
Abstract

Letter to the editor regarding: Yong Shen, Zeeshan M Sardar, Matan Malka et al, Characteristics of Spinal Morphology According to the “Current” and “Theoretical” Roussouly Classification Systems in a Diverse, Asymptomatic Cohort: Multi-Ethnic Alignment Normative Study (MEANS). Global Spine J. 2024 Feb 28. 1
We read this interesting publication about the “Current” and “Theoretical” Roussouly Classification Systems, where a discrepancy was identified when using the sacral slope (SS) or the Pelvic Incidence (PI) to classify an asymptomatic cohort, finding a mismatch rate between Current vs Theoretical in 3.7% Type 1, 33.3% Type 2, 37.9% type 3 and 35.9% type 4,1 but analyzing in depth the published results of the article, although this concept is interesting, reviewing its methodology and results, we made 3 observations from the article: 1. “The mismatch rate that occurred in the current vs theoretical Roussouly type 3 classification
2
was 37.9%”.
1
Possibly one of the reasons was that type 3 Anteverse Pelvic (3AP) subtype was not taken into account, which according to Laouissat et al is characterized by a PI < 50° and SS between 35° - 45°.
3
2. The asymptomatic population of the study, “as in Figure 1”, a notable difference was observed between the theoretical vs current Roussouly classification, one of the reasons is that the Sebaaly et al study was possibly not taken into account, where the evolutionary degenerative process that they suffer according to the Roussouly type is clearly explained, for example, type 4 due to its evolutionary degenerative process becomes type 3 and then a false type 2, so this would cause heterogeneity between the results.
4
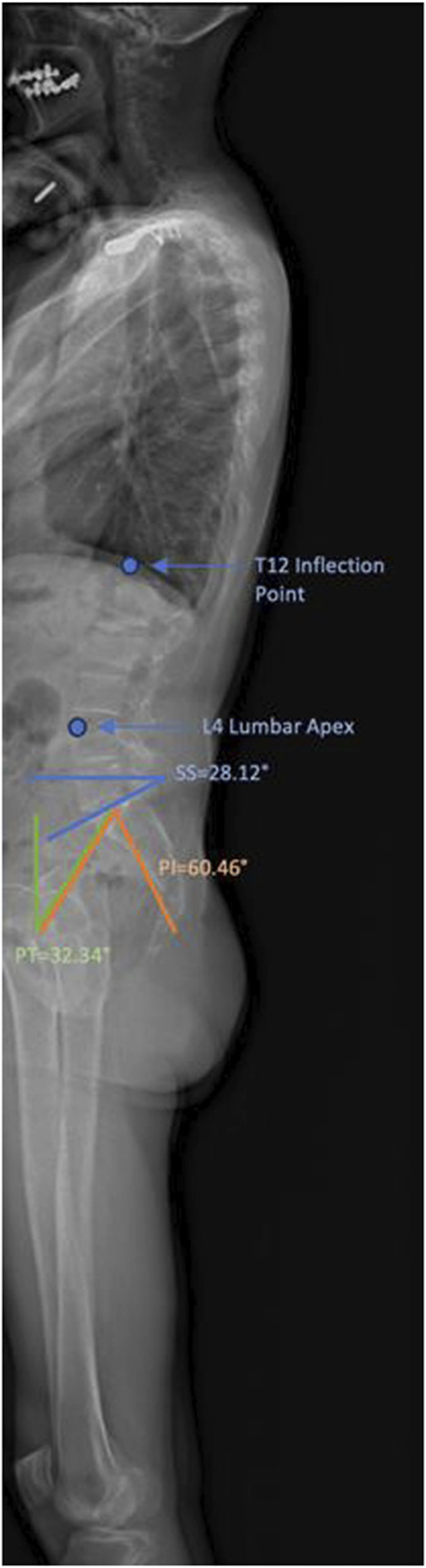
A French volunteer with a current-theoretical typemismatch. SS = 28.12 deg, PI = 60.4 deg, lumbar apex = L4, andinflection point = T12. This volunteer is current Type 2 buttheoretical Type 4. 3. The Roussouly classification refounding was carried out by Laouissat et al,
3
where the PI is taken into account first and then the SS, to properly classify the shape of the spine and therefore was able to identify a behavioral subtype of type 3. If asymptomatic people were studied, there would be no difference in their classification, this heterogeneity only exists because the degenerative process could occur early and this would affect their classification, so it is the degenerative evolutionary process of the classification must be taken into account and possibly by using the formulas described by Le huec et al,
5
a true theoretical Roussouly classification could be created, starting from the PI that is constant and an SS that is could be calculated with the formulas that previously mentioned.
5
We once again appreciate the author’s research and hope that our explanations and observations will help readers of this valuable journal.