
Abstract
Study design
Retrospective Cohort Study.
Objectives
Low bone mineral density (BMD) is a known risk factor for revision surgery in patients with adult spinal deformity (ASD). Hounsfield units (HUs) on CT scans have been suggested as a proxy for assessing BMD. This study aimed to determine HUs in the lumbar region and their association with mechanical failure in patients undergoing ASD surgery.
Methods
We included ASD patients undergoing surgery from 2010-2020 with minimum 2-year follow-up. We excluded patients without preoperative CT scans, or a CT scan more than 1 year before surgery. Mechanical failure was defined as proximal junctional failure, pseudarthrosis, or implant failure requiring revision surgery. On preoperative CT scans, HUs were measured on 3 axial slices on each vertebra from L1-L5 and, if available, at UIV and UIV + 1.
Results
We included 170 patients, mean age 63 (±12) years, with 108 (64%) females, and 13 [IQR 10-16] instrumented levels. Mechanical failure occurred in 27% (n = 46) of patients at 2-year follow-up. Mean lumbar HUs were 146 (±51) in the mechanical failure group and 135 (±52) in those without revision (P = .232). Area under the curve was 0.58 (95% CI: 0.48-0.68), corresponding to no to low discriminatory power in predicting mechanical failure using lumbar HUs. Univariate logistic regression revealed no significant difference between mechanical failure and lumbar HUs (OR = 1.00, 95% CI: 1.00-1.01, P = .239).
Conclusions
We found no association between mechanical failure and HUs on preoperative CT scans in ASD patients. Thus, we cannot recommend using HUs to predict mechanical failure in these patients.
Introduction
The risk of revision surgery following adult spinal deformity (ASD) surgery is up to 30%.1-3 The reasons for revision surgery include postoperative pseudarthrosis, wound infection, vertebral fracture of the upper instrumented vertebrae (UIV) leading to proximal junctional failure (PJF), and implant failure, such as rod-breakage and screw loosening.3-5 Despite the substantial risk associated with surgery, surgical treatment remains the preferred approach for treating ASD patients when conservative measures prove ineffective. 5 Low bone mineral density (BMD) is a known risk factor for revision surgery in ASD patients.6-8 Studies show a 2-fold higher risk of revision surgery in osteoporotic and osteopenic ASD patients compared to those with normal BMD.6-8 The gold standard for measuring BMD is dual-energy X-ray absorptiometry (DEXA) scans, which calculate bone absorption of radiation at the distal radius, hip, and spine. However, patients with ASD frequently display features such as spondylosis, pathological sclerosis, spinal rotation, and a history of previous instrumentation.9-12 These factors often lead to an overestimation of spinal BMD.9-12 Likely, DEXA-measured BMD may not align with actual BMD in the spine. Consequently, the utilization of Hounsfield units (HUs) on CT scans has been suggested as a proxy for assessing BMD.13,14 Schreiber et al identified HUs as an important clinical tool in predicting the stability of orthopedic implants. 13 Several studies suggest an association between PJF and low HUs measured at UIV or UIV ± 4.15-18 Interestingly, there has been limited focus on HUs in the lumbar region and its association with mechanical failure in ASD patients, despite this region’s susceptibility to rod breakages and screw loosening/breakage.
Our study aimed to evaluate HUs in the lumbar region and their association with mechanical failure in patients undergoing ASD surgery, with a minimum of 2-year follow-up.
Materials and Methods
To assess mechanical failure following ASD surgery, we conducted a retrospective cohort study at a single quaternary spine center. Project approval was granted by the National Health and Medical Authority and The National Data Protection Agency (30 Nov. 2018 R-21054762; 21 Oct. 2021 P-2021-777). The present study adhered to the STROBE guidelines. 19 We defined ASD surgery as all adult patients undergoing surgery for a sagittal deformity with an instrumented fusion of ≥5 vertebral levels to the sacrum/pelvis. This was done to ensure a more homogenous patient cohort with sagittal malalignment and the need for restoration of the sagittal profile.
Subjects
We included patients undergoing ASD surgery from January 1, 2010, to September 1, 2020, with a minimum of 2-year follow-up. We excluded patients without a preoperative CT scan, or a CT scan made more than 1 year before surgery. A standardized follow-up protocol was applied for all patients, including radiographic examination preoperatively, immediate postoperatively, and in-hospital clinical controls (3 months, 1 year, 2 years). In cases where mechanical failure was suspected, additional clinical assessments, including X-ray and CT scans, were conducted. Patient demographics, accessed through electronic medical journals, included history of previous spine surgery, comorbidities, current surgical procedure, length of stay (LOS), revision surgery, smoking status, body mass index and osteoporosis. Osteoporosis was defined as a T-score <−2.5 using DEXA scans.
Mechanical Failure
The primary outcome was revision surgery exclusively due to mechanical failure. Mechanical failure was defined as radiologically verified PJF, pseudarthrosis, or implant failure (rod breakage, set-screw dislodgement, screw-breakage, -loosening, or -pullout) requiring revision surgery at 2-year follow-up. Competing events, including death or non-mechanical failures requiring revision surgery, were censored and excluded from further analysis.
Surgical Procedure
Computer-assisted surgical planning was done for all patients using the online imaging system KEOPS (SMAIO). 20 The surgical procedure involved the use of a two-rod system with posterior pedicle instrumentation and CrCo rods. Complete facetectomies were made on instrumented levels alongside decortication at the transverse processes. All patients received locally harvested autologous bone graft in combination with either 1 batch of sterile, deep-frozen, and non-cleaned allogenic bone graft (femoral head) or commercially produced demineralized cortical fibers (DCF). All bone graft material was placed posterolateral in the lumbar region. For patients in need of major surgical correction, either three-column osteotomies (3CO) and/or lumbar interbody fusion cages were used.
Computed Tomography and HUs
On preoperative CT scans (2 mm slice thickness), HUs were obtained using the software system IMPAX Volume Viewing MIP/MPR, version 6.7.1.1506 (AFGA Healthcare, Belgium). The HUs were measured on 3 axial slices on each vertebra from L1 to L5 and, if available, at UIV and UIV + 1, in accordance to the method described by Schreiber et al
13
(Figure 1). In cases of previous instrumented surgery, the HUs were measured on 1 axial slice either above or below the pedicle screw (Figure 1). Illustration of Hounsfield units assessment. Hounsfield units were measured on 3 axial slices from L1 to L5 and, if available, at UIV and UIV + 1 (B–D). In cases of previous instrumented surgery, the Hounsfield units were measured on 1 axial slice either above or below the pedicle screw (A).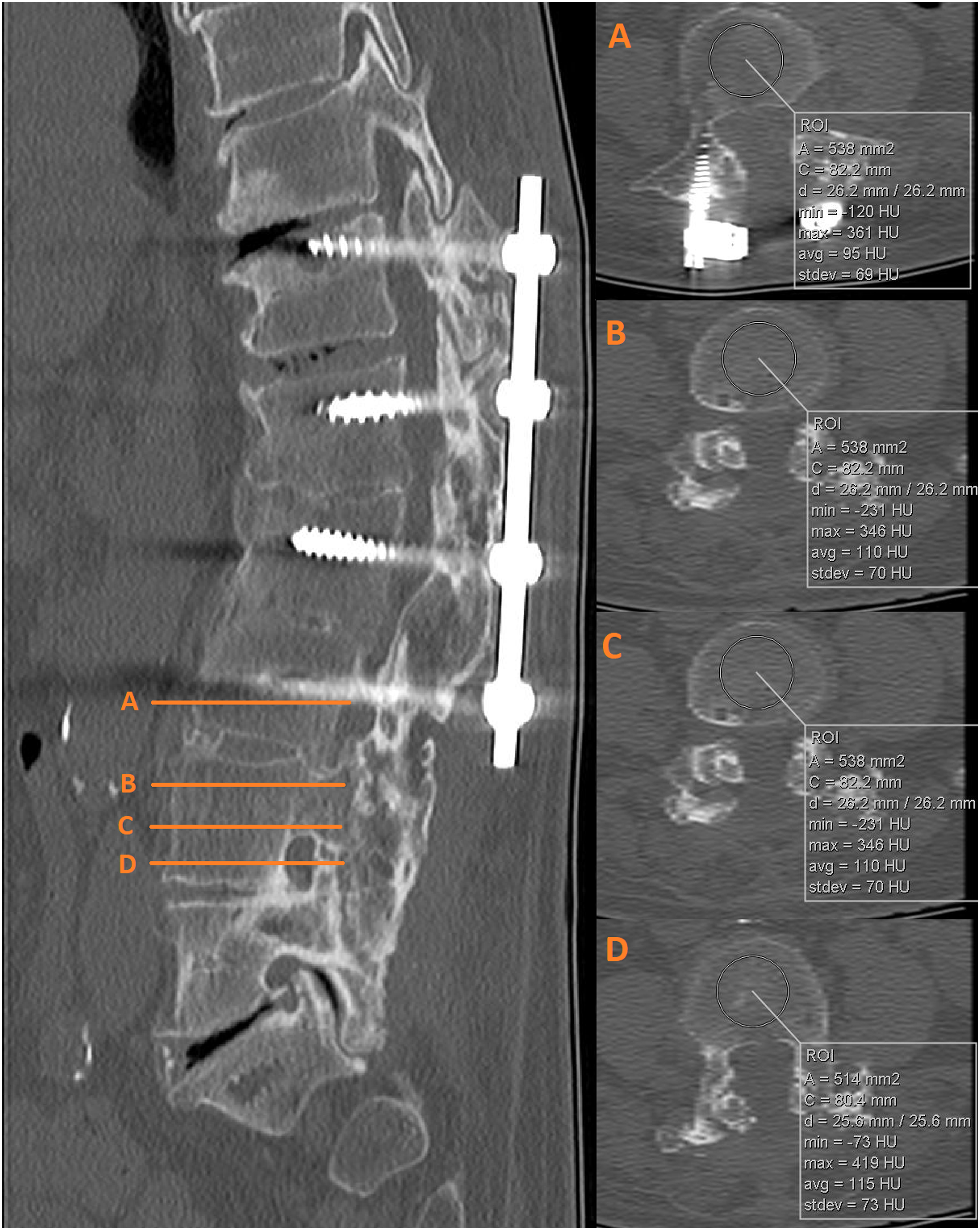
Statistics and Outcome
Statistical analyses were done using R, version 4.2.0 (R Development Core Team, Vienna, Austria, 2020). The distribution of continuous data was evaluated using histograms and Q-Q plots and results were reported as means (±SD), medians [IQR] or proportions (%). Normally distributed continous data were analyzed using a non-paired Student’s t test and Mann Whitney U test were used for non-normally distributed continous data. Pearson’s X 2 test was used for categorical data. The receiver operating characteristics curve was used to determine area under the curve (AUC) evaluating lumbar HUs as a predictive factor for mechanical failure. The diagnostic accuracy for AUC was categorized as follows: no to low discriminatory power (.5-.7), moderate discriminatory power (.7-.9), and high discriminatory power (≥.9). 21 Clinically relevant predictors of mechanical failure were assessed for multicollinearity (variance inflation factor <5) and then analyzed using univariable logistic regression analysis. Backward stepwise regression was applied to select variables used in multivariate regression (P < .3). Results are reported as odds ratios (OR) with 95% confidence interval (CI). We refrained from hypothesis testing within nested subgroups due to small sample sizes. P-values of <.05 were considered statistically significant.
Results
Subjects and Radiographic Parameters
Patient demographics on entire cohort without and with censoring.
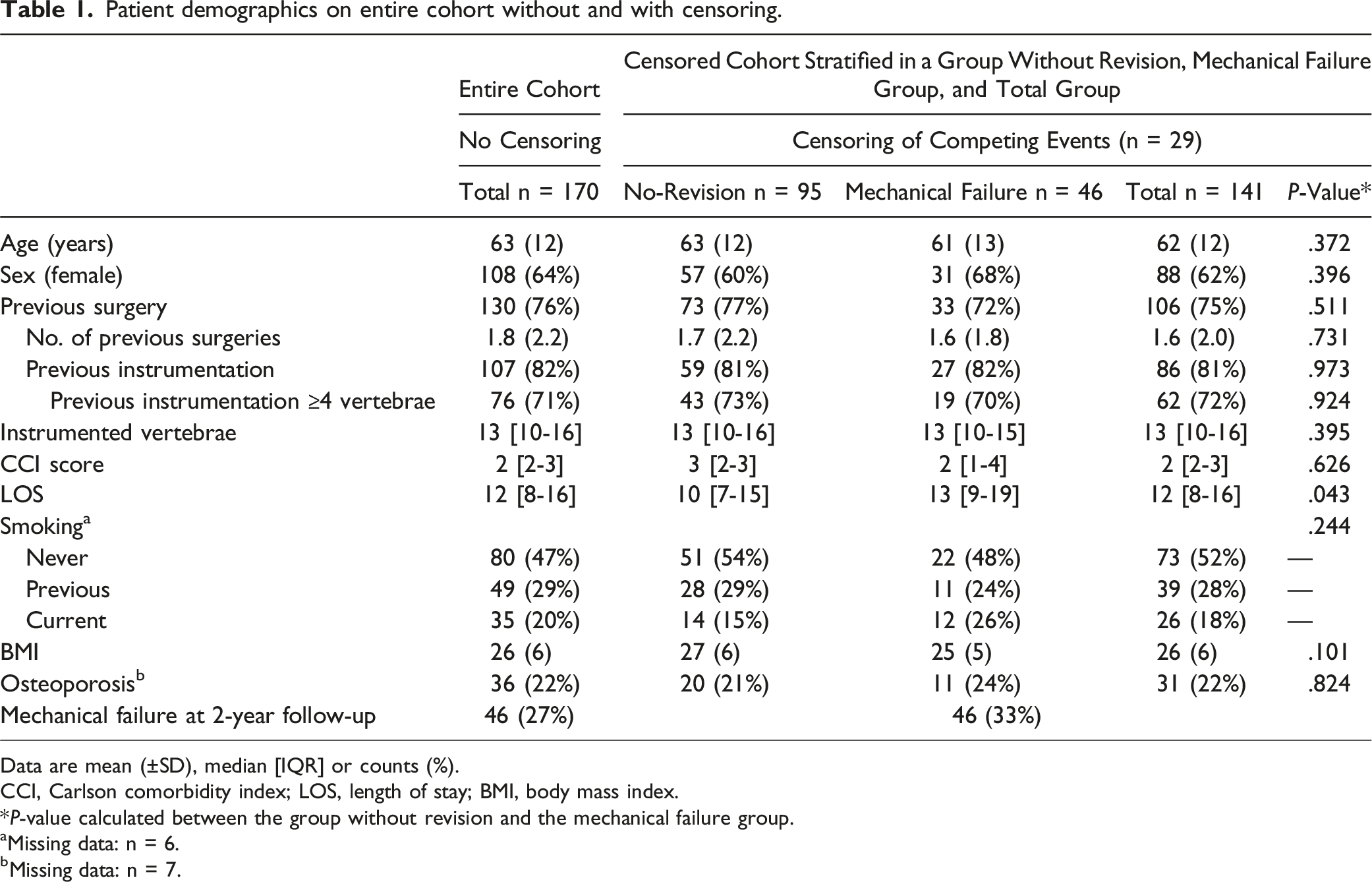
Data are mean (±SD), median [IQR] or counts (%).
CCI, Carlson comorbidity index; LOS, length of stay; BMI, body mass index.
*P-value calculated between the group without revision and the mechanical failure group.
aMissing data: n = 6.
bMissing data: n = 7.
Hounsfield Units and Predictors of Mechanical Failure
Hounsfield units stratified in the group without revision and mechanical failure group.
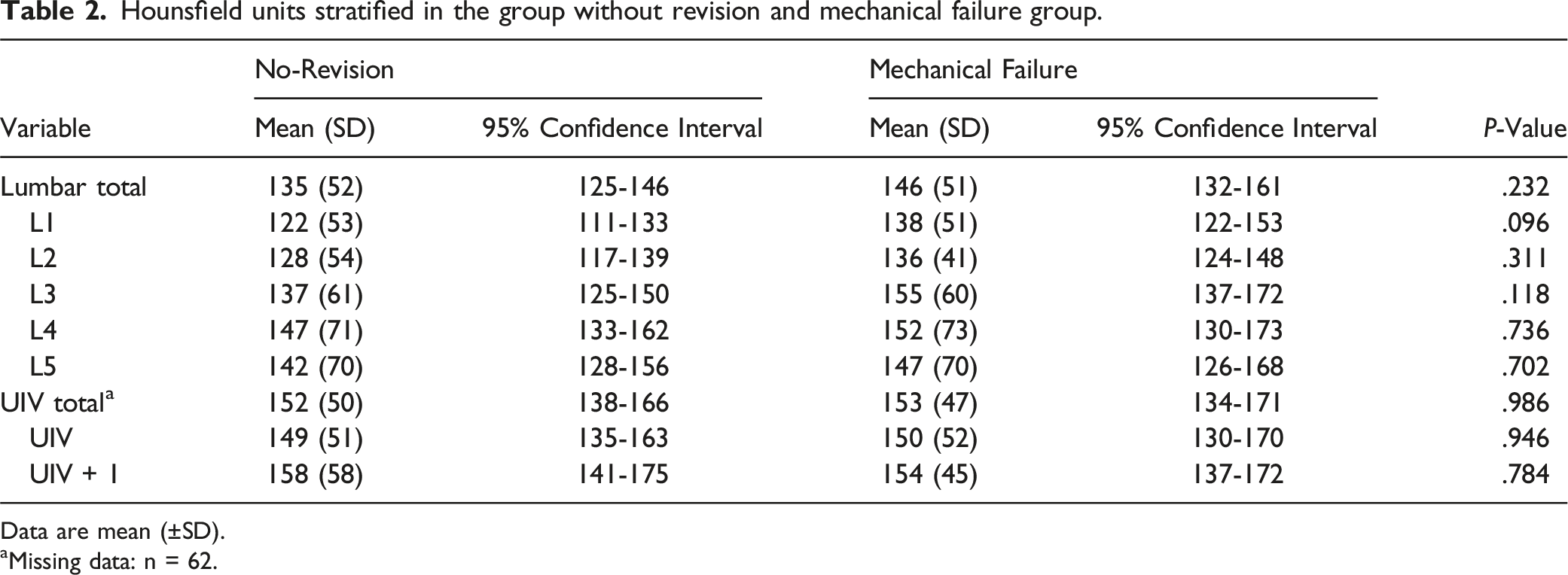
Data are mean (±SD).
aMissing data: n = 62.
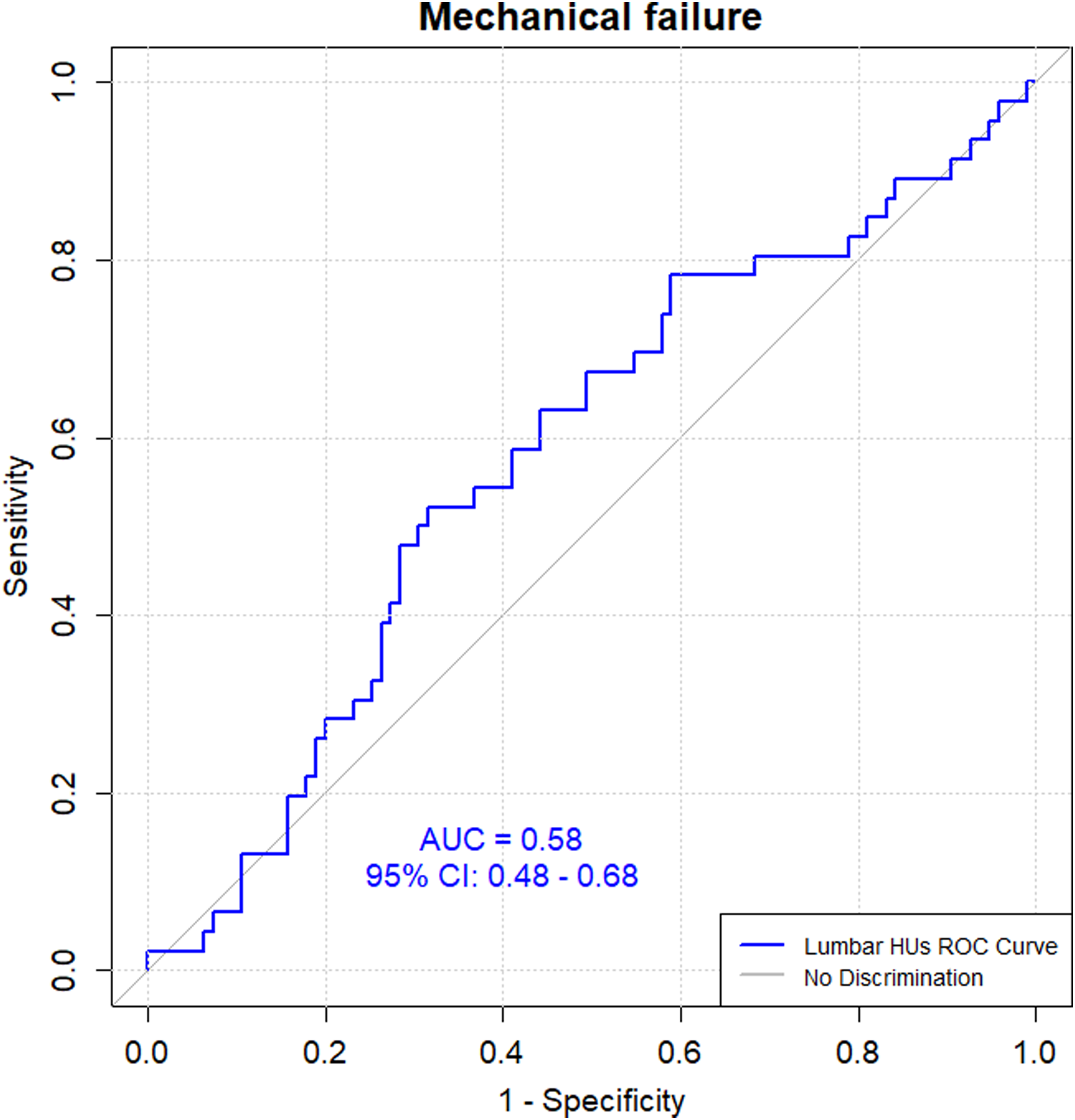
Lumbar Hounsfield units to predict mechanical failure using a receiver operating characteristics curve to determine area under the curve.
Predictors of mechanical failure using logistic regression analysis.
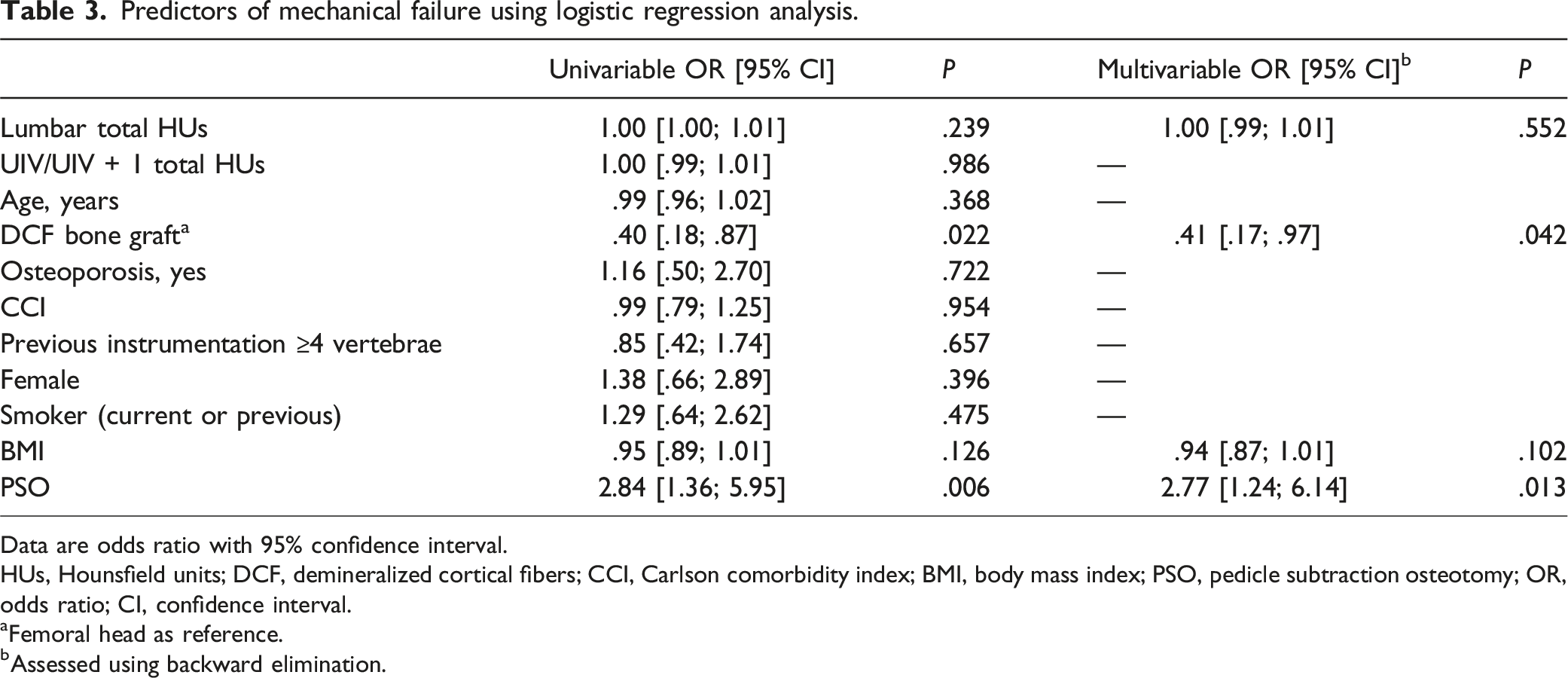
Data are odds ratio with 95% confidence interval.
HUs, Hounsfield units; DCF, demineralized cortical fibers; CCI, Carlson comorbidity index; BMI, body mass index; PSO, pedicle subtraction osteotomy; OR, odds ratio; CI, confidence interval.
aFemoral head as reference.
bAssessed using backward elimination.
Discussion
The present study aimed to investigate the association between lumbar HUs and mechanical failure in ASD patients. Our findings revealed no significant association between preoperative lumbar HUs and the occurrence of mechanical failure at 2-year follow-up.
DEXA vs HUs
The link between DEXA, BMD, and T-scores compared with CT-measured HUs seems to have varying correlations.13,14,22-24 Schreiber et al and Lee et al both found strong correlations between DEXA BMD and lumbar HUs in trauma and low back pain patients, respectively.13,24 Choi et al. found a strong correlation between T-scores and lumbar HUs in non-degenerative spine patients. 14 However, in degenerative spine patients, this correlation was significantly reduced. 14 Kohan et al found a poor correlation between lumbar HUs and femoral neck BMD and lumbar BMD in ASD patients. 22 Likewise, Chanbour et al found a weak correlation between DEXA-measured BMD, T-scores, and UIV HUs in the prediction of proximal junctional kyphosis (PJK), also in ASD patients. 23 Only DEXA-measured BMD was a significant risk factor of PJK. 23 The available data suggests that a good correlation between DEXA scans and CT scans exists only in non-degenerative spinal patients, and sufficient accuracy is lacking in ASD patients, where degeneration, pathological sclerosis, spinal rotation, and previous instrumentation are frequent. Hounsfield units might better represent true BMD in ASD patients. Recent studies have shown excellent intraobserver and interobserver reliability in HUs measurement, with consistent results across various CT scanners, thereby affirming the reliability of utilizing HUs.12,28
Upper Instrumented Vertebrae HUs
Several studies suggest an association between UIV HUs and the occurrence of PJK and PJF in ASD patients.15,16,18 The studies found mean UIV HUs between 138-161 for PJK, 131 for PJF and 162-163 in a control group without revision surgery.15,16,18 These findings are similar to our findings, despite not detecting differences between groups, with UIV HUs being close to 150 in both the mechanical failure group and in the group without revision. Duan et al. found a threshold for UIV HUs of 104 as a predictor of PJK. 16 Since our study did not investigate PJK, conclusions cannot be made in terms of predicting this outcome. Chanbour et al found low UIV HUs as a predictor for PJK but found no association between UIV HUs and implant failure or rod breakages. 15 Clearly, assessing the association between thoracic UIV HUs and a lumbar rod breakage is troublesome. The correlation between HUs in different spinal regions is still to be specified. Our data revealed a small difference in HUs between the UIV and the lumbar region, with the latter consistently exhibiting lower HUs.
Lumbar HUs
The studies that included lumbar HUs found values between 98-173.13,22,24-28 The studies included a range of conditions, including non-spinal trauma, lumbar degenerative diseases, back pain, ASD, variations in osteopenia or osteoporosis status and healthy controls. The inclusion of such diverse patient cohorts prevents direct comparison to our results. To our knowledge, only 2 studies have previously assessed lumbar HUs in ASD patients.22,28 Kohan et al. found a mean of 128 HUs in the lumbar region for primary ASD patients and a poor correlation between lumbar HUs and femoral neck DEXA. 22 The study only included 48 patients, measured lumbar HUs from L1-L4 and only 6% (n = 3) of the patients had osteoporosis. 22 Despite this, our study reported slightly higher lumbar HU in both groups. Kohan et al. concluded that lumbar HUs to assess BMD and thereby osteoporosis in patients undergoing ASD surgery might not be an effective tool. 22 Cho et al. found no statistically significant difference between mean HUs at the osteotomy site (70% of times at L3 or above) between patients having rod breakage (135 HUs) and those without (142 HUs). 28 Interestingly, the study also assessed HUs 1-year post-operatively and found no difference between groups. 28 In similarity to Cho et al.’s study, our study did not find a correlation between lumbar HUs and mechanical failure. 28 When adjusting for clinically relevant predictors, HUs at the lumbar and UIV region remain without significant predictive value. Only the use of PSO was a statistically significant predictor of mechanical failure in the multivariable logistic analysis. It is commonly known that ASD patients in need of 3CO belong to a more severe patient group in need of greater surgical correction with consequently increased risk of mechanical failure. 3 Even after accounting for 3CO, lumbar HUs continued to lack significant predictive value. Upon stratifying our mechanical failure group by causes, we refrained from hypothesis testing due to limited sample sizes. We did observe an interesting association between high lumbar HUs in cases of screw breakage (171 [151-187]; n = 4) and low lumbar HUs in cases of screw loosening (75 [66-83]; n = 2) (Supplemental Table 2). These small sample sizes pose a high risk of type II errors, although it is logical that low HUs, could results in screw loosening, while stronger bones (high BMD) might be associated with screw breakage. Clearly, this hypothesis needs validation in larger cohorts.
There are several limitations to this study. Patients are included over a long time period (10 years) and changes in treatment and diagnostics are apparent. For example, in the beginning of the inclusion period, more patients underwent procedures including 3CO, whilst this was less frequent in the later years of the inclusion period. Secondly, the introduction of a new bone graft (DCF) in our institution on February 1, 2017 had a significant impact on the rate of mechanical failures. 1 These factors in combination might mask an existing association between lumbar HUs and mechanical failures. For instance, a patient with low HUs at the study’s outset might encounter mechanical failure, whereas a patient with low HUs in the later years of inclusion might not necessitate revision surgery. To our surprise, neither osteoporosis, BMI, smoking, or comorbidities was statistically significantly associated with mechanical failure. We ascribe this lack of difference to the small sample sizes included.
In summary, our findings are of relevance to both patients, researchers, and clinicians. The current study did not confirm our hypothesis and continuous research is necessary to help in the risk assessment for mechanical failure after ASD surgery.
Conclusion
The current study found no association between mechanical failure and HUs on preoperative CT scans in ASD patients. The heterogenetic nature of ASD patients with multiple confounders diminishes the possible association between HUs and mechanical failure. Thus, we cannot recommend using HUs to predict mechanical failure in ASD patients.
Supplemental Material
Supplemental Material - The Association Between Hounsfield Units and Mechanical Failure in ASD Patients
Supplemental Material for The Association Between Hounsfield Units and Mechanical Failure in ASD Patients by Martin Heegaard, Kristin Ingadottir, Lærke Ragborg, Benny Dahl, Lars Valentin Hansen, Søren Ohrt-Nissen and Martin Gehrchen in Global Spine Journal.
Supplemental Material
Supplemental Material - The Association Between Hounsfield Units and Mechanical Failure in ASD Patients
Supplemental Material for The Association Between Hounsfield Units and Mechanical Failure in ASD Patients by Martin Heegaard, Kristin Ingadottir, Lærke Ragborg, Benny Dahl, Lars Valentin Hansen, Søren Ohrt-Nissen and Martin Gehrchen in Global Spine Journal.
Footnotes
Acknowledgments
Thank you to all contributing authors.
Author Contributions
Martin Heegaard - Substantial contributions to the conception or design of the work. - Substantial contributions to the acquisition, analysis and interpretation of data. - Revising the work critically for important intellectual content. - Final approval of the version to be published. Kristin Ingadottir - Substantial contributions to the conception or design of the work. - Substantial contributions to the acquisition of data. - Revising the work critically for important intellectual content. - Final approval of the version to be published. Lærke Ragborg - Substantial contributions to the conception or design of the work. - Substantial contributions to the acquisition of data.- Revising the work critically for important intellectual content. - Final approval of the version to be published. Benny Dahl - Substantial contributions to the conception or design of the work. - Revising the work critically for important intellectual content. - Final approval of the version to be published. Lars Valentin Hansen - Substantial contributions to the conception or design of the work. - Revising the work critically for important intellectual content. - Final approval of the version to be published. Søren Ohrt-Nissen - Substantial contributions to the conception or design of the work. - Revising the work critically for important intellectual content. - Final approval of the version to be published. Martin Gehrchen - Substantial contributions to the conception or design of the work. - Substantial contributions to the analysis and interpretation of data. - Revising the work critically for important intellectual content. - Final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MG: Institutional grants from Cerapedics, institutional grants from NuVasive, institutional grants from Stryker; BD: Stryker (consultancy), supported by The Alfred Benzon Foundation; the remaining authors report no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Code Availability
Code can be made available upon reasonable request.
Ethical Statement
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available due to national data protection law.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.