
Abstract
Study Design
Retrospective series.
Objective
Screw loosening in the surgical treatment of lumbar spine disease is a major complication of osteopenia or osteoporosis. This study investigated the risk of screw loosening following either MIS-TLIF or pedicle screw-based dynamic stabilization (DS) in patients with osteopenia or osteoporosis.
Methods
We retrospectively enrolled patients receiving 1- or 2-level MIS-TLIF or DS in a single institute. All patients were diagnosed as having lumbar spondylosis without concurrent spondylolisthesis and found by dual-energy X-ray absorptiometry to have osteopenia or osteoporosis. Screw loosening was identified by X-ray and CT. Clinical outcomes were also assessed.
Results
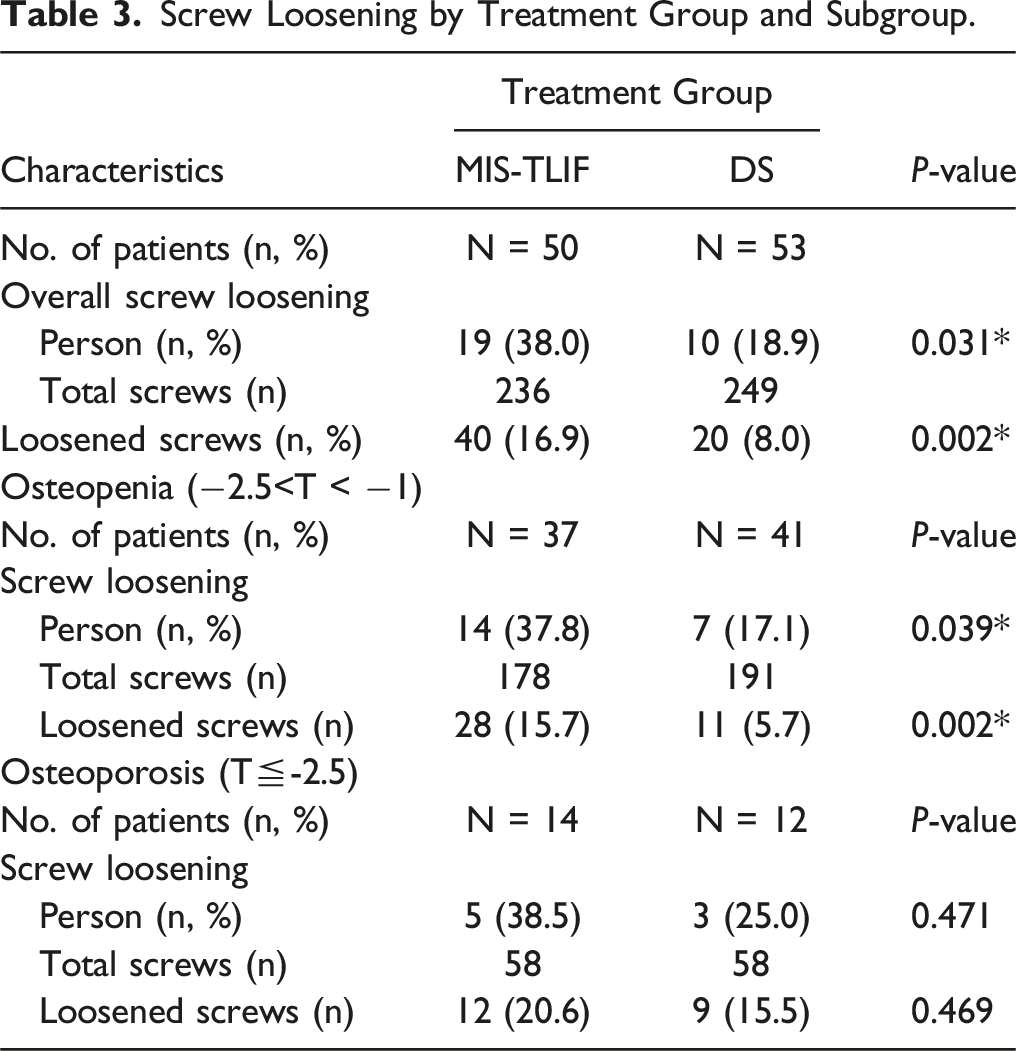
A total of 103 patients (50 MIS-TLIF and 53 DS) were confirmed to have osteopenia (−2.5<T-score < −1.0) or osteoporosis (T-score≦-2.5). The two groups, which were followed for 33.6 ± 24.7 and 52 ± 34.5 months, had similar T-scores (−1.97 ± 0.7 and −1.97 ± 0.6, respectively, P = 0.960). While both groups had significant improvements in back and leg pain assessed by VAS, ODI, and JOA scores, there was a significant difference in overall screw loosening rates between the MIS-TLIF and DS groups analyzed by percent of patients 38% and 18.9% (P = 0.039*) and by percent of screws 16.9% and 8% (P = 0.002*), respectively. Subgroup analysis showed a significant difference in screw loosening rate in osteopenia patients (P = 0.039* by person; P = 0.002* by screw), but no difference in osteoporosis patients.
Conclusion
The screw loosening rate was higher in the MIS-TLIF group in the entire cohort. Osteopenia patients receiving MIS-TLIF were at significantly higher risk of screw loosening, while that risk was not different for osteoporosis patients, compared to DS.
Introduction
Treatment of degenerative spondylosis and spondylolisthesis of the lumbar spine commonly begins with medications, injections, and physical therapy. In refractory cases, surgical decompression of the neural elements can relieve neurological symptoms, and surgical stabilization can reduce index-level pathology. One study of patients with these diseases treated with decompression with or without fusion reported them to have similar pain and disability outcomes, though those without fusion had higher reoperation rates.1,2
Recent advances in pedicle screws, interbody cages, biologics, and grafting materials have increased spinal fusion success. In 1982, Harms and Rolinger introduced transforaminal lumbar interbody fusion (TLIF),3-5 a development that improved decompression. Later, a minimally invasive TLIF (MIS-TLIF) allowed surgeons to perform TLIF with smaller wound sizes. Recently dynamic stabilization (DS) has emerged for managing lumbar spondylosis with low-grade spondylolisthesis. It is performed utilizing interspinous devices or pedicle screw–based stabilization systems. One very well-studied DS system, Dynesys dynamic stabilization (Zimmer Biomet), preserves flexibility in the instrumented spine and decreases adjacent level disease.6-11 Patients treated for degenerative spondylosis and spondylolisthesis of the lumbar spine often also have osteopenia or osteoporosis. The most widely accepted evaluation for osteopenia and osteoporosis is bone mineral density (BMD), which is measured by dual X-ray absorptiometry (DXA). The World Health Organization (WHO) defines osteoporosis as having a BMD of 2.5 SD or more below the average value for young healthy women (a T-score of ≦−2.5 SD). A second, higher threshold is used to define osteopenia with a T-score lying between −1.0 and −2.5 SD. 12 The surgical management of degenerative spinal disease in osteoporotic patients poses significant challenges. Osteoporosis-related loss of trabecular architecture weakens the bone, compromising pedicle screw mechanical retention, leading to screw loosening and subsequent complications. No study has compared the occurrence of screw loosening following one of two surgical instrumentation techniques, MIS-TLIF and DS. Therefore, we retrospectively performed a 24-month follow-up study of pedicle screw loosening and clinical outcomes in osteoporotic patients with medical-refractory lumbar spondylosis or degenerative disc disease causing stenosis with less than grade I spondylolisthesis treated with either MIS-TLIF or DS.
Material and Method
Patient Selection
This retrospective study was conducted using data extracted from the medical records of a single medical center’s digital database and questionnaires regularly administered between 2009 and 2019. Patients receiving 1- or 2-level MIS-TLIF or decompression plus DS were recruited consecutively. Evaluating these patients’ medical records, radiological images, and clinical evaluations, we included patients diagnosed as having symptomatic lumbar DDD or stenosis and confirmed to have osteopenia (−2.5<T-score < −1.0) or osteoporosis (T-score of ≦−2.5 SD) by DXA according to the WHO criteria 12 and found refractory to conservative treatment for at least 12 weeks before surgery. We excluded any patient who had concurrent spondylolisthesis, multiple levels (>2 levels) of disc disease, degenerative scoliosis, vertebral fracture, infection, or tumor or any patient who was lost to follow-up. After exclusion, the patients were categorized into either a MIS-TLIF group or DS group. The inclusion and exclusion criteria for either treatment group was similar. The decision to treat with MIS-TLIF or DS was based on mutual agreement between the patients and the surgeons after a thorough discussion of treatment options. A consensus regarding the treatment was arrived at in a meeting with the surgical team before surgery. All data were de-identified, so no consent was required. All protocols were approved by the Institutional Review Board in our hospital (IRB No:2023-12-009CC).
Surgical Techniques
On the day of surgery, patients received general anesthesia and were placed in a prone position with the lumbar spine in a neutral or slightly lordotic position. For patients in the MIS-TLIF group, we first placed tubular retractors and then placed the serial dilators on the indexed facet joint under fluoroscopy. Then, we performed facetectomy and partial laminectomy with high-speed drills and Kerrison rongeurs under microscopy. The same procedures were performed on the contralateral side. After resection of the hypertrophic ligamentum flavum and discectomy, we packed local bone autografts and demineralized bone matrix into the space left by disc removal. We then placed a polyetheretherketone (PEEK) interbody cage into the interbody space. The tubular retractor was then removed, and the pedicle screws were placed percutaneously under the guidance of intraoperative fluoroscopy.
For patients in the DS group (Dynesys), who received dynamic pedicle screw insertions, we first performed total laminectomy of the lumbar spine via a posterior midline incision. The decompressed bilateral neural foramen and lateral recesses were decompressed using Kerrison rongeurs, carefully preserving bilateral facet joints. Subdermal dissection of skin and muscle layers were performed via the same midline skin incision described above and Dynesys titanium alloy screws were inserted transpedicularly through the Wiltse plane. The elastic rods, polycarbonate urethane spacers, and polyethyleneterephthalate cords (Sulene-PET) were assembled without intentional intraoperative reduction of any spondylolisthesis or change of the lordotic curvature. The insertion of the pedicle screws was performed under lateral fluoroscopy. For both groups, all wounds were subsequently closed in layers after copious irrigation.
Clinical and Radiological Assessment of Pedicle Screw Loosening
Clinical outcomes were assessed using a visual analog scale (VAS) for back and leg pain, the Oswestry Disability Index (ODI), and the modified Japanese Orthopedic Association (JOA) clinical symptom scoring. Questionnaires were completed by the patients preoperatively and at 6, 12, 18, and 24 months postoperatively with the assistance of a nurse supervised by a physician during each visit.
Radiological evaluations of pedicle screws loosening were performed by X-ray and CT, with images obtained at each postoperative clinic visit. The CT scans were obtained before surgery, within five days after surgery, and then 12-24 months later. Radiolgical screw loosening was identified based on abnormal halo sign, screw migration, and peri-screw radiolucency findings. 13 Interbody fusion in the MIS-TLIF group was assessed primarily with dynamic lateral X-ray and CT scans, both of which have been found to be equally accurate. 14 When there was any ambiguity, CT scans were performed for final determination. All radiological evaluations were conducted independently by a neurosurgeon and a radiologist in a double-blind fashion. If there were any inconsistencies, evaluation was made by consensus by a team of physicians.
Statistical Analysis
Data are presented as the mean ± SD for continuous variables and frequency and percentages were used for categorical variables. All statistical tests were 2-tailed, and a P-value <0.05 was considered significant by independent t test, paired t test, or chi-square test.
All statistical operations were performed using Stata version 17.0 (StataCorp, College Station, TX 77845 USA).
Result
Preoperative Patient Characteristic and Clinical Evaluation.
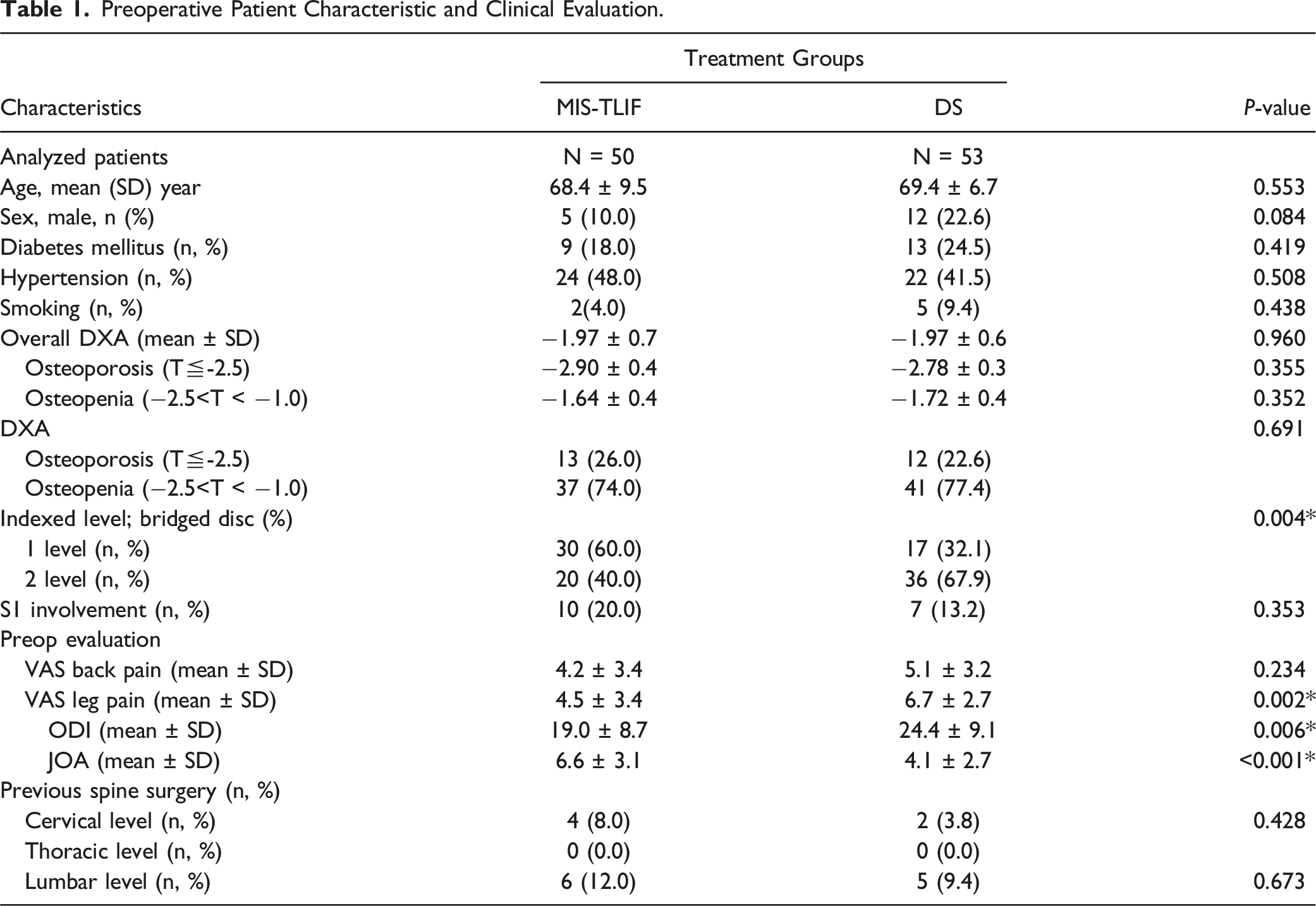
We found no significant differences between the MIS-TLIF and DS groups with regard to age, sex, and comorbidities including diabetes mellitus, cigarette smoking, and hypertension (P = 0.419, 0.438, and 0.508, respectively; Table 1). Before surgery, the two groups had similar clinical neurogenic claudication symptoms and radicular pain as well as similar VAS back pain, VAS leg pain, ODI, and JOA clinical assessment scores.
Clinical Outcomes
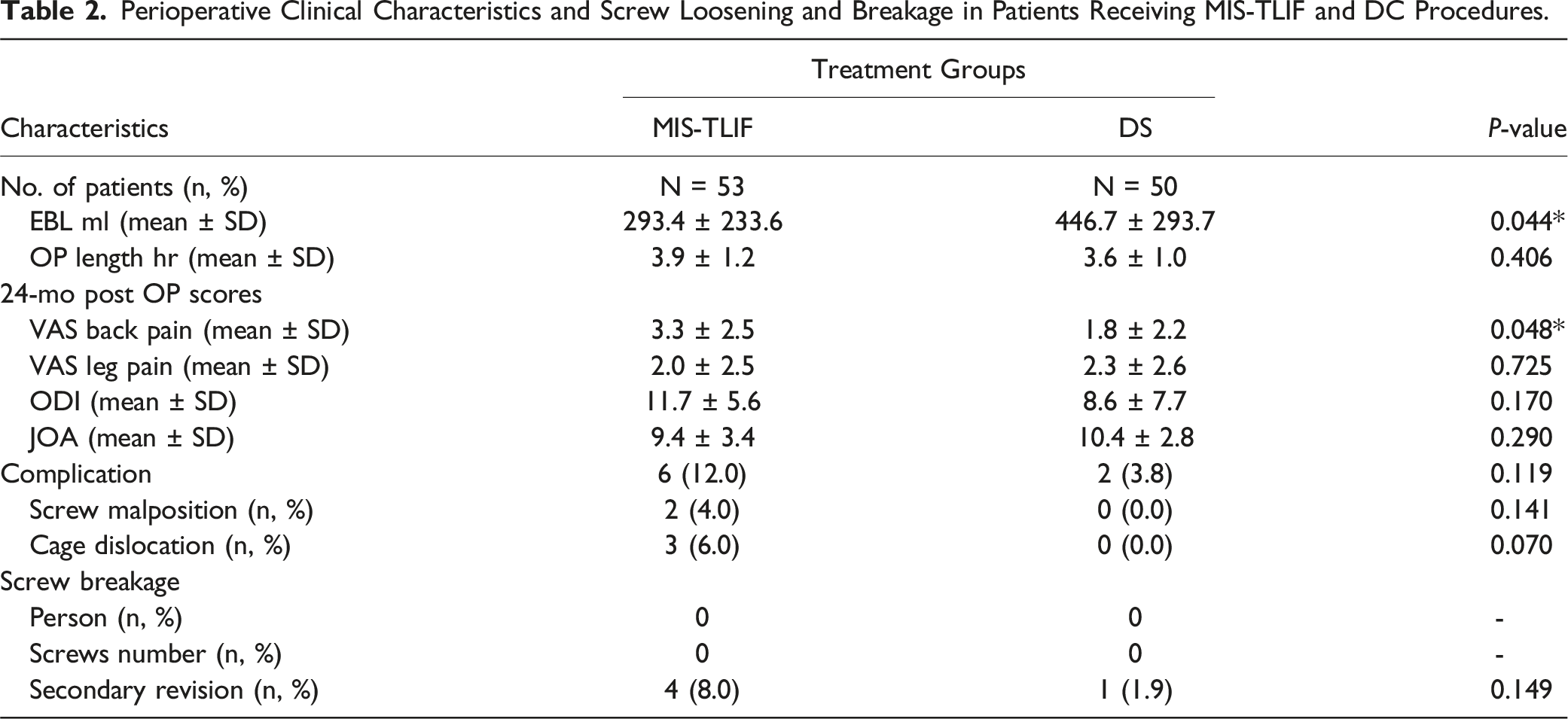
Perioperative Clinical Characteristics and Screw Loosening and Breakage in Patients Receiving MIS-TLIF and DC Procedures.
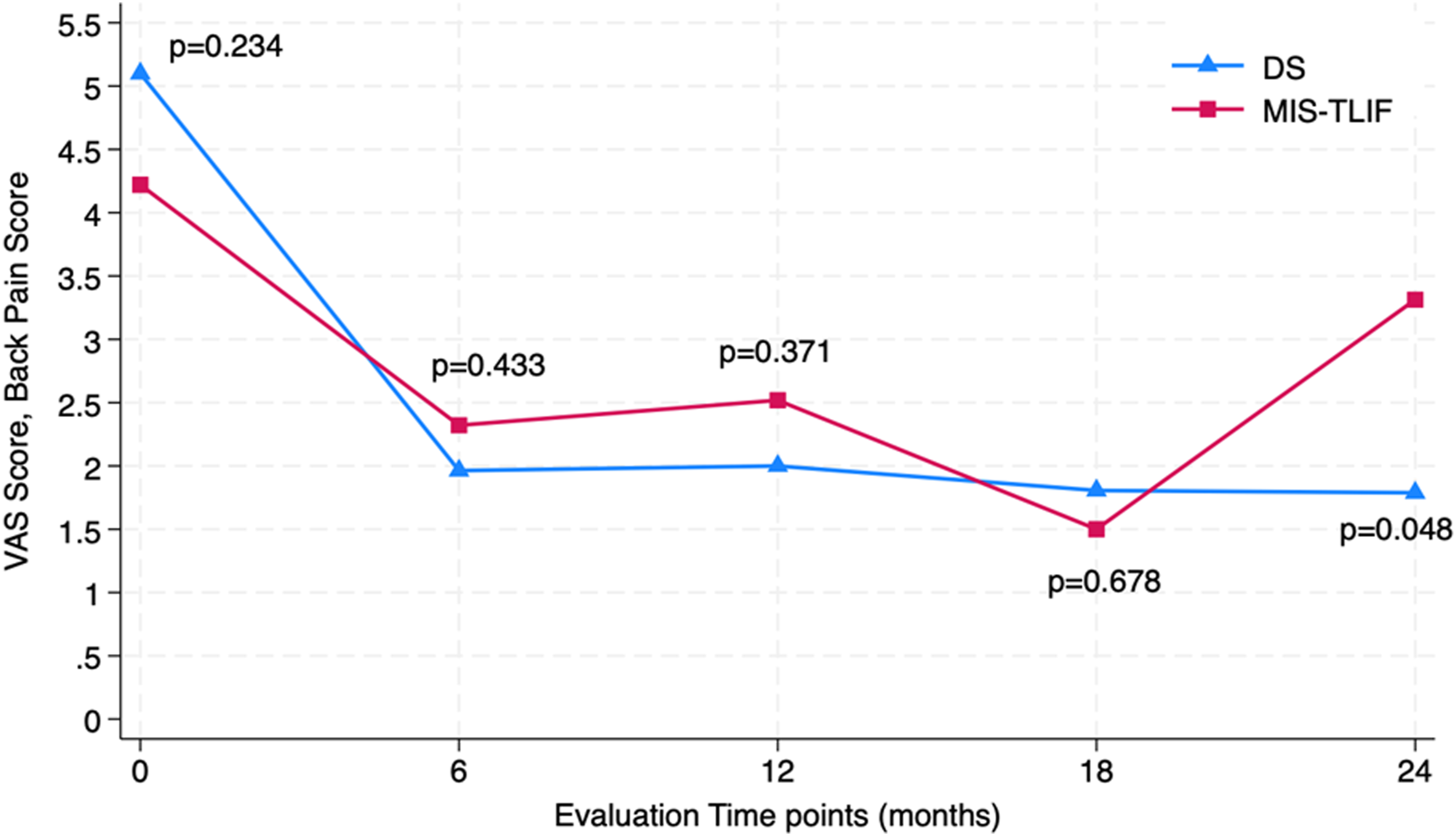
Average VAS back pain score of the two treatment groups at four time points compared to baseline. Both groups had significantly improved postoperative outcomes. No significant difference was found in clinical outcomes between the MIS-TLIF and DS groups at different time points until near the end of the follow-up period, at which time there was an increase in VAS in the MIS-TLIF group.
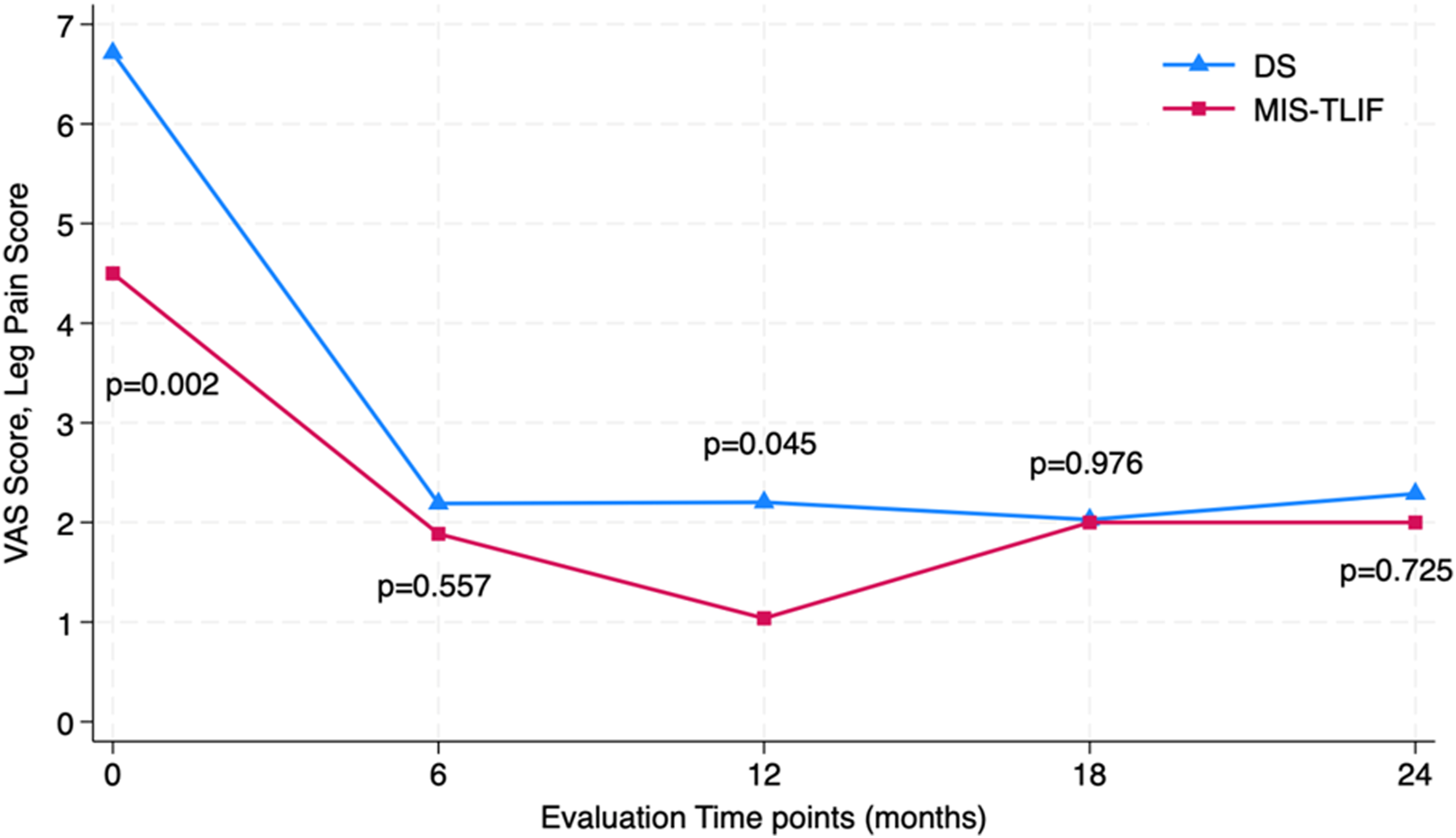
Average VAS leg pain scores for the two treatment groups at four time points compared to baseline, showing significant improvement postoperatively. There were no significant differences between the MIS-TLIF and DS groups at any time point.
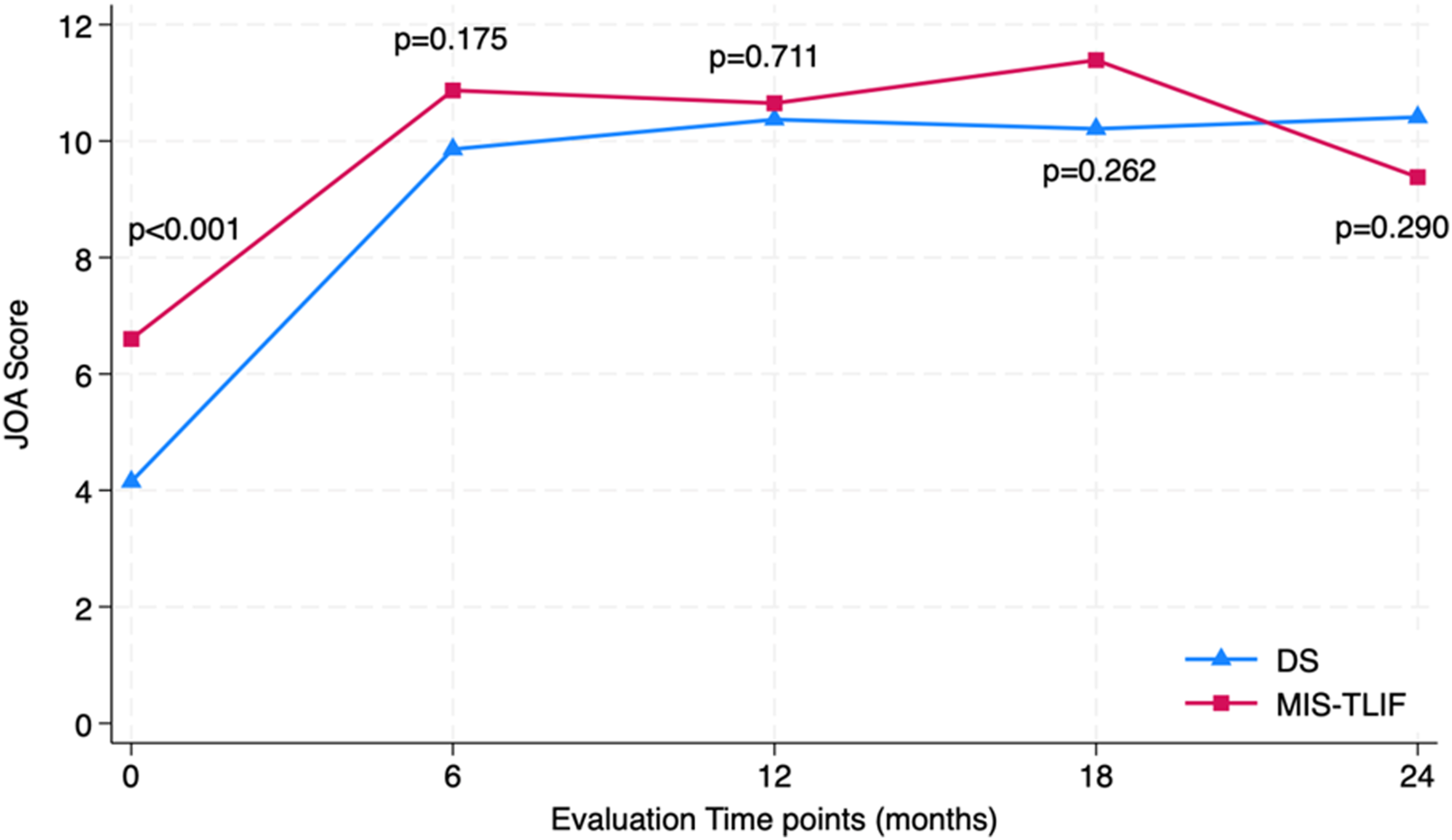
Both MIS-TLIF and DS groups had similar improvements in the ODI and JOA scores. Comparing preoperative values with two-year post-operative values, we found that the ODI improved from 19.0 ± 8.7 to 11.7 ± 5.6 and from 24.4 ± 9.1 to 8.6 ± 7.7 in the MIS-TLIF and DS groups, respectively (both P < 0.001). During this period, the JOA scores of both groups improved from 6.6 ± 3.1 to 9.4 ± 3.4 and from 4.1 ± 2.7 to 10.4 ± 2.8, respectively (both P < 0.001). There were no intergroup or intragroup differences at each evaluation time point (Tables 1 and 2; Figures 3 and 4). Average ODI scores at four postoperative timepoints, compared to baseline, showing significant improvement. There were no significant differences between the MIS-TLIF and DS groups at any time point. Average JOA scores as four postoperative timepoints, compared to baseline, showing significant improvement. There were no significant differences between the MIS-TLIF and DS groups at any time point.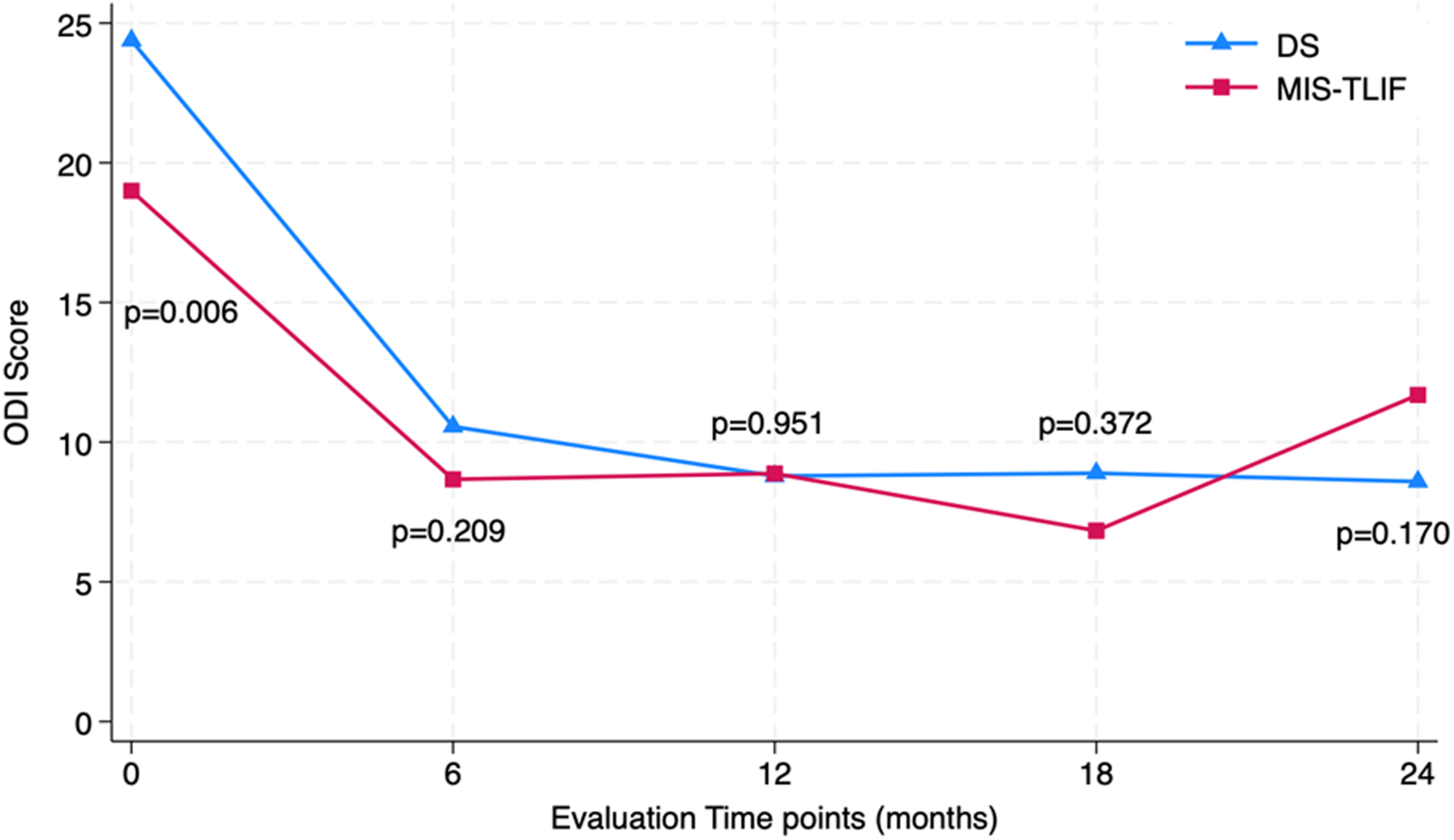
Radiological Evaluation for Pedicle Screw Loosening
Screw Loosening by Treatment Group and Subgroup.
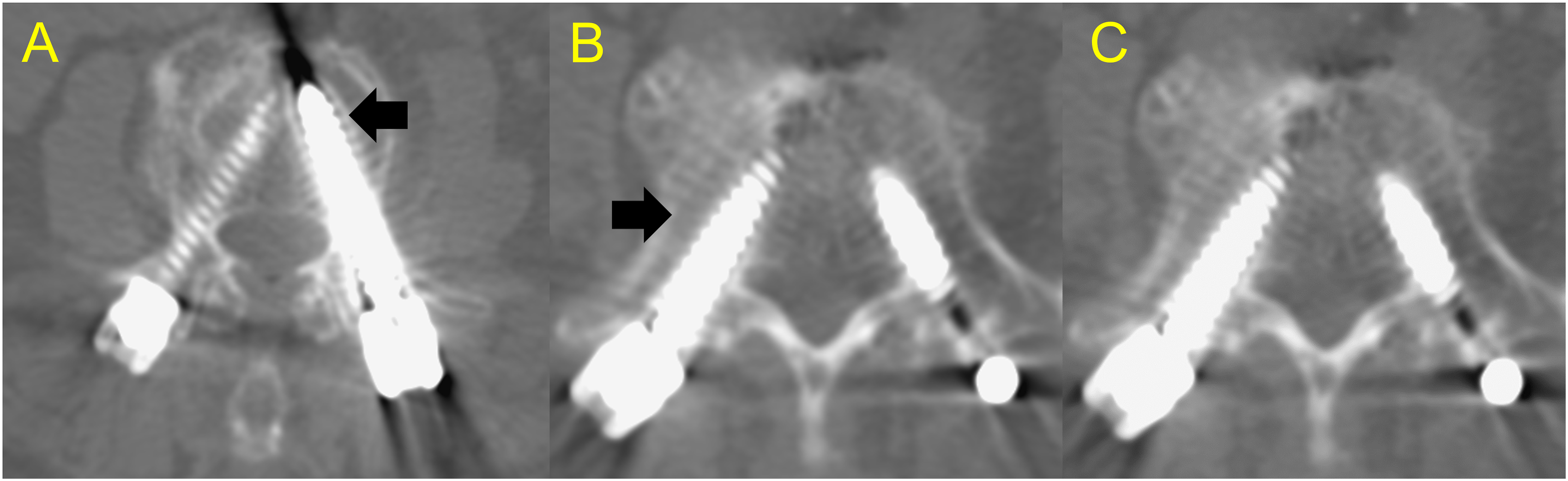
(A) A 60-year-old female patient who had received Dynesys dynamic stabilization (DS) system at L4-5. The preoperative DXA was −3.2. CT showed no screw loosening at 24 months postoperatively. (B) A 73-year-old female patient who had received minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF) at L3-4-5. The pre-operation DXA was −1.2. CT images at 8 months after surgery showed loosening of the left L3 pedicle screw and loosening at right L5 pedicle screw (C).
Discussion
To the best of our knowledge, this study is the first to perform a follow-up investigation comparing the incidence of pedicle screw loosening following MIS-TLIF and DS surgeries for osteoporotic patients with symptomatic lumbar DDD or stenosis without concurrent spondylolisthesis. The two treatment groups had similar post-surgical neurological functional and clinical outcomes (VAS, ODI, and JOA scores), but by the 24th month, the MIS-TLIF group had an overall significantly higher incidence of pedicle screw loosening and a slight recurrence of VAS back pain. TLIF has been used to treat patients with lumbar spondylosis and spondylolisthesis starting around the second half the 1990s. Later, the development of MIS-TLIF reduced collateral tissue damage and blood loss, shortened hospital stays, and speeded up recovery time, compared to conventional TLIF.15-20 More recently, DS has emerged as a means of managing lumbar spondylosis and low-grade spondylolisthesis. An alternative to fusion, DS offers several advantages, including protection of range of motion, preservation of spinal motion, and reduced risk of adjacent segment disease, etc.8,9,21-23 The Dynesys system, which has received US FDA approval for use as an adjunct to spinal fusion, has been used for non-fusion pedicle screw stabilization and has been reported to provide enough stability to prevent progression of low-grade spondylolistheses.6,10,11,24-26
The surgical management of lumbar degenerative spinal disease in patients with osteopenia or osteoporosis can be challenging. Spinal instrumentation, which is widely used to treat this degenerative spinal disease, necessitates the use of pedicle screws. The effectiveness of these screws as well as the patency of the instrumentation largely depends on the bone-screw interface. Osteopenia or osteoporosis of the pedicle or vertebrae is known to reduce bone-metal osteointegration, leading to screw loosening and screw pull-out.27-30 Pedicle screw loosening is a common complication following TLIF, especially in osteoporotic patients. One long-term follow-up study of 365 osteoporotic patients receiving 2038 pedicle screw placements during TLIF procedures found a loosening of 60% of the screws placed. 31 Screw loosening is also a well-known complication in pedicle screw-based dynamic stabilization, with one study finding a loosening in nearly 5% of screws placed in 20% of patients undergoing pedicle screw-based DS for lumbar degenerative disease in a single center. 13
There are several published series that specifically investigate pedicle screw loosening in patients with osteopenia or osteoporosis after lumbar fusion surgery. Formby et al 32 reported a higher rate of screw loosening in osteoporotic patients (4/18 patients, 22.2%) compared with non-osteoporotic groups (6/70 patients, 8.6%) in TLIF surgery. Wu et al, 33 reporting the results of a prospective randomized study on screw loosening in patients treated for spinal stenosis who also had osteoporosis and underwent fusion surgery, found that out of 464 conventional screws placed, 48 had loosened by the end of their 1-year follow-up (10.3%). While the impact of osteoporosis on screw loosening in TLIF surgery is generally accepted as a real possibility by many spine surgeons, few studies have investigated the correlation of screw loosening and osteoporosis in patients undergoing dynamic stabilization. In a retrospective study of the use of dynamic stabilization (Dynesys) for decompression of 1- or 2-level lumbar spondylosis in 71 patients with stenosis, spondylolisthesis, and radiculopathy, Ko et al 34 reported that 14 patients (19.7%) had screw loosening, and they reported a rate of 4.6% per screw (17/368 screws). Wu et al, 22 retrospectively performing a 24-month follow-up analysis of the patency of 658 screws placed during DS (Dynesys) after decompression in 126 patients, found loosening in 31 screws (31/658, 4.7%) implanted in 25 patients (25/126, 19.8%). They also reported 22 of 25 cases to have screw loosening (88%) within 6.6 months of surgery, with the screw loosening rate higher in those with diabetes than those without it. Neither study took osteoporosis into consideration, however. Chang et al conducted the first study to evaluate the impact of bone density on screw loosening in dynamic stabilization using CT Hounsfield Unit (HU) as a surrogate indicator of bone density. They concluded that the HU values were unrelated to screw loosening in dynamic stabilization.
We conducted the present study specifically focusing on the risk of screw loosening in both MIS-TLIF and DS cohorts, especially in those with osteopenia or osteoporosis. Overall, we found a greater incidence of screw loosening in the MIS-TLIF group (19/50, 38.0%), compared to the DS group (10/53, 18.9%) (Table 3). Forty of the 230 screws placed in the MIS-TLIF group and 20 of the 249 screws placed in the DS group had loosened. The overall higher incidence of screw loosening in the MIS-TLIF group might explain their slight increase in recurrent back pain near the end of the follow-up period (Figure 1). As can be seen Table 3, we also performed a subgroup analysis to investigate the screw loosening rate in patients with osteopenia (−2.5<T-score < −1) or osteoporosis (T-score≦-2.5) between the MIS-TLIF and DS groups. Our results showed that in osteopenia (−2.5<T-score < −1) patients, there was a significantly different risk of screw loosening between the two treatment groups (MIS-TLIF and DS), while there was no such difference in these treatment outcomes in the osteoporosis (T-score≦-2.5) patients. From a clinical biomechanism perspective, we inferred that in osteopenia patients (−2.5<T-score < −1.0), patient’s facet was destroyed and the vertebral disc was removed and replaced by cage in a MIS-TLIF surgery. But in DS group, we preserved bilateral facets and vertebral disc.35,36 There was more instability created in the MIS-TLIF than in the DS group, and thus MIS-TLIF was more likely to result in screw loosening in the osteopenia patients, whose bone quality were not as bad as that in the osteoporosis patients. However, for osteoporosis patients (T-score≦-2.5), osteoporosis itself is already a major and decisive risk factor known to induce screw loosening,29-31,37 and such a risk factor would lead to similar screw loosening rate in MIS-TLIF and DS group regardless of the greater instability created by MIS-TLIF.
This study has some limitations. One limitation is that it is a small and retrospective nonrandomized cohort study with inherent limitations. Because the present study investigated a specific group of patients, ie, osteopenia and osteoporosis, and because all patients enrolled had had pre-operative DXA to confirm their T-score, our case numbers were not large. Another limitation is that patient allocation to MIS TLIF and dynamic fixation was not random and involved surgeon’s bias. The choice of DS or MIS-TLIF was decided by the patient after consulting with the senior surgeon. Although both options were clearly presented and well explained, there is inevitably some selection bias in this retrospective study, either resulting from the patient’s or the surgeon’s preference. However, the demographic data was very similar between the two groups, indicating a minimal difference in both cohorts. Another limitation is that no definitive conclusion can be made about DS based on our results because more time is needed evaluate screw loosening pathology and the durability of the dynamic instrumentation.
Conclusion
Although the clinical pain, disability, and quality-of-life outcomes of MIS-TLIF and DS were similar among our patients with osteopenia or osteoporosis, the overall screw loosening rate was significantly higher in the MIS-TLIF group, possibly contributing to the mild recurrence of VAS for back pain near the end of the study period. Considering that we found less screw loosening in the DS group, dynamic stabilization may be a good alternative to rigid fusion in the treatment of 1- or 2-level degenerative lumbar spondylosis without concurrent spondylolisthesis in patients with osteopenia (−2.5<T-score < −1.0). There was no obvious difference in screw loosening rate in patients with osteoporosis (T-score≦-2.5).
Footnotes
Acknowledgments
We thank Dr Tsai-Tzu Ko for her contribution to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement regarding COI
There are no commercial or financial relationships that could be construed as a potential conflict of interest (COI). This article also not a clinical trial without ethical problem. There is also no funding related to this article.