
Abstract
Study Design
Narrative review.
Objectives
Adult spinal deformity (ASD) surgery has progressively transitioned from mean regional alignment targets to individualized segmental alignment goals, and from health-related quality of life (HRQL) alignment goals to the prevention of mechanical complications.
Methods
Narrative review discussing sagittal alignment concepts and goals in ASD surgery.
Results
Traditional metrics for measuring sagittal spinal alignment such as pelvic incidence - lumbar lordosis (PI-LL), thoracic kyphosis, and sagittal vertical axis (SVA) may lack the specificity necessary for individualized alignment planning. Compensatory pelvic retroversion and knee flexion are critical determinants of maintaining the upright position. Research has been conflicting as to whether postoperative sagittal alignment is associated with improvements in HRQOL’s. However, this may reflect a lack of sensitivity in the traditional alignment targets and PROM’s measures, rather than a true lack of relationship between sagittal alignment and functional outcomes. Recent studies show that sagittal parameters have a limited impact on HRQL scores in non-operated patients, but significantly impact post-operative HRQOL measures and mechanical complications in patients treated with spinal fusion. Latest evidence suggests that compensatory mechanisms need to be eliminated and the ideal shape needs to be restored with surgery, to reduce postoperative mechanical complications. Multiple alignment strategies are proposed for that purpose.
Conclusions
While best evidence shows an improvement in ASD alignment strategies over the last decade, mechanical failures and reoperations are still a cause for concern. This narrative review analyzes the strengths and weaknesses of the different alignment strategies and identifies the main areas of debate.
Keywords
Introduction
The aging population and increasing demand to remain independent without significant disability, together with a high prevalence of adult spinal deformity (ASD) above 60 years of age, lead to a marked increase in ASD surgery. 1 Early research defining surgical goals focused on the identification of parameters that depress health-related quality of life (HRQL) and cause disability in ASD patients. 2 Sagittal alignment parameters had the strongest correlations with HRQL, while coronal parameters played a limited role. While ASD surgery quality metrics improved over the last decade, 3 mechanical complications remain the most common reason for readmission and unplanned reoperation. Understanding spinal alignment and aiming for individualized postoperative alignment goals is associated with reduced postoperative mechanical complications. In 20 years, we have transitioned from regional alignment targets based on population means to individualized segmental alignment goals, and from HRQL alignment goals alone to inclusion of alignment goals that reduce mechanical complications.
The purpose of this review is to provide the latest insights on this matter.
Methods
This study is a narrative review of the literature identifying publications discussing sagittal alignment concepts and goals in ASD surgery. A summary is provided of the different philosophies and concepts as related to alignment, and their impact on HRQL and postoperative complications.
Normal Spinopelvic Alignment
Cone of Economy and Measures of Sagittal Alignment
The ‘Cone of Economy’ is a concept introduced by Dubousset that describes the range of sagittal postures within which a human can maintain upright, with minimal energy expenditure. 4 Deviations outside the cone of economy require compensatory mechanisms, increasing energy expenditure. The position within the cone of economy is determined by spinal alignment, pelvic tilt, and lower limb alignment.
Global sagittal alignment refers to the overall static shape of the spine and relative positions of the head, spine, and pelvis. “Sagittal Balance” indicates whether the spine is in equilibrium (‘balanced’) or not and is often considered a dynamic situation. A well-aligned spine enables efficient posture within the cone of economy, achieving economic balance. In contrast, spinal malalignment can result in poor sagittal balance, requiring compensatory mechanisms to maintain an upright position. 5
Normal Spinopelvic Alignment
The Pelvis
Pelvic incidence (PI) is a fixed parameter describing the angular relationship between the sacral endplate and the center of the femoral heads. Pelvic incidence, which indirectly describes the pelvic morphology of an individual, is the basis to understand spinopelvic alignment. PI gradually increases during childhood due anterior-posterior growth of the pelvis and remains nearly constant throughout adulthood, 6 except for some nutation/counternutation sacroiliac movement of an average of 2-3 degrees in adults. There also appear to be changes in PI patients with bilateral pelvic fixation (as a compensation mechanism). Across multiple studies, median PI for adults is between 50° to 55° (IQR between 45° to 60°).7–9 Some variation of PI between races has been observed in some US-centered studies, though this finding is not consistent.10–14
Sacral slope (SS) describes the orientation of the sacral endplate relative to the horizontal, and pelvic tilt (PT) describes the orientation of the sacrum relative to the hips when standing upright. Pelvic tilt (PT) and sacral slope (SS) are geometrically related to PI where PI = PT + SS, and while PT and SS are both strongly associated with PI, the relationship is complex Figure 1. For a given PI, a wide range of normal PT may exist and defining a normal PT or SS strictly based on PI may be misguided.
15
Pelvic parameters.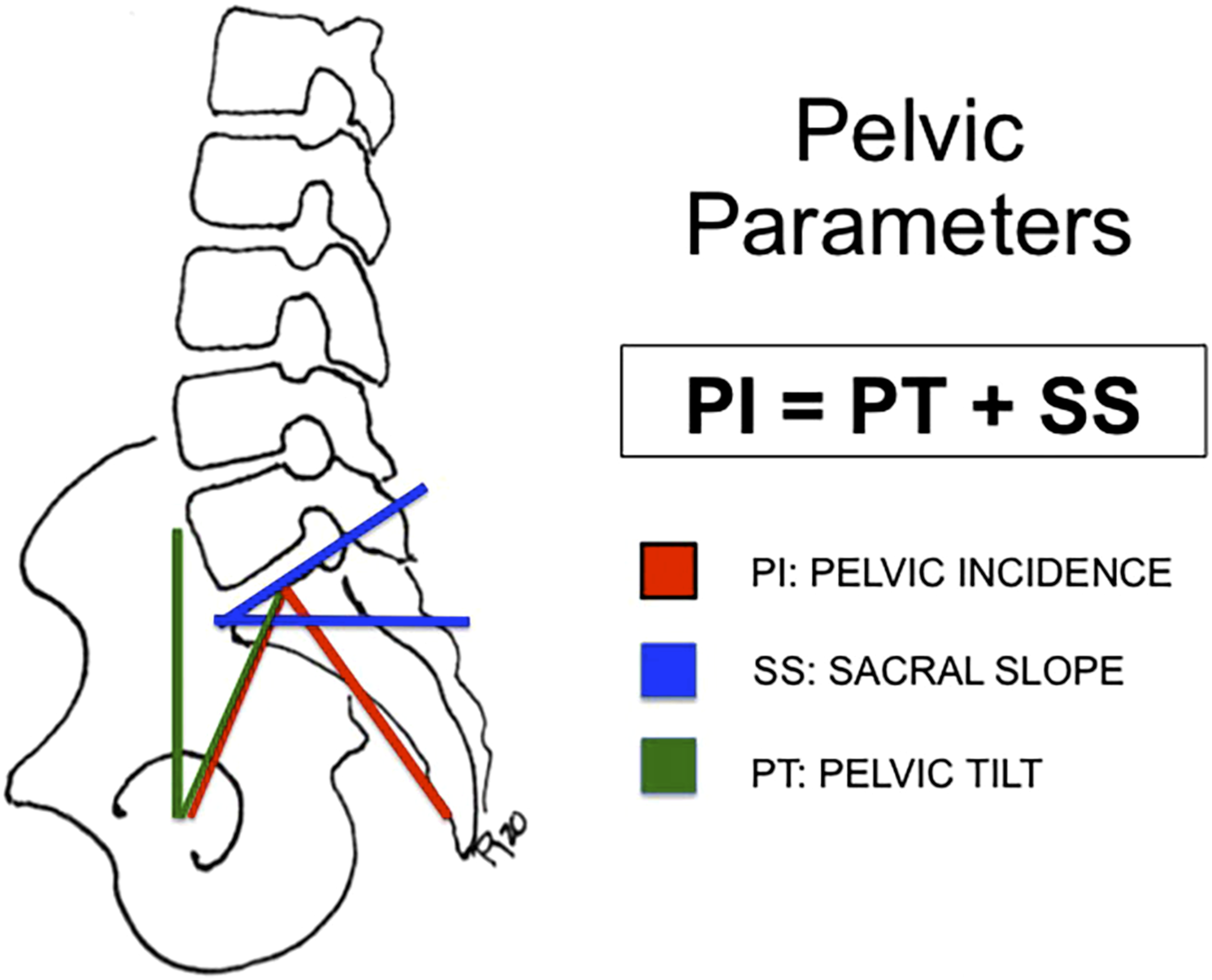
Regional Sagittal Alignment
Normative values for lumbar alignment have generally been consistent and in agreement across multiple studies. Historically, the pelvic incidence-lumbar lordosis (PI-LL) relationship was considered linear, with the concept of PI-LL mismatch emerging as a key factor in assessing sagittal balance and guiding alignment goals in spinal deformity surgery. The understanding of the complex relationship of lumbar alignment with PI has evolved over time. Multiple studies have reported a negligible association between L4-S1 lordosis and PI, with a median L4-S1 near 35° (IQR between 25° to 50°). 16 L1-S1 lordosis is associated with pelvic incidence but the relationship is non-linear and relatively weak (r2 ∼ 0.3).16,17 A normal L1-S1 can be roughly estimated as LL = PI x 0.6 + 30°. The measure of L1-S1 lordosis does not account for the distribution of the lordosis and the range of normal can be up to ± 20°. Thus, simple measures of lordosis and kyphosis are agnostic to the shape of the spine. The L1 pelvic angle (the spatial position of the centroid of L1 related to the hips) has a stronger association with pelvic incidence and a normal value can be described as L1PA = 0.5 × PI – 21°.
Roussouly studied asymptomatic individuals to describe 4 distinct lumbar shapes, based on the sacral slope, with differing upper and lower arcs of lordosis.
8
The lower arc of lordosis extends from S1 to the lumbar apex (the most anterior point of the lumbar spine touching a vertical line), and the upper arc extends from the lumbar apex to the thoracolumbar inflection point (which is the point where LL transitions into thoracic kyphosis-TK). Thus, the lower arc of lordosis is geometrically equal to SS, and the upper arc is relatively constant (∼18° in magnitude but differs in length) Figure 2.15,18 Since Roussouly reported his classification system based on both the distribution and magnitudes of the sagittal curvatures, also known as “the shape”, our understanding of normal spinal alignment has continued to evolve, now recognizing that normal sagittal alignment falls on a continuum rather than discrete categories. Sagittal shape distribution. UTA: Upper thoracic arc; LTA: lower thoracic arc; ULA: upper lumbar arc; LLA: lower lumbar arc; SS: sacral slope. T Apex: thoracic apex; IP: Inflection point; L Apex: lumbar apex. LLA and SS have the same magnitude. ULA and LTA have the same magnitude.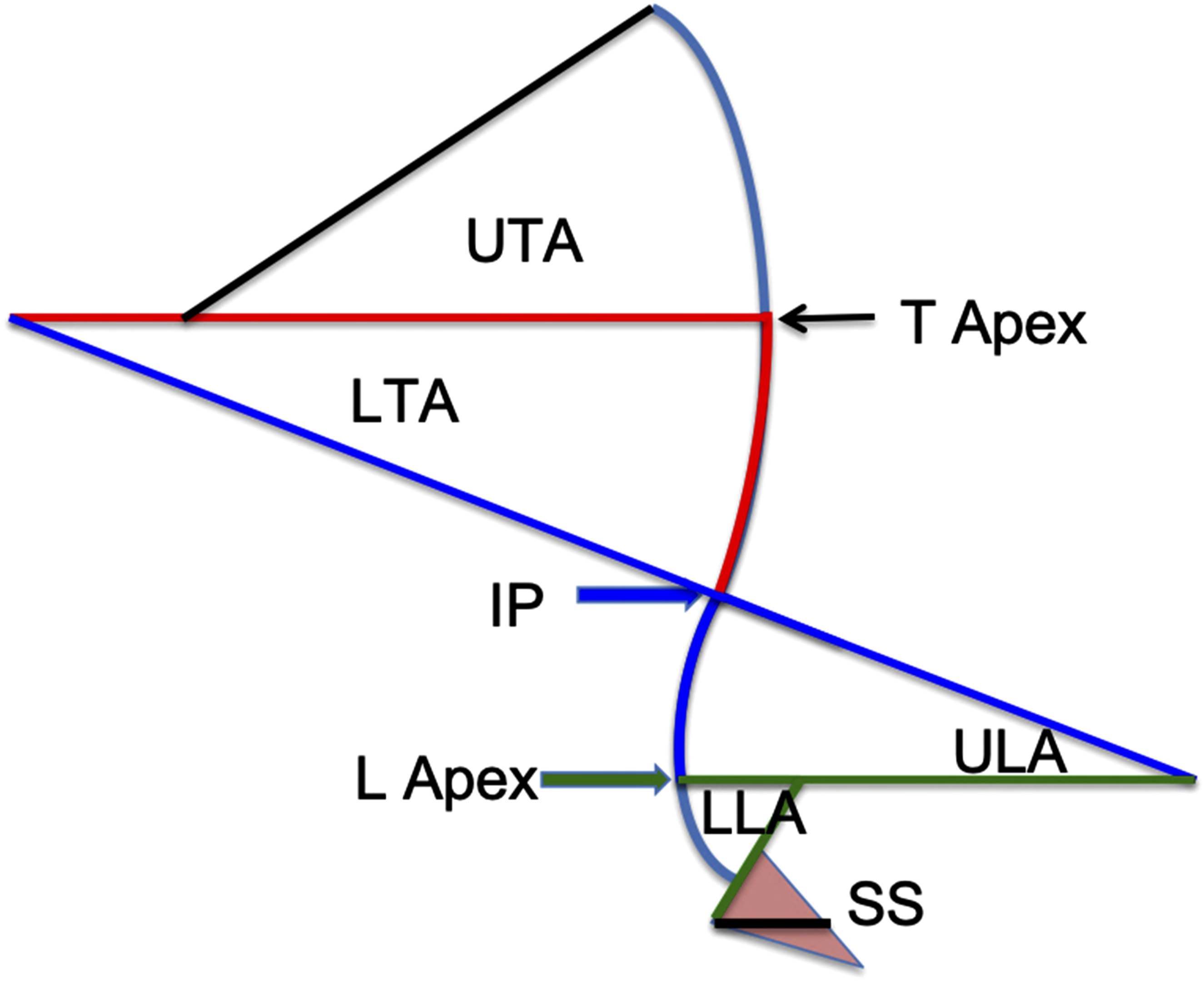
The vertebral pelvic angles (VPAs) are a newer alternative to sagittal Cobb angles to measure sagittal alignment. The VPA offer the benefit of representing the spinal shape and the relationship to the hips, representing pelvic version. From a mathematical perspective, the VPA offer a representation of the spline shape of the spine, where any vertebral body point is a knot within the spline. VPA have excellent intra- and interobserver reliability with measurement error typically less than 2° and numerous studies have advocated for using VPAs for measuring sagittal alignment.
19
Hills et al
7
studied 320 volunteer adults without radiographic evidence of degeneration or spinal deformity and without any history of spinal pathology from the MEANS (Multi-Ethnic Alignment Normative Study) cohort with the goal of describing normal regional and global sagittal alignment relative to PI using continuous measures and parameters that become fixed after instrumented fusion. They described the ‘T4-L1-Hip Axis’ Figure 3, which refers to the relatively strong relationships between L1PA and PI (r2, 0.58), and between T4PA and L1PA (r2, 0.81). According to their results, 80% of the population will have an L1PA = 0.5 × PI −21°, and a T4PA within 4° of L1PA. If T4PA = L1PA, a line from the T4 centroid to the hips will cross through the centroid of L1. The authors also reported sagittal Cobb measures for the entire spine, and consistent with prior studies, they found L1-S1 lordosis had a relatively weak and nonlinear association with PI (r2 = 0.3). They also found L4-S1 lordosis to be independent of PI with a median of 37° but reported a normal range of L4-S1 from 25° to 55° (unlike prior studies reporting a ‘constant’ value). These findings are consistent with the development of a normal sagittal alignment, where upper arc lordosis increases with increasing PI. The VPA are more strongly associated with PI and global alignment, have a lower measurement error rate, VPA’s inherently capture the distribution of lordosis and kyphosis, and VPAs become fixed after fusion to the sacrum highlighting some benefits of this assessment system. Common measures of lordosis and kyphosis (sagittal Cobb measures). Vertebral pelvic angles (angle formed by lines drawn from the vertebral centroid and the center of the superior S1 endplate to the bicoxofemoral axis) are shown for C2PA, T4PA, and L1PA. C2 tilt is the angle formed by a line from the center of the odontoid to the bicoxofemoral axis and a vertical line through the bicoxofemoral axis. Pelvic incidence (PI), pelvic tilt (PT) and sacral slope (SS) are illustrated.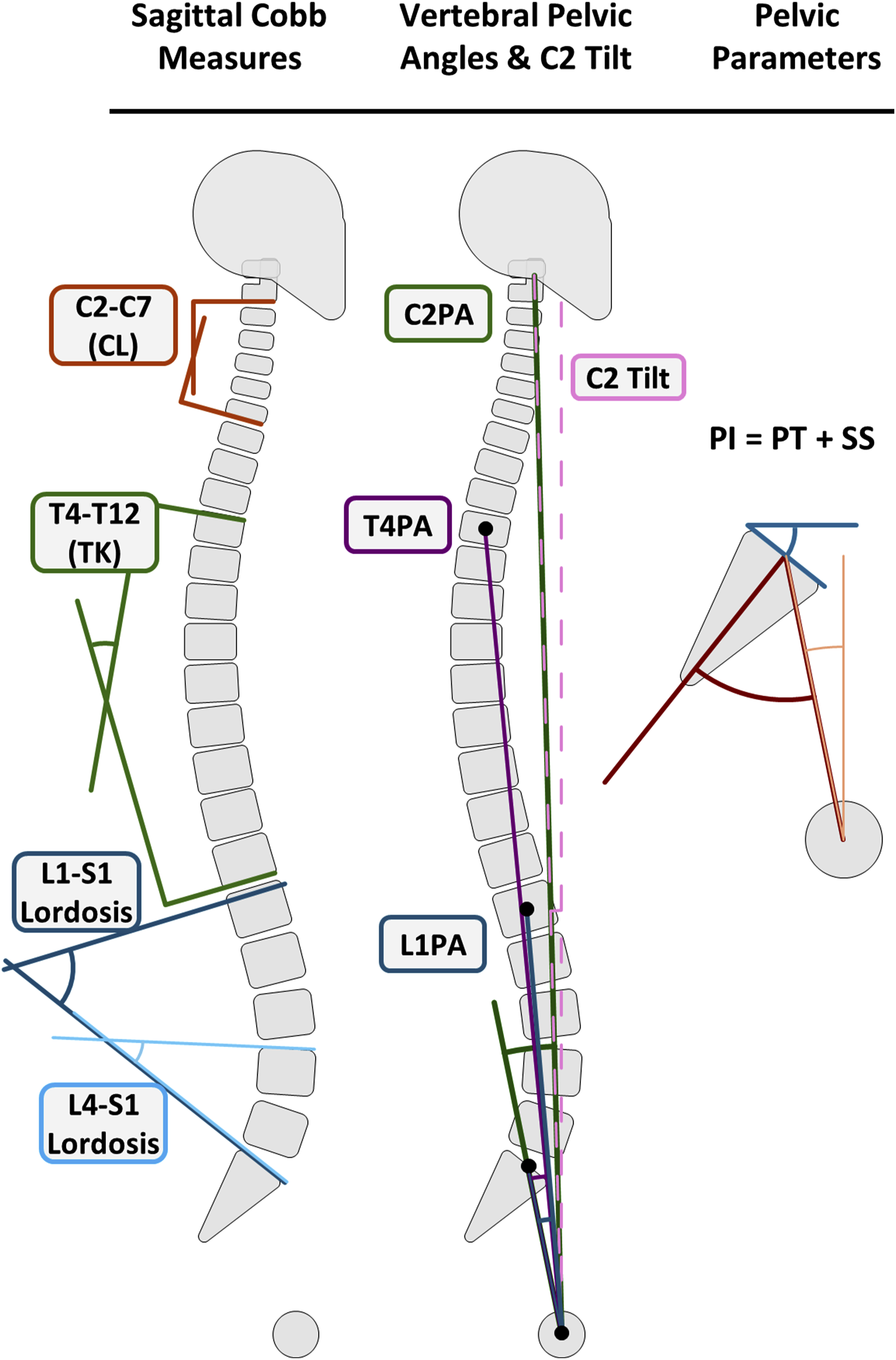
Global Sagittal Alignment
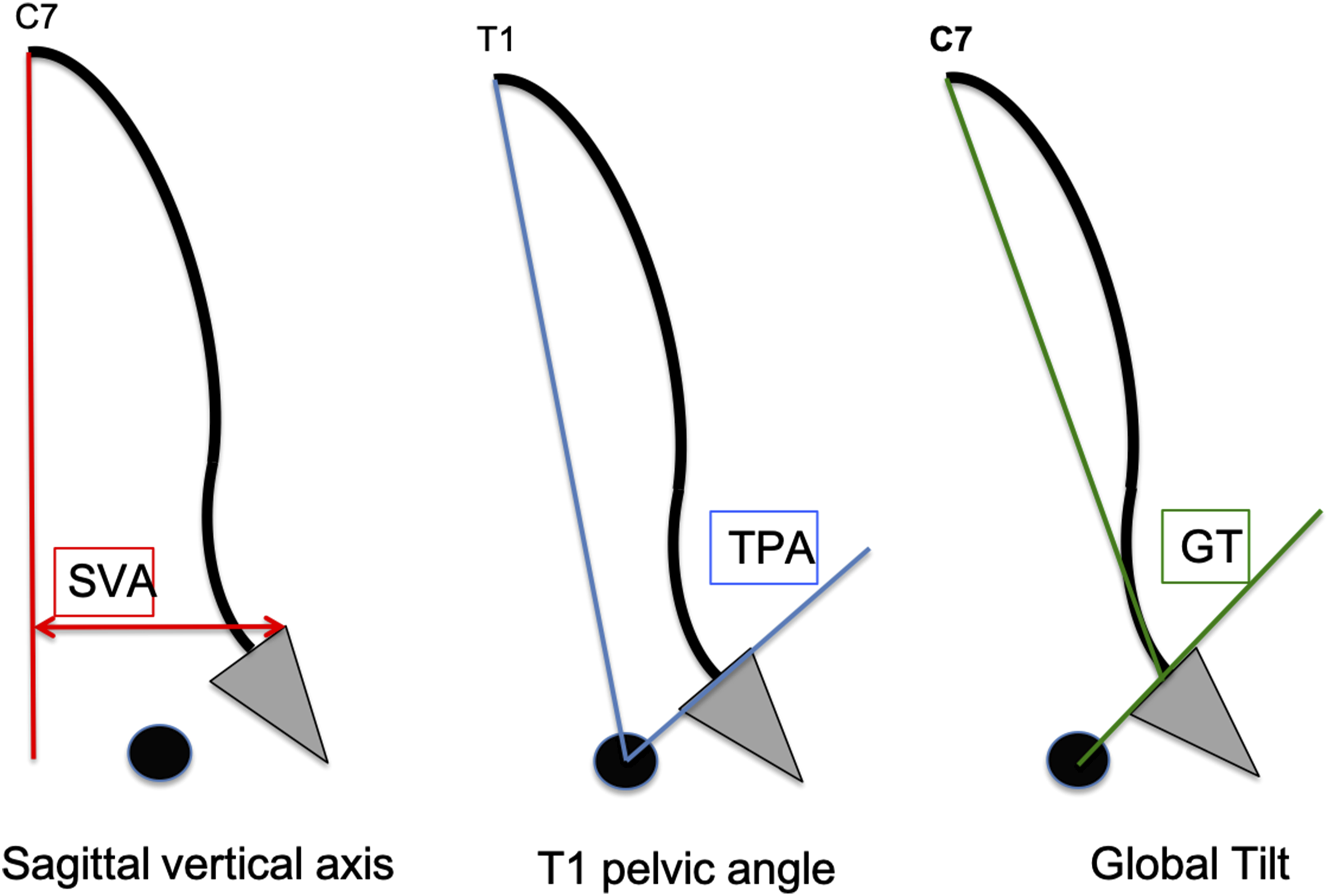
Several parameters have been reported for measuring global sagittal alignment and balance. The C7 Sagittal Vertical Axis-SVA (distance from the C7 plumb line to the posterior superior S1 endplate) is a classic measure of sagittal alignment. This measure is useful only to track an individual patient over time. It is immune to changes in pelvic tilt where C7 SVA can be 0 mm in a maximally compensated state or in a normal spine. Furthermore, C7 SVA varies with PI making between patient comparisons less informative.
Several studies have highlighted C2 tilt (also known as the Odontoid-Hip-Axis) as an ideal measure of global sagittal balance.7,20–22 C2 tilt is independent of PI and has minimal variation in normal individuals, with a median value of −2.7° (IQR, −4.4 to −1.1). Additionally, C2 tilt is geometrically related to C2PA and PT (C2 tilt = PT + C2PA). Because a normal C2 tilt appears likely to be an objective measure of balance within the cone of economy, PT will be nearly equal to C2PA in well-balanced individuals (normal C2 tilt) and within the relative boundaries of PT.
Degeneration of Normal Alignment and Age
Major Radiographic Parameters Normative Values Taken From the Multi-Ethnic Alignment Normative Study (MEANS) Cohort (320 International Asymptomatic Volunteers With No History of Spinal Disease or Spine Surgery) 7 .
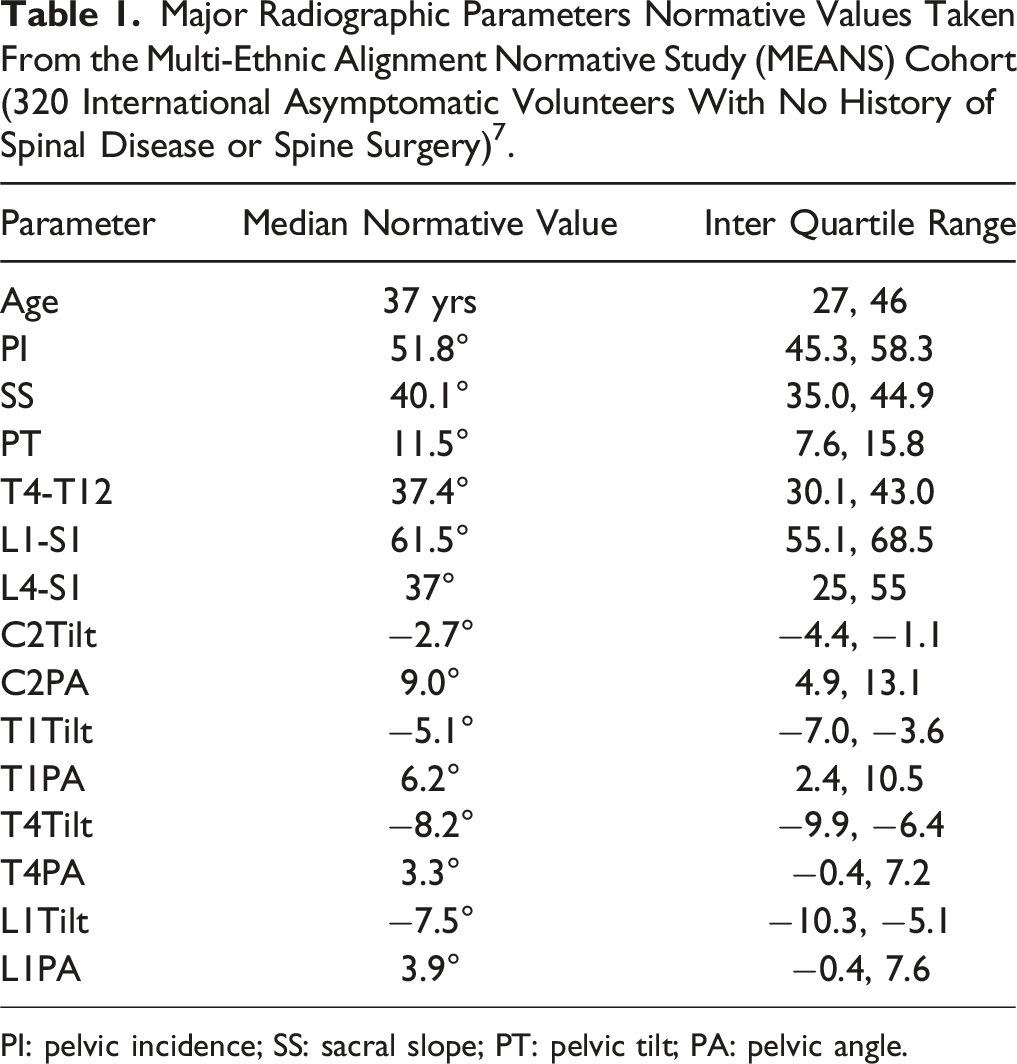
PI: pelvic incidence; SS: sacral slope; PT: pelvic tilt; PA: pelvic angle.
Global alignment measures.
Despite these changes, full body alignment, as measured from the center of the auditory meatus and the force plate-based gravity line, can remain stable with age14,30 due to compensatory mechanisms recruited at adjacent spinal segments, hip, and knee. As the MEANS study confirmed, volunteers used compensatory mechanisms such as slight pelvic retroversion, knee flexion and neck extension to maintain an aligned global sagittal posture, with their skull centered over their knees.
While multiple studies suggest that sagittal alignment becomes more kyphotic with age, it may be more accurate to attribute loss of sagittal alignment to spinal degeneration. Spinal degeneration is clearly associated with age, but an elderly individual with no signs of degeneration would not have an increase in TK. Therefore, age functions as confounding variable rather than a direct cause. Thus, achieving personalized alignment goals in spinal deformity surgery will require a detailed evaluation of the individual’s segmental, regional, and global alignment, rather than relying solely on average age-related changes.
Spinopelvic Malalignment and Adult Spinal Deformity
Compensatory and Reciprocal Changes in ASD
Sagittal plane malalignment can eventually lead to spinal imbalance, causing fatigue due to the energy expenditure associated with the engagement of compensatory mechanisms recruited to avoid imbalance. Reactions starts with a more lordotic alignment of the adjacent spinal segments and follows with pelvic retroversion, hip extension, pelvic shift, knee flexion, and finally ankle dorsiflexion. 5 In older patients with larger sagittal plane deformities (PI-LL >30°), the contribution of thoracic hypokyphosis and pelvic retroversion to the compensatory cascade decreases in favor of knee flexion and pelvic shift.31–33
Resolution of compensatory mechanisms is expected after most surgical realignments34–36 Reciprocal changes at the unfused spinal segments and lower extremities follow surgical correction in order to accommodate the new postoperative alignment.35–37 Klineberg et al. 38 showed that after a lumbar pedicle subtraction osteotomy (PSO), TK increases in those patients who did not undergo thoracic fusion. This is logical and follows the Roussouly classification, where the upper arc of lordosis is geometrically equal to the lower arc of TK. Similarly, thoracic PSOs showed correction of a preoperative hyperlordosis. Mobility of the unfused spine is required for these reciprocal changes to occur. 39 Reciprocal changes are not expected in situations like ankylosing spondylitis, and careful surgical planning is required to achieve spinal harmony and maintain horizontal gaze.
Patients with positive sagittal malalignment may develop cervical hyperlordosis 28 that can improve following lumbar PSO. 40 This effect may not be so evident after a thoracic PSO, 41 when the lumbar region is more prone to reciprocal changes than the cervical spine. 42 When alignment targets are not met, reciprocal changes may not work as expected and can have a negative effect leading to further malalignment. Lafage et al found an unexpected increase in TK (that worsened SVA and PT) in more than one-half of the cases with lumbar PSO and an upper-most instrumented vertebra (UIV) below T10. 43 This was linked to older patients with greater preoperative sagittal malalignment and higher PI. The authors suggested that inadequate correction in older patients, with resultant increased loading of the spine, combined with greater muscle atrophy, could explain the unexpected results.
Impact of ASD
ASD is one of the most common causes of severe functional disability and back pain.44,45 Early research using univariate analyses found positive correlations (with low r2) between sagittal spinopelvic parameters and HRQL scores in ASD patients, 9 suggesting that malalignment is associated with higher levels of disability.46–48 Besides the physical and mental impacts of the deformity, the degeneration may lead to neurological dysfunction and debilitating back pain that can be refractory to nonsurgical treatments. With the large heterogeneity in ASD, there is significant variability in the surgical and nonsurgical management of the condition. When surgery is performed, Takemoto et al showed that post-fusion sagittal spinopelvic parameters were significantly associated with postoperative Oswestry Disability Index-ODI, even after adjustment for covariates. 49 Thus, focusing on restoring physiological alignment is a goal of most surgical plans.
Surgical Realignment Goals in ASD
Alignment strategies aim to understand the normal spinal parameters. The various philosophies will be highlighted in the following section that include the Roussouly classification, SRS-Schwab classification, age-adjusted alignment goals, the GAP score, T4-L1-hip axis, and segmental alignment restoration.
Common Alignment Strategies
Roussouly
Failure to appropriately reconstruct the lordosis shape and arcs distribution as per the Roussouly classification has been associated with mechanical complications. 50 The classification describes shapes of spine subtypes based on young asymptomatic patients. There were 4 types described in his initial classification based on the magnitude of the sacral slope (SS), 8 with type 1 having a SS <35° and a lumbar apex of L5, type 2 has a SS <35° and a lumbar apex of L4, type 3 has a SS between 35 and 45° with an L4 apex and type 4 has a SS >45° with a lumbar apex of L3 or higher. A fifth type, type 3 AP was added in 2018 51 characterized by hyperlordosis, low-grade PI, and very low or negative PT with an anteverted pelvis. Patients with a low Roussouly subtype have a lower inflection point and fewer number of vertebrae in the lordotic segment, and those with a higher type have a higher inflection point and a greater number of vertebrae in the lordotic segment. The classification has an interobserver reliability ranging from 0.4 to 0.68. Understanding a patient’s Roussouly type can help surgeons plan the appropriate inflection point for their patients. Pizones et al. 52 demonstrated a 72% rate of mechanical complications in surgical patients not matching the ideal Roussouly type compared to 15% in patients where the Roussoly type was matched.
SRS-Schwab Classification
Schwab and colleagues used regression models to define thresholds for radiographic spinopelvic parameters associated with ODI >40 (moderate disability): PT >22°, SVA >47 mm, and PI-LL >11°. These data subsequently served as the basis for the Scoliosis Research Society-Schwab (SRS-Schwab) classification for ASD and the radiological thresholds were subsequently offered as alignment goals for ASD surgery.48,53–55 Schwab et al. 53 demonstrated that larger PI-LL mismatch, higher pelvic tilts and higher SVAs were associated with worse scores. The classification did not account for age, spinal shape, and used fixed levels to determine LL. As it was developed based on patient reported outcome scores of which alignment is only one aspect, external validation between the Schwab-SRS classification and mechanical failures has been challenging. Nevertheless, the classification highlighted the importance of proper alignment, the relationship between alignment and pelvic incidence, and led to significant research on alignment and outcome that has furthered our understanding of this complex topic.
Age-Adjusted Alignment Targets
The SRS-Schwab classification offered an initial framework to characterize alignment in ASD patients. To work toward more patient-specific alignment goals, Lafage et al proposed age-adjusted alignment goals. 56 To generate these goals, the authors investigated preoperative alignment values and HRQOL outcomes to determine age-specific realignment targets for PT, PI-LL, SVA and T1PA. To determine the alignment goals, the authors fit alignment goals to HRQOL through a series of regression models. They suggested that ideal spino-pelvic values increase with age, ranging from PT = 10.9°, PI-LL = −10.5°, and SVA = 4.1 mm for patients < 35 years to PT = 28.5°, PI-LL = 16.7°, and SVA = 78.1 mm for patients > 75 years. In a follow-up study, Lafage et al reported that PJK patients had smaller post-operative PI-LL mismatches (termed “overcorrected”) than non-PJK patients. In addition, middle-aged and older PJK patients were “over-corrected“ based on age-specific thresholds. 57 This work highlighted that overcorrection is similarly important as undercorrection, however, with the classification being based on outcome scores and not mechanical failures, attempts to validate age-adjusted alignment targets have not consistently demonstrated an improvement in outcomes based on these thresholds. 58 In addition, if one acknowledges that degeneration is associated with increasing age and degeneration is associated with spinal malalignment, then one can see in it a critical confounding variable.
Global Alignment and Proportion (GAP) Score
The Global Alignment and Proportion (GAP) Score was proposed as a method to estimate the risk for mechanical complications and define alignment goals following ASD reconstruction. 17 The GAP score includes an age modifier (defined by age ≥60) and stratifies patients into three categories associated with an increasing rate of mechanical complications. Like Roussouly targets, the GAP measures are based upon PI, allowing surgeons to personalize individual alignment goals for each patient using a single preoperative measure. The GAP score added the Global Tilt (GT), a measurement that added the C7 Vertical tilt - C7VT, (the angle formed between the C7 plumb line and a line from the middle of C7 to the middle of the S1 superior endplate) and the pelvic tilt, ie, GT = C7VT + PT.
The GAP score incorporated age, PI, SS, L1-S1 lordosis, L4-S1 lordosis and, based upon how those 4 domains differ from the ideal (relative pelvic version-RPV, relative lumbar lordosis-RLL, Lumbar distribution index-LDI and relative spinopelvic alignment-RSA) would create a risk prediction for mechanical failure. Scores of 0-2 were considered proportioned, scores from 3 to 6 were considered moderately disproportioned and scores between 7 and 13 were deemed severely disproportioned. External validation studies of the GAP score have shown mixed results.58–65 However, in a recent systematic review analyzing GAP score capacity in predicting mechanical complications occurrence, authors studied eleven retrospective articles plotting a global AUC of 0.68 ± 0.2, showing a moderate predictive accuracy. 66
T4-L1-Hip Axis
Hills et al introduced the T4-L1-Hip Axis concept by studying a volunteer population without evidence of spinal deformity or degeneration. 7 The T4-L1-Hip axis is comprised of 2 parameters: a normal L1PA (L1PA = 0.5xPI −21°) and a normal T4-L1PA mismatch (near 0°, meaning a line drawn from the T4 centroid to the hips will cross over the centroid of L1). T4PA can be measured intraoperatively and becomes fixed following instrumentation from the sacrum to T4.
This concept was studied in 247 adults that underwent long spinal fusion from the upper thoracic spine to the sacrum. 67 They identified 68 (27.5%) patients with mechanical complications, defined as radiographic PJK, displaced rod fractures, or revision for PJK or pseudarthrosis. While adjusting for age, they modeled L1PA deviation and T4-L1PA mismatch and found that deviation from a normal L1PA or T4-L1PA mismatch in either direction, overcorrection or undercorrection, was associated with a higher risk of mechanical complication. They reported the lowest risk of mechanical complications was with alignments falling within “normal alignment”. In their analysis, age was not associated with risk of mechanical failure. In addition, they found that increasing sagittal malalignment (deviation from normal) was associated with worse HRQOL at 1 year following surgery. The advantages of these parameters as alignment targets include their continuous nature rather than classification, and that both T4PA and L1PA can be measured intraoperatively and remain fixed following long instrumentation to the sacrum. Still, external validation is needed to better understand the implications of these alignment targets in ASD.
Segmental Alignment Goals
Bernhardt and Bridwell introduced normal segmental parameters for each level in the thoracic and lumbar spines. 68 Their model, which did not account for pelvic parameters, showed increasing lumbar lordosis moving caudal from L1 to S1 with lordosis at L1-2 of 4°, L2-3 of 7°, L3-4 of 13°, L4-5 of 20°, and L5-S1 of 28°. The thoracic spine showed maximal kyphosis at the apex measuring 5° at each level between T4 and T9 with gradual decreasing kyphosis as you move away from the apex proximally and distally to neutral cervicothoracic and thoracolumbar junctions. They describe an inflection point transitioning from kyphosis to lordosis at T12-L1. While the magnitude of the segmental angles may vary depending on a patient’s PI, the distribution of the kyphosis and lordosis described serve as an excellent template for rod bending for most constructs.
Pesenti et al. 16 described segmental alignments based on PI. They noted a relatively constant L4 to S1 lordosis of 35° independent of PI, with increasing L1 to L4 lordosis with increasing PI. They noted patients with a mean PI of 39.1° (low PI) to have segmental lordosis from L1-2, L2-3, L3-4, L4-5 and L5-S1 to be 1.4°, 5.7°, 9.4°, 14.6°, and 20.2° respectively, with these values being 2.3°, 7.7°, 11.6°, 16.2° and 20.5° respectively when the mean PI is 51.7° (average PI) and these values being 4.9°, 10.8°, 14.4°, 16.5° and 19.4° respectively in patients with a mean PI of 68.6° (high PI). The concept of obtaining 35° of L4-S1 lordosis was validated in a cohort of degenerative 1 to 3 level fusions showing a lower rate of adjacent level degeneration and revisions in patients where the distal lordosis goal was achieved. 69
Lai et al.
70
described the cranial SVA hip (CrSVA-H) alignment Figure 5, the distance from the center of the femoral hips to a vertical line running from the nasion-inion midpoint in the skull. In their series of 363 ASD patients, multivariable regression analysis demonstrated the CrSVA-H to be a significant independent predictor of 2-year SRS-22r scores. They recommended that the CrSVA-H should be used instead of the C7 SVA as a post-operative sagittal alignment goal. Schematic diagram of CrSVA-H measures. From Lai CS, et al. Cranial sagittal vertical axis to the hip as the best sagittal alignment predictor of patient-reported outcomes at 2 years postoperatively in adult spinal deformity surgery. J Neurosurg Spine. 2024;41(6):774-783. doi:10.3171/2024.5.SPINE231187.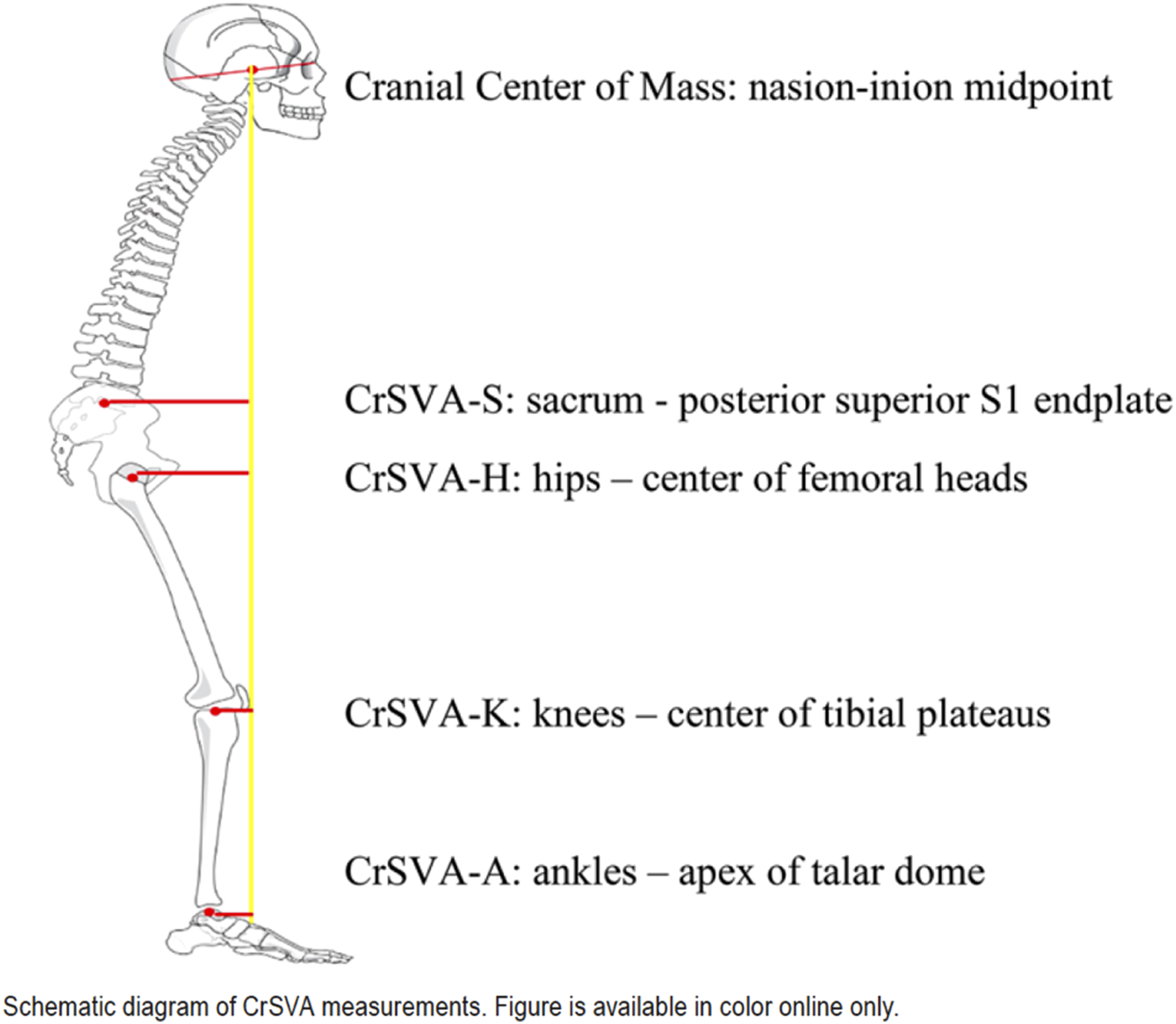
Limitations to Current Alignment Strategies and Areas of Controversy
Different Strategies to Meet Alignment Goals.
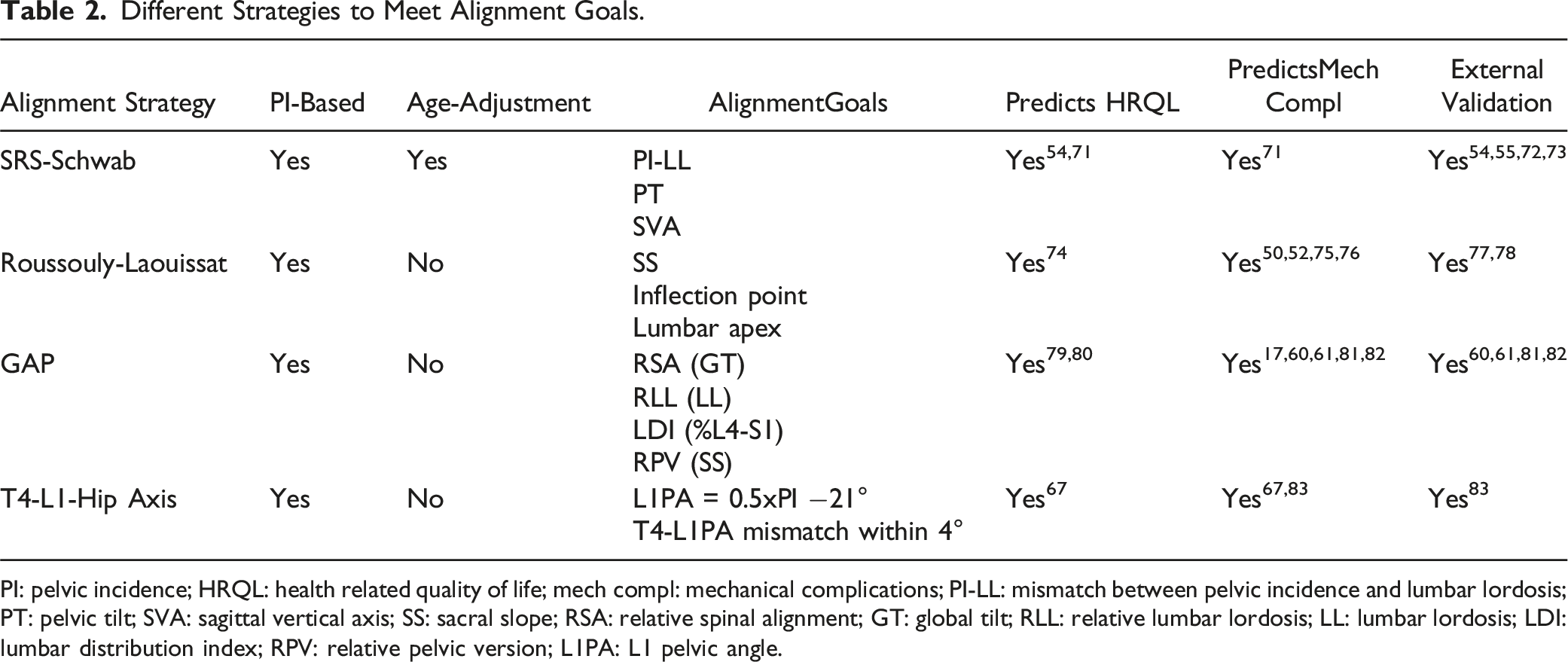
PI: pelvic incidence; HRQL: health related quality of life; mech compl: mechanical complications; PI-LL: mismatch between pelvic incidence and lumbar lordosis; PT: pelvic tilt; SVA: sagittal vertical axis; SS: sacral slope; RSA: relative spinal alignment; GT: global tilt; RLL: relative lumbar lordosis; LL: lumbar lordosis; LDI: lumbar distribution index; RPV: relative pelvic version; L1PA: L1 pelvic angle.
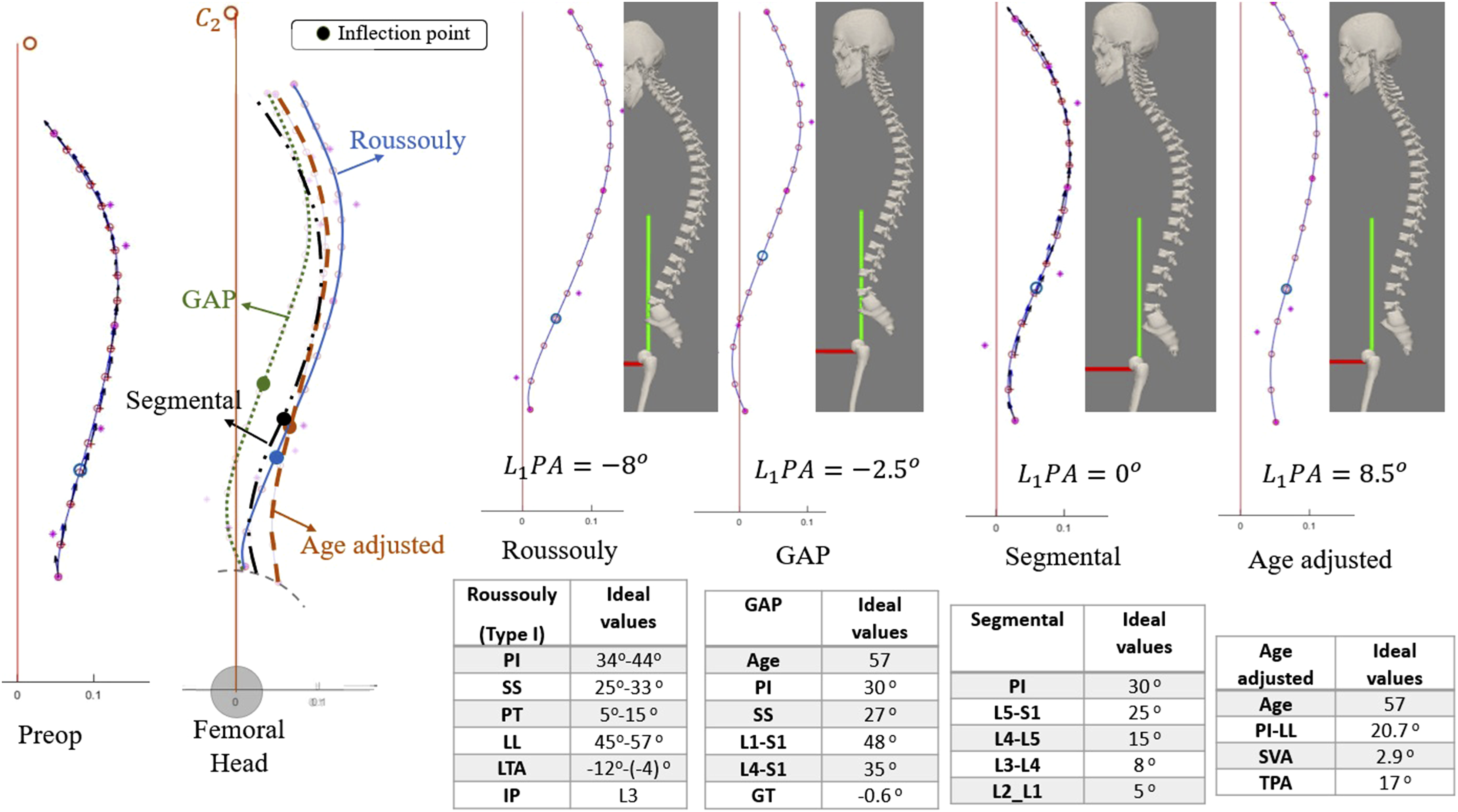
The comparison between four realignment strategies; Roussouly, age-adjusted, segmental, and GAP for a 57-year-old patient with PI = 30.
Reaching alignment goals as proposed by the SRS-Schwab classification is associated with better health-related quality of life 54 and fewer mechanical complications. 71 However, even among theoretically well-aligned patients, the rates of mechanical complications are still high. 84 The SRS-Schwab classification was based mainly in SVA (that does not reflect compensatory mechanisms) and PI-LL mismatch, ignoring qualitative parameters reflective of proper realignment such as lordosis shape 85 and distribution. 86 Roussouly 18 determined the high stress region in the spine and elucidated the need for proper range of lumbar distribution index (LDI), such that lower LL or flat back results in higher stress on the discs. The downside of his classification (and any other) is that it categorizes patients by PI when PI describes a continuum. 8 Alignment according to the GAP 17 score reflects ideal shape and distribution in a quantitative fashion depending on individual variability (relative pelvic version, relative LL, lordosis distribution index, and eventually relative sagittal alignment), but dismisses the thoracic region. Roussouly et al and GAP developers specified the range of 50% to 80% for its distribution in aligned cases and asserted that LDI paired with relative LL are associated with mechanical failure. 87 The reciprocal relationships between sacral orientation and spinal sagittal shape characteristics were well described in the study by Laouissat et al. 51 which illustrated that as undercountoured rod induces a pelvic retroversion, overcountoured causes postoperative hyperlordosis leading to postoperative iatrogenic anteversion of the pelvis. Finally, the T4-L1-Hip Axis seems to be a promising next step in sagittal alignment evaluation, accounting for both distribution and magnitude (spinal shape). However, although this method has been applied and tested in two adult deformity databases,67,83 it is still too novel, we still lack sound external validation.
One drawback of most alignment strategies is that they do not take TK or C2 Tilt into account. Some established alignment goals cannot be directly controlled during surgery, since most are just the expression of compensatory mechanisms or reciprocal changes (SVA, GT, TPA). If we consider the different interrelations of spinal curvatures Figure 2, we can understand the importance of restoring the lower lumbar arc to meet its ideal parameters, setting the lumbar apex in proper position, and extending the upper lumbar arc just as much as PI indicates, avoiding overcorrection and minimizing the posterior tilt of the inflection point.
Conclusions and Areas for Future Research
Although significant advances have been made in our understanding of what constitutes ideal spinal alignment, the topic remains controversial.88,89 It remains unclear whether ideal alignment for a fused spine should be the same as ideal alignment for an unfused spine, since the unfused patient is at no risk for mechanical failures and does not rely on unfused segments for compensation.
With regard to age-adjusted alignment thresholds, controversy exists whether older patients should be universally assumed to warrant less correction and be satisfied with greater positive sagittal malalignment and pelvic retroversion. If ideal alignment is based on patient age, this may guide us to fuse properly aligned elderly patients in mal-aligned (age-adjusted alignment) sagittal plane positions, which likely is not ideal. Further, if age-adjusted alignments goals are truly correct, what would be the long-term impact on a younger adult, instrumented and fused to age-adjusted alignment goals, in 20, 30, or 40 years following their fusions?
Modern medicine is moving toward more individualized patient care, including for ASD.90–92 There is growing recognition that ideal spinal alignment is not monolithic based on any single factor including age, but instead should be more individually defined. 88 Patient-related factors, that have not been accounted for in recent research (biology, genetics, -omics, etc) may contribute to the high rate of complications occurring after ASD surgery. 93 Nevertheless, we believe the concept of alignment targets to normalize shape-distribution-magnitude and eliminate compensatory mechanisms is important and worthy of future research.39,94 Ideal alignment and correction goals may need to account for variations in spinal morphology,51,52,74,89 individual patient symptoms and expectations, and tolerance for correction based on patient health and comorbidities. Individualized alignment goals may aid in balancing the risks and benefits of more aggressive corrections. Such complex modeling will likely require a large number of patients and may benefit from advances in machine learning and artificial intelligence. 90
Footnotes
Author Contributions
All authors have done: Substantial contributions to the conception and design of the work, acquisition, analysis, or interpretation of data. Drafting the work and revising it critically for important intellectual content. Final approval of the version to be published. And all authors agree to be accountable for the author’s own contributions and for ensuring that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and documented in the literature
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. All authors are sending their COI.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was organized and financially supported by AO Spine through the AO Spine Knowledge Forum Deformity, a focused group of international Adult Spinal Deformity experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Support was provided directly through AO Network Clinical Research.
Ethical Statement
ORCID iDs
Data Availability Statement
Not applicable as no patient data is included in the study. Data regarding the literature review is available upon request.