
Abstract
Study Design
A systematic review and meta-analysis comparing the outcomes of Anterior Cervical Discectomy and Fusion (ACDF) vs Anterior Cervical Corpectomy and Fusion (ACCF) in treating adjacent two-segment cervical spondylotic myelopathy.
Objective
To assess the clinical effectiveness and safety of ACDF compared to ACCF.
Methods
A literature search was conducted in Cochrane Library, Web of Science, PubMed, and Embase up to December 2023. Studies included were prospective and observational involving ACDF or ACCF for adjacent two-segment cervical spondylotic myelopathy. Data were analyzed using RevMan 5.4 software.
Results
Ten studies (nine case-control and one RCT) were included. ACDF showed a shorter hospital stay (SMD = −0.29, 95% CI: −0.53 to −0.04, P < 0.05), better Cobb angle (SMD = 0.52, 95% CI: 0.31 to 0.74, P < 0.01), and improved T1S (SMD = 0.54, 95% CI: 0.28 to 0.80, P < 0.01). No significant differences were found in upper limb VAS, neck VAS, JOA scores, NDI, fusion rates, C2-7 SVA, total complications, blood loss, and operation time.
Conclusions
ACDF and ACCF are both effective for adjacent two-segment cervical spondylotic myelopathy, with ACDF offering advantages in hospitalization duration and cervical curvature restoration, making it the preferred surgical approach. Further research is needed to validate these findings.
Introduction
Cervical Spondylotic Myelopathy (CSM), also known as Degenerative Cervical Myelopathy (DCM), is a condition resulting from degenerative changes in cervical discs, leading to compression of the spinal cord. 1 About 10% of individuals aged 55 and above have clinical CSM, with 50% showing cervical spondylosis on MRI. As age increases, so does the prevalence and severity of disc protrusions, exacerbating spinal cord compression.2,3
Adjacent Two-segment Cervical Spondylotic Myelopathy is the most common subtype, accounting for 56% of cases. 4 Its gradual onset and progression can cause irreversible cervical cord damage, potentially leading to limb paralysis and impacting daily life significantly. 5 Current treatments for CSM include conservative symptomatic management and surgical intervention. 6 Surgical intervention is recommended if conservative measures fail to show improvement within 3 months to prevent further deterioration and enhance neurological function. 7 Surgical approaches include anterior, posterior, or combined anterior and posterior decompression procedures. 6 Generally, anterior surgeries, such as Anterior Cervical Discectomy and Fusion (ACDF) and Anterior Cervical Corpectomy and Fusion (ACCF), have shown favorable clinical outcomes. 8
However, the superiority between ACDF and ACCF remains controversial. Previous studies suggest that ACDF may reduce surgical time, decrease blood loss, and lower complication rates, but it comes with a higher non-union rate due to a larger graft-host interface.8,9 On the other hand, ACCF demonstrates better complete decompression with a lower risk of pseudoarthrosis, 10 but it is a more complex and challenging procedure, associated with higher rates of complications such as spinal cord or nerve root injury, excessive bleeding, and graft displacement or compression. 9
To guide surgeons in choosing the best approach and improve patient outcomes, we conducted a systematic review and meta-analysis comparing ACDF and ACCF procedures.
Materials and Methods
This review follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and AMSTAR guidelines.11-14 This study was registered in the international prospective register of systematic reviews (Prospero).
Ethics and Dissemination
In conducting this meta-analysis, no IRB/ethics committee approval was sought as it does not involve direct interaction with human subjects or the collection of primary data. Furthermore, patient consent to procedure was not applicable as this study solely relies on published data from previously conducted research. As such, ethical considerations regarding patient consent and IRB approval are not relevant to this meta-analysis.
Inclusion and Exclusion Criteria
Inclusion criteria: ① Patients with adjacent two-segment myelopathic cervical spondylosis meeting clinical diagnostic criteria; ②Study types: Prospective and observational studies; ③Interventions: ACDF and ACCF; ④ Outcome measures: Upper Limb Visual Analog Scale (VAS), Neck VAS, Hospital Time, Neck Disability Index (NDI), Japanese Orthopaedic Association (JOA), Cobb Angle, Thoracic Vertebra 1 Slope (T1S), Fusion Rate, Cervical Vertebra 2-7 Sagittal Vertical Axis (C2-7 SVA), Total Complications, Blood Loss, Operation Time.
Exclusion criteria: ① Non-English literature; ② Duplicate publications; ③ Inability to obtain the full text or full text containing only abstract; ④ Articles with incomplete data.
Search Strategy
The computer-based search will be conducted inin the Cochrane Library, Web of Science, PubMed, and Embase databases. The search period extended from the inception of the databases to December 2023. Additionally, references of included studies were supplemented by conducting manual searches. The search strategy involved a combination of subject terms and free-text terms. Supplemental Document 1 provides the complete search strategy.
Data Collection and Analysis
Two researchers independently conducted literature screening and data extraction based on the inclusion and exclusion criteria, with cross-verification. In case of discrepancies, a third researcher was involved for collaborative decision-making. After screening titles and abstracts, studies that potentially met the criteria underwent further assessment of full-text content. The extraction process included the following information: researchers, publication date, patient age, gender, sample size, study type, follow-up duration, and outcome indicators.
Assessment of Risk of Bias
Divergences were resolved through consensus, with a third author consulted if needed. Risk of bias assessment utilized the Newcastle-Ottawa Scale for cohort and case-control studies, and the Cochrane Handbook version 5.1.0 for Randomized Controlled Trials (RCTs).15,16 The Newcastle-Ottawa Scale evaluated study selection, comparability, and outcome/exposure assessment, with a total score ranging from 0 to 9 points. For RCTs, bias risk was categorized as low, unclear, or high across seven criteria, determining the study’s quality level as Grade A, B, or C accordingly.
Statistical Analysis
A meta-analysis using RevMan 5.4 software analyzed both continuous and dichotomous outcomes. Relative risk (RR) and standardized mean difference (SMD) with a 95% confidence interval (CI) were used. Heterogeneity was assessed with the χ2 test and I2 statistic. Low heterogeneity (P > 0.1 and I2 < 50%) justified a fixed-effects model; otherwise, a random-effects model was used. Subgroup and sensitivity analyses were conducted to explore heterogeneity sources. A significance level of P ≤ 0.05 indicated statistical significance.
Results
Study Selection
A preliminary search of the database yielded a total of 667 relevant articles. After removing duplicates using Endnote 20 software and reviewing titles and abstracts, 25 articles were selected for full-text review. Ultimately, 10 articles were included in the final analysis. The literature screening process is depicted in Figure 1. Screening flowchart.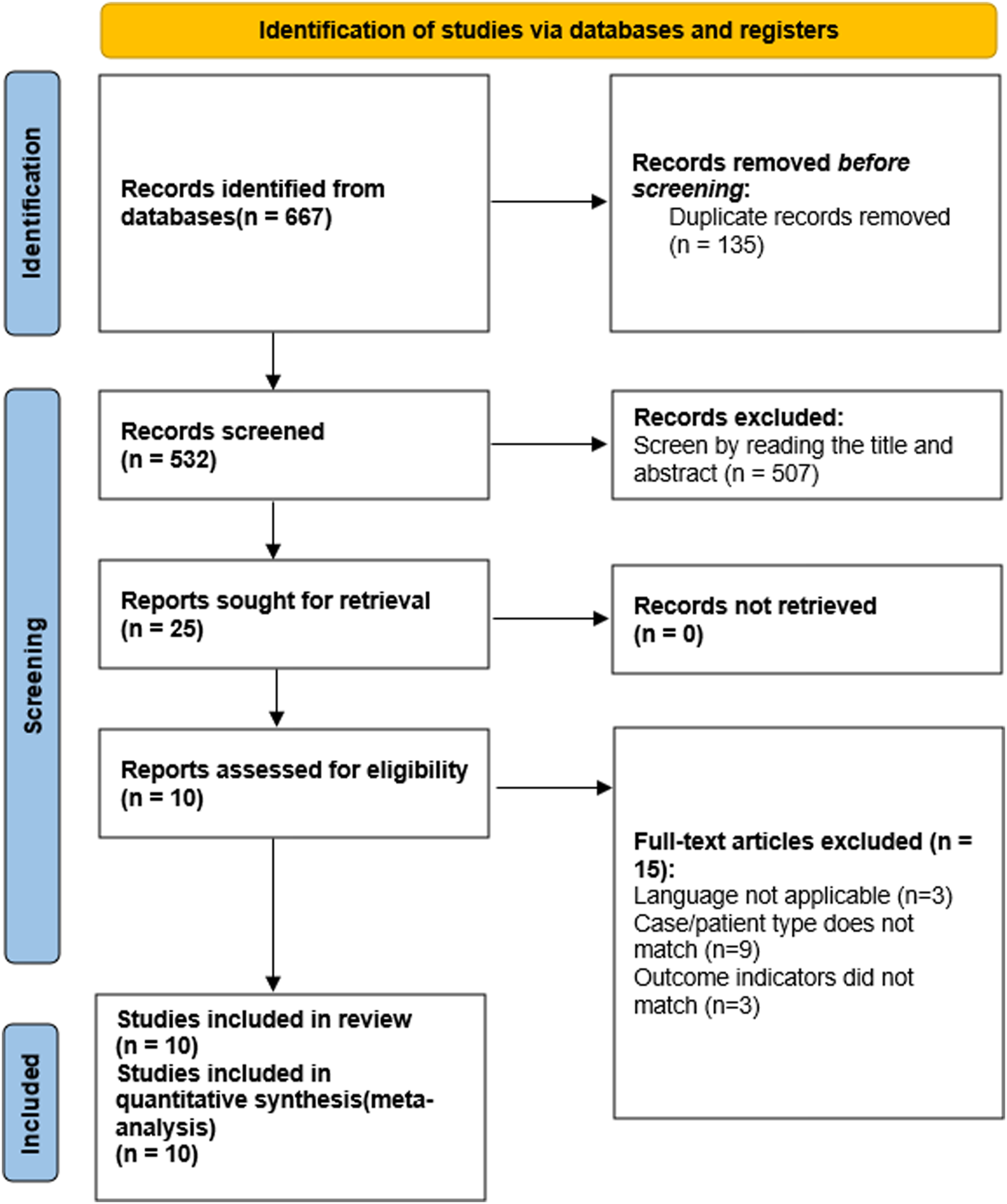
Study Characteristics
Characteristics of Included Studies.
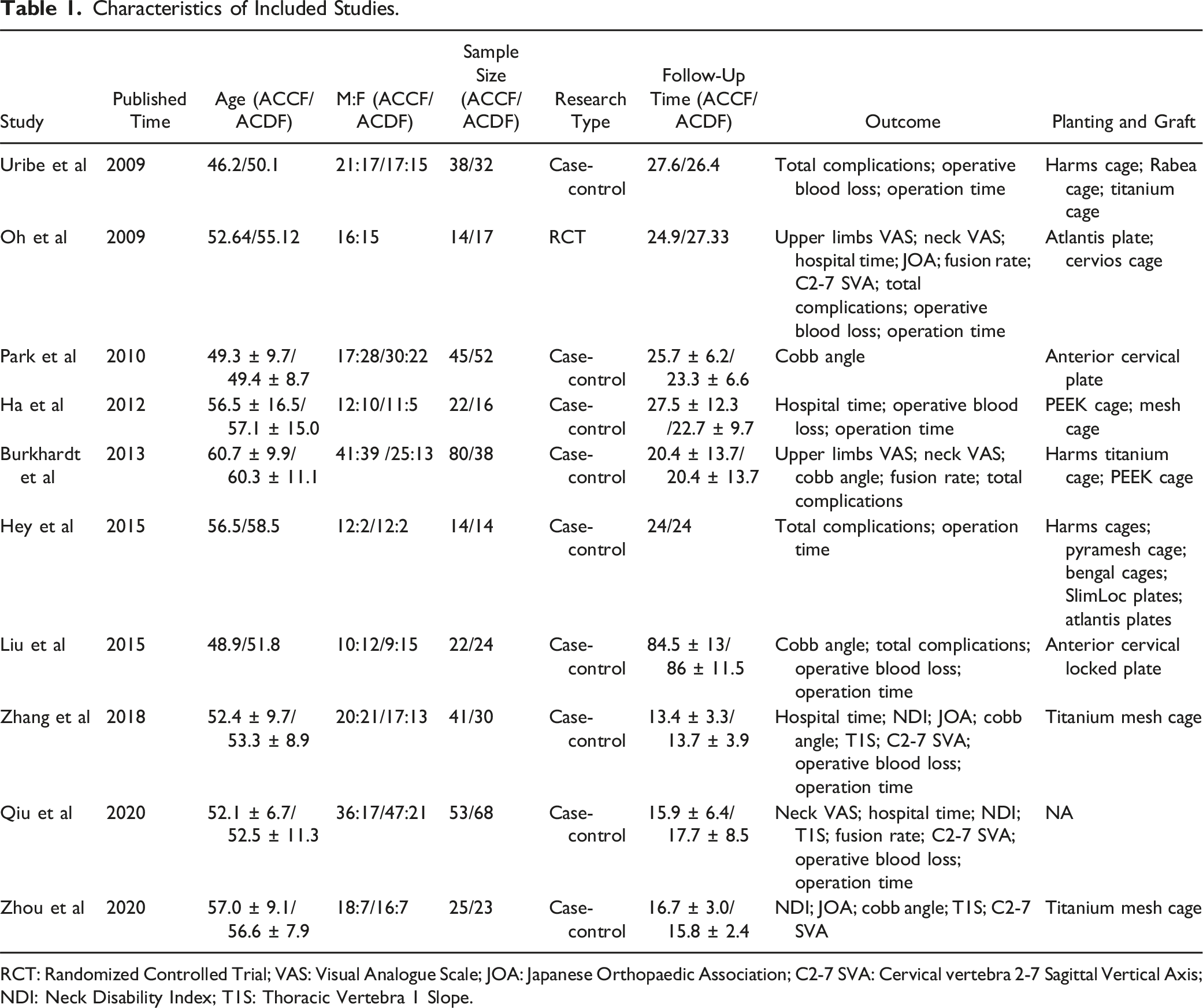
RCT: Randomized Controlled Trial; VAS: Visual Analogue Scale; JOA: Japanese Orthopaedic Association; C2-7 SVA: Cervical vertebra 2-7 Sagittal Vertical Axis; NDI: Neck Disability Index; T1S: Thoracic Vertebra 1 Slope.
Study Quality
The single included RCT 17 did not clearly describe the methods and process of randomization, resulting in a high risk assessment for blinding of participants and personnel. All other aspects were deemed low risk, leading to an overall quality rating of Grade B. Among the 9 case-control studies, Burkhardt, 18 Uribe, 19 Hey 20 scored 6 points each, indicating studies of moderate quality.Ha 21 , Zhang, 22 Liu, 23 Park, 24 Zhou, 2 Qiu 25 scored 7, 7, 8, 8, 7, and 8, respectively, placing them in the category of high-quality research.
Results
Clinical Outcomes
Upper Limb VAS
Two studies17,18 reported the impact of ACDF and ACCF on Upper Limb Visual Analog Scale (VAS) scores, and no heterogeneity was found between the studies (P = 0.49, I 2 = 0). A fixed-effects model was employed for the Meta-analysis. The results indicated no statistically significant difference in Upper Limb VAS scores between the two surgical approaches (SMD = 0.28, 95% CI: −0.08 to 0.63, P = 0.12), as shown in Supplemental Document 2.
Neck VAS
Three studies17,18,25 reported the impact of ACDF and ACCF on Neck VAS scores, and no heterogeneity was observed between the studies (P = 0.59, I 2 = 0). A fixed-effects model was employed for the Meta-analysis. The results indicated that there was no statistically significant difference in Neck VAS scores between the two surgical approaches (SMD = 0.06, 95% CI: −0.19 to 0.31, P = 0.62), as shown in Supplemental Document 3.
Hospital Time
Four studies17,21,22,25 reported the postoperative hospitalization duration for ACDF and ACCF. No heterogeneity was observed between the studies (P = 0.28, I
2
= 22), and a fixed-effects model was employed for the Meta-analysis. The results indicated a statistically significant difference in hospitalization duration between ACDF and ACCF, with ACDF showing a shorter postoperative hospital stay compared to ACCF (SMD = −0.29, 95% CI: −0.53 to −0.04, P < 0.05), as illustrated in Figure 2. The impact of ACDF and ACCF on the hospital time.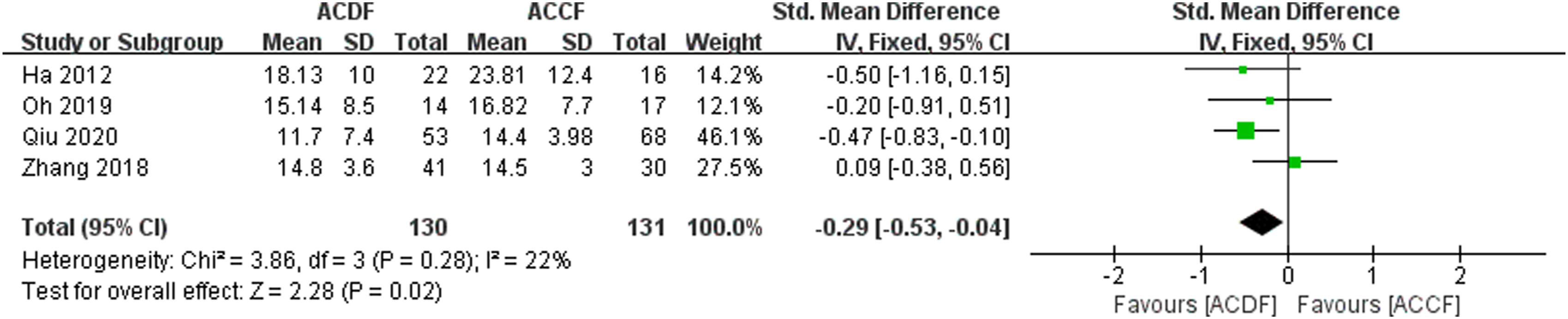
Neck Disabilitv Index
Four studies2,19,22,25 reported the impact of ACDF and ACCF on NDI scores, and no heterogeneity was observed between the studies (P = 0.90, I 2 = 0). A fixed-effects model was applied for the Meta-analysis. The results indicated that there was no statistically significant difference in NDI scores between the two surgical approaches (SMD = 0.22, 95% CI: −0.04 to 0.47, P = 0.10), as illustrated in Supplemental Document 4.
Japanese Orthopaedic Association
Four studies2,17,22,23 reported the impact of ACDF and ACCF on JOA scores. No heterogeneity was observed between the studies (P = 0.92, I2 = 0), and a fixed-effects model was employed for the meta-analysis. The results indicated that there was no statistically significant difference between the two surgical approaches in terms of JOA scores (SMD = 0.22, 95% CI: −0.07 to 0.50, P = 0.13), as shown in Supplemental Document 5.
Radiographic Outcomes
Cobb Angle
Five studies2,17,18,22,24 assessed the impact of ACDF and ACCF on cobb angle, and no heterogeneity was observed between the studies (P = 0.21, I
2
= 31). A fixed-effects model was applied for the meta-analysis. The results indicated that compared to ACCF, ACDF significantly improved the cobb angle of the cervical spine postoperatively, with a statistically significant difference (SMD = 0.52, 95% CI: 0.31 to 0.74, P < 0.01), as shown in Figure 3. The impact of ACDF and ACCF on the Cobb angle.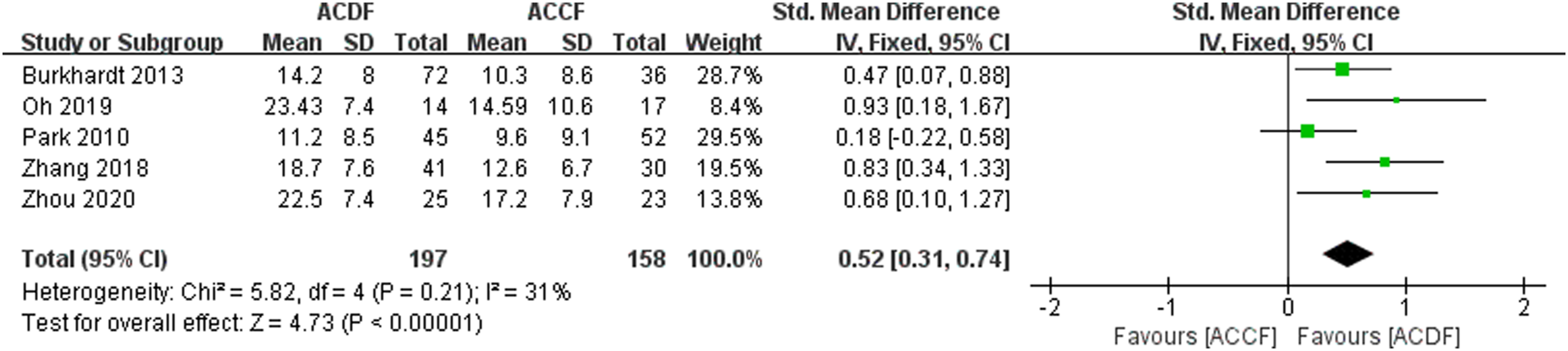
Thoracic Vertebra 1 Slope
Three studies2,22,25 evaluated the impact of ACDF and ACCF on T1S, and no heterogeneity was observed between the studies (P = 0.23, I
2
= 32). A fixed-effects model was applied for the Meta-analysis. The results indicated that postoperatively, ACDF significantly improved T1S in the cervical spine compared to ACCF, with a statistically significant difference (SMD = 0.54, 95% CI: 0.28 to 0.80, P < 0.01), as shown in Figure 4. The impact of ACDF and ACCF on the T1S.
Fusion Rate
Four studies17,18,23,25 assessed the fusion rate postoperatively for ACDF and ACCF, and no heterogeneity was observed between the studies (P = 0.19, I2 = 41). A fixed-effects model was applied for the Meta-analysis. The results indicated that there was no statistically significant difference in fusion rates between the two surgical approaches (RR = 0.99, 95% CI: 0.94 to 1.04, P = 0.71), as shown in Supplemental Document 6.
Cervical Vertebra 2-7 Sagittal Vertical Axis
Two studies22,25 assessed the impact of ACDF and ACCF on C2-7 SVA, and no heterogeneity was observed between the studies (P = 0.89, I 2 = 0). A fixed-effects model was applied for the Meta-analysis. The results indicated that there was no statistically significant difference between the two surgical approaches in terms of C2-7SVA (SMD = 0.15, 95% CI: −0.13 to 0.44, P = 0.30), as shown in Supplemental Document 7.
Surgical Outcomes
Total Complications
Six studies17-21,23 compared complications after ACDF and ACCF treatment for two-segment cervical spondylotic myelopathy. With moderate heterogeneity (P = 0.05, I 2 = 54%), a random-effects model was used. Results showed no significant difference in complications (RR = 0.63, 95% CI: 0.36 to 1.08, P = 0.09). Subgroup analysis for various complications found no significant differences between the procedures (all P > 0.05). See Supplemental Document 8 and Supplemental Document 9.
Blood Loss
Six studies17,19,21-23,25 compared the surgical blood loss between ACDF and ACCF, and there was heterogeneity among the studies (P < 0.01, I 2 = 98). A random-effects model was applied for the meta-analysis. The results indicated that there was no statistically significant difference in surgical blood loss between the two surgical approaches (SMD = −1.85, 95% CI: −3.92 to 0.22, P = 0.09), as shown in Supplemental Document 10.
Operation Time
Seven studies17-23,25 compared the surgical duration between ACDF and ACCF, and there was heterogeneity among the studies (P < 0.01, I2 = 96). A random-effects model was applied for the Meta-analysis. The results indicated that there was no statistically significant difference in the surgical duration between the two surgical approaches (SMD = −0.15, 95% CI: −1.22 to 0.92, P = 0.78), as illustrated in Supplemental Document 11.
Sensitivity Analysis
There was substantial heterogeneity in both blood loss and operation time, and we conducted sensitivity analyses to assess their robustness. A leave-one-out sensitivity analysis was performed for these two outcomes. The results of the analysis showed that the pooled results for blood loss and operation time remained unchanged when each study was sequentially omitted, indicating the robustness of the findings. Unfortunately, despite these efforts, the high heterogeneity in blood loss and operation time could not be mitigated.
Publication Bias
Due to the inclusion of fewer than 10 studies for all outcome measures in this study, a funnel plot analysis was not conducted.
Discussion
Anterior cervical decompression surgery has gained popularity for its direct decompression of the spinal cord and nerve roots, correcting cervical lordosis and restoring normal spine curvature. 26 ACDF and ACCF are the main procedures, each with its own safety and effectiveness. However, it remains uncertain which is better for adjacent two-segment cervical spondylotic myelopathy. Our meta-analysis compared outcomes from 10 articles published between 2009 and 2020 using ACDF and ACCF for this condition, representing the first analysis of its kind.
The JOA score is a valuable tool for assessing neurological function in cervical myelopathy patients post-surgery, 27 while the NDI is widely used for evaluating functional impairment related to cervical spine dysfunction. 28 The VAS helps gauge pain intensity and overall health status. 29 This meta-analysis found significant improvements in JOA scores, upper limb VAS, neck VAS, and NDI scores after both ACDF and ACCF surgeries for adjacent two-segment cervical myelopathy. Importantly, there were no significant differences between the two procedures, indicating both effectively decompress the spinal cord and improve neurological function with positive clinical outcomes.
Concerning hospitalization duration, the meta-analysis results indicate that ACCF requires a longer hospital stay, ranging from 9 to 36 days with an average stay of 11 to 24 days, while ACDF ranges from 4 to 28 days with an average stay of 7 to 22 days, demonstrating a significant statistical difference. This discrepancy is explained by the more complex nature of the ACCF procedure, which exposes patients to more severe spinal cord injuries than those undergoing ACDF, resulting in a slower postoperative recovery period. 30
Maintaining a balanced cervical sagittal profile reduces neck muscle energy consumption, preserving normal physiological cervical spine movement, preventing adjacent segment degeneration, and crucially informs surgical approach selection. Basic parameters include T1S, cobb angle, C2-7 SVA, among others.2,31,32 Basic parameters like T1S, cobb angle, and C2-7 SVA were analyzed. This study found that ACDF, compared to ACCF, notably increases cobb angle and T1S, restoring cervical spine curvature. This aligns with Huang et al’s findings. 33 Cervical lordosis may explain this, causing decreased cobb angle and T1S due to curvature loss and segment subsidence. ACDF offers more traction and fixation points, distributing force evenly on the vertebral body, preventing subsidence, and maintaining/improving cervical lordosis and segmental height.17,34 In contrast, ACCF employs a titanium mesh, lacking pre-bending capability, providing primarily axial support and straightening the cervical spine, leading to uneven force distribution. 2 Studies have found that sagittal imbalance is associated with persistent pain and overall spinal alignment dysfunction. Worsening of the T1S and Cobb angle can partially indicate functional impairment and poorer quality of life in patients. 35
Regarding C2-7SVA, there was no significant difference between ACDF and ACCF, but studies disagree on their effect. Zhou et al. 2 claim ACDF increases C2-7SVA, while ACCF decreases it; Zhang et al. 22 argue the opposite. Qiu et al 25 found both surgeries reduce C2-7SVA. The limited number of studies (only 2 articles22,25 included) may contribute to this discrepancy, potentially resulting in false-negative findings. Surgery improves Cobb angle and T1S, but internal fixation may not fully restore curvature, hastening adjacent vertebral body degeneration. Postoperative C2-7 SVA increase can overload motion segments, raising Adjacent Segment Disease risk.36-38 Surgeons often prioritize Cobb angle and T1S recovery, neglecting C2-C7 cSVA impact on cervical degeneration. Future studies should thoroughly investigate ACDF and ACCF effects on C2-7SVA.Postoperative interbody fusion rate in anterior cervical spine surgery impacts spinal stability, reoperation rates, and patient recovery, crucial in imaging outcomes. 5 This study shows both ACDF and ACCF achieve high fusion rates with no significant difference, consistent with Wen et al, despite varying opinions in the literature. 39 Initially, ACCF had a higher fusion rate than ACDF within the same postoperative timeframe. However, by the last follow-up, ACDF showed comparable or even superior fusion rates. Despite early advantages for ACCF, pseudarthrosis formation has little impact on clinical outcomes, and bone healing is slow. 25 Over time, differences between the two procedures are expected to diminish, ultimately achieving comparable high fusion rates. Fusion rate also correlates with the number of fused segments. 40 Selecting cases with equal segment numbers in this study may have influenced observed fusion rate differences. Nonetheless, both procedures effectively maintain cervical spine stability. However, detecting subtle differences in literature is limited by small sample sizes and segment considerations. Larger, more diverse samples in future studies are recommended for deeper insights.This study examined procedure safety regarding total complications, blood loss, and operation time, finding no significant differences between ACDF and ACCF. Complications are a critical aspect of surgical outcomes, and this study not only analyzed the total number of complications but also performed a meta-analysis for each specific type. The results showed no statistically significant differences, either in the overall number of complications or in individual categories, which may be due to the limited number of included studies. Therefore, further high-quality and detailed research is needed to explore this area more comprehensively.Yu et al's 41 subgroup analysis similarly showed no difference in total complication rates between the two procedures. Despite some studies suggesting ACCF procedures are more complex with greater blood loss and longer operation times, our study found no significant differences in these aspects.30,33 Zhang et al proposed factors like implants, segment levels, and surgical techniques impact outcomes. With various implants and segment levels in our study, we hypothesize blood loss and operation time are influenced by procedure complexity, surgeon expertise, and implant types.42,43Moreover, autografts have been associated with higher rates of donor site bleeding, infection, and pain compared to other grafting materials. 8 The resluts included in this research used various grafting materials, such as titanium mesh cages, autografts, and plates, across different segment levels. We hypothesize that blood loss and operative time are influenced not only by the complexity of the procedure but also by segment levels, the surgeon’s expertise, and the types of implants used. Further research is needed to validate this hypothesis.
The selection of plates and implants remains a challenge in both ACCF and ACDF procedures. To provide more evidence in this area, this study analyzed the plates and implants used in the included studies (Table 1). Unfortunately, the literature did not consistently report details on the choice of plates and implants, and the variety in brands and specifications was considerable, making direct comparison and analysis difficult. This represents a limitation of the current research. Future studies should focus on standardizing and analyzing these variables to provide more clinically relevant guidance.
Subsidence is a common occurrence following both ACCF and ACDF procedures; however, this study did not conduct a detailed analysis of subsidence rates, as only one included study provided specific data, most of which lacked statistical significance. The available evidence indicates that subsidence primarily occurs within the first 6 weeks postoperatively, characterized by a reduction in disc height and localized cervical lordosis, with more pronounced effects observed in the ACCF group. 24 Although subsidence may increase the risk of hardware failure and fusion complications, its impact on overall cervical alignment and clinical outcomes appears to be limited. In fact, mild subsidence may even facilitate the fusion process.19,44 Preventing excessive distraction and preserving endplate integrity can help reduce subsidence. While anterior cervical plates may improve fusion rates, they could also inhibit subsidence and affect graft-endplate contact. 45 We encourage future research to involve more investigators in exploring whether subsidence has a positive impact on ACCF and ACDF, or in conducting quantitative studies on the effects of subsidence in these procedures. Such investigations would enhance clinicians’ understanding of patients' long-term outcomes and reoperation indications.
In summary, both ACCF and ACDF have their respective advantages in anterior cervical decompression surgery, and the choice of procedure should be based on the specific condition and characteristics of the compression in each patient. For patients with posterior vertebral compression, especially those with large endplate osteophytes or significant disc herniation, ACCF offers greater surgical access and more effective decompression. Conversely, ACDF is more suitable for patients with soft disc herniation or those who do not require extensive decompression, as it preserves vertebral structure, minimizes damage to the anterior column, and typically results in shorter operation times and less blood loss. With advancements in medical technology, the indications for ACDF have gradually expanded, and its surgical limitations have diminished.7,25,46 The results of this study indicate that ACDF is superior in improving cervical curvature and reducing hospital stay; thus, it may be a more effective choice in the majority of anterior cervical decompression surgeries. However, when selecting a surgical strategy, it is essential to consider factors such as patient age, symptom severity, the extent of decompression required, and the risk of postoperative complications to achieve individualized treatment and optimize clinical outcomes.
Limitations
Due to the nature of systematic reviews and meta-analyses, our analysis relies solely on the available literature. Firstly, the quantity and quality of included studies were limited, leading to insufficient exploration of critical factors such as C2-7 SVA and fusion rates. Secondly, important indicators like complete blood count and rehabilitation protocols were not addressed in the literature, impacting our assessment of intervention outcomes. Lastly, significant heterogeneity was noted in blood loss and operation time, which remained unchanged after sensitivity analysis. Further high-quality studies are needed to comprehensively explore these factors, considering potential influences from cervical compression severity and surgical expertise.There is a significant lack of literature regarding the long-term efficacy and reoperation rates of ACCF and ACDF, which has important implications for the conclusions of this study. Existing research primarily focuses on short-term outcomes, failing to adequately address the reoperation risks for patients, which is crucial for clinical practice. Future studies should emphasize the collection of long-term follow-up data to fill this gap and provide more reliable guidance for clinical decision-making.
Conclusions
In conclusion, anterior cervical decompression surgery, including ACDF and ACCF, demonstrates significant efficacy in treating adjacent two-segment cervical spondylotic myelopathy. Both procedures effectively improve clinical outcomes, with comparable results in terms of neurological function enhancement and pain reduction. While ACCF may necessitate longer hospitalization due to its complexity, ACDF offers advantages in restoring cervical curvature. Additionally, both procedures exhibit comparable rates of interbody fusion and safety profiles. Considering factors such as patient age, symptom severity, and compression source, ACDF emerges as a preferred option, given its expanding indications and diminishing surgical limitations. Nonetheless, further research is warranted to explore the long-term impact on cervical degeneration and validate these findings. Overall, ACDF stands out as a more effective surgical approach for anterior cervical decompression procedures in the treatment of adjacent two-segment cervical spondylotic myelopathy.
Supplemental Material
Supplemental Material - Meta-Analysis of Treatment for Adjacent Two-Segment Cervical Spondylotic Myelopathy: A Comparison Between Anterior Cervical Corpectomy and Fusion and Anterior Cervical Discectomy and Fusion
Supplemental Material for Meta-Analysis of Treatment for Adjacent Two-Segment Cervical Spondylotic Myelopathy: A Comparison Between Anterior Cervical Corpectomy and Fusion and Anterior Cervical Discectomy and Fusion by Lei Chen, Zhongyi Zhang, MD, Ju Li, Peijian Tong, and Taotao Xu in Global Spine Journal.
Footnotes
Acknowledgments
We thank all the individuals whose contributions and support have been invaluable throughout the process of writing this paper. All authors contributed to the study conception and design. The basic framework and conception of this article were performed by Lei Chen and Zhongyi Zhang. The first draft of the manuscript was written by Lei Chen, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Each author certifies that there are no funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members.
Funding
This work was supported by grants from Traditional Chinese Medicine Science and Technology Program of Zhejiang Province (No. 2023ZL367), National Natural Science Foundation of Zhejiang Province (No. LY24H270001) and 2024 Zhejiang Chinese Medicine University Cultivation Plan for Top Innovative Talents of Postgraduates (No. : 2024YJSBJ011).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.