
Abstract
Study Design
Machine learning model.
Objectives
This study aimed to develop and validate a machine learning (ML) model to predict moderate-severe anterior bone loss (ABL) following anterior cervical disc replacement (ACDR).
Methods
A retrospective review of patients undergoing ACDR or Hybrid surgery (HS) at a single center was performed. Patients diagnosed as C3-7 single- or multi-level cervical disc degenerative diseases (CDDD) with more than 2 years of follow-up and complete pre- and postoperative radiological imaging were included. An ML-based algorithm was developed to predict moderate-severe ABL based on perioperative demographic, clinical, and radiographic parameters. Model performance was evaluated in terms of discrimination and overall performance.
Results
A total of 339 ACDR segments were included (61.65% female, mean age 45.65 ± 8.03 years). During a follow-up period of 45.65 ± 8.03 months, 103 (30.38%) segments developed moderate-severe ABL. The model demonstrated good discrimination and overall performance according to precision (moderate-severe ABL: 0.71 ± 0.07, none-mild ABL: 0.73 ± 0.08), recall (moderate-severe ABL: 0.69 ± 0.08, none-mild ABL: 0.75 ± 0.07), F1-score (moderate-severe ABL: 0.70 ± 0.08, none-mild ABL: 0.74 ± 0.07), and area under the curve (AUC) (0.74 ± 0.10). The most important predictive features were higher height change, higher post-segmental angle, and longer operation time.
Conclusions
Utilizing a ML approach, this study successfully identified risk factors and accurately predicted the development of moderate-severe ABL following ACDR, demonstrating robust discrimination and overall performance. By overcoming the limitations of traditional statistical methods, ML can enhance discovery, clinical decision-making, and intraoperative techniques.
Keywords
Introduction
Anterior cervical disc replacement (ACDR) has received much attention in recent years as an effective surgical treatment for cervical disc degenerative diseases (CDDD). 1 Its objective is to preserve motion in the surgical segment, thereby reducing the occurrence of adjacent segment disease (ASD). 2
Although ACDR is widely performed, it presents certain implant-related complications, including heterotopic ossification (HO), implant migration, and implant subsidence. 3 In contrast to the excessive bone formation characteristic of HO, anterior bone loss (ABL) has emerged as a notable concern in recent years after ACDR. ABL is the process of bone remodeling in the ventral part of vertebral bodies and can typically be recognized from lateral radiographs. 4 Heo et al. 5 reported that the incidence of ABL after ACDR is 60.4%. Kieser et al. 4 observed that 57.1% of patients treated with ACDR developed ABL, with the majority of cases being mild. However, severe ABL occurs in approximately 3.0% of patients. Several studies have reported the risk factors of ABL. Kieser et al. 6 found no association between age, sex, postoperative alignment, or range of motion (ROM) and ABL. In contrast, Wu et al. 7 observed significant correlations between ABL and younger age. Additionally, some researchers reported that the stress-shielding effect caused by insufficient prosthetic coverage of the endplate could be one of the factors of bone loss.8,9 Currently, there is debate over whether ABL should be considered a complication. Some researchers are prone to regard it as a common phenomenon because of its nonsignificant clinical or radiological effects in most patients. However, moderate and severe ABL were observed to be associated with persistent pain, segmental kyphosis, HO, and implant subsidence. 10 Therefore, early identification of risk factors for moderate-severe ABL is crucial to prevent these.
To date, there remains a paucity of studies using machine learning (ML) to predict ABL after ACDR. The objective of the present study was to identify risk factors associated with moderate-severe ABL by examining comprehensive demographics, various imaging parameters, and surgical characteristics. This was achieved through the development and validation of a novel ML algorithm. The findings of this study may guide clinical decision-making and further demonstrate the value of ML in the field of spine surgery.
Methods
Study Design and Patient Population
This retrospective study included patients who underwent ACDR or Hybrid surgery (HS) at a single medical institution, with a minimum follow-up period of 2 years. HS consisted of ACDR and Anterior cervical discectomy and fusion (ACDF). All procedures were performed by the same experienced surgeon between January 2009 and January 2020. Patients were included if they were diagnosed with C3-7 single- or multi-level CDDD causing symptomatic radiculopathy or myelopathy and were refractory to conservative treatment for at least 6 weeks. Additionally, complete perioperative radiographic data were accessible for review. The exclusion criteria included: (1) instability, irreducible kyphosis, or severe degeneration at the surgical segment; (2) patients diagnosed as non-degenerative cervical spine diseases; (3) osteoporosis ((T-score ≤ −2.5)). Eligible patients underwent additional evaluation to document demographic details and radiological metrics. ABL was evaluated using postoperative lateral radiographs obtained at final follow-up radiographs according to the Kieser’s methods. 4
Surgical Techniques
ACDR
All operations were performed by the same senior spine surgeon. The patient was placed with the neck in a neutral position after general anesthesia, and a right-side Smith-Robinson approach was performed at the index level. After exposure, the anterior longitudinal ligament, intervertebral disc, posterior longitudinal ligament and osteophytes were removed to achieve a complete discectomy and decompression. A high-speed burr was used to manage anterior osteophytes, whereby the posterior osteophytes were removed using a rongeur and a curette. The high-speed burr was used to carefully prepare the endplate and a trial implant was used to determine the size of prosthesis. Then, a rail cutter guide and bit were used to drill the fixation channels in the endplate and a correctly sized disc was inserted into the prepared intervertebral space. After verification of the proper placement of implant through anterior-posterior and lateral fluoroscopy, copious irrigation with normal saline was used to wash away the bone dust during endplate preparation in every case. The same procedure was performed at other level in patients with multilevel segmental lesions.
ACDF
All procedures were performed by a single surgeon with a standard right-side Smith-Robinson approach to reveal the surgical segment. The normal anatomy was carefully preserved and identified in preparation for the next step. Complete discectomy was conducted at the indicated levels by removing the disk tissue, posterior longitudinal ligament, and osteophytes to achieve thorough decompression. A high-speed burr was used to prepare the endplates, and a properly sized Zero-P implant (Synthes, Oberdorf, Switzerland) filled with a composite synthetic bone graft (beta-tricalcium phosphate, ChronOS; DePuy Synthes, Paoli, CA, USA) was inserted into the indicated levels. Proper placement of the implants was verified by C-arm fluoroscopy. Finally, the muscle was closed with sutures, and the subcutaneous tissue and skin were then sutured layer by layer after drainage insertion.
Outcome and Candidate Predictive Features
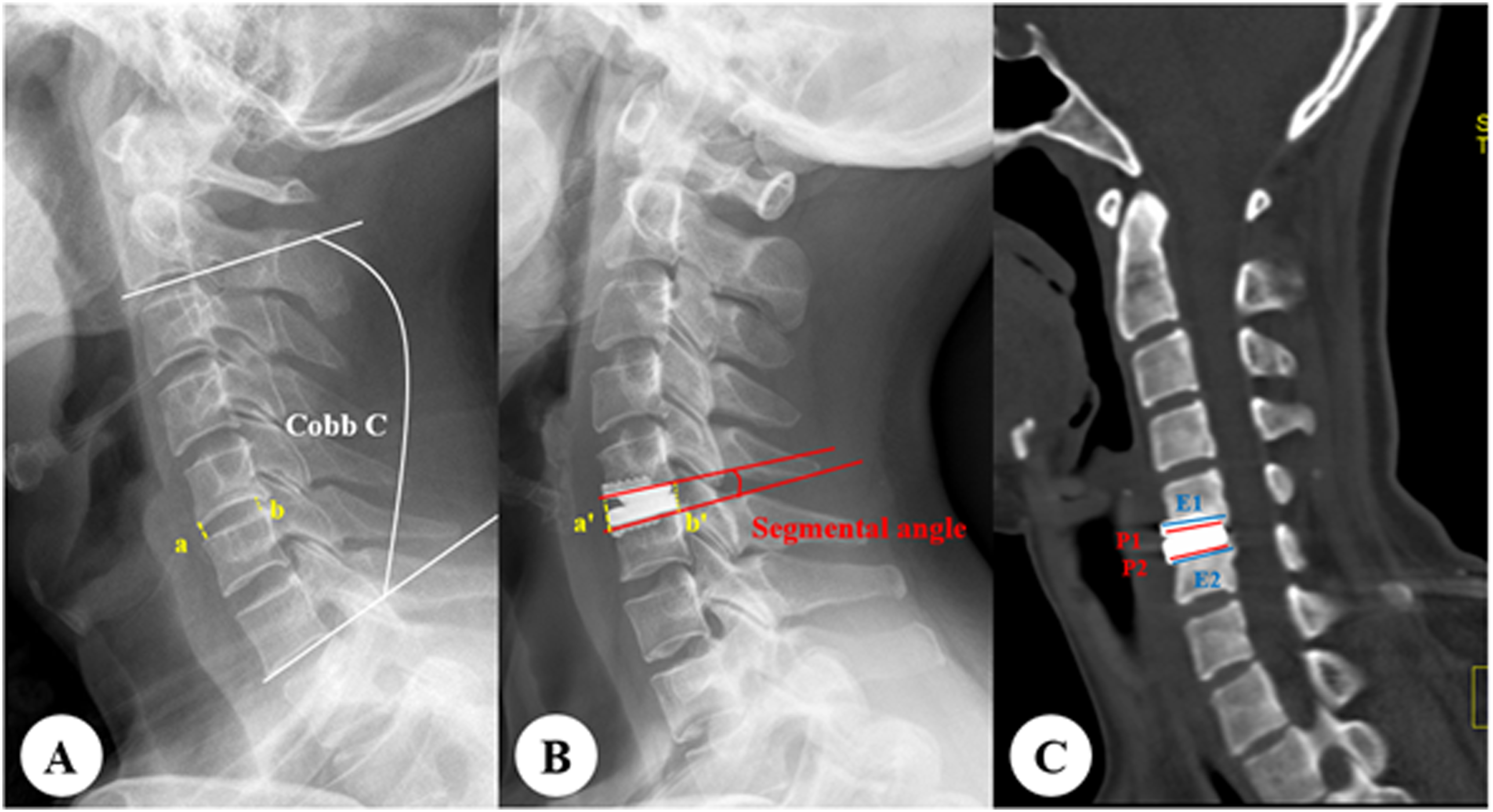
The primary outcome was development of moderate-severe ABL following ACDR. ABL was graded based on the Kieser’s criteria and classified into three grades (Figure 1; Table1). Distinguishing between the no ABL and mild ABL was challenging due to measurement error. Additionally, patients with moderate and severe ABL exhibited similar clinical presentations. Therefore, patients with none and mild ABL were combined into the none-mild ABL group, while those with moderate and severe ABL were grouped together as moderate-severe ABL. Analyzed variables included demographic factors (age, gender, BMI, bone mass density [BMD], smoking status, alcohol history, follow-up time, calcium [Ca], phosphorus [P], alkaline phosphatase [ALP], total protein [TP], albumin [Alb], hemoglobin [Hb], hypertension, diabetes, coronary artery disease [CAD], stroke, hyperlipidemia, spine surgical history, american society of anesthesiologists [ASA]), operative characteristics (surgery level, multilevel surgery, HS, post-operative use of NSAIDs, operation time, blood loss, prosthesis type, prosthesis-endplate depth ratio, post-operative change of intervertebral disc height), and imaging parameters (preoperative ossification, preoperative fatty infiltration, preoperative and postoperative: cervical lordosis [Cobb C], C2-7 range of motion [CobbC ROM], segmental angle, ROM at index level [Segmental ROM]). Preoperative ossifications were evaluated in lateral X-rays according to the following criteria: (1) ossification of anterior and/or posterior longitudinal ligament; (2) preoperative bubble osteophytes; (3) ROM-limiting osteophytes; and (4) ligamentum nuchae ossification. Disc height was measured at the lateral radiograph before and after surgery
11
(Figure 2). The prosthesis-endplate depth ratio was calculated on the median sagittal plane of reconstruction computed tomography (CT) as dividing the length of the prosthesis by the immediate post-operative length of the endplate. Cervical lordosis was the angle formed between the inferior endplate of C2 vertebra and the inferior endplate of C7 vertebra. Cobb ROM and segmental ROM were measured on the flexion and extension radiographs using the Cobb method. Segmental angle was defined as the angle drawn from the superior and inferior endplate of the prosthesis (Figure 2). The Goutallier classification of cervical paraspinal muscles (CPM) was assessed using a 0-4 scale, which involved a qualitative evaluation of fat atrophy in the muscle multifidus. All measurements were conducted on an axial T2 weight section from MRI, at the C5/6 level as a representative, which was a common practice in CPM studies.
12
All imaging outcomes were analyzed by two independent reviewers (both of them with junior titles) independently. For qualitative data, if there was a disagreement between two reviewers, the issue was referred to a third, more experienced surgeon for resolution. For angle-related measurements, if the difference between two reviewers was less than one degree, the average of their measurements was used as the final result. If the difference exceeded one degree, the measurement was repeated until the error meets the standard. For disc height measurements, the threshold was one millimeter. Importantly, for variables with less than 30% missing data, imputation of both categorical and continuous variables was performed using the k-nearest neighbors strategies. Variables with more than 30% missing data were excluded from the analysis. Anterior bone loss was calculated as (a-b)/a in the lateral X-ray. The a was defined as the endplate length at immediate postoperative, while b was defined as the endplate length at last follow-up. Classification for ABL After ACDR. Measurement of radiological parameters. (A, B) Post-operative change of intervertebral disc height is calculated as (a'+ b')/2 − (a + b)/2. (C) Prosthesis-endplate depth ratio is calculated as (P1/E1 + P2/E2)/2.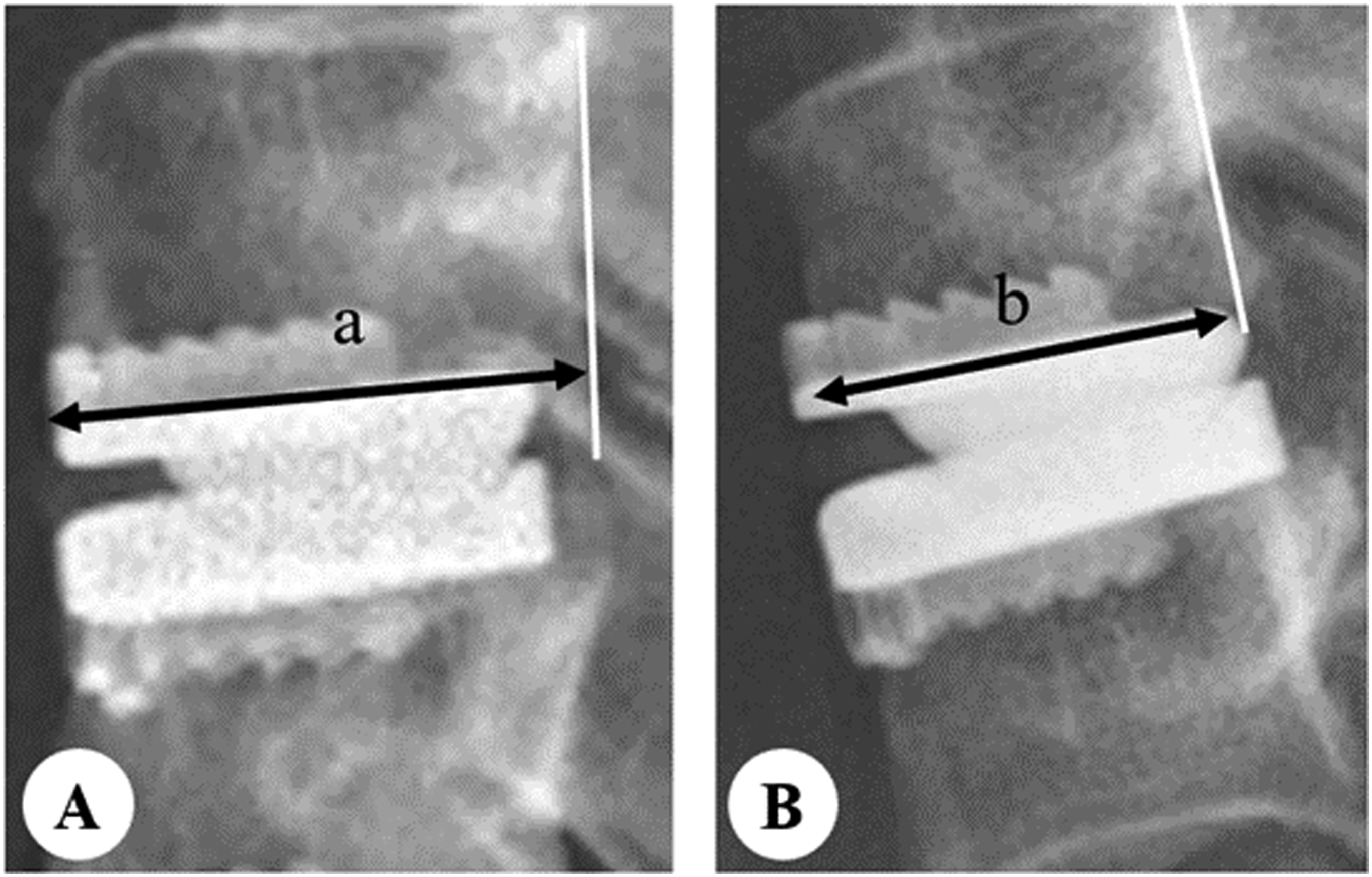

Statistical Analyses and Multivariable Predictive Modeling
Demographic, clinical, and imaging information was analyzed using R (RStudio, PBC, Boston, MA). Differences between none-mild ABL group and moderate-severe ABL groups were assessed via chi-square and t test for categorical and continuous variables, respectively. All data are depicted as frequencies and percentages for categorical variables, and as mean ± standard deviation for continuous variables. Statistical significance was set at P < 0.050.
Programming for ML model development was performed using Python version 3.10.9 (Python Software Foundation, Wilmington, DE). Four ML algorithms—Balanced Random Forest (BRF), Extreme Gradient Boost, Elastic-Net Penalized Logistic Regression, and Support Vector Machine—were employed. These selections were made based on their frequent appearance in literature, their capacity to handle imbalanced data through calibration, and their innate ability to rank features by predictive importance. Patients were divided into training (80%) and testing (20%) groups randomly. The training group was used to develop the model, allowing for the identification of the optimal predictive algorithm from the available data. Subsequently, this algorithm was applied to the testing group to validate the model’s predictive accuracy. The target variable’s classification was imbalanced, so we employed Borderline Synthetic Minority Oversampling Technique to oversample the minority class and improve model training. 13 For the BRF algorithm, data normalization is unnecessary; however, we standardized data in other models to prevent the scale from impacting the results. The model’s performance was assessed using discrimination metrics such as precision, recall, and F1-score. Additionally, the overall performance of the model was further assessed using the area under the curve (AUC) of the receiver operating characteristic (ROC) curve. The feature importance scores from the highest-performing model were analyzed. To ensure reliable performance estimation despite inherent randomness in data partitioning, model training, and optimization, the analysis pipeline was iterated 50 times using 50 random seeds for reproducibility. Additionally, 95% confidence intervals were calculated for both the AUC and feature importance estimates.
Results
Baseline Demographic Characteristics.
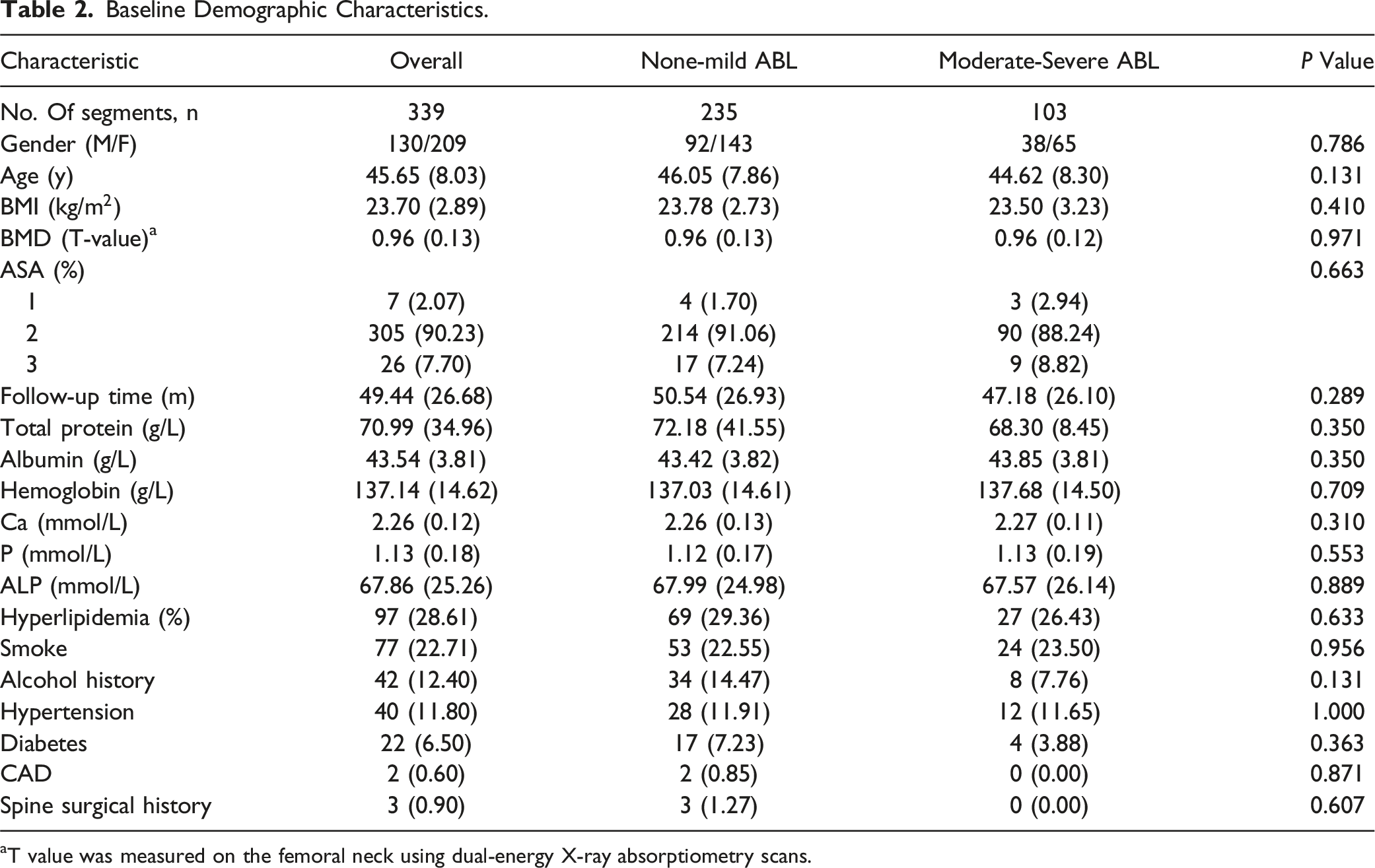
aT value was measured on the femoral neck using dual-energy X-ray absorptiometry scans.
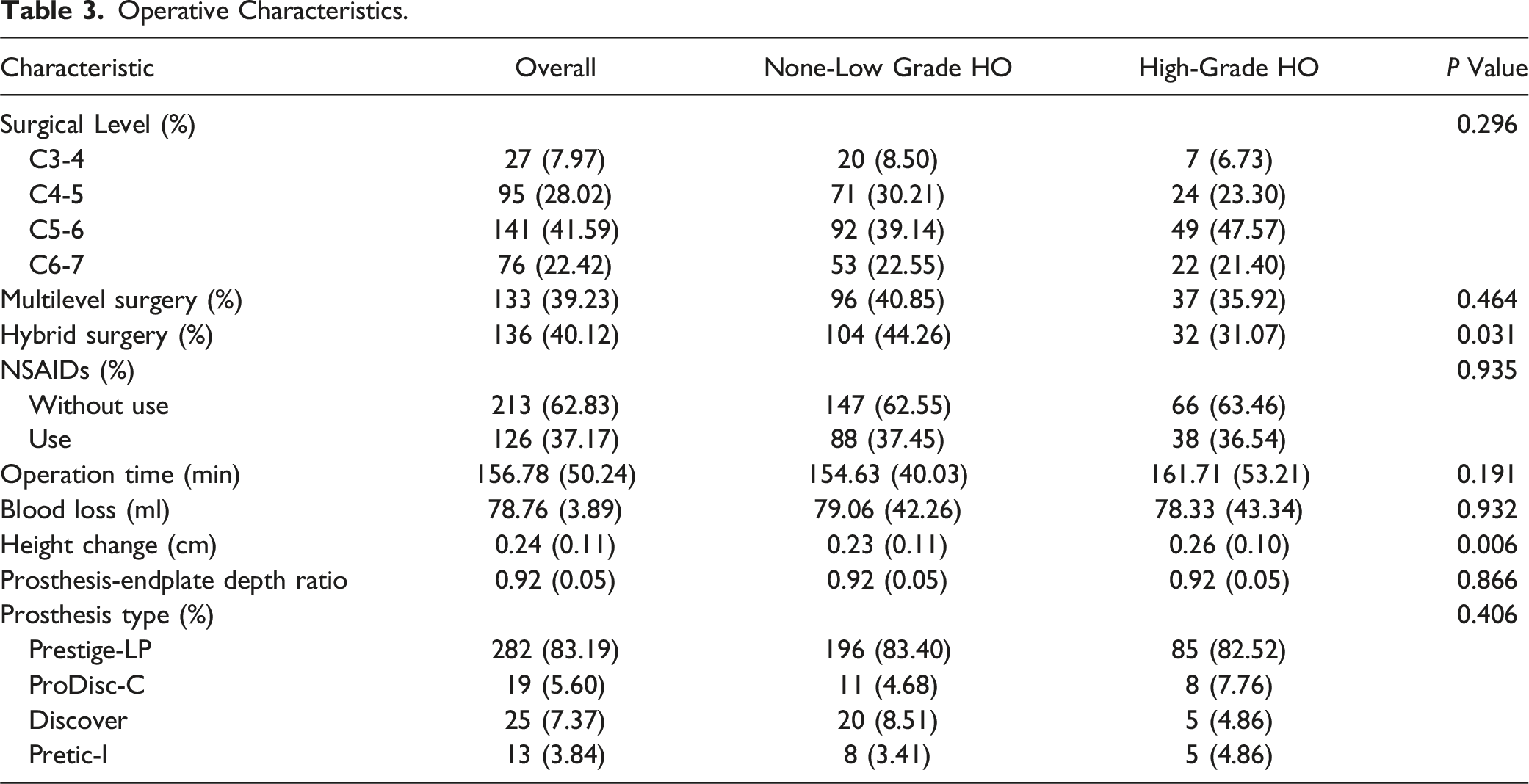
Operative Characteristics.
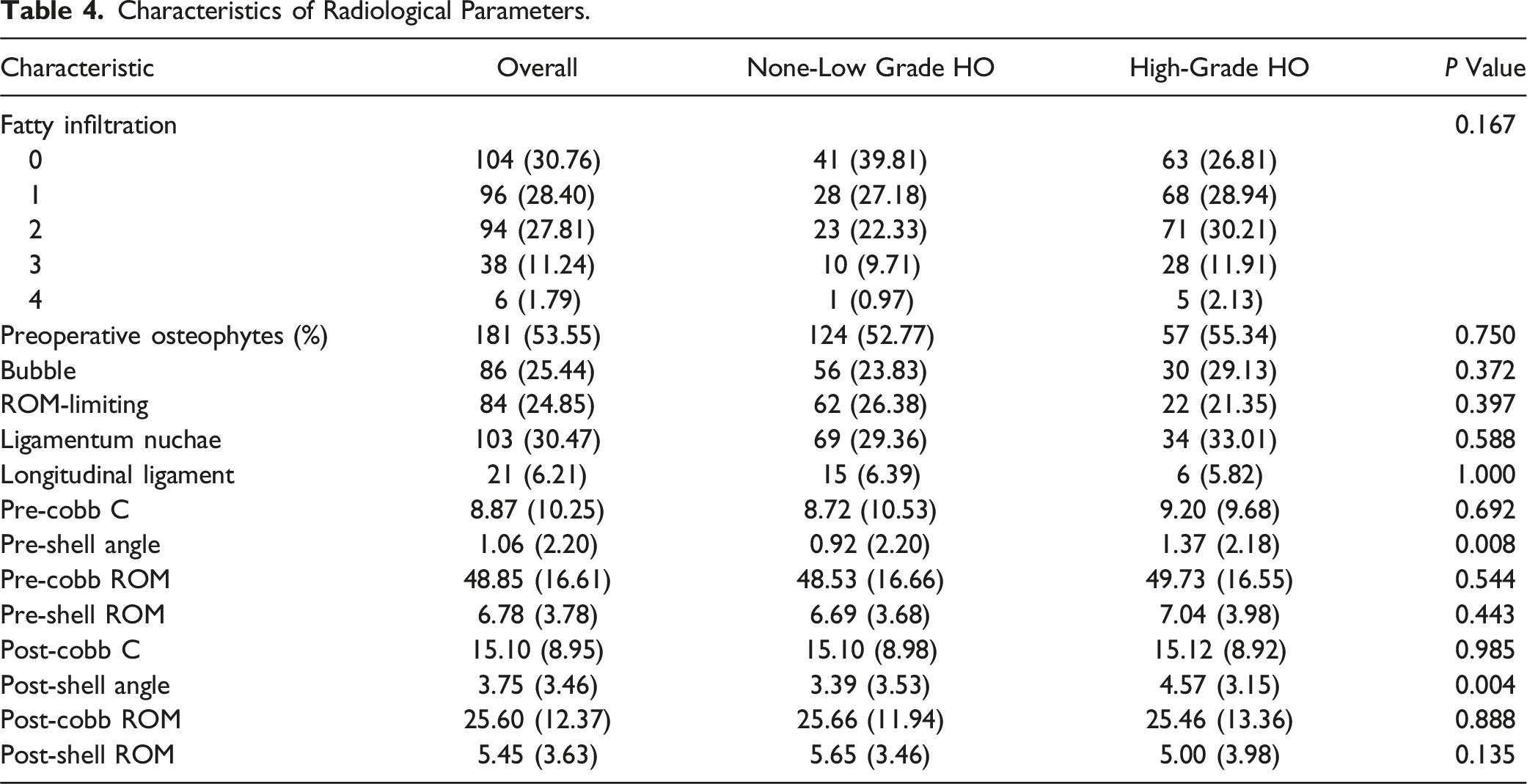
Characteristics of Radiological Parameters.
Model Performance and Feature Importance
Performance of Machine Learning Models.

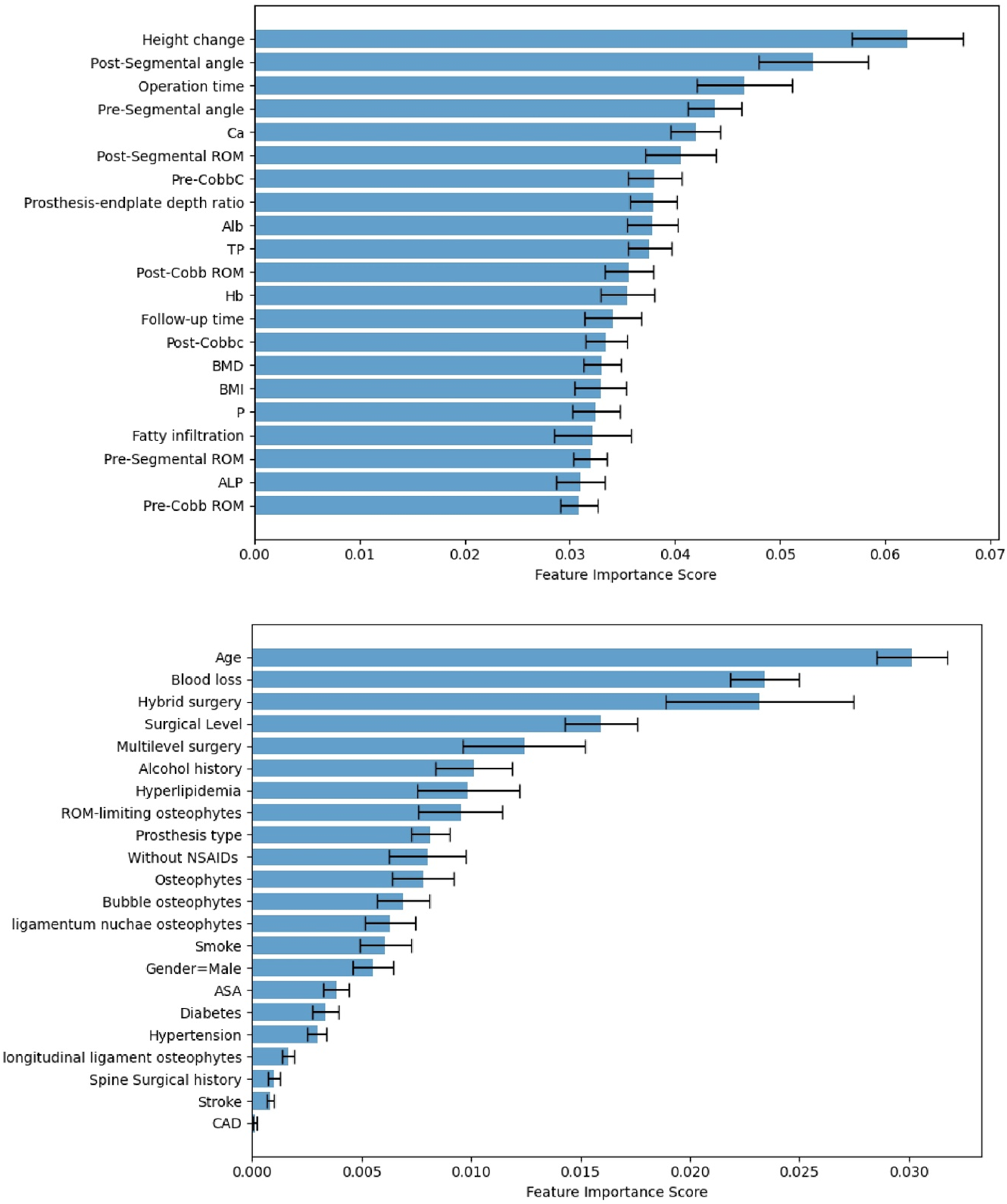
Feature importance measured according to usefulness within the model for predicting development of Moderate-Severe ABL.
Discussion
Although ACDR is widely performed and patients have benefited because of its satisfactory results, it has some implant-related complications. In contrast to excessive bone formation (ie, HO), ABL is another implant-related condition after ACDR and has garnered more attention in recent years. 10 Although several studies have reported the clinical characteristics of ABL and considered its pathogenic mechanism, these are easily disregarded in ACDR. Compared with mild ABL, moderate-severe ABL has been proven to influence implant subsidence, segmental kyphosis, and local pain.5,14,15 Timely recognition of influencing factors is important during perioperative period. ML algorithms are increasingly used to predict postoperative outcomes for patients because they can perform complex calculations encompassing various patient-specific factors. However, thus far, no study has attempted to comprehensively study the formation of ABL after ACDR using a complete set of patient-specific factors. We aimed to develop and validate a ML model to predict moderate-severe ABL after ACDR.
In our analyses, the BRF algorithm was the highest-performing model for prediction. This may be attributed to its unique advantages over other models in handling imbalanced and relatively small sample data. 16 Feature importance analyses indicate that the formation of moderate-severe ABL is driven by a comprehensive range of patient-specific factors, with surgical-related factors playing a major role. Height change, post-segmental angle, and operation time were identified as the most relevant predictive features. Calcium test also contributed to the model prediction. Interestingly, age, gender, and comorbidities were less important. It is worth mentioning that although the statistical difference was observed in univariate analysis, HS had little influence on the ML model.
As an extension of Wolff’s law, Frost 17 ’s theory of bone physiology posits that bone tissue can adjust its strength through remodeling mechanisms to accommodate the magnitude of mechanical loads applied to it. Chen et al. 18 suggested that a larger angle in the segmental angle may be a risk factor for developing ABL after ACDR. The larger angle implies that more loading force or stress is shifted to the posterior aspect of the vertebral body. Meanwhile, the anterior aspect of the vertebral body sustains less loading force or stress. This has been proven by infinite analysis of pressure distribution in the bone-implant interface. 19 In this study, the moderate-severe ABL group exhibited higher segmental angles preoperatively and postoperatively, which have led to a decrease in stress at the anterior aspect. Additionally, a higher change in intervertebral height was observed in this group. We believe that it primarily stems from the attempt to restore the physiological curvature of the cervical spine. However, when the change in intervertebral height is greater than it should be, the stress distribution will be closer to the posterior aspect, subsequently causing a more obvious bone resorption anteriorly. Interestingly, contrary to our expectations, the prosthesis-endplate depth ratio did not play a significant role as it does for HO. 20 It may be because endplate coverage cannot significantly change stress transmission as it does other factors. However, further biomechanical studies are required to confirm this. Unexpectedly, operation time constituted the third most important feature for prediction. Previous studies did not yield similar findings.6,7,18 Given that previous studies often used logistic regression as a multivariable model, variables that did not reach significance were rarely included in subsequent analyses. The meaning behind this variable may have been overlooked. We hypothesize that prolonged surgical duration may be associated with more intraoperative procedures, leading to increased damage to the vertebral body, thus contributing to the occurrence of ABL. Additionally, a prolonged time may indicate that the insertion and adjustment of the prosthesis may be challenging, and the imperfect fit between the prosthesis and the endplate can lead to uneven stress distribution. 21 Kieser et al. 6 found that multilevel surgery presented an increased risk of any and severe ABL (P = 0.013). They speculated that the occurrence of severe ABL may be associated with ischemic necrosis of the vertebral endplate caused by vascular damage. However, there was no difference in our model.
Numerous studies have sought to characterize the risk of developing ABL after ACDR according to demographic characteristics.6,7,22 Some studies discovered that younger age was an independent influencing factor for ABL. 7 They believed that this phenomenon may be attributed to more active bone metabolism in younger patients. In our study, although moderate-severe ABL seemed to occur in young patients, it did not meet the criteria. We speculate that the relatively long follow-up period may have attenuated its impact. Bone remodeling is a process that lasts a long time. After surgery, there is a changed biomechanical environment for the vertebral body to adapt. ABL is a dynamic reconstruction process that indicates a changed biomechanical environment. As the duration of follow-up increases, this process tends toward stability. Prior research 8 revealed that the majority of cases of ABL after ACDR occurred in 3 months, and were confined within 1 year. Therefore, in our study, which spanned over 2 years, the absence of differences in bone metabolism indicators and age is considered acceptable. Although most osteogenic-related factors exhibit no correlation with moderate-severe ABL, it is worth noting that the relatively prominent position of calcium in the ML model may serve as a clue to this due to the special logic of BRF. Essentially, BRF is a forest composed of multiple decision trees. In these trees, the branches closer to the trunk contribute more to the model, and their order of consideration during decision-making is prioritized, with subsequent parameters being further divided based on the preceding ones. 16 Considering the previous debates, this model prompts us to consider whether the role of individual metabolic capacity in ABL formation requires preconditions such as a discernably changed mechanical environment. Additionally, Wu et al. 7 suggested that BMI may influence the occurrence of aseptic loosening of implants by affecting the stress on bone tissue, which has also been reported in total hip arthroplasty. 23 However, because the neck is not the primary weight-bearing unit of the body, its influence on vertebral segment stress may be minimal. Notably, at the research design stage, we speculated that muscle quality may be related to ABL. When the CPM is atrophied, its function as a stabilizer in an abnormal mechanical environment becomes challenging. 24 Although fatty infiltration condition appeared worse in the moderate-severe ABL group, it did not exhibit a discernible effect.
Outcome prediction remains constrained by traditional statistical methods using univariate and multivariate analyses, as demonstrated by considerable heterogeneity in the results of previously reported studies. Sophisticated ML-based predictive modeling methods can enhance analysis and patient identification, thereby advancing clinical practice. Previous studies often focused on a specific view in attempting to explain phenomenon occurrence with a single variable of difference. However, according to the results of this study, moderate-severe ABL is influenced by multiple factors, with intraoperative manipulations affecting postoperative mechanical balance predominantly. Compared with other uncontrollable factors, we can invest more research in this area to reduce such incidents.
Our study is subject to the limitations of any retrospective study. Moreover, considering that this study used data from a single academic institution, we recognize that the small size of our cohort, together with the decision to exclude patients without sufficient follow-up time, may have introduced a degree of selection bias, which restricted the generalizability of the model. Additionally, considering the data imbalance and the relevant small sample data, the prediction of related complications would be more appropriately studied in a multicenter study. Nonetheless, this study focusing on global imaging and clinical phenotypes is the first in the field to address moderate-severe ABL in ACDR via ML analytics and offers a unique perspective on predictive modeling for these patients, providing credence to new lines of future research.
Conclusion
Using preoperative demographics, comorbidities, and perioperative imaging parameters, a model was developed using ML techniques to predict development of moderate-severe ABL following ACDR. With good discrimination and overall performance, the predictive model identified higher height change, higher post-segmental angle, and longer operation time as the most important features, indicating that the presence of these findings contributes to greater risk for moderate-severe ABL. The findings of this study demonstrate the predictive value of ML and serve to validate its implementation, as well as that of artificial intelligence more broadly, to guide clinical decision-making and intraoperative techniques.
Footnotes
Acknowledgements
We are very grateful to those who helped in the study process.
Authors’ Contributions
RZ conducted the design of the study and drafted the manuscript with the help from CG and JBH. TKW and CG helped in the statistical analysis. RZ, CG, and JBH conducted the interpretation of data. TKW and HL contributed to the revision. The authors have read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Provincial Science and Technology Plan Project Special Fund Transfer Payment Project (2021-YF08-00113-GX), National Natural Science Foundation of China (82302785), and the 1.3.5 project for Postdoctoral Foundation of West China Hospital of Sichuan University (2023HXBH080).
Ethical Statement
Data Availability Statement
Datasets are available from the corresponding author on reasonable request.