
Abstract
Study Design
Retrospective comparative study.
Objectives
This study aimed to determine whether the severity of preoperative gait disturbance remains after surgical resection in patients with intramedullary spinal cord tumors (IMSCTs), and to identify any factors influencing poor improvement in postoperative gait disturbance.
Methods
The study included a total of 128 patients with IMSCTs requiring surgical excision between 2006 and 2019. Based on the degree of preoperative gait disturbance assessed by the modified McCormick scale (MMCS) grade, patients were categorized into Mild (I-II) and Severe (III-V) groups. The mean postoperative follow-up period was 55.5 ± 34.3 months, and demographic and surgical characteristics were compared between the two groups.
Results
Significant differences were observed in age at surgery, tumor location, tumor size, estimated blood loss, intraoperative motor-evoked potential disappearance, extent of resection, and tumor histopathology between the Mild and Severe groups. In the Mild group, at the final follow-up, only 7.3% of patients experienced improvement, 56.0% showed no changes, and 36.7% experienced deterioration. Conversely, in the Severe group, 26.3% of patients experienced improvement, 31.6% showed no changes, and 42.1% experienced deterioration. Tumor location and age at surgery were identified as factors correlated with poor improvement in postoperative gait disturbance in the Mild group.
Conclusions
Irrespective of the preoperative gait disturbance degree, approximately 40% of patients with IMSCTs experienced deterioration in gait after tumor resection. For preoperative MMCS grade I-II cases, older age at surgery and thoracic IMSCTs would be important factors associated with poor improvement in postoperative gait disturbance.
Keywords
Introduction
Intramedullary spinal cord tumors (IMSCTs) are relatively rare, with an incidence of approximately 1.1 cases per 100 000 people, constituting 2-4% of all neoplastic lesions in the central nervous system.1-3 The majority of these tumors necessitate treatment due to the manifestation of sensory and/or motor disorders, including pain, numbness, muscle weakness in the extremities and trunk, and gait disturbances. Specifically, the onset of gait disturbance and the progression of lower limb paralysis in the preoperative period significantly diminish the patient’s quality of life, representing a serious condition.4-7 Despite surgical resection being the primary treatment for IMSCTs, concerns arise due to the tumor’s origin from the intramedullary spinal cord, raising apprehensions about the surgical procedure potentially invading the normal spinal cord and exacerbating postoperative neurological symptoms.5,8,9 The decision on whether to perform surgical resection when preoperative neurological symptoms are mild or more severe, such as the presence of gait disturbance, remains inconclusive and requires careful consideration.
Recent studies have reported surgical outcomes for each histological type of IMSCTs and the prognostic factors influencing them, highlighting tumor histology as the most critical predictor of neurological outcomes after surgical resection.10-16 However, these reports have predominantly focused on individual histological types, with only a limited number providing a comprehensive analysis of all histological types together. In addition, they did not specifically address preoperative degree of gait disturbance and solely evaluated the involvement of preoperative neurological status. Therefore, evaluating the postoperative progression in patients with IMSCTs, particularly those with mild or severe preoperative gait disturbance, and comprehending the factors influencing the exacerbation of postoperative gait disturbance, are crucial for confirming the advantages of surgical procedures in this patient population.
The objective of this study was to examine the surgical and clinical outcomes following tumor resection in patients with IMSCTs, and to evaluate whether the severity of preoperative gait disturbance remains postoperatively.
Materials and Methods
Study Design, Participant Demographics, and Characteristics
This retrospective comparative study included consecutive 128 patients with primary IMSCTs at the cervical level (central region between C1 and C7) or thoracic area (T1 to T12), requiring surgical excision at our institution between 2006 and 2019. The inclusion criteria were as follows: 1) patients diagnosed with IMSCTs who underwent tumor resection without facetectomy or fixation with spinal instrumentation, 2) those without neuromuscular disorders, trauma, congenital vertebral deformity, or other pathological conditions, 3) those without a previous history of spinal surgery, and 4) those with a minimum of 3-year follow-up after tumor resection. Patients who underwent postoperative radiotherapy/chemotherapy or had a dumbbell-shaped tumor, intradural extramedullary spinal cord tumor, or extradural spinal cord tumors, such as metastatic tumors, were excluded. All surgeries for the resection of IMSCTs were conducted by the same skilled orthopedic spine surgical team. In our institute, for cases of IMSCTs confined within five vertebral bodies, tumor removal is performed only by decompression without spinal fixation. As all eligible patients with IMSCTs met these conditions, no cases were treated with spinal fusion. Intraoperative motor evoked potentials (MEP) were necessarily performed at the time of tumor removal for all patients with IMSCTs in the study, irrespective of tumor localization or size. Data on demographic characteristics (age at surgery, sex), imaging findings (tumor location, size [sagittal, axial view max]), and surgical characteristics (surgical time, estimated blood loss [EBL], approach for tumor resection, intraoperative MEP disappearance, resection, and histopathology of tumor) were retrospectively obtained by reviewing patients’ medical records and magnetic resonance imaging (MRI) findings.
This study received approval from the Ethics and Institutional Review Board at Keio University School of Medicine (Approval number: #20110142), and all participants provided their informed consent for inclusion in the study before undergoing tumor resection.
MRI Results
Preoperative MRI was conducted to validate the extent of tumor location and size. The maximum size of each IMSCT was examined on sagittal or axial views on T2-weighted MRI. An orthopedic spine surgeon not directly involved in the surgeries measured the tumor size at three different time points. The average of these measurements was used as the tumor size. The intraobserver reliabilities, examined using the intraclass correlation coefficient (ICC) (1, 1) and ICC (1, 3) formulas, were 0.86 and 0.95, respectively. To examine interobserver error, 100 randomly chosen axial MRI findings were independently evaluated by three orthopedic spine surgeons not directly involved in the surgeries. The interobserver reliabilities, tested using the ICC (2, 1) and ICC (2, 3) formulas, were 0.85 and 0.94, respectively. Postoperatively, MRI was performed to confirm the extent of tumor resection, categorized into two types according to the operative records: gross total resection (GTR) and partial resection (PR). The standard definition of GTR was employed, indicating complete removal of the tumor, confirmed by the absence of microscopic remnants and no neoplasm at the tumor’s origin site. Conversely, PR was defined when a small tumor fragment or an extraforaminal or paravertebral portion remained unexcised, based on the documented removal of 50% to 99% of the tumor, as confirmed by intraoperative ultrasonography or postoperative MRI findings. 17 An independent radiologist from our institution reviewed the MRI images each time to evaluate the extent of tumor resection.
Assessment of Neurological Function and Clinical Outcomes
All patients with IMSCTs in this study were evaluated for the degree of gait disturbance at “pre-operation,” “immediately after surgery,” and “the final follow-up” using the modified McCormick scale (MMCS; grade I, normal gait; grade II, mild gait disturbance not requiring support; grade III, gait disturbance requiring support; grade IV, with assistance; and grade V, wheelchair needed).18,19 Additionally, to determine whether the degree of preoperative gait disturbance can affect clinical outcomes after surgery, the participants were divided into two groups according to preoperative MMCS. Patients with preoperative MMCS grade I-II were included in the Mild group, while patients with preoperative MMCS grades III-V were assigned to the Severe group. The outcome variables were compared between the two groups, and changes in postoperative MMCS were analyzed.
Statistical Analysis
All data were presented as mean ± standard error of mean, and categorical variables were expressed as percentages. Demographic and surgical characteristics data based on the degree of preoperative gait disturbance were compared at “preoperation,” “immediately after surgery,” and “the final follow-up” using the Kruskal–Wallis test, followed by the Dunn test for multiple comparisons. The Mild and Severe groups were assessed using the Mann–Whitney U test or Fisher’s exact test, respectively. A P-value of <0.05, <0.01, or <0.001 was considered statistically significant. Additionally, univariate analysis was conducted on all variables to identify potential factors influencing improvement in postoperative gait disturbance in the Mild group. Variables with a P-value of < 0.25 in the univariate analysis were included in the multiple logistic regression analysis. P-values of < 0.05 with a 95% confidence interval were considered statistically significant in the univariate and multivariate logistic regression analyses. All statistical analyses were performed using Statistical Package for the Social Sciences software version 29.0 (IBM Corp., Armonk, NY, USA).
Results
Demographic and Clinical Characteristics of all Patients With IMSCTs.
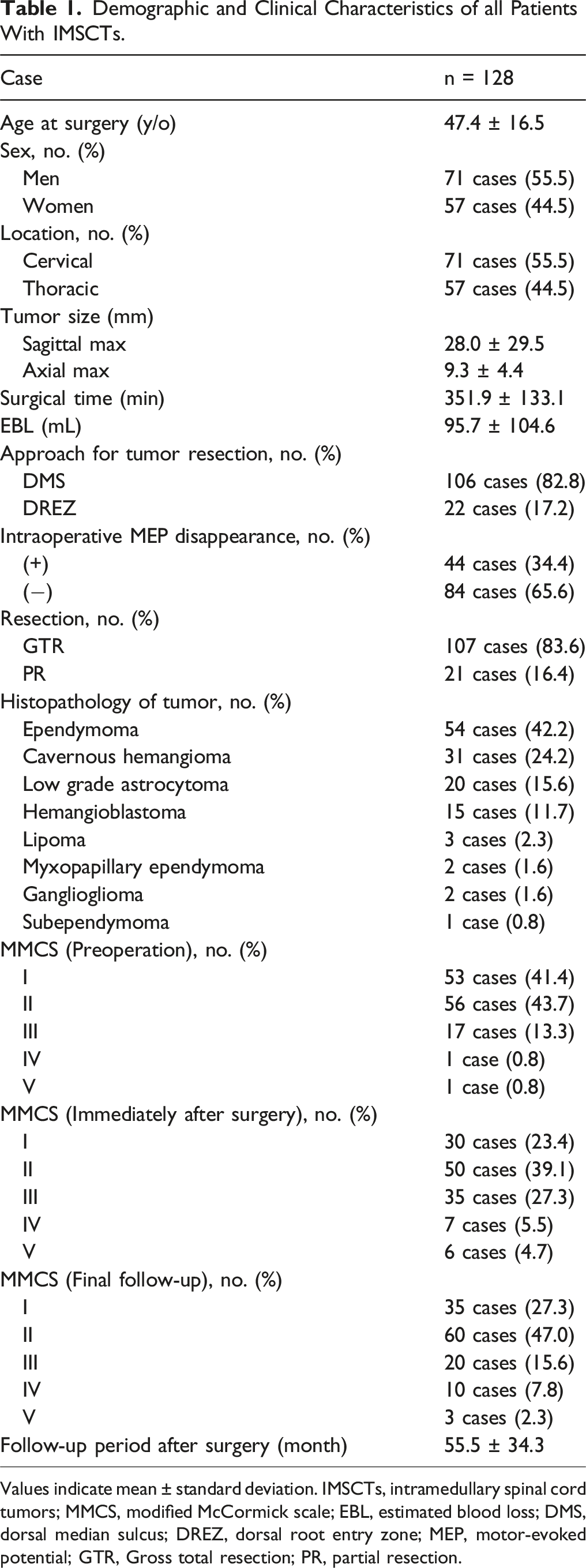
Values indicate mean ± standard deviation. IMSCTs, intramedullary spinal cord tumors; MMCS, modified McCormick scale; EBL, estimated blood loss; DMS, dorsal median sulcus; DREZ, dorsal root entry zone; MEP, motor-evoked potential; GTR, Gross total resection; PR, partial resection.
Comparison of Demographic and Surgical Data According to the Degree of Preoperative Gait Disturbance in Patients With IMSCTs.
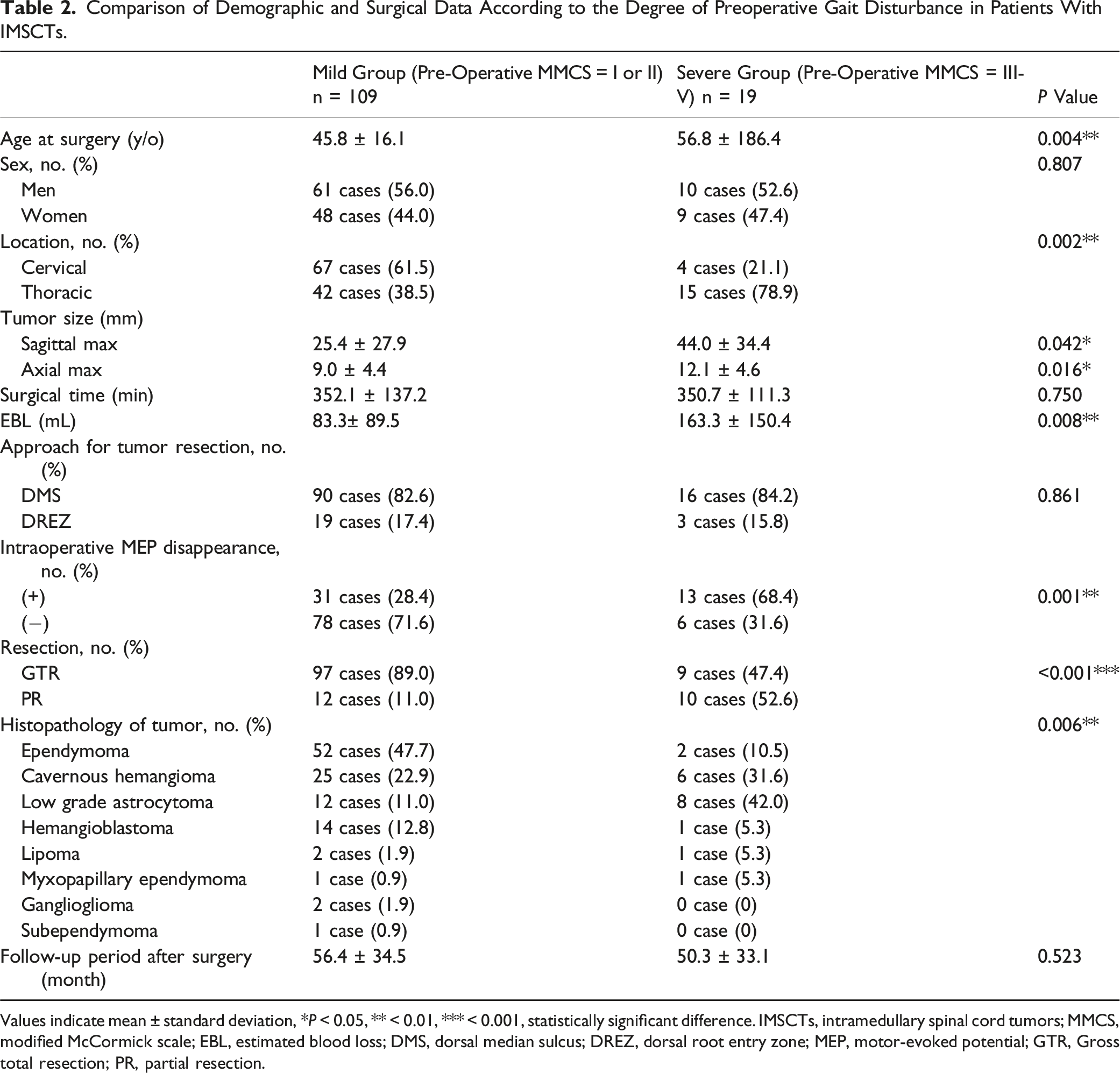
Values indicate mean ± standard deviation, * P < 0.05, ** < 0.01, *** < 0.001, statistically significant difference. IMSCTs, intramedullary spinal cord tumors; MMCS, modified McCormick scale; EBL, estimated blood loss; DMS, dorsal median sulcus; DREZ, dorsal root entry zone; MEP, motor-evoked potential; GTR, Gross total resection; PR, partial resection.
Summary of Changes in MMCS Grade Immediately After Surgery and the Final Follow-Up in Patients With IMSCTs.
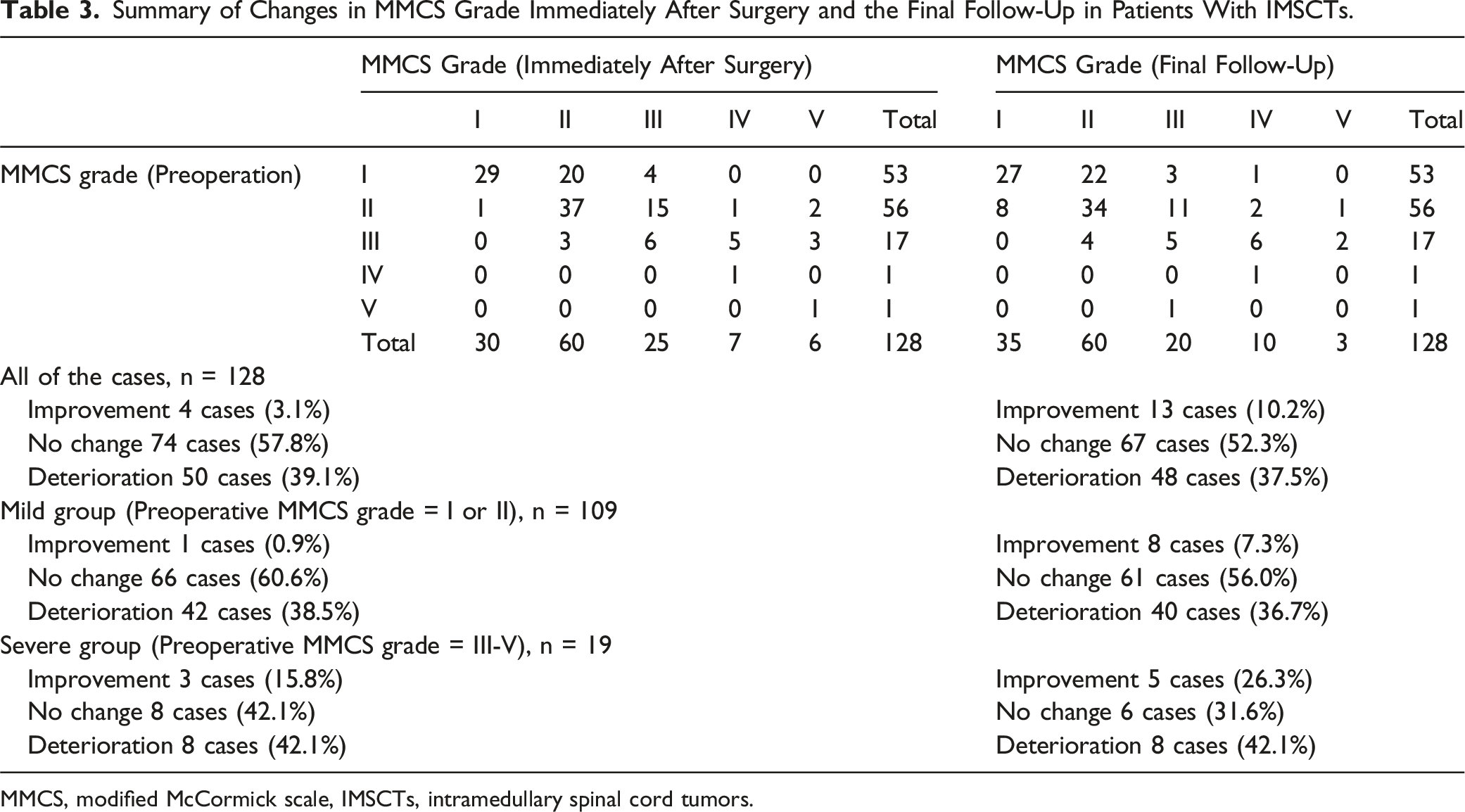
MMCS, modified McCormick scale, IMSCTs, intramedullary spinal cord tumors.
Univariate Analysis for Possible Factors Affecting Residual Gait Disturbance After Tumor Resection in the Mild Group.
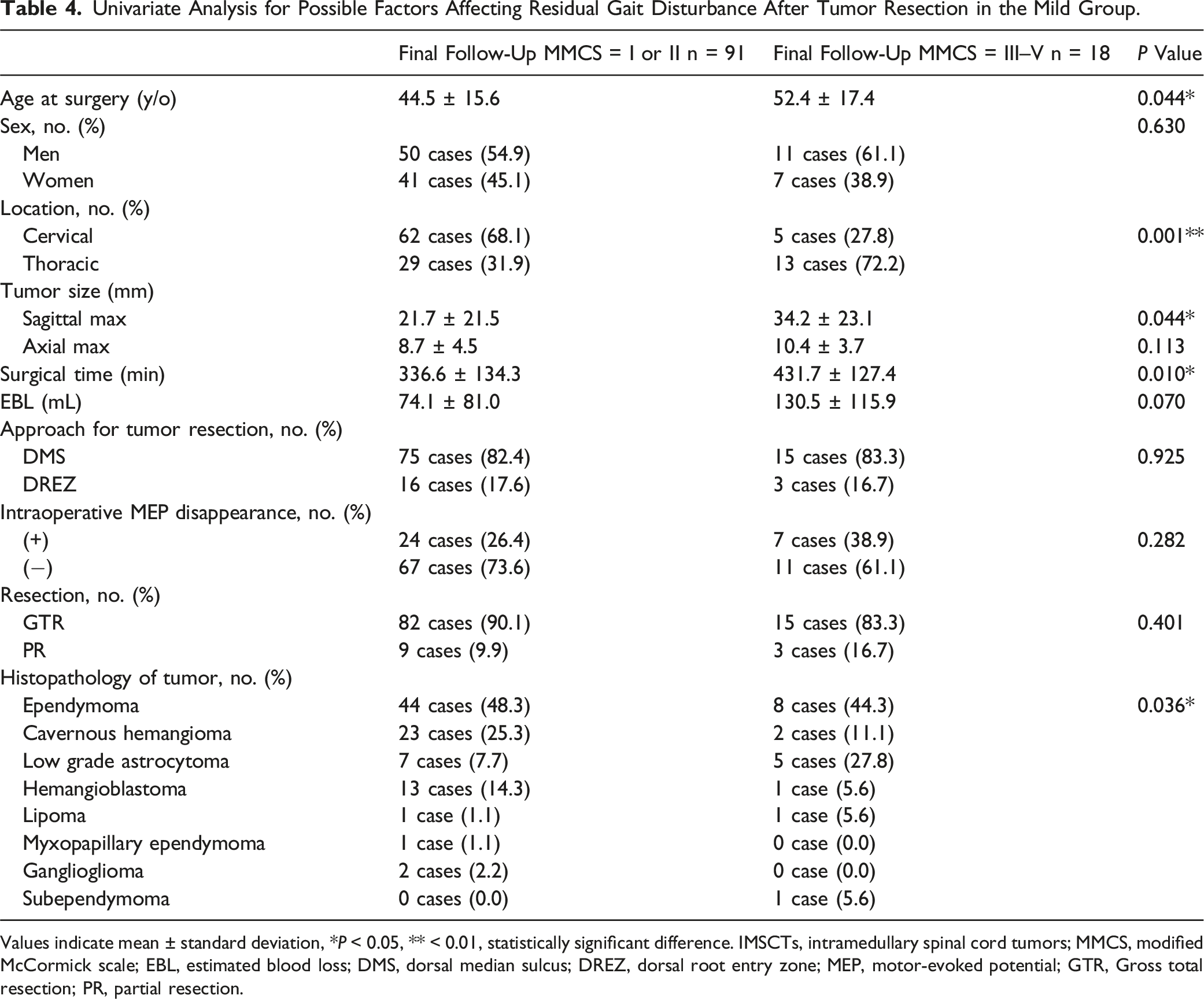
Values indicate mean ± standard deviation, * P < 0.05, ** < 0.01, statistically significant difference. IMSCTs, intramedullary spinal cord tumors; MMCS, modified McCormick scale; EBL, estimated blood loss; DMS, dorsal median sulcus; DREZ, dorsal root entry zone; MEP, motor-evoked potential; GTR, Gross total resection; PR, partial resection.
Multivariate Logistic Regression Analysis of MMCS in the Mild Group at the Final Follow-Up.
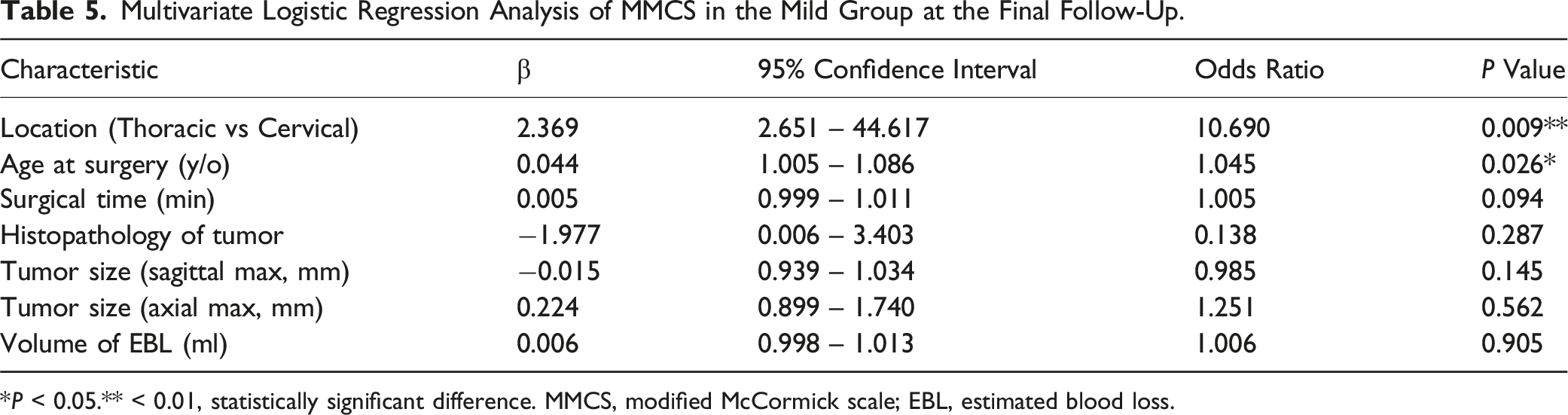
*P < 0.05.** < 0.01, statistically significant difference. MMCS, modified McCormick scale; EBL, estimated blood loss.
Comparison of Postoperative Outcomes According to the Severity of Preoperative Gait Disturbance in Patients With Cervical or Thoracic IMSCTs.
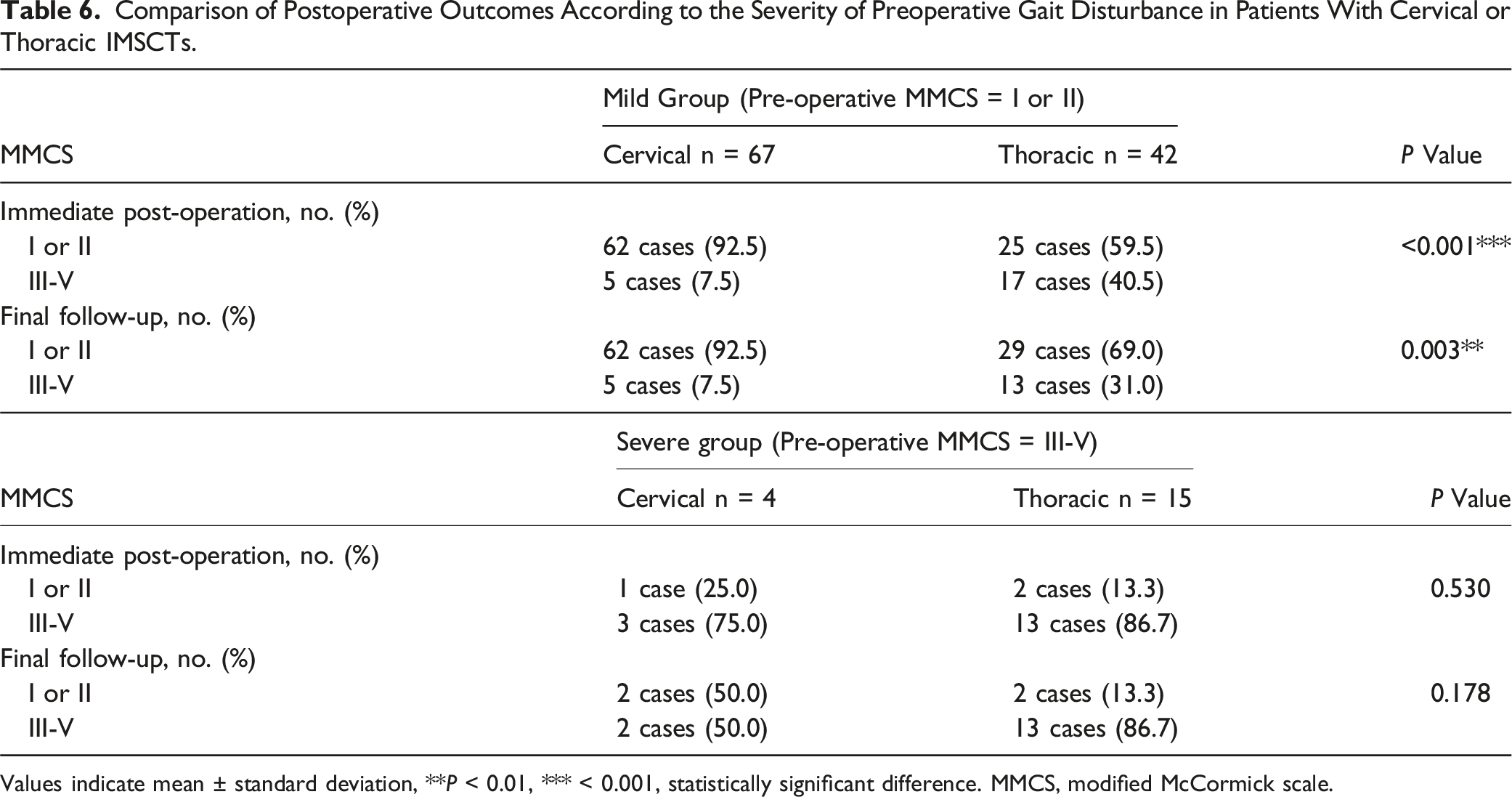
Values indicate mean ± standard deviation, **P < 0.01, *** < 0.001, statistically significant difference. MMCS, modified McCormick scale.
Discussion
The present study investigated whether the severity of preoperative gait disturbance remains after tumor resection in patients with IMSCTs using the MMCS grade. At the final follow-up, 74.2% of patients with IMSCTs were capable of walking without support. However, concerning the improvement of gait disturbance, only 10.2% of all cases demonstrated improvement, while the remaining 89.8% either remained unchanged or worsened. Specifically, 39.1% of patients with IMSCTs experienced gait disturbance immediately after surgery, and 37.5% of the patients continued to experience gait disturbance at the final follow-up. Additionally, tumor location and age at surgery were identified as factors influencing poor improvement in postoperative gait disturbance in patients with IMSCTs who had mild gait disturbance preoperatively. Our findings bear significant implications for studies investigating the efficacy of tumor resection, as few studies have comprehensively examined changes in postoperative neurological status based on the degree of preoperative gait disturbance in patients with IMSCTs.
To date, numerous studies have described the pathogenesis, treatment, and surgical outcomes of IMSCTs.3-9 In a retrospective review focused on cervical IMSCTs, Xu et al 20 observed improved neurological outcomes in 77.6% of their study patients. Karikari et al 3 noted that there was no statistically significant difference in functional outcomes based on tumor location. Baig et al demonstrated that IMSCTs spanning a greater number of vertebral levels were significantly associated with poor MMCS outcomes. They also found that the presence of pre-operative gait disturbance was related to unfavorable outcomes in both postoperative MMCS and Nurick scores. 4 Suzuki et al 7 showed that the higher the lower-limb function scores in the early phase, the better the improvement in walking ability was predicted 1 year after IMSCTs resection. Endo et al 5 reported that 251 patients with IMSCTs showed improvement, 500 remained unchanged, and 160 experienced worsened MMCS grades after 6 months postoperatively. Conversely, Alizada et al 6 found that despite immediate postoperative worsening of neurological status, a great number of patients with IMSCTs showed improvement at the last follow up. However, only a limited number of reports have comprehensively summarized postoperative changes in neurological status based on preoperative gait disturbance or clearly indicated the presence or absence of changes in gait disturbance after surgical resection. Furthermore, the factors influencing postoperative MMCS grade have not been fully elucidated. Therefore, this study assessed in detail whether the severity of preoperative gait disturbance affects changes in neurological status after surgery by comparing patients with IMSCTs in the Mild and Severe groups.
Most IMSCTs belong to histological types such as ependymomas and astrocytomas, but there are also various other types, including cavernous hemangiomas and hemangioblastomas.10-18 Alhalabi et al 10 found that the presence of gait disturbance or ataxia increased the risk of incomplete long-term recovery after spinal ependymoma resection. Tsuji et al 11 identified worse preoperative MMCS as independent risk factors for motor deterioration after ependymoma resection. Eroes et al 13 highlighted that an MMCS of less than 3 and a tumor extent of less than 5 levels were crucial factors for a favorable postoperative functional outcome in low-grade astrocytoma and ependymoma. Nagoshi et al 15 demonstrated that among patients with cavernous hemangiomas, those with unstable gait prior to surgery had a higher frequency of hemorrhagic episodes, as assessed by the MMCS. Schwake et al 16 reported that surgery on patients with hemangioblastomas displaying no or minor neurological deficits (MMCS grade I or II) was associated with a favorable postoperative outcome and overall higher quality of life compared to those with severe neurological deficits (MMCS grade III or IV). While the above results focus on specific histological types of IMSCTs, in a comprehensive review of IMSCTs as a whole, Karikari et al 3 showed that tumor histology played a predictive role in functional neurological outcomes, suggesting that most patients with non-astrocytic IMSCTs undergoing surgical resection would maintain their neurological status. Endo et al 5 reported that the histopathological type of IMSCTs was a significant factor associated with mortality and functional outcomes. However, in this study, the histopathology of the tumor was not a factor influencing residual gait disturbance after tumor resection in the Mild group. This difference may be attributed to the study’s focus on the Mild group, as its purpose was to determine whether the severity of preoperative gait disturbance remains after tumor resection. Another possibility is the exclusion of cases where only a biopsy was performed (eg, high-grade astrocytoma), despite no significant difference in tumor histology between the Mild and Severe groups.
Recently, several reports have assessed the clinical characteristics of pediatric IMSCTs and identified differences between pediatric and adult cases.21-23 McGirt et al noted that approximately one-third of pediatric patients might experience improvement in motor, sensory, and urinary dysfunction years after IMSCTs resection, whereas the majority would continue to experience long-term dysesthetic symptoms. 21 Ahmed et al 22 described that pediatric IMSCTs patients with MMCS grade I at presentation were more likely to show functional improvement by final follow-up compared to those with MMCS Grades II-V. Umebayashi et al 23 found that preoperative MMCS were compatible between pediatric and adult patients with IMSCTs. The proportions of patients with MMCS grade V neurological function increased immediately after surgery, while the proportions of those with MMCS grade I and II neurological function increased as well. Postoperative deterioration of MMCS at discharge was more common in pediatric patients than in adult. In contrast, Pennington et al 24 suggested that advanced age (≥ 63 years) and worse baseline neurological function were the strongest predictors of long-term neurological worsening. Tsuji et al 11 reported that age at surgery was independent risk factors for motor deterioration after ependymoma resection. In our current study, multivariate logistic regression analysis revealed that age at surgery influenced residual gait disturbance after IMSCTs resection in the Mild group. The reasons for these results include the fact that there were only six cases of pediatric IMSCTs patients in this study, which is extremely low. Additionally, in the Severe group, there was a relatively high proportion of elderly individuals aged 65 and above, with 8 out of 19 cases (42.1%). Therefore, based on the results of this study, further research should be validated in the future, including more pediatric patients, regarding whether postoperative MMCS for each age group will be changed over long-term periods.
In patients with spinal cord tumors, the MMCS serves as the standard clinical outcome tool—a physician-rated assessment encompassing global functional impairment, including neurological status and walking ability.17-19 While there is a growing emphasis on employing patient-rated outcome measures to evaluate clinical outcomes in various spinal surgeries, a limited number of reports have explored postoperative neurological symptoms using patient-rated outcome scales specifically in IMSCTs resection surgery.25-28 Nakamura et al demonstrated that all 36-item Short-Form (SF-36) Health Survey subscores of the patients with IMSCTs were significantly lower than the national average, postoperatively. They also identified a significant negative correlation between SF-36 and Neuropathic Pain Symptom Inventory (NPSI) subscores. 25 Myrseth et al 26 similarly discovered significantly lower SF-36 results across all five subdomains related to physical function, while scores for mental health and role emotional showed no significant differences compared to Norwegian norms. Xiao et al 27 reported no significant changes between preoperative and postoperative EuroQol 5-Dimensions (EQ-5D), Pain Disability Questionnaire (PDQ), or Patient Health Questionnaire-9 (PHQ-9). Tufo et al 28 highlighted a significant interaction between MMCS grade and scores on the Pain Catastrophizing Scale (PCS) and Pittsburgh Sleep Quality Index (PSQI). Higher MMCS grades were associated with increased pain perception and poor sleep quality perception long after surgery. Simultaneously, SF-36 subscales exhibited a significant interaction with the degree of the role-physical subscale, correlating lower scores with MMCS grades II and III. Unfortunately, in this study, postoperative outcomes for patients with IMSCTs were assessed solely using the physician-rated MMCS. Consequently, direct comparisons with patient-rated outcomes like SF-36, NPSI, EQ-5D, and others could not be made. To comprehensively gauge the impact of the disorder on QOL and daily functioning, it is imperative to evaluate outcomes from the patient’s perspective. Additionally, for future research, we believe that more comprehensive clinical studies should be conducted with larger sample sizes and evaluations from the patient’s perspective, using patient-rated questionnaires. This approach would offer a more thorough assessment of clinical outcomes associated with the surgical resection of IMSCTs.
Our study had several important limitations that should be considered. First, the retrospective design of the study inherently reduced the level of evidence. Second, the sample size was relatively small, and the statistical power was not robust enough to draw definitive conclusions regarding accurate clinical outcomes in patients with IMSCTs. Third, the patients with IMSCTs included in this study underwent tumor removal within approximately one year of symptom onset. Unfortunately, due to the absence of data on patients experiencing symptoms for more than one year, we were unable to explore the relationship between symptom duration and postoperative neurological outcomes. Finally, the surgical outcomes may have been influenced by the diverse techniques, experiences, and skills of the four orthopedic spine surgeons who performed IMSCTs resection. Despite these limitations, the current study can provide important insights into the surgical and clinical outcomes of tumor resection in patients with IMSCTs, particularly based on the severity of preoperative gait disturbance. This study is primarily focused on novel analyses that center on the postoperative course of patients with IMSCTs who exhibit mild or severe preoperative gait disturbance.
Conclusion
Here, in the present study, with a focus on the severity of preoperative gait disturbance, we performed a follow-up study on 128 patients with IMSCTs to evaluate postoperative clinical outcomes. At the final follow-up, 74.2% of patients with IMSCTs could walk without support. However, only 10.2% showed improvement in gait disturbance, while 89.8% either remained unchanged or worsened. Specifically, 39.1% of patients with IMSCTs experienced immediate postoperative gait disturbance, and 37.5% continued to experience it at the final follow-up. Factors influencing poor improvement in postoperative gait disturbance in patients with mild preoperative gait disturbance included tumor location and age at surgery. The results of this study will provide valuable information for patients with IMSCTs considering tumor resection, particularly regarding postoperative outcomes and potential complications. They will also assist spine surgeons in explaining surgical plan and clinical outcomes, such as during preoperative informed consent with IMSCTs patients. While the current study involved a relatively small number of patients, future research with a larger sample size is warranted to yield more precise and comprehensive conclusions.
Footnotes
Acknowledgments
The authors would like to express our gratitude to Dr Hirokazu Fujiwara, the radiologist from our institution, for evaluating the extent of tumor resection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.