
Abstract
Study Design
Retrospective single-center multi-surgeon cohort study.
Objectives
Compare the post-operative changes in the compensatory mechanisms of the sagittal balance according to the type of pelvic fixation: S2-Alar-iliac screws (S2AI) vs iliac screws (IS) in patients with Adult spine deformity (ASD).
Methods
ASD patients who underwent spino-pelvic fixation and remained with a PI-LL >10° mismatch post-operatively were included. Pre-operative and 1-year-follow-up PI, Lumbar lordosis (LL), pelvic tilt (PT), sacral slope (SS), thoracic kyphosis (TK), femur obliquity angle (FOA), knee flexion angle (KFA) and ankle flexion angle (AFA) were analyzed on EOS imaging. Patients were categorized based on their pelvic fixation type (S2AI vs IS), and the pre-operative to 1-year-post-operative changes (ΔX°) in the compensatory mechanisms were compared between groups.
Results
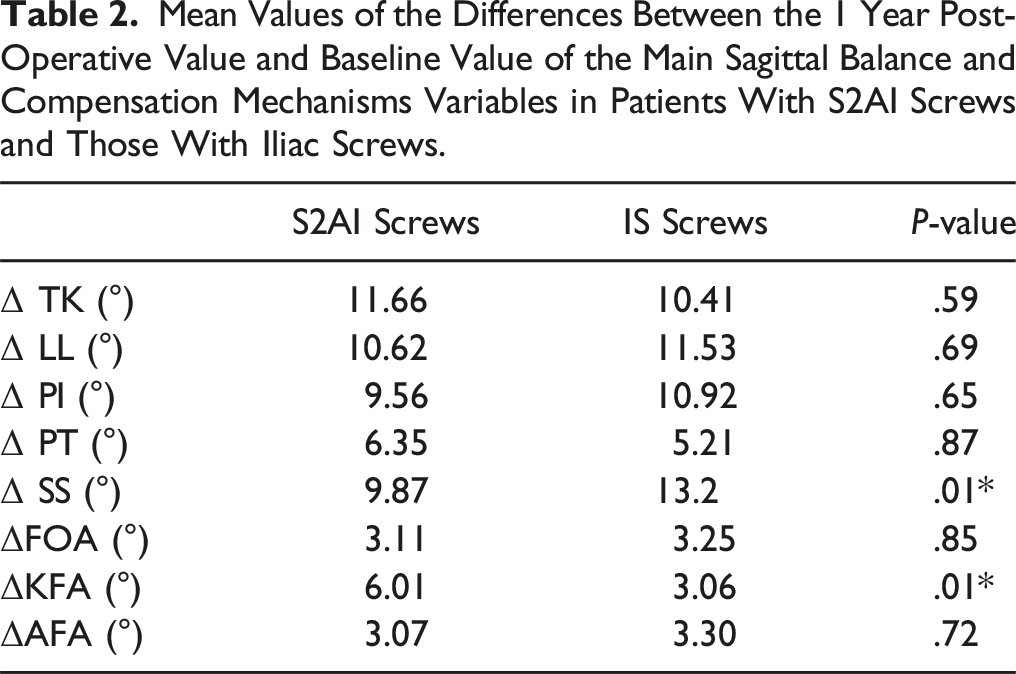
Patients with S2AI (n = 53) and those with IS (n = 26) screws were comparable at baseline. ΔSS averaged 9.87° in the S2AI compared to 13.2° in the IS (P = .001), whereas the ΔKFA reached 6.01° in the S2AI as opposed to 3.06° in the IS (P = .02). The ΔPT was comparable between both groups (6.35°[S2AI group] vs 5.21°[ISgroup], P = .42). ΔTK, ΔLL, ΔFOA and ΔAFA were comparable between both groups.
Conclusion
The type of pelvic fixation impacts significantly the post-operative compensatory mechanisms in patients with ASD. Patients with S2AI screws are more likely to compensate their remaining post-operative PI-LL mismatch through their knees and less likely through their pelvis compared to patients with IS, despite similar changes in PT. This could be explained by an increased SI joint laxity in ASD patient and the lower resistance of the iliac connectors to the junctional mechanical stresses, allowing for sacro-iliac joint motion in patients with IS.
Introduction
Adult spine deformity (ASD) is a common, but complex, multifactorial condition occurring in as many as 68% of people over the age of 60. 1 Although the deformity caused by this disorder is multiplanar, sagittal malalignment has the greatest impact on patient pain, gait, posture and disability.2,3 Dubousset’s “Conus of economy” concept defines a chain of balance in which the head, the spine and the lower extremity attempt to maintain balance within a narrow range using a minimal muscle energy. 4 Deviations from this narrow range require increased muscle recruitment and more energy expenditure to maintain the upright standing posture. 4
During the decades following the diffusion of Dubousset’s chain of balance concept, the importance of the sagittal balance was increasingly recognized. 5 The advent of full body stereo-radiographs showed that, in response to spine malalignment, the human body recruits compensatory mechanisms to maintain the head over the pelvis and to retain a horizontal gaze. 6 This occurs through an exaggerated lordosis in the remaining mobile segments of the spine, a retroversion of the pelvis through lumbar and hip extensor muscle contraction, an increased knee flexion and an increased ankle dorsiflexion. 5 The analysis of reciprocal changes in these mechanisms showed that the relative contributions of spine, pelvis and lower extremities may vary.7-9 The few studies that evaluated the reciprocal changes of the mechanisms of compensation after ASD surgical treatment, showed that pathologic compensatory mechanisms can be reversed if adequate thoracolumbar alignment was obtained in long spinal fusion with pelvic fixation.10-13 When surgical correction for ASD is indicated after conservative interventions are exhausted, restoration of sagittal alignment is critical. 14 However, sagittal balance is not always obtained post-operatively as some patients remain unbalanced after spino-pelvic fixation for ASD.15-17 Moreover, achieving fusion remains also a challenge for spine surgeons pushing them to adopt robust pelvic fixation. 17 Modern iliac screws (IS) and S2-alar-iliac screws (S2AI) are the most popular methods of lumbo-pelvic fixation and their use is associated with reduced rates of pseudarthrosis in the lumbosacral area in patients with ASD. 18
It was recently shown that a significant proportion of patients with lumbo-pelvic fixation for ASD, had a considerable (>5°) post-operative change in their baseline PI.19-21 This was partially attributed to the use of S2AI screws.19-21 We hypothesize that the lumbo-pelvic fixation type strategy will influence the reciprocal relationship among the spine, the pelvis and the lower extremities. This is the first study to evaluate the impact of the type of pelvic fixation (IS vs S2AI screws) on the compensation mechanisms in a subset of patients who had residual sagittal imbalance after lumbo-pelvic fusion for ASD.
Methods
This retrospective study contains data that were prospectively collected in a degenerative spine surgery tertiary center. It was approved by our institution review board (IRB). Adult patients (≥18 years old) who remained with a lumbo-pelvic mismatch/malalignment [Pelvic Incidence (PI) – Lumbar lordosis (LL) > 10°] 22 1 year after a surgical correction for their ASD (minimal lumbar coronal spine deformity of 10°) with ≥3 levels fusion and lumbo-pelvic fixation were included in this study. A/P and lateral standing full body EOS imaging was performed pre-operatively and at 1 year post-operatively for all included patients. Patients with spinal deformity secondary to neuromuscular disorders, congenital syndromes, trauma and tumors were excluded, as well as those with incomplete charts.
Data collection included demographic characteristics (age, body mass index (BMI), sex and diagnosis). Surgical data collected were the upper instrumented vertebra, the type of pelvic fixation (IS vs S2AI) and the number of performed TLIFs. Pre-operative and 1 year follow-up PI, LL, thoracic kyphosis (TK), pelvic tilt (PT), sacral slope (SS), PI-LL mismatch, femur obliquity angle (FOA), knee flexion angle (KFA), ankle flexion angle (AFA) and the offset between the C7 plumb line (C7PL) and the center sacral vertical line (CSVL) (C7PL/CSVL) were analyzed on full body standing anteroposterior and standing EOS films. Measurements were performed by two independent fellowship trained spine surgeons.
The absolute value (modulus) of the difference between the 1 year post-operative value of a variable and the pre-operative value of the same variable was named ΔX(°), were X is the variable. Absolute value metric was chosen to assess the magnitude of the change in the corresponding compensation mechanism irrespective of the direction of the change.
Patients were categorized intro two groups according to the type of pelvic fixation: S2AI vs IS. The pre-operative, 1 year post-operative and ΔX(°) values were calculated for all the variables and compared between both groups.
Patients were all operated by the same group of surgeons, using similar surgical techniques, instruments and implants, except for the type of pelvic fixation that was decided per-operatively on a case by case basis, based on the patient’s anatomy and the surgeon’s judgment, without any preference between surgeons. Patients were all positioned prone on a Jackson trail table with hip extension, maximal possible lumbar lordosis and sacrum falling anteriorly with gravity. Smith-Peterson or pedicle substraction osteotomy were performed when needed to address sagittal imbalance; and circumferential interbody fusion was performed through one or multiple transforaminal lumbar interbody fusions using cages; mainly at the L4-L5 and L5-S1 levels. Sagittal cantilever technique was used at the final rod insertion to achieve satisfactory/planned lumbar lordosis. All patients in the IS group had their IS connected to the main construct using connectors. This was done to avoid extreme rod bending and bulky constructs that might impinge on the surrounding soft tissues causing secondary local symptoms.
Statistical Analysis
Descriptive analysis included demographics radiological and surgical characteristics. Differences in quantitative variables were tested using an unpaired t test. Differences in qualitative variables were tested using Chisquare test or Fisher exact test depending on the respective conditions of validity. Confidence interval for percentages was determined using Wilson’s score method. Interobserver and intraobserver reliability were evaluated using intra-class correlation coefficients (ICC). ICC >.90 was judged as excellent, .71 < ICC <.90 was good and .51<ICC <.70 was regarded as fair. All analyses were performed using the R software version 4.0.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
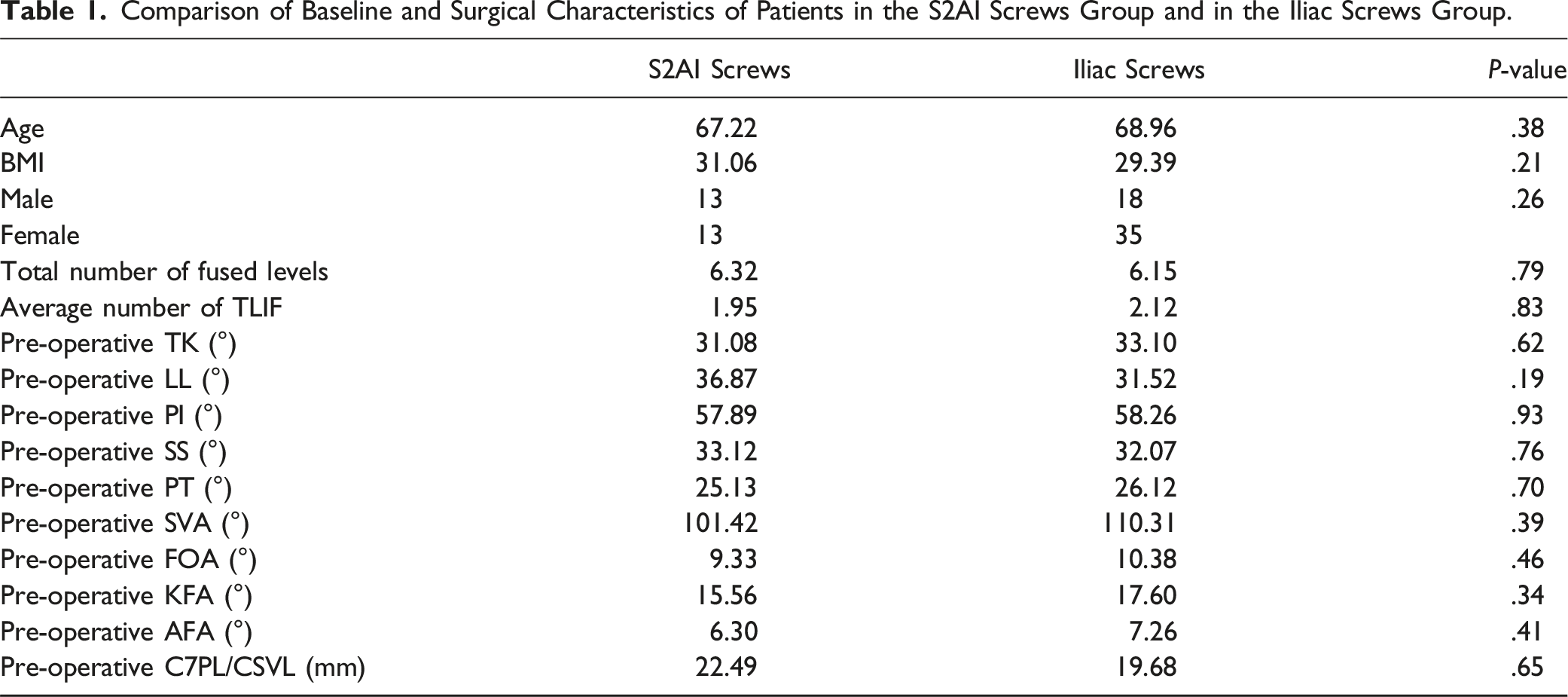
A total of 79 patients were included in this study, with a mean age of 67.8 (±8.9) years and a mean BMI of 30.52 (±5.36) kg/m2. There were 48 females (61%) and 31 males (39%).
Intra-observer reliability for all pre-operative and post-operative x-ray measurements was excellent (ICC = .91), whereas inter-observer reliability for the same measurements was good (ICC = .83). About 62% of the patients operated by the surgeon 1, 70.9% of the patients operated by surgeon 2 and 68.8% of the patients operated by surgeon 3 had S2AI screws (P = .76).
Pre-operative SVA averaged 96.79 mm (±52.27); while mean pre-operative PI was 58.01° (±15.56) mean pre-operative LL was 35.19° (±16.19) and mean pre-operated C7PL/CSVL reached 20.43 mm (±7.72). SS averaged pre-operatively 32.8° (±12.41) while PT reached 25.44° (±9.83). In the lower extremities, the mean FOA was 9.67° (±5.2), while the mean KFA reached 16.21° (±7.17) and the mean AFA reached 6.61° (±3.73). At 1 year follow-up, SVA averaged 89.77 mm (±57.08), whereas mean PI was 60.01° (±13.97) and mean LL was 38.97° (±13.07). Mean FOA reached 9.63° (±5.34), while KFA averaged 17.07° (±6.96) and mean AFA was 7.56° (±3.06).
Categorization by Type of Lumbo-Pelvic Fixation
Comparison of Baseline and Surgical Characteristics of Patients in the S2AI Screws Group and in the Iliac Screws Group.
Mean Values of the Differences Between the 1 Year Post-Operative Value and Baseline Value of the Main Sagittal Balance and Compensation Mechanisms Variables in Patients With S2AI Screws and Those With Iliac Screws.
Discussion
An adequate thoracolumbar sagittal alignment after long fusion to the sacrum/pelvis in ASD restores gradually the pathologic compensatory mechanisms in the unfused segments of the spine as well as in lower extremities. 11 Knee flexion for example was shown to decrease in a linear correlation with the optimal thoracolumbar correction achieved. However, partial rather than full resolution of the pathologic compensations were observed according to series, likely due to pathologies in the corresponding joints (contraction, osteoarthritis.) or to a pre-operative status of compensated sagittal alignment in asymptomatic adults. 11
Patients who remain in a sub-optimal sagittal correction state after surgery are expected to keep the same profile of pathologic compensatory mechanisms involvement after their “failed” surgery. However, to the best of our knowledge, these profiles were never previously analyzed post-operatively in this subset of patients with spine fusion down to the pelvis. We hypothesized that the type of pelvic fixation (S2AI vs IS screws) could influence the reciprocal changes in the unfused segments post-operatively; and proceeded with a two group comparisons of the sagittal balance and compensation mechanisms components at 1 year of follow-up. We chose to assess the outcomes at 1 year post-operatively, because despite highly variable post-operative recovery trajectories in patients with ASD, most of them reach steady state at 12 months.
Patients is both groups of this study remained with a PI-LL mismatch at 1 year of follow-up as an adequate lordosis could not be reached during the index surgery. These patients were operated by the same group of surgeons and were comparable at baseline for all the sagittal parameters of the spine and lower extremities. Post-operatively, the pathologic compensation mechanisms were not restored in both groups, as expected; however, a difference in pre-operative to post-operative variations in some parameters was recorded.
In patients with a large fixation screw transfixing the sacro-iliac (SI) joint (S2AI group), ΔKFA was significantly higher than patients with direct IS and connectors to bind them to the spinal construct (IS group). These patients had significantly more variation in pre-to post-operative knee flexion (increase or decrease) than those who received IS. Conversely, patients with IS had more variation in pre-to post-operative sacral slope (increase or decrease) compared to those who had S2AI. Pre-to post-operative variations in all the remaining parameter, mainly TK, PI and PT were comparable between both groups of this study.
In both groups, post-operative PT value was high (>25°) meaning that the pelvis is at a maximum of retroversion. More subtle changes and adaptations had to occur in the remaining unfused segments. Variations in the unfused thoracic spine were comparable between groups, however, patients in S2AI groups used more of their knees to adapt, compared to patients with IS fixation who used more of their sacrum; despite a comparable changes in pelvic tilt. This observation suggests that significantly more motion occurs in the SI joint in the patients of the IS group than the patients in S2AI group, who should amplify the modification in their KFA to compensate this lack of movement through the SI joint.
We believe that this is due mainly to an increased SI joint laxity in this population. As it was shown by Jean et al and later by others, the increased pelvic retroversion in patients with long standing sagittal imbalance in ASD. forces the sacrum down putting the SI joint in a more vertical angle. 23 In this position, the SI joint is subject to more shearing and increasing rotational forces that will end up inducing SI joint ligament disruption and therefore increased SI joint range of motion. The more the sagittal imbalance is pronounced, the more the pelvis is retroverted and the more the shear is exerted on the SI joint.23,24 As the time passed in this conformation increases, more SI joint ligament disruption, and therefore increased laxity are expected. This theory was supported by Kwon et al. in their clinical study showing an increased SI joint laxity and degeneration in patients with ASD and sagittal imbalance compared to balanced aged and sex matched patients with lumbar stenosis. 25 This increased range of motion in the SI joint might account for the recorded difference is the pre-operative to post-operative variability in SS between both groups. IS connected through rods and metallic connectors to the spinal construct do not allow for a rigid fixation that outweighs the SI joint laxity in patients with persistent spino-pelvic mismatch. S2AI screw were shown on cadaveric studies to violate the SI articular cartilage in 60% of cases, allowing therefore for a stronger fixation of this increasingly mobile joint. This accounts for the lesser variation in SS witnessed in patients within this group. Therefore, post-operatively, these patients had to have more variability in their knee flexion to keep their head over their spine and their horizontal gaze.
Despite cadaveric studies showing no difference in biomechanical stiffness, screw toggle, rod strain and load to failure between S2AI screws and IS constructs; clinical studies showed IS screws to be associated with higher rates of implant failure, pseudarthrosis, screw breakage and screw loosening. 26 This is most likely due to the continuous micromotion that occurs through the connector joining the iliac screws to the rest of the construct. This continuous motion in a population of patients with increased SI joint laxity might account pseudarthrosis and increased rate of mechanical complications. On the other hand, in patients with S2AI screws, one should keep an eye during follow-up on the knee flexion as a chronic knee flessum deformity might affect knee related functional outcomes in an elderly population subject to degenerative knee disease.27,28
This study has several limitations. Despite prospective data collection our study remains retrospective with risks of selection bias and incomplete data collection. More, it is a single center experience, limiting therefore the number of included patients. However, the single center setting reduces heterogeneity related to different surgeons’ practices and techniques. Data related to the type and number of osteotomies performed in each cohort was not collected. Functional outcomes weren’t assessed in this study as this was not the objective of this work.
Conclusion
This study is the first to show that the type of pelvic fixation impacts significantly on the post-operative compensatory mechanisms of the body’s sagittal profile in patients with ASD. Patients with S2AI screws are more likely to compensate their remaining post-operative PI-LL mismatch through their knees and less likely through their sacrum compared to patients with IS. This is due to an increased SI joint laxity in ASD patients with sagittal imbalance leading to continuous micro-motion through the metallic connector in patients with IS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article. This study was approved by the institutional review board of our institution.
IRB Statement
This study was approved by the institutional review board of our institution. IRB approval number: 22.029.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publically available, but are available from the corresponding authors on reasonable request.