of future studies aimed at reducing reoperation rates and optimizing procedure selection.
Conclusion
The reoperation rate after LDH surgery increases gradually with longer follow-up, up to 5 years after which it reduces. The overall rate is approximately 8.5%, with higher rates observed in patients with diabetes, older age, smoking history, and larger annular defects. Identifying high-risk patients may guide decisions toward extended conservative management or tailored postoperative follow-up. Fusion and discectomy are the most common revision procedures; however, further research is needed to determine which surgery yields superior outcomes and to identify which patient subgroups benefit most from each procedure.
Supplemental Material
Supplemental Material - Risk Factors and Reoperation Rate in Revision Lumbar Disc Herniation Surgery: A Systematic Review and Meta-Analysis of 1,031,348 Patients
Supplemental Material for Risk Factors and Reoperation Rate in Revision Lumbar Disc Herniation Surgery: A Systematic Review and Meta-Analysis of 1,031,348 Patients by Ahmed Samir, Ahmed Ashraf, Esraa Mohamed Mosaid, Islam Saeed Elhois, Ahmed Abdullah, Farah Ahmed Elzanaty, Ahmed Oun, Ahmed Wael Moftah, Magdy Elsisi and Mohamed Gomaa Sobeeh in Global Spine Journal
Supplemental Material
Supplemental Material - Risk Factors and Reoperation Rate in Revision Lumbar Disc Herniation Surgery: A Systematic Review and Meta-Analysis of 1,031,348 Patients
Supplemental Material for Risk Factors and Reoperation Rate in Revision Lumbar Disc Herniation Surgery: A Systematic Review and Meta-Analysis of 1,031,348 Patients by Ahmed Samir, Ahmed Ashraf, Esraa Mohamed Mosaid, Islam Saeed Elhois, Ahmed Abdullah, Farah Ahmed Elzanaty, Ahmed Oun, Ahmed Wael Moftah, Magdy Elsisi and Mohamed Gomaa Sobeeh in Global Spine Journal
Supplemental Material
Supplemental Material - Risk Factors and Reoperation Rate in Revision Lumbar Disc Herniation Surgery: A Systematic Review and Meta-Analysis of 1,031,348 Patients
Supplemental Material for Risk Factors and Reoperation Rate in Revision Lumbar Disc Herniation Surgery: A Systematic Review and Meta-Analysis of 1,031,348 Patients by Ahmed Samir, Ahmed Ashraf, Esraa Mohamed Mosaid, Islam Saeed Elhois, Ahmed Abdullah, Farah Ahmed Elzanaty, Ahmed Oun, Ahmed Wael Moftah, Magdy Elsisi and Mohamed Gomaa Sobeeh in Global Spine Journal
Footnotes
Author Contributions
Idea conception: Ahmed Samir.
Systematic search: Ahmed Samir, Ahmed Oun.
Title and abstract filtration: Islam Saeed Elhois, Esraa Mohamed Mosaid, Farah Ahmed Elzanaty, Ahmed Ashraf, Ahmed Wael Moftah.
Full-text filtration: Islam Saeed Elhois, Esraa Mohamed Mosaid, Farah Ahmed Elzanaty, Ahmed Ashraf, Ahmed Wael Moftah.
Data extraction: Ahmed Wael Moftah, Ahmed Abdullah, Esraa Mohamed Mosaid, Farah Ahmed, Magdy Elsisi.
Risk of bias assessment: Ahmed Ashraf, Islam Saeed Elhois, Magdy Elsisi.
Meta-analysis: Ahmed Samir, Ahmed Oun.
Manuscript writing: All authors.
Revision and proofreading: Ahmed Samir, Mohamed Gomaa Sobeeh, Esraa Mohamed Mosaid.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No datasets were generated or analyzed during the current study.
PROSPERO Registration Number
(CRD420251035279).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.