
Abstract
Study Design
Literature review with clinical recommendations.
Objective
To highlight important studies related to spinopelvic fixation and provide recommendations to practicing clinicians on interpretation and utilization of the evidence included in these studies.
Methods
Important literature related to spinopelvic fixation was reviewed and clinical recommendations were formulated. Recommendations were graded as strong or conditional.
Results
Three articles were selected and reviewed for the strength of methodology and scientific evidence. Article 1: Biomechanical analysis of lumbosacral fixation in Lumbar Fusion and Stabilization was granted conditional recommendation to consider biomechanical factors associated with different pelvic constructs. Article 2: Low profile pelvic fixation: anatomic parameters for sacral alar-iliac fixation vs traditional iliac fixation was granted strong recommendation to consider risk and benefits in choosing S2AI vs traditional iliac screw for pelvic fixation. Article 3: Rates of loosening, failure, and revision of iliac fixation in adult deformity surgery was granted a conditional recommendation, for taking into account different potential failure mechanisms in S2AI vs traditional iliac screws in pelvic fixation.
Conclusions
Currently evolving strategies have included multiple points of pelvic fixation, multiple rods to the pelvis and strategies with concomitant fusion of the sacro-iliac joints. The high mechanical failure rate at the lumbosacral junction indicates that there is still further opportunity for optimization. It is important to consider the risks and benefits of different pelvic fixation methods to optimize the outcomes for individual patients.
Keywords
Introduction
One important technical aspect of adult spinal deformity (ASD) surgery is the need for achieving stable and durable fixation at the caudal end of thoracolumbar fusion constructs. This is particularly true when fusions to the sacrum/pelvic are being performed. The need for strong, durable sacropelvic fixation has become well-established in long constructs extending to the sacrum. In the context of ASD, increased strength of fixation has been shown to reduce rates of pseudoarthrosis, improve fusion rates,1–8 prevent distal junctional failures,9,10 and allow for more powerful deformity corrections.
The current state-of-the-art regarding sacropelvic fixation continues to evolve. The spine surgery community has come to recognize that there exist several biological and mechanical nuances surrounding sacropelvic instrumentation in the setting of ASD. This review aims to highlight, summarize and critique three seminal articles focused on sacropelvic instrumentation, which have significantly added to our current understanding of this crucial component of spinal deformity surgery. The three articles summarized in this review were chosen for the following reasons: the article by McCord et al 11 continues to be the most important biomechanical article concerning spinopelvic fixation. The study by Chang et al 12 describes the advent of S2 alar iliac fixation, which represented a paradigm shift in sacropelvic fixation and became an effective and highly utilized technique, alongside traditional iliac fixation. Lastly, the study by Eastlack et al 13 is the largest clinical series focused on complications of spinopelvic fixation and fusion to the pelvis.
Clinical Rationale
McCord et al 11 performed a biomechanical study to understand the loading and failure modes of fixation strategies. At the time of publication of this study, transpedicular fixation was relatively new. In this study, the authors endeavored to determine if newer transpedicular fixation demonstrated biomechanical advantages over Harrington and Luque instrumentation with specific regards to fixation at the lumbosacral junction. Beyond this, they sought to assess biomechanical differences between different types of screw fixation, and lastly to determine relative differences in stability for different types of instrumentation crossing the sacroiliac joint (SIJ), as there were notable differences in design and technique between Galveston instrumentation and iliac screws.
Study Summary
Iliac fixation began with the Galveston technique.
14
This involved bending a smooth rod and inserting it into the ilium in the cancellous channel of the tear drop. With the increased use of pedicle screws, a screw (or bolt) was adopted to be used in place of the difficult to contour rod, making this approach modular. The key finding of this study is that fixation that extends anterior to the pivot point undergoes cantilever loading instead of experiencing in line pull-out failure. The fixation strategy that extends the most anterior is the iliac screw and this performs better than S1or S2 pedicle screws. Additional findings of importance included the biomechanical importance of triangulation of pedicle screws, which have been shown to have improved pullout strength compared to screws directed straight-forward. Lastly, the older Harrington and Luque systems demonstrated limited resistance to strain, which called into question the clinical utility of these systems (Figure 1). (A) Crossing the S1 joint is only biomechanically justified when fixation extends anterior to the projected image of the middle osteoligamentous column on the lateral radiograph. On the left is a coronal view of the ISOLA Galveston and ISOLA iliac screw constructs. Note the diverging iliac rods and screws between the inner and outer iliac cortices. The S1 screws converge medially in a triangular fashion. On the right, this sagittal view demonstrates the middle osteoligamentous column (heavy black line) and introduces the concept of a pivot point. The iliac screw goes a significant degree farther anteriorly towards the superior acetabular bone than bicortical S1 or S2 screws. (Note, this schematic depicts the human, not the calf, lumbosacral junction). (B) A view of the pelvis looking distally. Note the iliac screws/rods are significantly farther anterior to the middle osteoligamentous column (Axis of M.C.). For illustrative purposes, the S2 screws are medially converging: however, they were placed laterally diverging for actual testing. (C) This illustration defines the biomechanical concept of the lumbosacral pivot point concerning lumbosacral instrumentation. It is the intersection point of the middle osteoligamentous column and the L5-S1 intervertebral disc.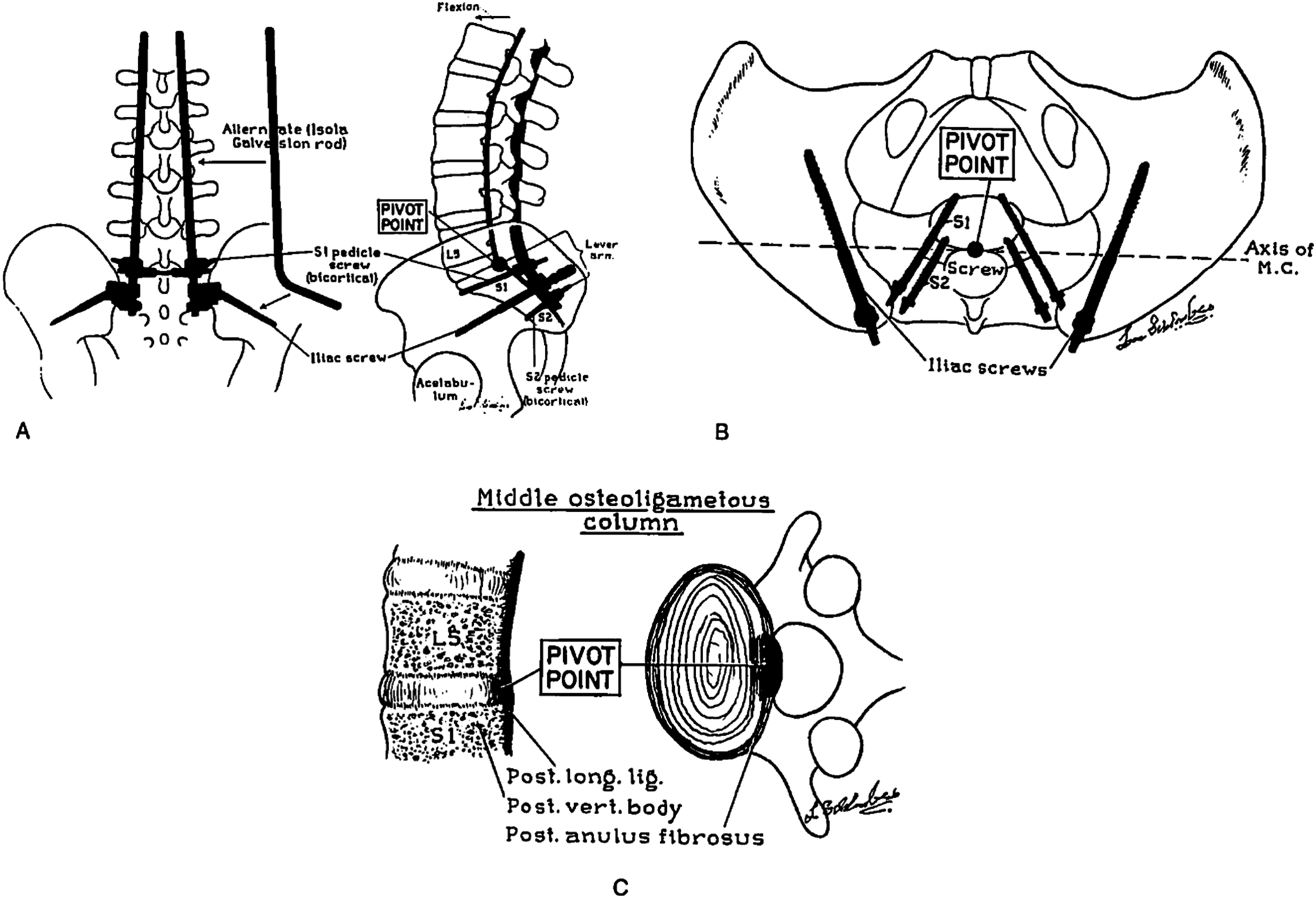
Assessment of Methodology
Biomechanical analysis of different lumbosacral spine fixation systems using a calf spine-pelvis model was utilized. In this study, ten different systems were evaluated and tested for biomechanical parameters, with three specific objectives in mind: (1) Determining whether newer transpedicular systems of instrumentation had biomechanical advantages over Harrington and Luque systems; (2) Assessing generic differences in fixation based on screw location, ie, S1 pedicle fixation vs S2 pedicle fixation vs iliac fixation; (3) to determine if all devices crossing the SIJ were equally stable, ie, comparing Galveston-style iliac crest rods vs iliac screws. Biomechanical parameters and endpoints of interest included system-specific ranges in flexion and extension (degrees), maximum moment (Nm) at failure, maximum stiffness (Nm/degree) at failure, maximum angulation (degrees) at failure, and maximum strain (%) at failure.
Overall, this is a well-conducted biomechanical comparative study of the commonly used lumbopelvic instrumentation systems that were commercially available and widely used at the time of publication. The findings of this study provide important insights into the biomechanical concepts and characteristics of lumbopelvic fixation that have become central to modern systems of instrumentation in ASD. These notions include the improved biomechanics of longer pelvic instrumentation extending anterior to the pivot point of the osteo-ligamentous middle column, as well as the enhanced pullout strength of medialized pedicle screws. Study limitations include in vitro biomechanical analysis, loading of specimens in flexion alone, anatomical differences between calf spine models and humans, and testing done in the horizontal, as opposed to vertical, positions. The quality of the evidence is thus low.
Recommendation for Integrating into Your Clinical Practice
This study, offers important insights into sacropelvic mechanics, and has informed spinal surgery in several important ways, which continue to be relevant three decades later. Whether one chooses to employ a traditional iliac screw or an S2 alar iliac (S2AI) screw as the distal anchors in a fixation construct continues to be at the discretion of the surgeon, as both techniques have their respective advantages and drawbacks. However, to create a construct of optimal biomechanical strength, the length of the pelvic screws is critical. This study shows that the mode of loading shifts from in-line pullout to cantilever loading when screws cross the pivot point, and the further anterior to the pivot point that the screws extend, the greater the strength of the construct in flexion. We have become increasingly aware of distal junctional failures (DJF) after surgical treatment of ASD.10,15–19 One clear strategy for improving the biomechanical characteristics of sacropelvic fixation constructs involves maximizing pelvic screw length. This translates into reduces rates of DJF, and improved clinical outcomes. 13
This article merits a conditional recommendation for incorporation into clinical practice. DJF is challenging problem to treat, typically requiring complex revision surgery. This study provides clear insight as to the manner in which one can surgically plan for anchors of optimal strength and loading mechanics at the base of the fusion construct so as to avoid downstream DJF. Therefore, it is our opinion that the true effect of placing sacropelvic fixation anterior to the pivot point, as described in this seminal study, lies close to that observed by McCord et al.
Clinical Rationale
Traditional iliac screws used in lumbopelvic fixation constructs have the disadvantages of being clinically prominent, frequently causing pain, and difficult to connect to the rostral anchors in the construct, commonly necessitating use of offset connectors. Chang et al 12 described the anatomical parameters of a new form of iliac fixation, the S2 alar iliac screw (S2AI), wherein the screw utilizes a sacral start point, in line with the S1 pedicle screw start point. The authors compare this with a traditional iliac screw.
Study Summary
When placing a conventional iliac screw, the dissection is challenging and adds significant time to the procedure. The S2AI screw, by contrast, does not require exposure of the iliac wing and does not require offset connectors. It allows extension well anterior to the pivot point so that the biomechanical performance is comparable to a conventional iliac screw. One stated criticism of S2AI fixation has been that it crosses an unfused SIJ. However, a conventional iliac screw or even the original Galveston technique spans an unfused SIJ. Moreover, it is more technically challenging to insert an S2AI screw, as there can be a tendency for the probe or awl to skive when crossing the SI joint and deviate outside of the ilium. Nevertheless, multiple case series have demonstrated clinical success with the S2AI technique. With regards to S2AI technique, correct screw placement can be made rendered less challenging with use of enabling technologies, such as robotics and navigation. However, freehand technique can be used as well with good technical result, and screw position can be confirmed using fluoroscopic teardrop views. Systematic reviews comparing S2AI to conventional iliac screws have shown a lower revision rate although there is debate about this. Furthermore, this study shows a clear benefit of S2AI fixation over conventional iliac screws, in that they are seated deeper, and therefore are less likely to cause issues with tulip prominence. This may be of considerable benefit in patients that are chair-bound, such as those with neuromuscular scoliosis.
Assessment of Methodology
Computed tomography (CT)-based study in 20 non-consecutive skeletally mature adolescent patients evaluating the three-dimensional radiographic characteristics of S2AI screws based on ideal start points and trajectories. For the S2AI corridor, maximal mean S2AI distance, narrowest mean width of the ileum along the trajectory, mean angulation in the transverse and sagittal planes, location of mean start point and mean distance from the skin was measured. For each subject, mean maximal length from the PSIS to the AIIS, as a proxy for mean maximal iliac screw length, and distance from the PSIS to the skin was also measured.
In terms of data reporting, Table 1 shows the mean radiographic measurements for the S2-iliac technique. Key findings included comparable mean maximal distance for S2AI screws to the maximal mean length for PSIS screw insertion, being 105 mm and 118 mm respective, with both measurements extending anterior to the pivot point, and the start point for S2AI screws being 19 mm deep to the PSIS, and in line with the S1 pedicle start point.
Overall, this was an informative and well-conducted study that highlighted some of the important differences between S2AI and conventional iliac screws, with S2AI fixation offering similar biomechanical advantages compared to PSIS-entry iliac fixation, while also affording reduced implant prominence and decreased soft-tissue dissection. The quality of the evidence is this study is moderate, keeping in mind that this is a CT-based study of anatomical parameters associated with two different techniques for sacropelvic instrumentation, and there is no assessment of clinical outcomes. That said, the directness of the evidence and precision of measurements are consistent with moderate quality evidence (GRADE). 20
Recommendation for Integrating into Your Clinical Practice
At the present time, there is no data showing obvious clinical or biomechanical superiority of S2AI fixation over conventional iliac screws. Both techniques have their respective advantages and drawbacks, and it behooves the modern spinal surgeon, particularly those treating ASD, to be knowledgeable and proficient with both techniques. The S2AI screw offers the advantage of being low-profile, which in turn may result in less pain and potentially better function. As an alternative, a modified iliac screw start point has been described, which utilizes a sub-crestal start point, and is more low-profile than one with a conventional PSIS start point. 21
Overall, this article merits a moderate recommendation to be incorporated into clinical practice. The findings in this study suggest that both conventional iliac fixation and S2AI fixation confer similar mechanical fixation strength, which is consistent with the practice patterns at the present time. There exists equipoise with regards to the biomechanical and clinical superiority of one technique over the other, and there are instances where one technique may be more appropriate for a specific patient. Notably, this study highlights some distinct advantages of S2AI fixation over conventional iliac fixation, while acknowledging that conventional iliac screws are a time-honored and effective technique.
Clinical Rationale
Given that pelvic fixation failure rates are not insignificant, and associated with impaired clinical outcomes, Eastlack and the International Spine Study Group 13 evaluated pelvic fixation failure rates and modes of failure, between traditional iliac and S2AI fixation, in a large cohort of adult spinal deformity patients with fusions to the pelvis.
Study Summary
This study involved high quality clinical and radiographic data collection across multiple centers that are performing high volumes of adult spinal deformity surgery. The authors analyzed clinical and radiographic failure modes and rates, for both traditional iliac screws and S2AI screws. The authors concluded that the rates of lumbopelvic fixation failure were high following adult spinal deformity surgery, and failures were associated with diminished clinical improvements. While S2AI screws were more prone to loosening, they were less frequently linked to rod fractures in the lumbopelvic region when compared to traditional iliac screw fixation. The authors further noted that rates of lumbopelvic fixation failure and revision surgery remain high after ASD correction. The overall rate of fixation failure in this study was quoted at 23.74%.
Assessment of Methodology
Retrospective cohort study of 1422 ASD patients that had undergone deformity correction with more than five level fusion and pelvic fixation, comparing S2AI screws to traditional iliac screws (IS). Data was collected from a prospectively collected database through the International Spine Study Group (ISSG), including thirteen centers across the US. Baseline demographic, clinical, and radiographic data and were collected, as were patient-reported outcomes measures (PROMs) at both baseline and follow up. Outcomes of interest included the radiographic presence of iliac or S1 screw loosening, iliac screw fracture/breakage, rod fracture below L4 level and the occurrence of subsequent revision surgery involving the lumbopelvic region. Univariate using t-tests and chi-square tests, and multivariate logistic regression were performed to control for possible confounding factors, to examine the effects of S2AI vs IS fixation with respect to the different modes of failure, while maintaining statistical power.
With regards to data reporting, Tables 1 and 2 showcased baseline preoperative patient and radiographic characteristics, respectively. Table 3 reported on different modes of failure within the IS and S2AI cohorts, while Table 4 reported on the odds ratios (OR) of different modes of failure for S2AI fixation. Table 5 reported on overall lumbosacral and pelvic fixation failure rates relative to specific factors/scenarios. Table 6 reported PROMs within the two groups at 2-year follow up.
This is a thoughtful, well-conducted and appropriately powered analysis of a large cohort of ASD patients undergoing surgical correction with use of sacropelvic fixation, and overall the quality of the evidence is moderate. The study design is a retrospective observational cohort study, although the quality of the study is strengthened by precision of measurements, large magnitude of effect as evidenced by P-values below 0.05, and a large sample size. 20 Of note, the S2AI group was shown to have increased odds of pelvic and S1 screw loosening, while IS fixation was associated with increased odds of rod fracture in the lumbopelvic region.
Recommendation for Integrating into Your Clinical Practice
Irrespective of one’s chosen method of sacropelvic fixation, a significant proportion of patients undergoing fusion to the pelvis for ASD experience fixation failure, which in turn is associated with significantly diminished clinical outcomes. Nearly one in four patients undergoing these procedures will experience failure of fixation, and these findings are in line with the findings of several other studies.22–28 With regards to the findings of this study, S2AI screws had greater odds of loosening compared to traditional iliac screws. This finding contradicted those observed in other studies, where, by contrast, iliac screws were more likely to loosen compared to S2AI screws,23,26,28,29 while others found no difference in rates of loosening.22,24 One possible explanation for the high observed rates of lumbopelvic fixation failure for both traditional iliac screws and S2AI screws involves the considerable stresses exerted on the distal fixation due to the motion at the SIJ41SIJ. 30
Overall, this article merits a conditional recommendation to be incorporated into clinical practice. It reports a 25% failure rate and sheds light on an important and previously under-acknowledged issue of sacropelvic fixation failure, irrespective of the specific fixation strategy. It reports different common modes of failure for the 2 techniques, although some of the observed results in this study are different from previous scholarship, thus further study is warranted.
Conclusions
In summary, our understanding of spinopelvic fixation has dramatically evolved over the last four decades. We have a better understanding of sacropelvic anatomy, loading parameters, biomechanics of fixation and surgical techniques for optimizing fixation. Based on the three articles that have been reviewed, one can conclude that surgical strategy at the sacropelvic junction can have significant biomechanical and clinical consequences. Ensuring that the distal anchors placed in the pelvis bypass the osteo-ligamentous pivot point likely reduces rates of DJF. Furthermore, an understanding of the different characteristic features of various types of sacropelvic fixation can be beneficial when selecting a fixation strategy at the distal end of the construct. Lastly, rates of DJF regardless of sacropelvic fixation strategy are non-trivial, and with more prolonged clinical follow up these rates likely increase. 19
Footnotes
Acknowledgements
This work was organized by AO Spine through the AO Spine Knowledge Forum Deformity, a focused group of international Spinal Deformity experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Support was provided directly through AO Network Clinical Research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.