
Abstract
Study Design
Randomized Clinical Trial.
Objective
To compare the clinical efficacy and restoration of working capacity after MI (minimally invasive)-TLIF and O (open)-TLIF in railway workers with lumbar degenerative disease.
Methods
83 patients, who were indicated for two-level lumbar decompression and fusion were randomly assigned to one of two groups: group 1 (n = 44) had MI-TLIF procedure and group 2 (n = 39) had O-TLIF procedure. The functional status was assessed using SF-36, ODI and VAS for back and leg pain, preoperatively, at discharge, and at 3, 6, and 12 months postoperatively. MRI and CT were obtained 1-year follow-up. The percentage of patients who returned to work at 1-year, work intensity and the time to return to work post-operatively were analyzed.
Results
At 1-year follow-up, the MI-TLIF group had significantly better ODI, VAS and SF-36 scores compared to the O-TLIF group. The postoperative MRIs revealed a statistically significantly less multifidus muscle atrophy in the MI group compared to the Open group. At 1-year follow-up, a comparable fusion ratio between MI group and Open group was recorded. After MI-TLIF procedure, depending on the workload, patients had a statistically significantly earlier return to work (P < .05) and statistically significantly higher return to work rate compared with the O-TLIF group (P < .05).
Conclusions
The use of two-level MI-TLIF in railway workers has made it possible to significantly improve long-term clinical results, reduce the risk of surgical complications, muscle atrophy and time to return to work compared to O-TLIF.
Keywords
Introduction
Spinal fusion is indicated for patients with lumbar degenerative disease who have failed conservative measures. 1 There is controversy regarding the benefits of minimally invasive over open decompression-stabilization techniques with some studies noting the advantages of MI-TLIF compared to O-TLIF,2,3 while others reporting comparable long-term clinical and radiological results.4,5
Returning to their previous work activities is an important postoperative outcome for patients. 6 The inability to return to previous work has significant financial implications for patients, their families and society. 7
Further, prolonged disability can adversely affect the physical and mental state of patients. 8 In addition to such factors as the initial physical status, age, and comorbidities, the nature of the workload and the magnitude of surgical intervention affect the ability to return to work. 9
A population with regular heavy physical exertion at work and high requirements for admission to work are Railway workers. 10 The ability to safely and effectively continue one’s professional activity as soon as possible after surgical treatment is an important consideration for surgical intervention in these patients. 11
In this study, we conducted a prospective, blinded, and randomized trial to determine the clinical effectiveness and restoration of working capacity within the first year following MI-TLIF and O-TLIF in railway workers with lumbar degenerative disease.
Methods
Patient Population
This prospective randomized study was approved by the ethics committee of Irkutsk State Medical University (No.1, dated February 24, 2021). Each patient gave voluntary statement regarding informed consent to be included in the study. The analysis of the clinical material was carried out in accordance with the principles of the Declaration of Helsinki. The data used to support the findings of this study are restricted by the Ethics Committee of Irkutsk State Medical University in order to protect patient privacy. Data are available from the corresponding author (VAB) for researchers who meet the criteria for access to confidential data.
The trial was registered with the Unified State Information System for Recording the Results of Research, Development and Technological Works for Civil Purposes (USISR RDTWCP; https://rosrid.ru/), and its clinical trial registration no. is 622011400059-4. The study was conducted at the Center for Neurosurgery of the Irkutsk Railway Hospital and enrolled 83 consecutive patients, including 27 women (32.5%) and 56 men (67.5%) who underwent decompression and fusion surgery of the lumbar spine between March 2021 and December 2021 (Figure 1). The diagnoses treated included lumbar degenerative scoliosis with stenosis or spondylolisthesis. The surgical procedures involved a minimally invasive and open two-level decompression of adjacent spinal segments with transforaminal lumbar interbody fusion and transpedicular fixation. CONSORT flow diagram of study.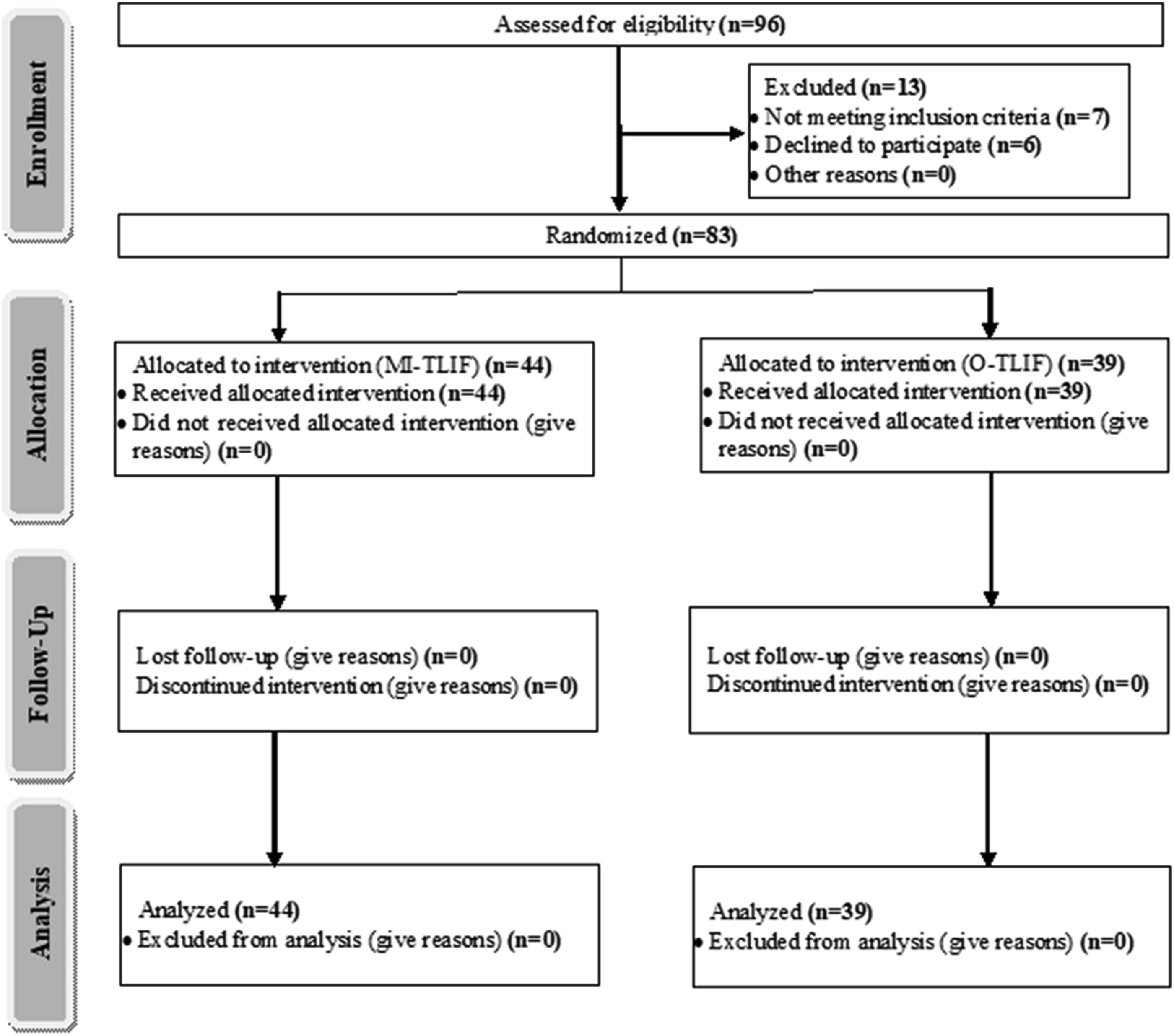
Patients were excluded from the study if they met any of the following criteria: unable to read or understand the study protocol, had a contraindication to study medications or anesthesia, had a condition that could impact the required neurological assessments (e.g., insulin-dependent diabetes mellitus, neuropathy in the lower extremities, demyelinating disease, or history of stroke), had hepatic or renal failure, used opioids chronically, had an active history of substance abuse, were pregnant, had a deficit in hearing or vision that prevented study assessments, had a history of cognitive impairment or dementia with a baseline score of less than 23 on the Mini-Mental State Examination (MMSE), had a history of anxiety and/or depression according to the Hospital Anxiety and Depression Scale (≥11 points), had an American Society of Anesthesiologists (ASA) status greater than III, had an educational level less than grade 9, or had a history of mental illnesses.
Protocol
All the patients were randomly assigned to one of two treatment groups: group 1 received MI-TLIF, and group 2 received O-TLIF. The randomization was based on a computer-generated randomization sequence (https://www.randomizer.org). The random assignment of each patient was determined by opening a sealed envelope just prior to surgery.
Surgical Techniques
One primary surgeon (V.A.B.) performed all of the MI-TLIF, as well as the O-TLIF procedures.
In the MI-TLIF group (n = 44), we used an intermuscular paramedian approach with an expandable tubular dilatator, decompressing the spinal canal using an “Over the Top” technique 12 – bilateral decompression from a unilateral laminotomy approach, removal of the undersurface of the contralateral lamina, discectomy and MI-TLIF with percutaneous bilateral transpedicular fixation were performed; in the O-TLIF group (n = 39), intervention was performed from a median approach with bilateral dissections of the paravertebral muscles, partial or complete laminectomy, discectomy and O-TLIF, and open transpedicular fixation.
Inclusion Сriteria
- lumbar degenerative spondylolisthesis; - bisegmental lesion and/or the need for a two-level surgical intervention; - radiological signs of segmental instability: Slip Percentage >15%, Dynamic Slip >4.5 mm, Dynamic Segmental Angle >15° (L1-L2, L2-L3, L3-L4); >20° (L4-L5); >25° (L5-S1)
13
; - primary decompression and stabilization intervention in the lumbar spine.
Exclusion Сriteria
- lumbar degenerative disease without segmental instability; - monosegmental lesion and/or the need for one level surgical intervention; - polysegmental lesion and/or the need for three or more level surgical intervention; - decompression without stabilization; - revision cases; - refusal to participate in the study.
Data Analyzed
The demographic parameters obtained through a review of medical records included sex, age, body mass index.
All patients were assessed when they checked in for surgery, at the time of hospital discharge, and at follow-up appointments 3, 6, and 12 months after surgery. Patients completed a questionnaire at each follow-up appointment yielding their Oswestry Disability Index (ODI) score. The ODI score was considered the primary outcome. Pain severity was evaluated using the visual analog scale (VAS). Quality of life studying according to SF-36.
Radiological outcomes before operation and at the last follow-up included the multifidus muscle area, calculated from anonymized axial T2w MRI images using the MultiVox DICOM Viewer software (Gamma Multivox, Moscow, Russia) by two independent experts (neurosurgeon and radiologist) blinded to the treatment group of each patient. Statistical evaluation of expert agreement on each question was carried out using Kappa statistics (Graph Pad Software, Inc, USA). Multifidus muscles were segmented from preoperative and postoperative MRIs using anatomical landmarks, and the total area for the right and left sides of each level were recorded. The average muscle area across all three levels was calculated. Statistical analysis was performed on the percent area change metric as one indication of muscle atrophy. In this study, multifidus fat content was not assessed. We performed postoperative MRIs on all patients at long-term follow-up, regardless of their neurological status, to assess the completeness of the decompression and to determine the degree of atrophic changes in the paravertebral tissues.
The status of intervertebral fusion was measured using the Bridwell evaluation criterion 14 at last follow-up.
The criterion for restoration of working capacity was the absence of pain and neurological disorders during the performance of physical activity loads with resumption of previous employment.
Return to Work – number of patients who returned to work at 1 year following their surgery and the number of days after surgery it took for patients to resume working. The date of the return to work was self-reported in the follow-up questionnaires. Specifics such as part-time vs full-time work and workplace restrictions were not captured. Baseline workload was self-reported at baseline in the preoperative patient questionnaire and was categorized as sedentary to very heavy based on lifting pattern as defined by the dictionary of Occupational Title (https://occupationalinfo.org). This study divided workloads into 3 categories: sedentary, light-moderate and heavy-very heavy.
Statistical Analysis
Statistical processing of the study results study was carried out on a personal computer using the Statistica 13.5 program. The necessary statistical power of the study and the number of cases in each group were calculated, and the ODI score was considered the main indicator of functional outcome. A minimum of 37 cases was needed in each group to achieve 80% statistical power, with P < .05 as the 2-tailed level of significance indicating achievement of the minimum clinically significant 10-point difference in ODI score (standard deviation = 15).
The character of the distribution of signs was evaluated by the Shapiro — Wilk, Kolmogorov — Smirnov and Lilliefors tests for normality. Considering the presence of statistically significant differences according to these tests (P < .05), the distribution was considered to be different from normal. In this regard, the criteria of nonparametric statistics were used to assess the significance of the differences in the samples. The obtained results are presented by the median, the values of the 1st and 3rd quartiles — Me (Q25; Q75). For a comparative analysis of the obtained values, the Mann — Whitney U—test and the Wilcoxon criterion, the χ2 criterion for binomial signs were used.
Results
General Data of the Studied Patients.
An intergroup comparison of intraoperative parameters and the course of the postoperative period revealed statistically significantly lower parameters in the MI-TLIF group, as compared with the O-TLIF group: the operative time - 155 (125; 175) min vs 200 (165; 245) min, respectively (P = .01); the volume of blood loss 130 mL (100; 180) vs 550 mL (350; 800), respectively (P = .002); time to mobilization 1 (1; 2) day vs 2 (1; 3) days, respectively (P = .02); duration of inpatient treatment 5 (4; 6) days vs 8 (6; 9) days, respectively (P = .006).
VAS scores (Figure 2) indicated considerable back pain and leg pain relief immediately after surgery (P < .01) and remaining low thereafter. There was significantly lower back pain (discharge, P < .001; 3 months, P < .001; 6 months, P < .001; 12 months, P < .001) and leg pain (discharge, P < .001; 3 months, P < .001; 6 months, P < .001; 12 months, P < .001) in the MI-TLIF group than in the O-TLIF group. During the observation period, the level of pain in the back and legs did not exceed 20 mm in either group. Pain visual analog scale (VAS) scores before operation, at discharge, and 3, 6, and 12 months postoperatively in the 2 groups of prospective study (n = 83), shown as the median and interquartile range. VAS score of 0 indicates absence of pain; 100 is the highest possible level of pain intensity.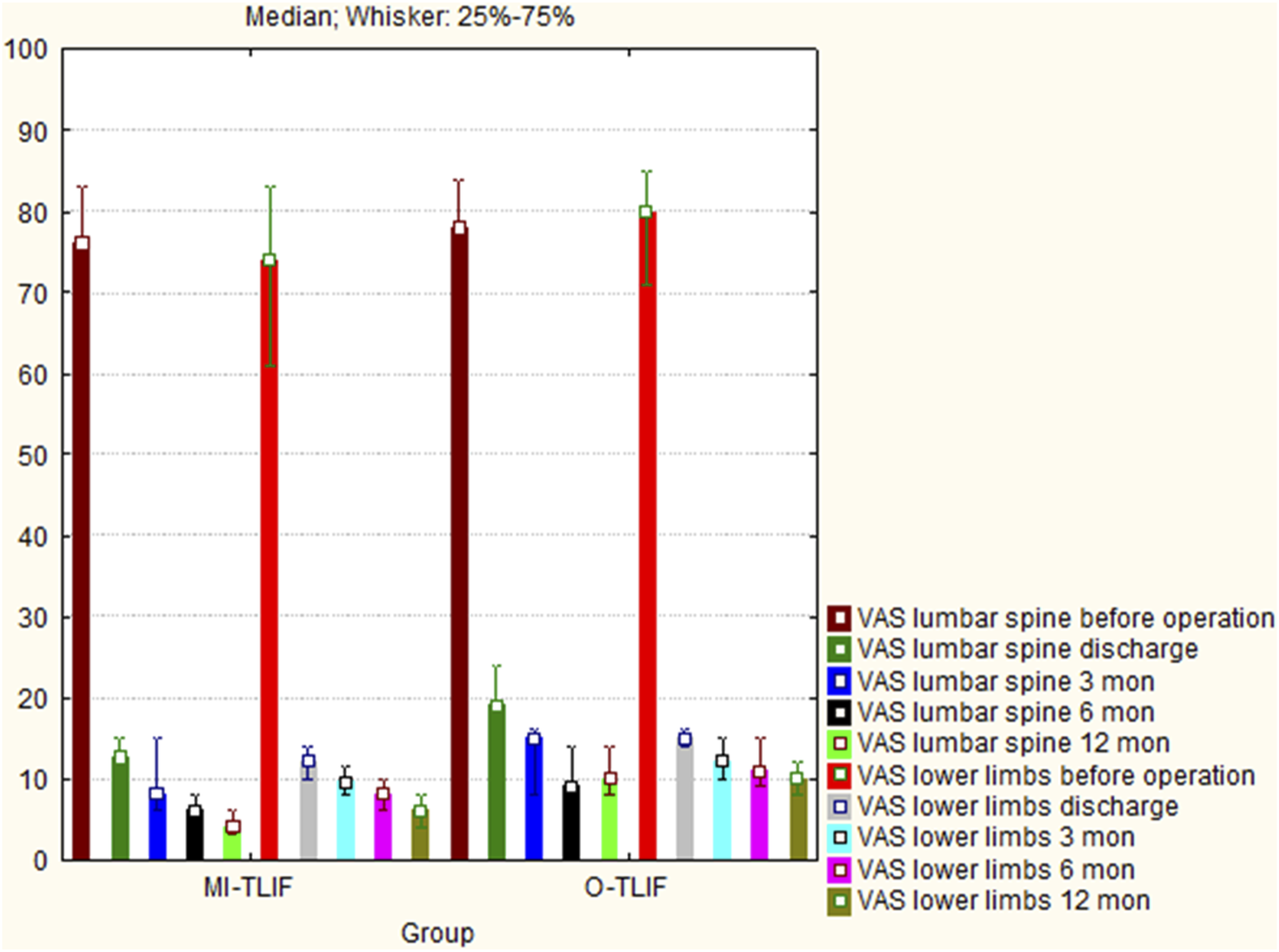
At discharge, ODI scores indicated highly significant improvement in patients’ quality of life in both groups (P < .01) (Figure 3). Intergroup comparison showed difference in the patients’ ODI scores across groups at discharge, 3, 6, and 12 months after lumbar fusion (P = .001, P = 0,01, P < .001, P < .001, respectively). Oswestry disability index (ODI) scores before operation, at discharge, and 3, 6, and 12 months postoperatively in the 2 groups in the prospective study (n=83), shown as the median and interquartile range. The lowest ODI score corresponds to the best functional state.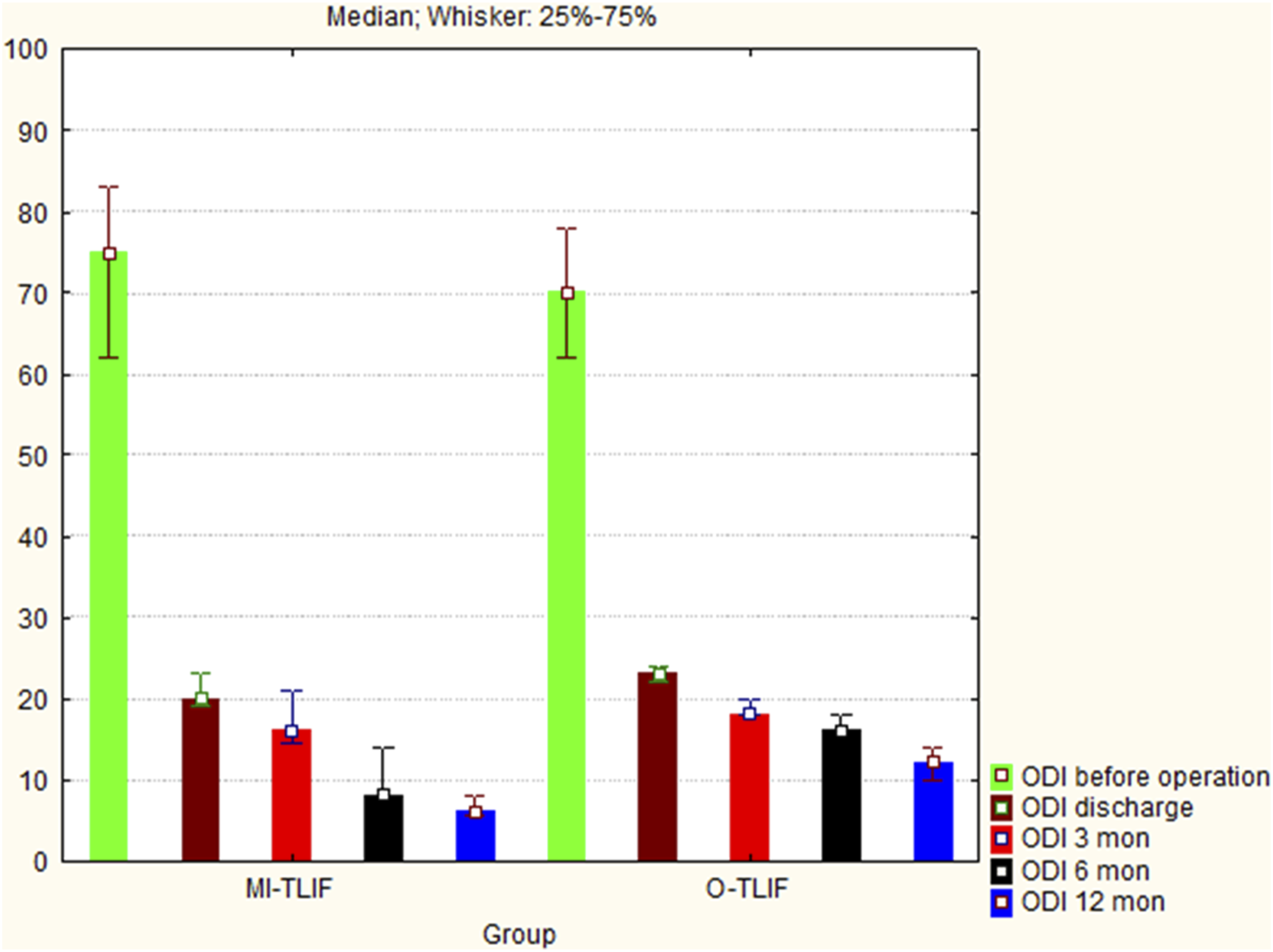
Intergroup comparison showed better outcomes after MI-TLIF in comparison to O-TLIF according to SF-36 (Figure 4). There was significantly higher PCS (discharge, P = .001; 3 months, P < .001; 6 months, P < .001; 12 months, P < .001) and MCS (3 months, P < .001; 6 months, P < .001; 12 months, P < .001) in the MI-TLIF group than in the O-TLIF group. At discharge MCS was comparable in both groups (P = .93). SF-36 (physical component score (PCS) and mental component score (MCS)) scores before operation, at discharge, and 3, 6, and 12 months postoperatively in the 2 groups in the prospective study (n = 83), shown as the median and interquartile range. The highest SF-36 score corresponds to the best quality of life.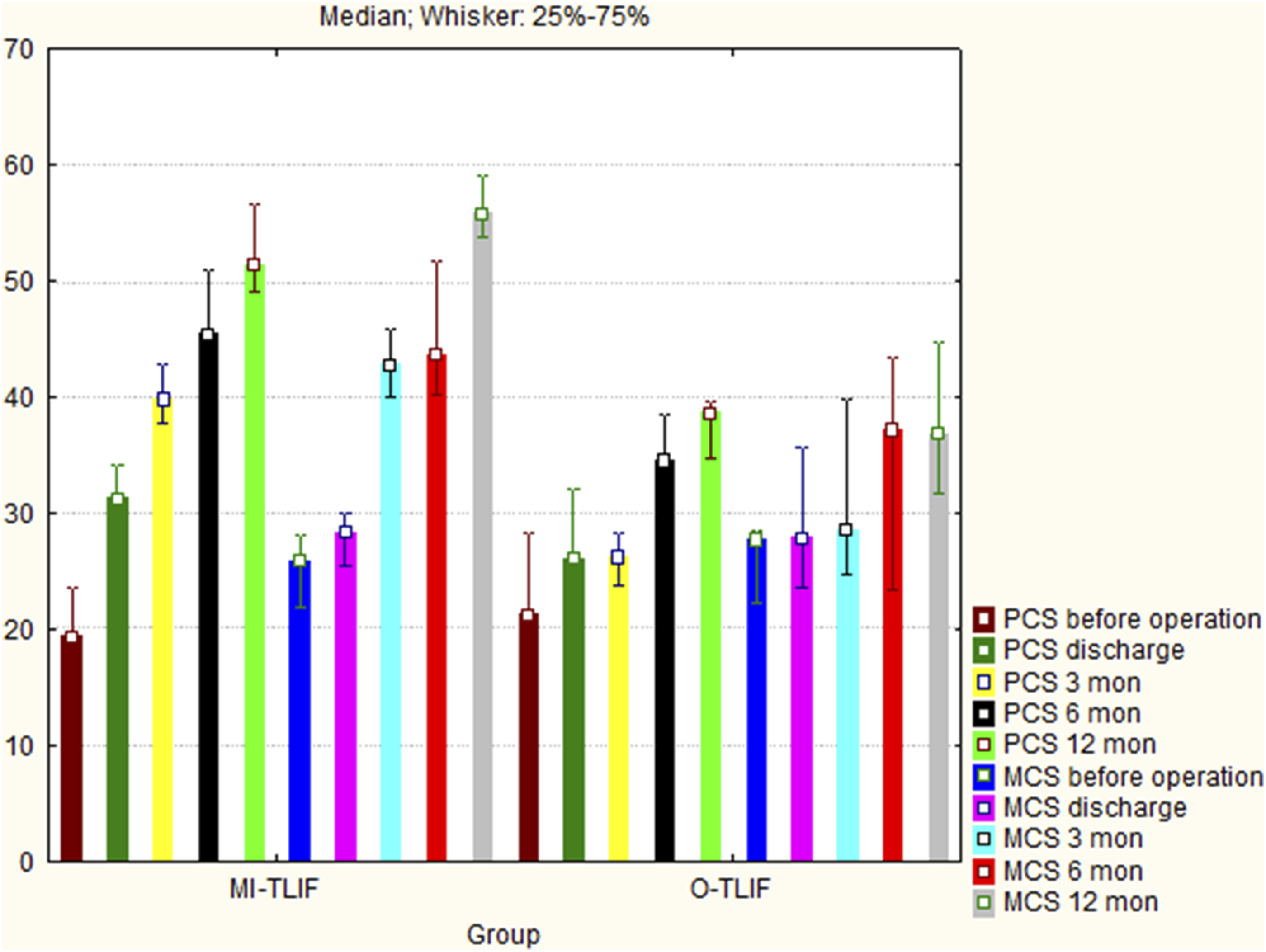
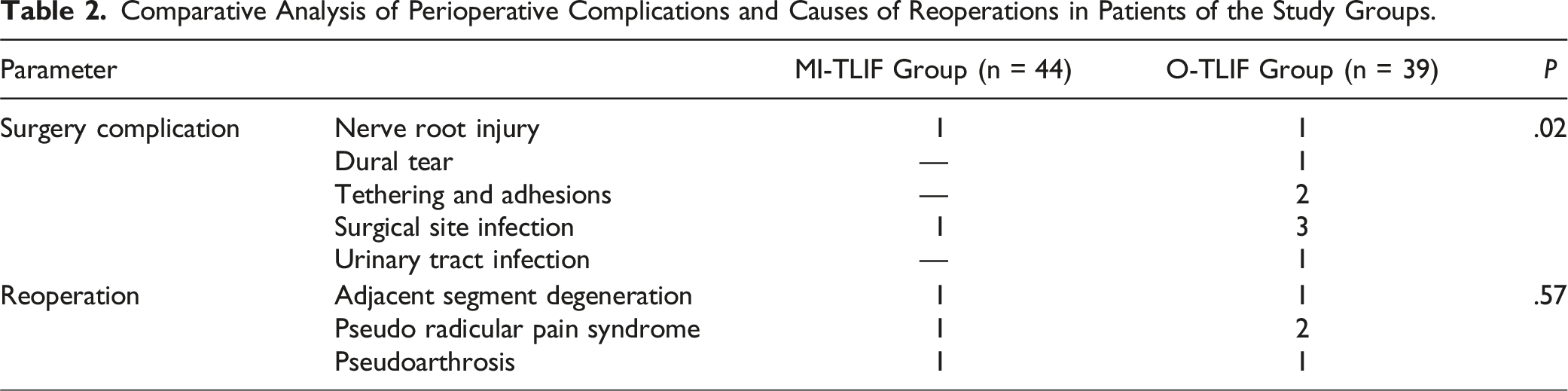
Comparative Analysis of Perioperative Complications and Causes of Reoperations in Patients of the Study Groups.
Inter-observer agreement of the multifidus muscle area according to MRI based on Kappa Statistics was excellent pre-operatively − .920 + .018 (.812-1.000, 95% CI), as well as post-operatively – .806 + .042 (.718-1.000, 95% CI).
Changes of the Multifidus Muscle of the Studied Group of Patients.

Inter-observer agreement of the Bridwell evaluation criterion at last follow-up based on Kappa Statistics was excellent – .906 + .044 (.796-.908, 95% CI) for upper level and .872 + .016 (.770-.924, 95% CI) for lower level.
According to the Bridwell evaluation criterion of intervertebral fusion for upper level were Grade I 35 cases (79.5%) in MI-TLIF group and 30 cases of (76.9%) in O-TLIF group, Grade II were 9 cases (20.5%) in MI-TLIF group and 9 cases (23.1%) in O-TLIF group (P = .77); for lower level were Grade I there were 34 cases (77.3%) in MI-TLIF group and 28 cases of (71.8%) in O-TLIF group, Grade II were 10 cases (22.7%) in MI-TLIF group and 11 cases (28.2%) in O-TLIF group (P = .56).
Time to Return to Work (in Days) and Return to Work Rate at 1 year Stratified by Workload and Surgical Procedure.
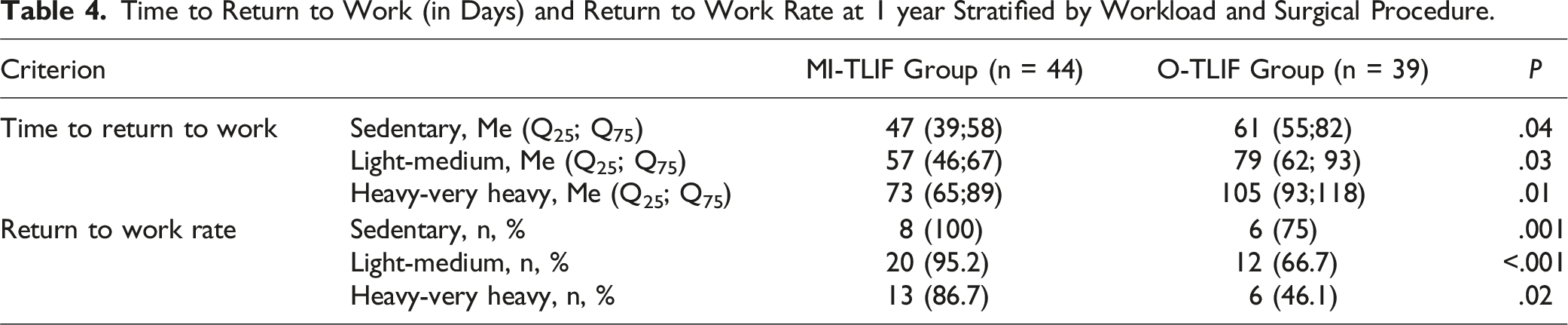
The overall return to work rate in this study for MI-TLIF was 93.2% and for O-TLIF was 61.5% - 41 patients and 24 patients, respectively, returned within 1 year after surgery. In a comparative analysis, depending on the workload, a statistically significantly higher return to work rate was found after MI-TLIF compared with O-TLIF (P < .05).
Discussion
Lumbar degenerative scoliosis with stenosis or spondylolisthesis is often associated with radicular pain syndrome, which significantly reduces the quality of life of patients. If conservative treatment is ineffective, fusion surgery is indicated. 15 Compared to open procedures, MI-TLIF techniques have been associated with less damage to paravertebral tissues, early functional recovery, better clinical outcome and decreased postoperative pain.16,17
Railway workers are a special group of patients with a high baseline level of physical activity. Employees and employers are highly motivated to return workers to their previous functional state in the shortest possible time without worsening their work performance. 18 Inability to work due to degenerative spine disease greatly impacts the psychological, social and financial well-being of railway workers. 11 To our knowledge, this is the first study to report the rate and time to return to work based on workload intensity in railway workers who have undergone two-level lumbar spine surgery.
There are few studies describing work-intensity recovery. Singh S. et al 7 reported on return-to-work rates 1 year after fusion surgery. Depending upon their levels of physical work requirements, return to work rates were as follows: 80% for sedentary, 79% for light-medium, and 73% for heavy-very heavy physical labor. Median time to return to work was between 70-97 days (10-14 weeks) following fusion and did not vary significantly based on the anticipated workload.
It has been established that heavy physical activity prolongs the time to return to work and the duration of disability after lumbar spine surgery.19,20 Therefore, spinal surgeons use their recommendations to return to professional duties, depending on the type of operation and the requirements of the workplace.21,22 For fusion surgeries, most surgeons recommended 7-12 weeks off work before returning to a sedentary to light-moderate workload job, and 12-24 weeks off work for a heavy-very heavy workload job. 7
MI-TLIF has been demonstrated to be superior to O-TLIF for degenerative spinal conditions, causing less iatrogenic damage to paravertebral tissues and postoperative muscular atrophy, better functional outcomes and a shorter rehabilitation period.2,3 In addition, meta-analyses show that the long-term clinical and radiological results of MI-TLIF and O-TLIF are comparable.4,23 However, to our knowledge, there is minimal data regarding the difference in return-to-work rates between MI-TLIF and O-TLIF. 7
We found that both MI and O-TLIF procedures for two-level lumbar degenerative disease had comparable need for additional procedures (P = .57). The use of MI-TLIF compared favorably to O-TLIF with improved long-term ODI (P = .03), back pain (P < .001), leg pain (P < .001), SF-36 (P < .001), as well as reduction in atrophy of the multifidus muscle (52.2% vs 12.4%, respectively, P < .001) with fewer surgical complications (20.5% vs 4.5%, P = .02, respectively) compared with the O-TLIF. After MI-TLIF procedure, depending on the workload, patients had a statistically significantly faster time to return to work (P < .05) and statistically significantly higher return-to-work rates compared with O-TLIF (P < .05).
Limitations
The main limitations of this study were: (1) single center nature of the study; (2) study subjects primarily composed of a unique, relatively homogeneous population of railway workers with risky, strenuous labor responsibilities; (3) relatively short follow-up period of 1-year; (4) only two decompression and decompression-stabilization techniques; (5) only patients who were working before surgery (since this was the only group for which we could obtain the workload information needed to stratify the 3 cohorts) so our results may not be applicable to patients who were not working pre-operatively; (6) information on post-operative rehabilitation and overall post-operative management were not available so the effect of rehabilitation could not be included.
Despite these limitations, the strengths of the study include its 1-year follow-up on a large population of patients, with randomized treatment, with a single diagnosis, treated by a single team without numerous confounding variables.
Conclusion
Our results suggest that both methods of rigid stabilization are highly effective in improving clinical results at 1 year follow-up in railway workers. However, the MI-TLIF technique has statistically significant advantages in the level of back pain and leg pain, restoration of the functional state and quality of life compared to O-TLIF. In addition, after minimally invasive surgery, there was a shorter time of disability and a higher return-to-work rate, which is most likely due to decreased muscle atrophic changes and a lower rate of surgery complications compared with open surgical techniques.
Footnotes
Authors Contributions
Each author made significant individual contributions to this manuscript. VAB (0000-0003-4349-7101)*, AAK (0000-0002-6059-4344)*, YYP (0000-0001-7076-571X)* and KDR (0000-0003-2083-9375)* were the main contributors to the drafting of the manuscript. VAB, AAK, YYP, DVH (0000-0001-8112-1645), RAK (0000-0003-4160-3177) and MYB (0000-0003-4821-2654)* evaluated the data from the statistical analysis. VAB, AAK, YYP and KDR performed the literature search and review of the manuscript, and contributed to the intellectual concept of the study. *ORCID (Open Researcher and Contributor ID).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.