
Abstract
Study Design
retrospective study.
Objective
To investigate the incidence of all-cause revision surgery between plated vs stand-alone cage constructs for single level ACDF.
Methods
We retrospectively analyzed a commercial insurance claims database. Patients 18–65 years-old were included if they underwent single-level inpatient ACDF (defined with CPT codes) from 2010 – 2018, with a minimum of 2-year continuous insurance enrollment. The primary independent variable was the use of anterior plating vs zero profile device or stand-alone cage. Synthetic (ie, metal, PEEK, etc.) vs allograft interbody was a secondary independent variable. The primary outcome variable was revision cervical arthrodesis after the index operation.
Results
In total, 21092 patients undergoing single-level inpatient ACDF were included. 10.0% received a stand-alone cage during the index operation. Mean follow-up duration was 4.5 years. Revision arthrodesis occurred in 8.2% of patients overall, at a mean of 2.4 years after the index surgery. Patients with anterior plating had a lower rate of all-cause revision surgery in unadjusted (overall rate 8.1% vs 9.6%, P = 0.0185) and adjusted analysis (OR 0.78, P = 0.0016) vs stand-alone cages. Patients with stand-alone cages had higher rates of revision with a posterior approach than did patients with plated constructs. In sub-analysis, the combination of a stand-alone interbody device with an allograft had significantly higher odds of revision than other combinations of devices.
Conclusion
Among commercially insured patients ≤65 years-old undergoing single-level ACDF, anterior plating was associated with a reduced incidence of revision surgery compared to stand-alone cages within the follow up period of our study.
Keywords
Introduction
Anterior cervical discectomy and fusion (ACDF) was first described in the 1950s, 1 and is one of the most commonly performed cervical spine surgeries around the world. Approximately 137000 ACDF procedures are performed in the United States annually, and the incidence is expected to increase markedly over the next two decades.2–4
The vast majority of ACDFs are performed using an interbody device or allograft interbody stabilized with an anterior plate. 4 The concerns with anterior plating are potentially elevated risks of dysphagia and adjacent segment disease. 6 Zero-profile devices, also known as stand-alone anterior cervical cages, were developed to address these issues, wherein the interbody itself is directly fixed to the adjacent vertebral bodies obviating the need for an additional anterior plate. The concern with zero-profile devices is a potentially elevated risk of pseudarthrosis.6,8 A number of studies have compared outcomes of ACDF with anterior plating vs stand-alone cages,1,2,5–13 concluding relatively few differences in clinical outcomes, and mixed radiographic outcomes.
The aim of our current study was to investigate the incidence of all-cause revision surgery between plated vs stand-alone cage constructs for single level ACDF. We hypothesized that revision surgery would occur less frequently among patients with anterior plating vs those with stand-alone interbody devices due to additional biomechanical stability.
Methods
Data Source
This was a retrospective cohort study using the MarketScan database (IBM Watson Health, Ann Arbor, MI). The MarketScan database contains approximately 35 billion claims from >300 private insurers. Patients included in the database are ≤65 years-old, enrolled in plans such as those provided by large, self-insured companies, as well as early retirees, Consolidated Omnibus Budget Reconciliation Act (COBRA) enrollees, and their dependents. Institutional Review Board approval was not needed for this study.
Patient Selection
Informed consent was not required due to being a database study. Patients were included in the study if they met all of the following criteria: presence of a CPT code for anterior cervical discectomy and fusion (22551, 22554) as an inpatient from 2010 – 2020; underwent a single-level procedure (defined as the absence of CPTs for additional levels [22552, 22585, 22846, 22847]); were between ages 18 – 65 at the time of surgery; and had a minimum of 2 years post-operative continuous enrollment in the database. Due to minimum follow-up requirements, only patients from 2010 – 2018 were ultimately included. Patients with traumatic, infectious, or oncologic etiologies were excluded.
Variables
The primary independent variable in this study was the use of anterior plating (CPT code 22845). The primary dependent variable was the occurrence of revision arthrodesis, defined using CPT codes. Both inpatient and outpatient revision surgeries were included. A revision was defined as the presence of CPT codes for cervical arthrodesis (22600, 22551, 22552, 22554) after the date of the index procedure. Revisions were stratified by approach and setting. Additional variables were age, sex, year, and region. Subanalysis was performed based on the presence of an allograft vs synthetic interbody device (synthetic: CPT 22851/22853).
Statistical Analysis
Descriptive statistics were generated. Chi squared testing was used to assess differences in proportions of revision arthrodesis by anterior plating vs stand-alone cage instrumentation. Multivariable logistic regression was utilized to adjust for confounding factors including age, sex, year, and region. Subanalysis was further performed with multivariable logistic regression. Survival analysis was performed to assess the proportion of patients undergoing revision over time. Statistical significance was considered P < 0.05. All analysis was performed using SAS 9.4 (SAS Institute, Cary, NC).
Results
Study Population
Descriptive Statistics.
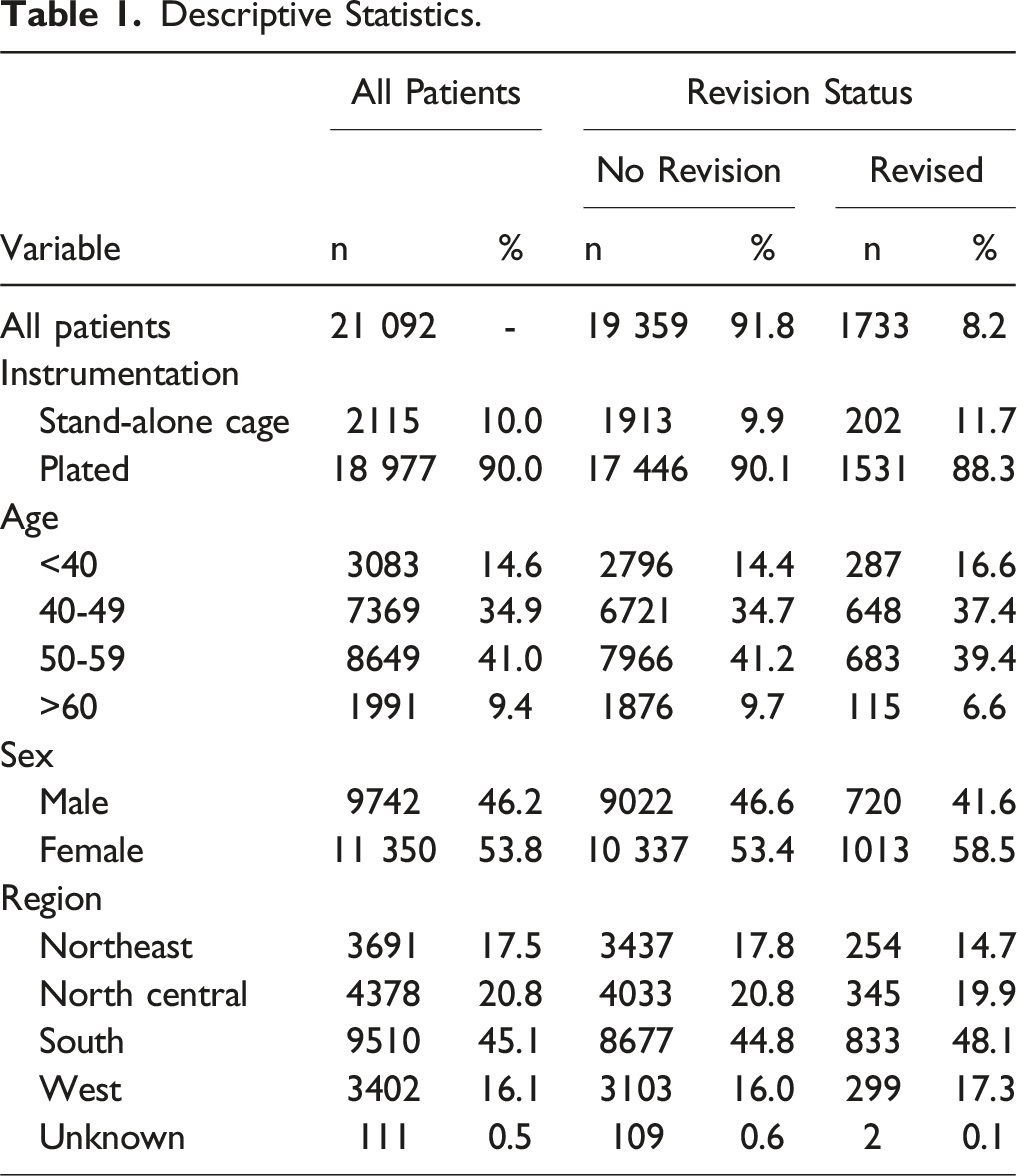
Revision Surgery
Revision surgery occurred in 8.2% (n = 1733) of patients and occurred at a mean of 869 days after the index surgery (2.4 years, SD 693 days). (Figure 1) The vast majority of revisions were anterior approach-only (69.3%, n = 1201), with a smaller proportion of posterior-only (22.2%, n = 385) and combined surgeries (8.5%, n = 147). (Table 3) Most revisions occurred in the inpatient setting (78.1%, n = 1354). Revision Surgery by Days Following Index Surgery.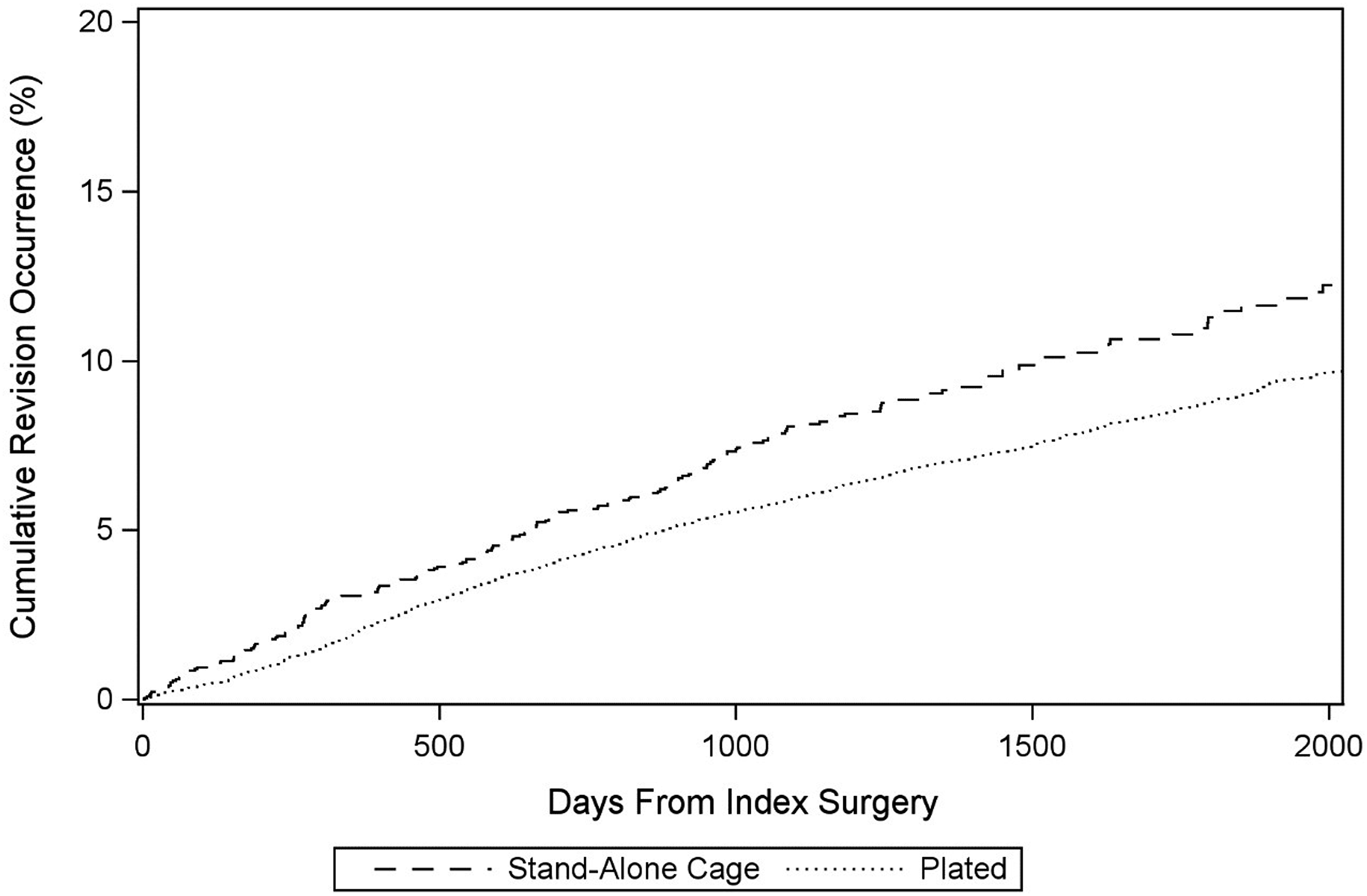
Revision Surgery by Index Surgery Type.
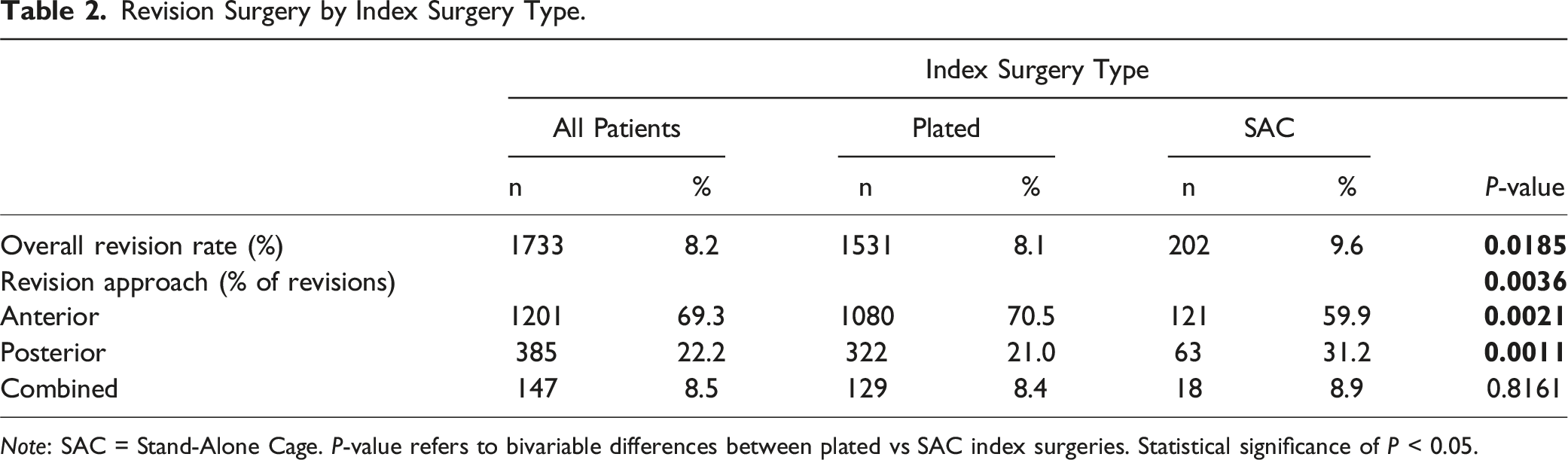
Note: SAC = Stand-Alone Cage. P-value refers to bivariable differences between plated vs SAC index surgeries. Statistical significance of P < 0.05.
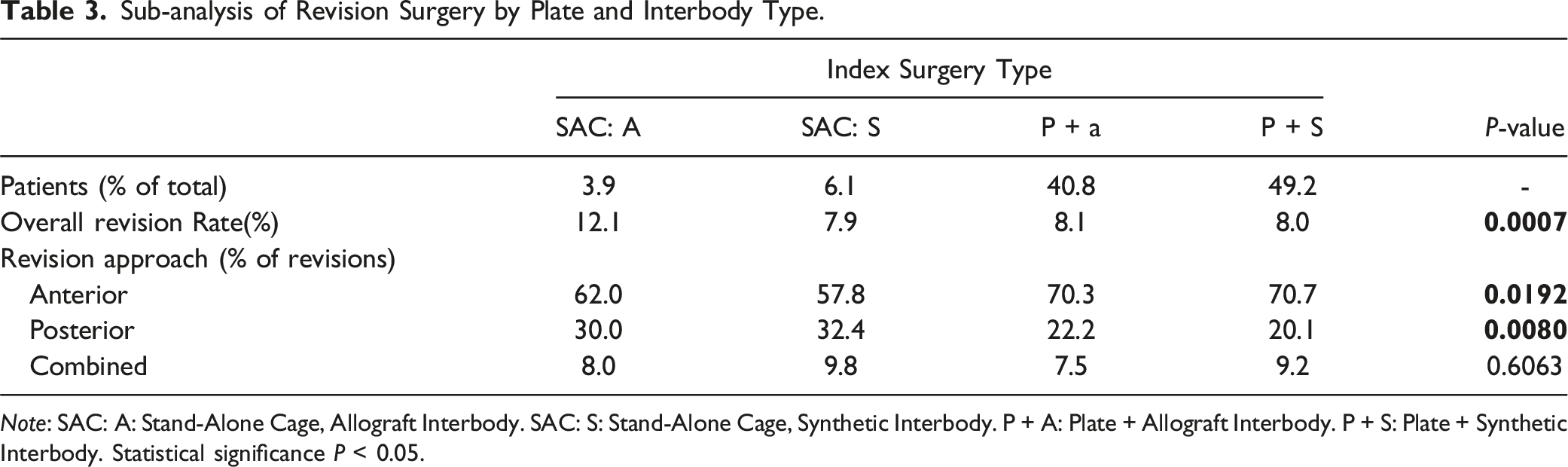
Subanalysis–Allograft vs Synthetic Interbody Device
A sub-analysis was performed, stratifying results by the presence of an allograft vs synthetic interbody device. Overall, 3.9% of patients had a stand-alone cage with allograft (SAC:A), 6.1% stand-alone cage with synthetic interbody (SAC:S), 40.8% plated with allograft interbody (P + A), and 49.2% plated with a synthetic interbody (P + S). In bivariable analysis, the proportion of patients who underwent revision surgery was highest in the SAC:A group: SAC:A 12.1%, SAC:S 7.9%, P + A 8.1%, P + S 8.0% (P = 0.0007). In multivariable analysis, adjusting for confounding factors, SAC:A was associated with markedly increased odds of revision vs P + S (OR 1.65, 95%CI 1.32 – 2.06, P < 0.0001). There was no significant difference between SAC:S and P + S (P = 0.5168). (Figure 2) (Table 3). Revision Surgery by Days Following Index Surgery–Subanalysis By Interbody Type. Sub-analysis of Revision Surgery by Plate and Interbody Type. Note: SAC: A: Stand-Alone Cage, Allograft Interbody. SAC: S: Stand-Alone Cage, Synthetic Interbody. P + A: Plate + Allograft Interbody. P + S: Plate + Synthetic Interbody. Statistical significance P < 0.05.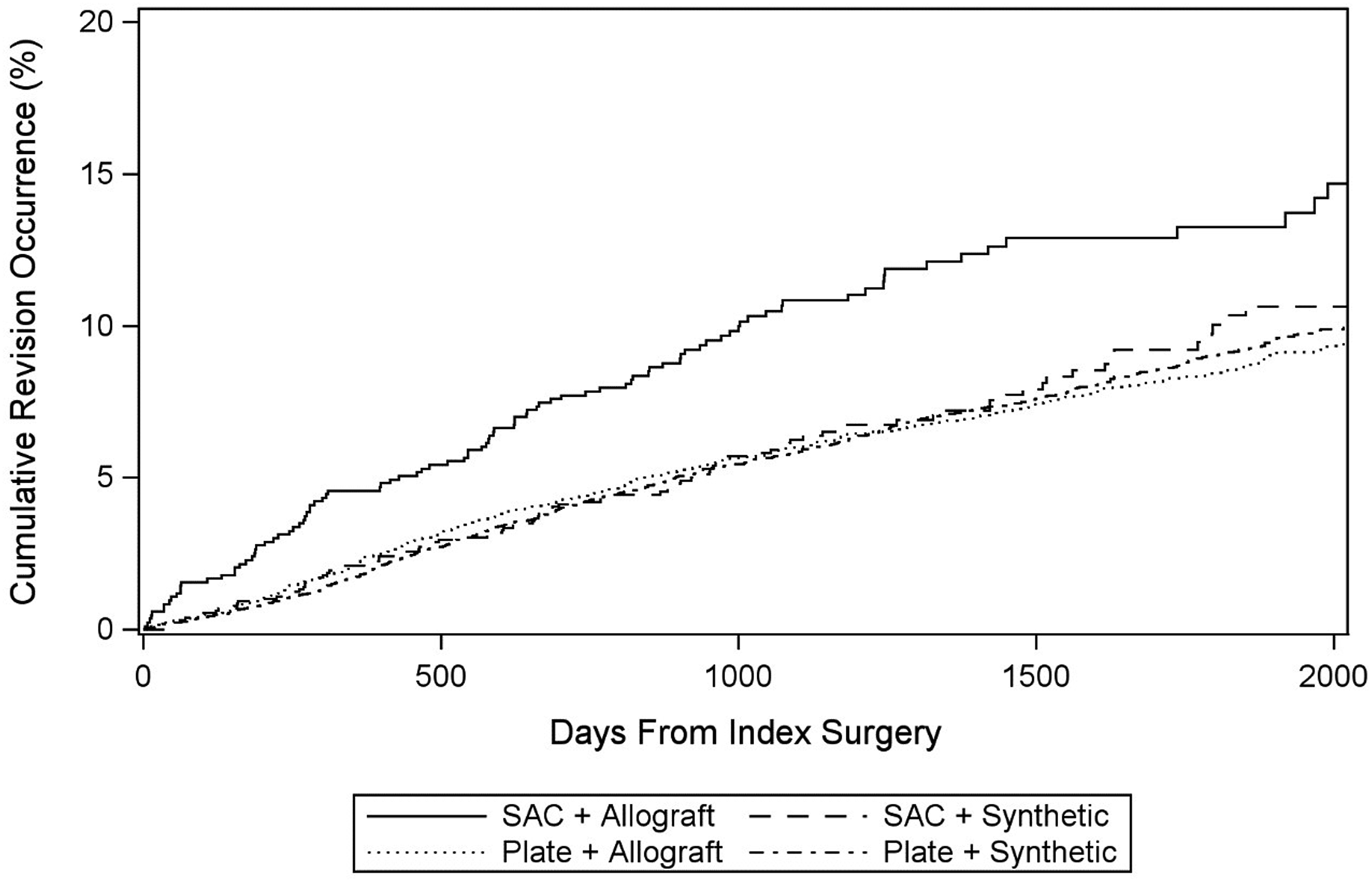
Discussion
This study analyzed a large, commercial insurance dataset of patients ≤65 years-old undergoing single-level ACDF in the inpatient setting, and found approximately 10% of patients received a stand-alone cage during the index operation. Revision arthrodesis occurred in approximately 8% of patients overall, with a higher revision rate with stand-alone cages compared to plated constructs. Sub-analysis revealed patients undergoing surgery with stand-alone cages with allograft interbody devices to be at particularly elevated risk of revision surgery.
Evidence comparing anterior plating vs stand-alone interbody devices in ACDF has been mixed, even among high-quality trials. A recent systematic meta-analysis by Zhao et al 7 included 7 randomized trials found no significant differences in arthrodesis rates, JOA scores, VAS pain scores, NDI score, length of hospital stay, and radiographic parameters including subsidence, cervical lordosis, segmental angulation, or disc height. The authors reported lower rates of adjacent segment ossification with stand along cages. 7 In another meta-analysis, Cheung et al 5 analyzed 19 studies (15 retrospective, 4 prospective) and found that stand-alone cages were associated with lower incidence of postoperative dysphagia, but higher rates of subsidence, and less restoration of cervical lordosis as compared to plated ACDF. 5 Neither of these studies reported a comparison of all-cause revision rates, likely due to limited follow-up of the analyzed trials. In our study, the mean duration of follow-up was 4.5 years, and we found that revision rates increased steadily with time after the index surgery in both groups.
The most common reasons for revision surgery after ACDF are symptomatic adjacent segment degeneration and symptomatic pseudarthrosis at the index level. We found that patients with stand-alone cages had higher rates of revision with a posterior approach and patients with plates had higher rates of revision with an anterior approach. Our results are consistent with the literature, which generally supports higher rates of adjacent segment degeneration with anterior plating and higher incidence of cage subsidence and pseudarthrosis with stand-alone cages. Litrico et al conducted a retrospective cohort study of 288 patients undergoing ACDF with a mean 14.5 year follow-up 14 and observed adjacent segment disease requiring revision in 5.9% patients. Yue et al. performed a similar retrospective review of 71 patients with 7.2 years mean follow-up after ACDF with anterior plating, and observed a 19.7% revision rate, where the vast majority were for adjacent segment degeneration. 15 Wu et al. retrospectively followed 57 patients who underwent ACDF with a stand-alone cage with minimum 5-year follow-up, observing a relatively high rate of cage subsidence (19.1%). 16 Finally, Zhou et al compared stand-alone cage with anterior-plated ACDF with a minimum 3-year follow-up in 98 patients, 17 and observed high rates of adjacent segment degeneration for anterior plating (14.9% vs 2.0%), but no differences in clinical outcomes, subsidence or arthrodesis rates between the groups.
In sub-analysis, we observed that patients with stand-alone cages with allograft interbody devices were at particularly elevated risk of revision surgery. The odds of revision were not increased for patients with stand-alone cages and synthetic interbody devices. Interestingly, a previous study by Marrache et al 18 demonstrated that, overall, synthetic cages are associated with higher rates of all-cause reoperation after ACDF. 18 Taken together, our results suggest that a stand-alone cage with an allograft interbody may be particularly predisposed to failure, via pseudarthrosis, implant malfunction, or another mechanism. Further research examining these devices maybe warranted.
Our study demonstrated that approximately 30.7% of revision surgeries were performed either posteriorly alone or anterior-posterior combined. These techniques are often used to treat symptomatic pseudarthrosis after anterior fusion. We found that the rates of posterior or combined revision were particularly higher for patients with stand-alone cages, suggesting that there may be higher rates of symptomatic pseudarthrosis with stand-alone cages compared to plated constructs. However, we are limited in our study by the lack of clinical variables to ascertain the exact reason for revision (eg, pseudarthrosis, adjacent segment disease, degeneration at distant segments, instrumentation failure, etc.). Additional limitations of our study include coding errors inherent to claims analysis, missing confounding factors in multivariable analyses, and lack of data on patients who switched insurances and were excluded due to lack of minimum 2-year follow-up.
Conclusions
Among commercially insured patients ≤65 years-old undergoing single-level inpatient ACDF, anterior plating was associated with a reduced incidence of revision surgery compared to stand alone cages within follow up period of our study. Patients with a stand-alone cage were particularly at risk for revision surgery. Further long-term and more in-depth studies are warranted to assess specific clinical reasons for revision, and whether differences in risk of revision surgery exist between specific stand-alone cage designs, particularly those with allograft interbody devices.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.