
Abstract
Study Design
Retrospective cohort study.
Objectives
To evaluate whether different radiographic clusters of adult spinal deformity identified using artificial intelligence-based clustering are associated with distinct surgical outcomes.
Methods
Patients were classified based on the results of a previously conducted analysis that examined clusters of deformity, including Moderate Sagittal (Mod Sag), Severe Sagittal (Sev Sag), Coronal, and Hyper-Thoracic Kyphosis (Hyper-TK). The surgical data, HRQOL, and complication outcomes of these clusters were then compared.
Results
The final analysis included 1062 patients. Similar to published results on a different patient sample, Mod Sag and Sev Sag patients were older, more likely to have a history of previous spine surgery, and more disabled. By 2-year, all clusters improved in HRQOL and reached a similar rate of minimal clinically important difference (MCID).
The Sev Sag cluster had the highest rate major complications (53% vs 34-40%), and complications leading to reoperation (29% vs 17-23%), implant failures (20% vs 8-11%), and operative complications (27% vs 10-17%). Coronal patients had the highest rate of pulmonary complications (9% vs 3-6%) but the lowest rate of X-ray imbalance (10% vs 19-21%). No significant differences were found in neurological complications, infection rate, gastrointestinal, or cardiac events (all P > .1). Kaplan-Meier survival curves demonstrated a lower time to first complications for the Sev Sag cluster.
Conclusions
All clusters of adult spinal deformity benefit similarly from surgery as they all achieved similar rates of MCID. Although the rates of complications varied among the clusters, the types of complications were not significantly different.
Keywords
Introduction
Adult spinal deformity (ASD) affects as many as 60% of the elderly population and often leads to detrimental effects on function and quality of life.1-3 Bess et al demonstrated that ASD affects the patient’s quality of life to the same degree as other debilitating chronic diseases such as diabetes, heart disease, and rheumatoid arthritis. 4 Surgical deformity correction is often indicated to provide improvement in quality of life in patients with reduced disability; however, careful consideration of patient and deformity characteristics is paramount in surgical decision-making at the individual patient level. 5
Classification systems of ASD driven by artificial intelligence (AI) algorithms have the potential to provide valuable patient-focused data to help guide surgical decision-making and patient counseling.6,7 Kim et al. used a two-step cluster analysis to determine 3 distinct clusters of cervical deformity. 8 Using unsupervised hierarchical clustering, Ames et al. identified twelve subgroups of ASD patients based on radiographic, surgical, and patient factors to aid with preoperative decision-making. 9 Finally, Lafage et al applied an unsupervised AI approach to a large multicenter database of complex ASD patients and identified 4 natural clusters of deformity, including Hyper-Thoracic Kyphosis (Hyper-TK), Moderate Sagittal (Mod Sag), Severe Sagittal (Sev Sag), and Coronal. 10 Moreover, these deformity cohorts were associated with distinct perioperative outcomes.
These studies highlight the extensive clinical and radiographic heterogeneity of ASD and warrant a more thorough evaluation of the differences in surgical and patient-reported outcomes across deformity clusters. Therefore, the current study applied the previously established AI-based clustering techniques 10 on a separate database of surgical ASD patients and compared the treatment outcomes associated with various deformity clusters. We hypothesized that distinct clusters of deformity would be associated with differences in 2-year postoperative HRQOL outcomes after ASD surgery.
Methods
Patient Population
We conducted a retrospective analysis of a prospective multicenter database of ASD patients. Institutional review board (IRB) approval was obtained at each site prior to study initiation, and informed consent was obtained from each patient. We included patients above 18 years of age who met the radiological criteria of ASD (coronal Cobb angle >20°, sagittal vertical axis [SVA] >5 cm, pelvic tilt [PT] >25°, or TK >60°) and underwent ASD surgery. Exclusion criteria included trauma, active tumor, inflammatory conditions, and neuromuscular disorders. Details can be find on ClinicalTrials.gov website, under ID NCT00738439.
Data Collection
Prospective data were collected via IRB-approved proprietary study group clinical research forms that included demographic data (age, sex, race, body mass index [BMI]) and past medical history (Charlson Comorbidity Index [CCI], prior spine surgery, American Society of Anesthesiologists [ASA] score). Collected surgical details included locations of the posterior instrumentation upper-most instrumented vertebra (UIV) and lower-most instrumented vertebra (LIV), utilization of interbody fusion (IBF), direct decompression, osteotomy, and 3-column osteotomy (3CO). Perioperative data including length of hospital stay (LOS), intensive care unit (ICU) stay, and estimated blood loss (EBL) were also recorded.
Standardized patient-reported outcomes (health-related quality of life [HRQOL]) were collected preoperatively and 2 years postoperatively and included numeric rating scale (NRS) for back and leg pain, Oswestry Disability Index (ODI), 36-Item Short Form Survey (SF-36), and Scoliosis Research Society 22-Item Scale (SRS-22). Achievement of minimal clinically important difference (MCID) was analyzed, which was defined as a change pre- to post-operatively greater than 15 points for ODI, 5.2 points for SF-36, .374 points for SRS Activity, .586 points for SRS Pain, and .790 points for SRS Appearance. Complications within the 2-year postoperative period were recorded and stratified based on severity (major vs minor adverse event, requirement of reoperation) and type (medical vs surgical).
Full-length free-standing anterior-posterior and lateral spine radiographs were obtained pre- and postoperatively and were analyzed by 2 trained independent observers using a dedicated software (Spineview, ENSAM Laboratory of Biomechanics, Paris, France). 11 Radiographic parameters were extracted and calculated using Matlab (MathWork, Natick, Massachusetts). Radiographic parameters collected included pelvic tilt (PT), pelvic incidence (PI), lumbar lordosis (LL), spinopelvic mismatch between PI and LL (PI-LL), T1 pelvic angle (TPA), sagittal vertical axis (SVA), and thoracic and thoracolumbar Cobb angles. Patients were also classified according to the SRS-Schwab Classification. 12
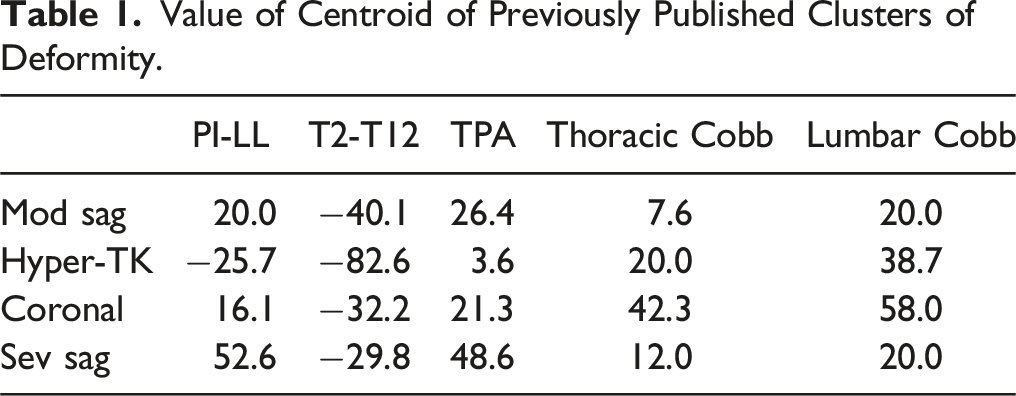
Deformity Clusters
Value of Centroid of Previously Published Clusters of Deformity.
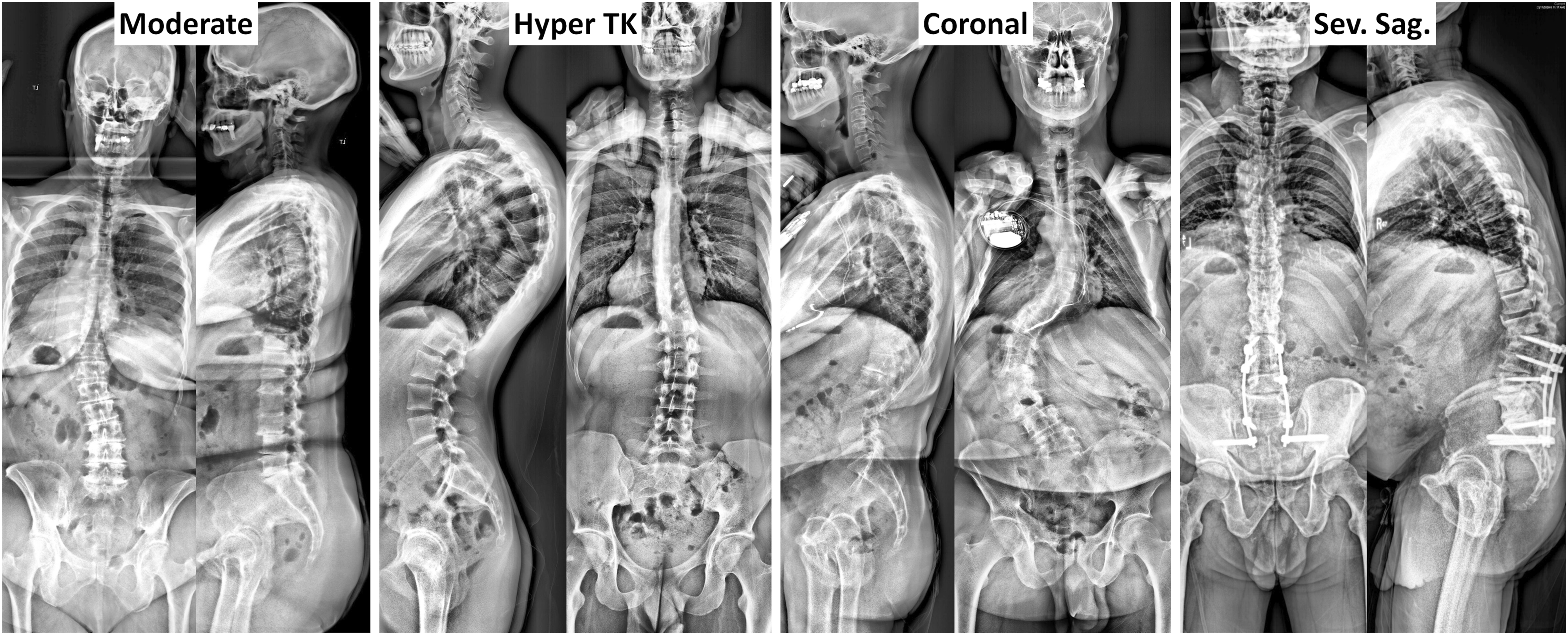
Examples of type of deformity from previously published cluster of deformity.
Statistical Analysis
Descriptive statistics were provided for all demographic, clinical, and radiographic data using mean ± standard deviation (StD), median and interquartile range (IQR), or frequencies, as appropriate. Deformity cluster cohorts were compared based on preoperative information, perioperative variables, and 2-year postoperative outcomes (pre- to postoperative changes in HRQOLs, rate of MCID achievement, and complication rates) using Kruskal-Wallis, analysis of variance (ANOVA), or Chi-Square test, as appropriate. After stratification by deformity type, multivariate logistic regression controlling for age, BMI, CCI, ASA, and preoperative HRQOL was conducted to evaluate whether surgical procedure was independently associated with MCID achievement or complication. All statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY). The level of statistical significance was set at P < .05 a priori.
Results
Cohort Description
There was a total of 1476 eligible patients in the database, out of which 1062 patients (72%) completed their 2-year postoperative follow-up and were included in the study. The median follow-up period was 25 months (IQR 24 to 30 months). The study cohort had a mean age of 60.6 ± 14.2 years, mean BMI of 28.1 ± 5.9 kg/m2, 809 (76.2%) female patients, and 935 (88.0%) white patients. Median CCI was 1.5 (IQR 0 to 3), 528 (49.7%) patients with ASA grade 2, and 432 (40.7%) patients with ASA grade 3. Preoperative HRQOLs revealed moderate to severe baseline disability and pain, with a median NRS back pain of 8 (IQR 6 to 9) and 59.5% of patients with ODI >40. In assessment of preoperative SRS Classification, there were 431 (40.6%) patients classified with a curve type of N, 339 (31.9%) classified with L, and 249 (23.4%) classified with D. 682 (64.2%) patients had a PI-LL modifier of “+” or “++,” 708 (66.7%) patients had a PT modifier of “+” or “++,” and 636 (59.9%) patients had an SVA modifier of “+” or “++.”
Posterior fixation was performed in 99.0% of patients included in the analysis. Median number of levels treated was 9 (IQR 8 to 14), 59.8% of patients had between 5 to 12 levels treated, and 29.1% had 13 or more levels treated. Direct decompression was performed in 59.0% of the cases. Some osteotomy was performed in 70.9% of cases, while major osteotomy (pedicle subtraction osteotomy [PSO] or vertebral column resection [VCR]) was performed in 17.4% of cases. 65.0% of cases involved interbody fusion techniques. Supplemental rod was used in 19.5% of cases, while bone morphogenetic protein (BMP) was used in 68.0% of cases.
The median EBL was 1300 cc (IQR 600 to 2150). 64.9% of patients required ICU stay postoperatively, and 13.7% required longer than 48 h of ICU stay. The median LOS was 7 days (IQR 5 to 9).
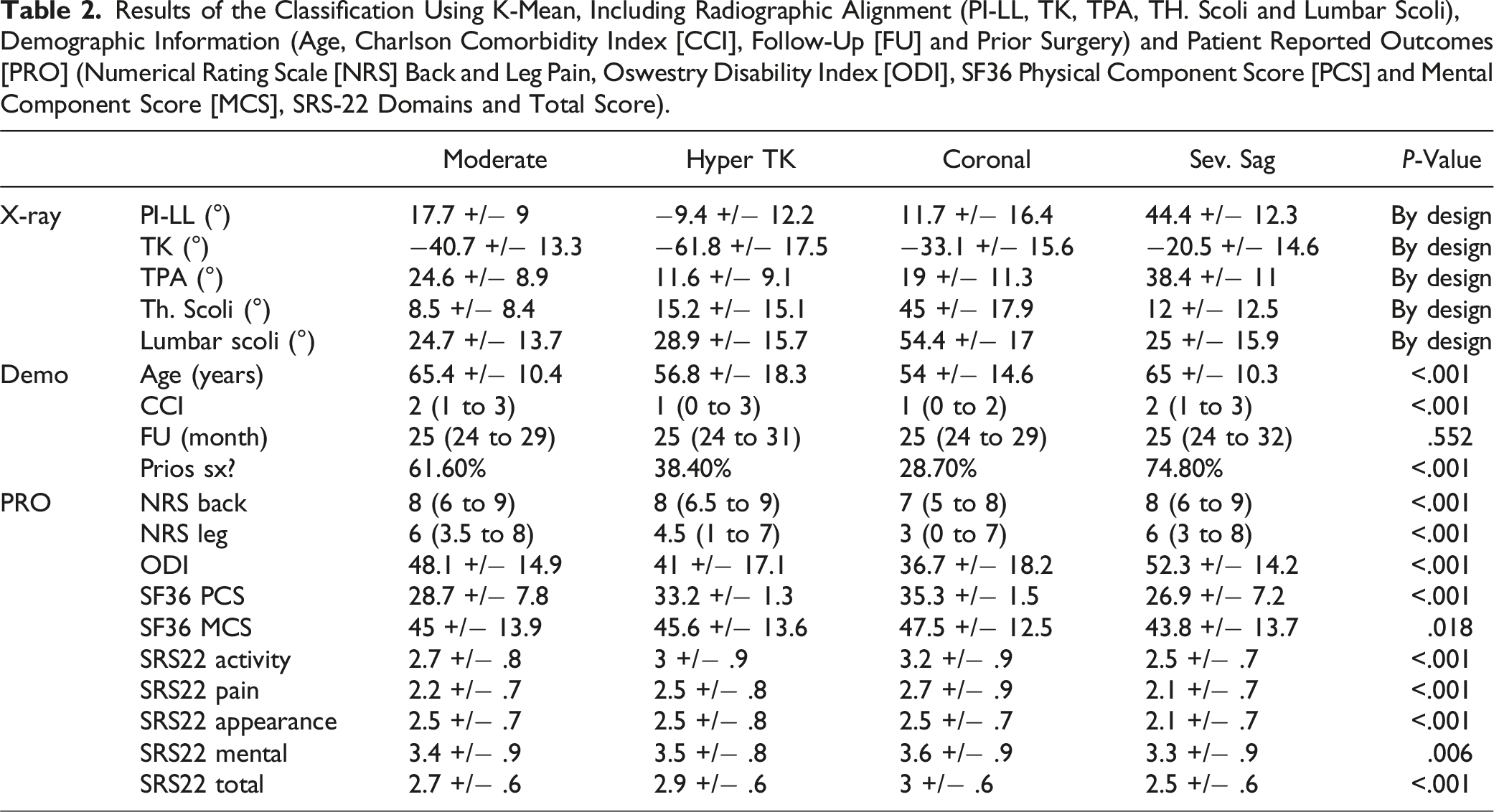
Type of Deformity
Results of the Classification Using K-Mean, Including Radiographic Alignment (PI-LL, TK, TPA, TH. Scoli and Lumbar Scoli), Demographic Information (Age, Charlson Comorbidity Index [CCI], Follow-Up [FU] and Prior Surgery) and Patient Reported Outcomes [PRO] (Numerical Rating Scale [NRS] Back and Leg Pain, Oswestry Disability Index [ODI], SF36 Physical Component Score [PCS] and Mental Component Score [MCS], SRS-22 Domains and Total Score).
2-Year Postoperative Outcomes
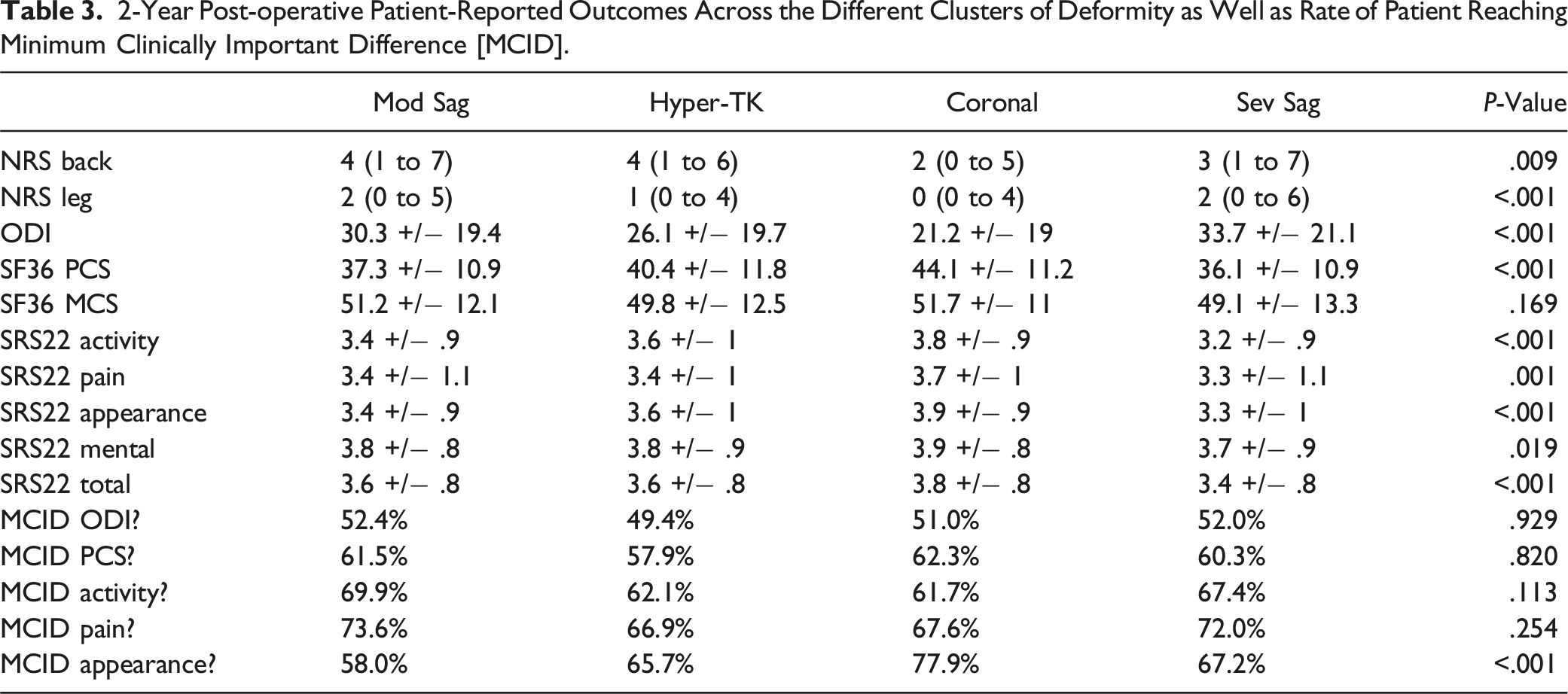
Comparison of 2-year postoperative HRQOL outcomes demonstrated significant differences among the different types of deformity, except for the SF-36 Mental Component Score. Compared to other types, Coronal patients generally had better outcomes, with lower pain scores (NRS back 2 vs 3-4, P = .009; NRS leg 0 vs 1-2, P < .001), less disability (ODI 21.2 vs 26.1-33.7, P < .001), better appearance score (3.9 vs 3.3-3.6, P < .001), and higher activity score (3.8 vs 3.2-3.6, P < .001). Conversely, Sev Sag patients had higher disability at 2-year follow-up than other clusters (33.7 vs 21.2-30.3, P < .001).
There were significant differences in SRS-22 Patient Satisfaction scores at 2-year follow-up between the clusters. Coronal patients demonstrated higher satisfaction (4.3 ± .9) than other types of deformity (Mod Sag: 4.1 ± 1.0; Hyper-TK: 4.1 ± 1.0; Sev Sag: 4.1 ± 1.0, P < .035). In response to the question, “Are you satisfied with the results of your back management?” 75.5% of Coronal patients answered either “Satisfied” or “Very satisfied,” compared to 64.0% for Sev Sag, 66.4% for Mod Sag, and 72.4% for Hyper-TK (P = .017). However, there was no statistically significant difference among the deformity types in their responses to the question, “Would you have the same management again if you had the same condition?,” with the response rate of either “Probably” or “Definitely” ranging from 77.2% to 84.4% (P = .103).
2-Year Post-operative Patient-Reported Outcomes Across the Different Clusters of Deformity as Well as Rate of Patient Reaching Minimum Clinically Important Difference [MCID].
Survival curves up to 730 days (2 years) was analyzed and revealed significant differences in survival functions among types of deformity (Figure 2). For any type of complication (log rank P = .014, pairwise comparison demonstrated a significant difference between Hyper-TK and other types (all P < .05). For any complication outside of adverse events (log rank P = .001), Hyper-TK patients had a higher survival rate than other types (all P < .05). Sev Sag had a lower survival curve than Coronal (P = .021) and a trend toward lower survival curve than Mod Sag, although it was statistically insignificant (P = .052). There was no significant difference in survival function between Coronal and Mod Sag. When evaluating survival functions for major complication leading to reoperation (log rank P = .003), Sev Sag type demonstrated significantly lower survival function than Coronal (P < .001), Mod Sag (P = .028), and a trend toward lower than Hyper-TK (P = .059). There were no significant differences for major complication not leading to reoperation (log rank P = .057), although Sev Sag trended toward having a lower survival function. There were no significant differences in survival functions for medical complications (log rank P = .061). For survival rate of surgical complications (log rank P < .001), there were significant differences in survival function between Coronal/Hyper-TK vs Mod Sag vs Sev Sag types (all pairwise P < .05). However, there was no significant difference between Coronal and Hyper-TK types. Kaplan-Meier survival curves up to 720 days by type of deformity including survival rate until first complication (top left); survival rate until first complication outside of unrelated AE (top right); survival rate until first major complication requiring a reoperation (middle left); survival rate until first major complication not requiring a reoperation (middle right); survival rate until first medical complication (bottom left); and survival rate until first surgical complication (bottom right).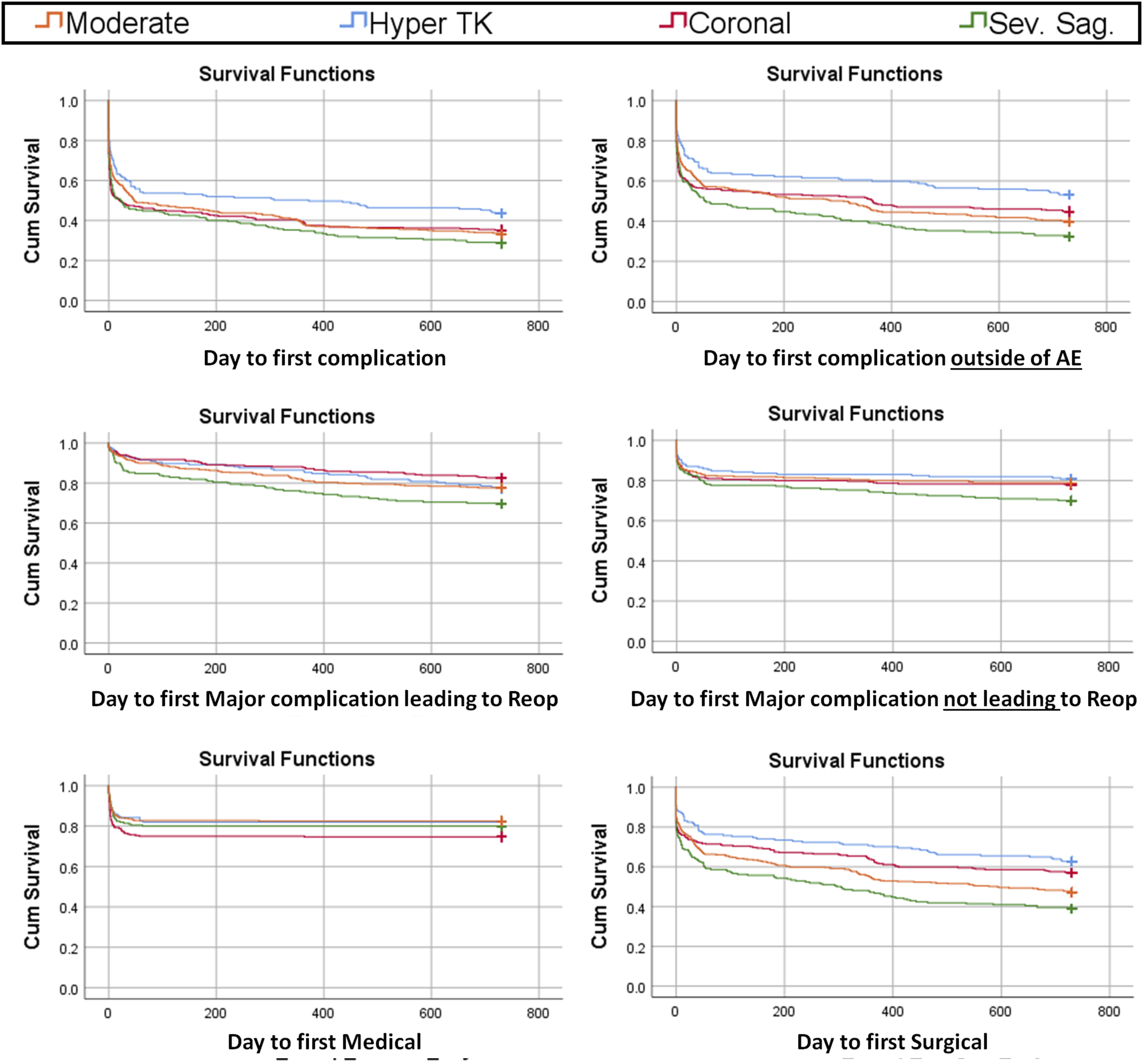
Multilinear analyses were performed within each cluster, controlling for preoperative information. For Mod Sag patients, having more than 12 levels fused increased the likelihood of reaching MCID for ODI (odds ratio [OR] 3.456 [1.389 – 8.596]) and MCID for PCS (OR 3.456 [1.389 – 8.596]), while having 1-4 levels fused decreased the likelihood of having any complication (OR 0.364 [0.182 – 0.730]) and major complications (OR 0.402 [0.196 – 0.827]). In addition, the use of BMP increased the likelihood of complication (OR 1.778 [1.008 – 3.138]), while 3CO increased the likelihood for major complication (OR 3.774 [1.837 – 7.753]) and reoperation (OR 2.520 [1.247 – 5.093]).
Within the Coronal cluster, use of IBF increased the likelihood of reaching MCID for ODI (OR 2.470 [1.311 – 4.656]) and SRS-22 Activity (OR 2.141 [1.105 – 4.150]), but also increased the likelihood of any complication (OR 2.337 [1.249 – 4.375]) and major complication (OR 2.210 [1.167 – 4.185]). The use of supplemental rod increased the likelihood of reaching MCID for ODI (OR 2.057 [1.006 – 4.206]) and SRS-22 Activity (OR 2.281 [1.049 – 4.959]) and decreased the chance of reoperation (OR 0.255 [0.093 – 0.701]). Long constructs increased the likelihood of complication (OR 1.897 [1.013 – 3.553]), major complication (OR 2.878 [1.538 – 5.388]), and reoperation (OR 2.949 [1.371 – 6.346]), while use of osteotomy decreased the likelihood of complications (OR 0.449 [0.218 – 0.925]).
For the Hyper-TK clusters, use of BMP decreased the likelihood of reaching MCID for PCS (OR 0.308 [0.112 – 0.847]) and the likelihood of having a major complication (OR 0.237 [0.093 – 0.606]). Use of minimally invasive (MIS) techniques for posterior fusion decreased the likelihood of reaching MCID for SRS-22 Appearance (OR 0.246 [0.063 – 0.968]) and having a major complication (OR 0.117 [0.023 – 0.594]). Having a long construct increased the likelihood of having a complication (OR 4.313 [1.433 – 12.98]).
Finally, among Sev Sag patients, having a short construct decreased the likelihood of reaching MCID for SRS-22 Activity (OR 0.052 [0.004 – 0.630]) and Appearance (OR 0.090 [0.008 – 0.967]).
Discussion
Adult spinal deformity has a profound impact on patient quality of life.4,13 The substantial clinical, radiographic, and operative heterogeneity associated with ASD often makes clinical decision-making and patient counseling challenging.14-16 AI-based hierarchical clustering has the promising potential to augment patient-specific care by incorporating numerous variables into granular patient population segmentation.17-19 In the current study, we employed a previously established unsupervised clustering algorithm to categorize 1062 ASD patients into 4 distinct deformity subgroups and investigated the 2-year postoperative outcomes for each deformity type. While the deformity clusters exhibited differences in baseline and postoperative HRQOLs, the rates of MCID achievement were similar. These findings provide valuable insights into the heterogeneity of ASD patients, emphasizing the importance of understanding distinct clusters of deformity and their implications for surgical outcomes.
The deformity subtypes utilized in this study were described in a previous clustering analysis of a database of 286 complex ASD patients, which showed that radiographic clustering was intimately associated with host characteristics such as demographics and level of disability. 10 Although these 4 clusters are not the only presentations of complex ASD, they serve as a reflection of the significant heterogeneity of the ASD population. In our cohort, the 4 clusters had distinct baseline clinical and radiographic properties, with the Hyper-TK subtype generally being younger and associated with the lowest disability and pain scores preoperatively. Conversely, Mod Sag and Sev Sag cohorts were older, more disabled at baseline, and more likely to have a history of spine surgery. These findings are consistent with the published results on a different dataset and may reflect the fact that thoracic hyperkyphosis in adults often results from long-term progression of a congenital condition, such as Scheuermann’s kyphosis, as opposed to a predominantly degenerative disease.10,20
All clusters demonstrated significant improvements in HRQOLs postoperatively, achieving MCID at similar rates by 2 years postoperatively. However, the magnitude and trajectory of improvement varied among clusters, with some groups experiencing more pronounced residual disability and pain at the 2-year follow-up. Coronal patients generally had better postoperative outcomes, with lower pain scores, less disability, better appearance score, and higher activity score. In addition, the Coronal cluster had a higher rate of MCID achievement for SRS-22 appearance compared to the Mod Sag cluster. Conversely, Sev Sag patients were most likely to remain disabled postoperatively than other cohorts and demonstrated lower survival function for major complications leading to reoperation. This is consistent with the previously demonstrated linear relationship between the degree of sagittal imbalance and severity of disability in patients with adult spinal deformity.21,22 Such direct relationship with clinical outcomes has been less consistently reproduced with regard to coronal balance, with several investigations finding that coronal malalignment is not a predictive factor for complications and reoperation after ASD surgery.23-25
The current study also evaluated the surgical factors associated with outcomes for each cluster. Within the Mod Sag cluster, fusion involving more than 12 levels increased the likelihood of achieving MCID for ODI and PCS, and 1-4 level fusion was associated with a lower complication risk. Among Coronal patients, the use of a supplemental rod was associated with favorable outcomes, increasing the likelihood of MCID achievement for ODI and activity scores while decreasing the risk of reoperation. Long constructs were associated with higher rates of all complications, major complications, and reoperation. Long constructs were similarly associated with poor outcome in the Hyper-TK cohort, increasing the likelihood of complications. Lastly, within the Sev Sag cluster, short constructs were associated with lower likelihood of achieving MCID for activity and appearance.
Several limitations must be considered when interpreting this study. The retrospective study design limits the level evidence and the conclusions that can be drawn. This radiographic classification is limited to ASD patients who were surgically treated only by members of our study group; inclusion of non-operative patients and patients treated at additional clinical sites may reveal greater diversity of deformity clusters. In addition, this classification does not consider the cervical spine, horizontal gaze acquisition, or lower extremity compensation. Thus, further investigation incorporating full-body image analysis may allow the development of a more detailed classification system. Finally, while our study provides valuable data on 2-year postoperative outcomes, future studies with longer follow-up periods may provide additional insight as some patients may experience loss of alignment and deterioration beyond the 2-year follow-up period.26,27
Conclusion
This study applied established AI-based clustering techniques on a database of surgical ASD patients and compared the treatment outcomes associated with various deformity clusters. All clusters of deformity achieved MCID at similar rates, although the Coronal deformity cluster showed significantly higher MCID achievement rate in appearance score. Although the rates of complications varied among the clusters, the types of complications were not significantly different. By elucidating distinct ASD clusters and their clinical implications, the current study may allow for better anticipation of long-term surgical outcomes and underscores the potential utility of machine learning clustering as a prognostic tool in ASD patients.
Footnotes
Author’s Note
The manuscript submitted does not contain information about medical device(s)/drug(s).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The International Spine Study Group (ISSG) is funded through research grants from DePuy Synthes (current), Nuvasive (current), K2M (current), Innovasis (past), Biomet (past), and individual donations. Funding sources did not play a role in the investigation.
IRB Approval
This study was conducted according to strict institutional review board standards at each institution and abided by ethical guidelines for human subject research. Details can be found on ClinicalTrials.gov under ID NCT00738439.