
Abstract
Study Design
Retrospective Cohort Study.
Objective
The primary objective of this study is to evaluate the efficacy of early administration of Teriparatide in preventing the necessity of surgical intervention in individuals with osteoporotic vertebral compression fractures.
Methods
In a 24-month follow-up retrospective analysis, 191 OVCF patients from January 2016 to October 2020 were randomly assigned to Non teriparatide Group A (n = 104) or Group B teriparatide (n = 87). At baseline, 6 months, 1 year, and 2 years following treatment, demographic data and need of surgical intervention, VAS, ODI, union rates, and kyphosis development, were examined.
Results
Our study found that non-teriparatide group individuals had an 11.53% higher risk of non-union formation that required surgery. Only 8.63% of teriparatide group patients needed surgery. Both groups had significant VAS score reductions. Non-teriparatide group scores declined from 8.38 ± 0.74 to 3.15 ± 1.40, while teriparatide group scores decreased from 8.49 ± 0.73 to 1.11 ± 0.31. The 2-year follow-up ODI scores significantly decreased, with values of 25.02 ± 13.94 for non-teriparatide patients and 15.11 ± 2.17 for teriparatide patients. The kyphosis progression angles in the teriparatide group were considerably lower (4.97 ± 0.78°) compared to the other group (8.09 ± 1.25°).
Conclusion
With increasing elderly populations, it is necessary to take measures to prevent surgical intervention in osteoporotic spinal compression fractures. Teriparatide can be employed as an early medication in the management of these fractures to avert non-union and the minimise the progression of kyphosis.
Introduction
Osteoporotic vertebral compression fractures (OVCF) are increasingly recognised as a substantial health concern affecting the elderly population, particularly in developing nations that poses significant problems to the worldwide health care sector. Fragility fractures are associated with intense back pain, aberrant posture, gastrointestinal or respiratory disturbances, and poor prognosis leading to diminished quality of life. 1 These fractures, characterised by their fragility, can also lead to notable depression and psychosocial issues in older individuals. 2
Antiresorptive treatment with bisphosphonates are the standard currently being used, has been shown to decrease pain and the chances of vertebral collapse by 40% - 50%, but are still considered to be insufficiently effective in preventing the risk of fracture non-union in OVCF. 3 Risedronate, zoledronate (ZOL), and alendronate are often utilised bisphosphonates that offer both convenience and cost-effectiveness.
Unlike bisphosphonates, which are primarily antiresorptive treatments, teriparatide has been increasingly popular in the past decade for managing fractures due to its crucial function in regulating the calcium and phosphate pathway. Teriparatide (TTPD) is a synthetic version of human parathyroid hormone that enhances the activity of osteoblasts. Teriparatide (rPTH) is a pharmacological agent with anabolic properties that specifically targets PTH type 1R receptors found on several cell types including osteoblasts, osteocytes, and renal tubular cells. PTH type 1R receptors are G-protein-coupled receptors that play a crucial role in the effects of PTH on the regulation of calcium and phosphate levels and bone health. Activation of adenylate cyclase (ACN) through Gs and activation of protein kinase C (PKC) through Gq occur as a result of ligand binding to the receptor. Adenylate cyclase produces cyclic adenosine monophosphate (cAMP), which triggers the activation of protein kinase A (PKA). The PKA-dependent route is largely utilised for its anabolic and catabolic effects on bone, even though PTH activates both PKA- and PKC-dependent signalling pathways. 4
Teriparatide has been demonstrated in numerous previous studies to effectively enhance lumbar bone mineral density (BMD), hence aiding in the treatment of osteoporosis. 5 Bisphosphonates exhibit a comparatively lower impact on bone mineral density (BMD) as compared to teriparatide. Additionally, they are associated with undesirable effects such as osteonecrosis of the jaw or atypical femoral fractures. 6,7 The primary distinguishing feature of TTPD, as compared to bisphosphonates, is its anabolic effect which has the propensity to stimulate bone formation and enhance osteoblast activity, resulting in increased bone production in osteoporotic vertebral compression fractures.8–10
The primary objective of this study is to evaluate the efficacy of early administration of TTPD in preventing the necessity of surgical intervention in individuals with osteoporotic vertebral compression fractures (OVCF). The purpose of this study is to examine the development of local kyphosis, the likelihood of non-union, the improvement in fracture union, and the clinical and radiological outcomes in terms of preventing surgery and disease progression in Osteoporotic vertebral compression fractures treated with early Teriparatide.
Materials and Methods
This study retrospectively analysed a cohort of 191 patients who visited our spine outpatient department with an osteoporotic vertebral compression fracture between 2016 and 2020. These patients were treated conservatively and followed up prospectively over time. The analysis was conducted after obtaining approval from the local ethics committee and the institutional review board (Bombay hospital and Medical research centre [BH-EC-0133]). Informed consent was obtained from all patients before to treatment, and the utilisation of this data for further research analysis was elucidated. The treatment plan provided to all patients consisted of conservative therapy, which involved pain management through the use of NSAIDs and opioids. During the initial acute pain phase, which lasted for the first 2 weeks of treatment, only nonsteroidal anti-inflammatory medications (NSAID) and opioids were given. Consequently, the dosage of these medications was gradually decreased and eventually stopped for all patients. In addition, patients were instructed to utilise a lumbo-sacral belt for support, and early mobilisation was performed based on their individual pain threshold. The current study followed a specific procedure in which all participants were allowed to engage in their regular daily activities while wearing the lumbo-sacral (ls) belt. Every patient received ergonomic education to promote the prevention of sudden and unregulated movements. Furthermore, patients were not explicitly advised to engage in complete bed rest until they experienced acute and intense discomfort. Every patient was offered osteoporosis treatment consisting of bisphosphonates and teriparatide, based on their acceptability and compliance with anabolic and anti-resorptive drugs. All patients were provided with comprehensive treatment including nutrition and hydration, a diet rich in protein, as well as supplementation of vitamin D and calcium.
The cohort was subsequently separated into two distinct groups: Group A, consisting of patients who chose not to undergo combination therapy which included teriparatide, and Group B, consisting of patients who elected to receive treatment with combination therapy of teriparatide and bisphosphonates. All treatment methods adhered to, as previously stated, were same in both groups. Group A was administered Alendronate sodium 70 mg once weekly, while Group B (TTPD) got a daily subcutaneous injection of Teriparatide (20 μg/day) in addition to Alendronate sodium 70 mg weekly both for 18 months.
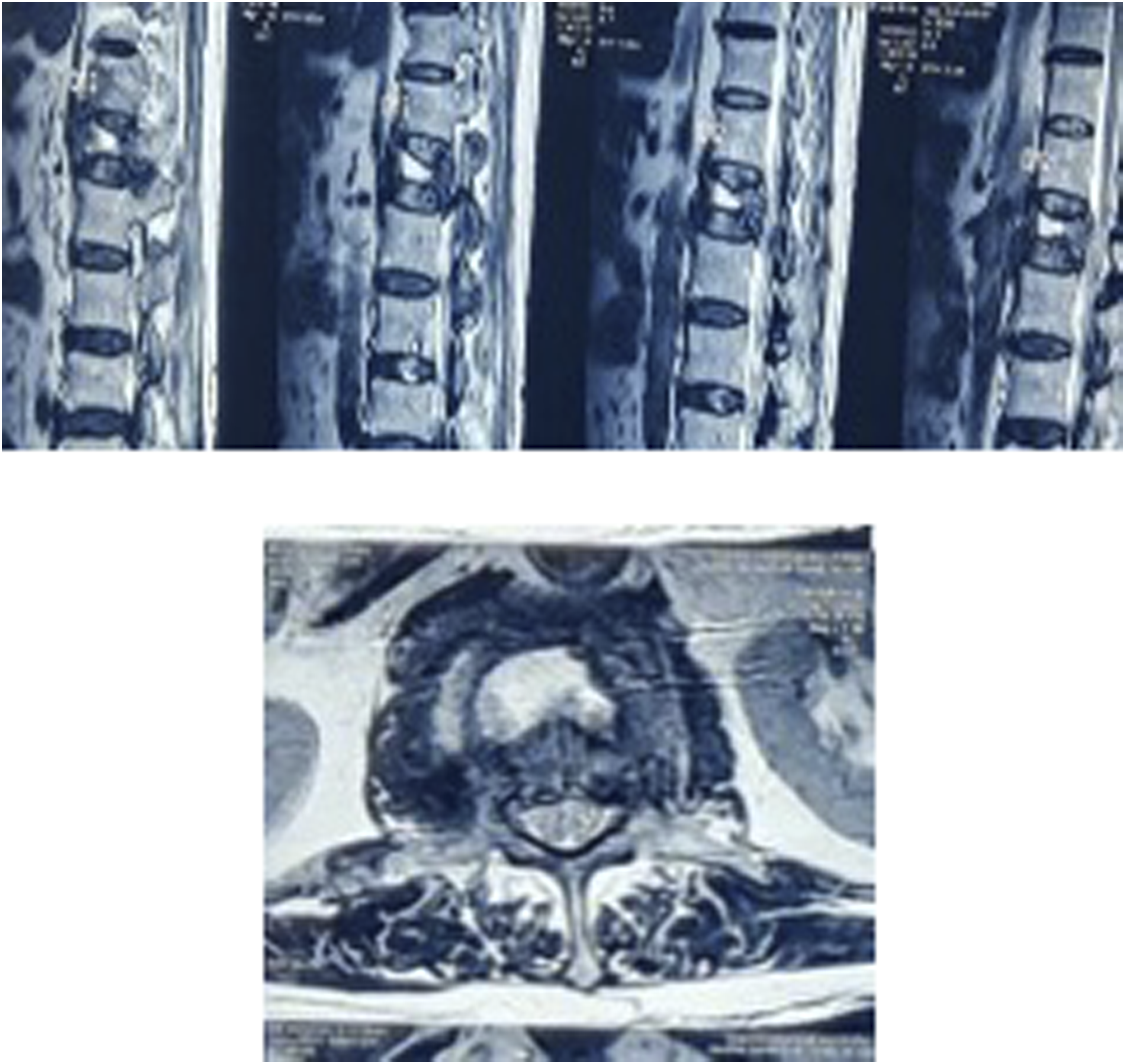
During a follow-up period of up to 2 years, surgical therapy was indicated based on the presence of progressing pain, new-onset discomfort, or any recent neurodeficit. Subsequent X-ray images were captured at regular intervals to assess the degree of local kyphosis in the affected area, with the patient lying on their side and sitting upright. The progression angles of segmental kyphosis in patients receiving Group A (Non Teriparatide) and Group B (Teriparatide) were measured at all follow-up visits to compare the advancement of kyphosis in both groups. The degree of segmental kyphosis was assessed using a lateral radiograph. This involved measuring the angle between a line parallel to the upper endplate of the upper vertebra and the lower endplate of the vertebra below, with respect to the fractured vertebra. Magnetic resonance imaging (MRI) was exclusively conducted on patients who exhibited any indication of non-union throughout the 6-month follow-up period.
Demographic factors, including age, sex, body mass index (BMI), bone mass density (BMD), percentage of vertebral body collapse, facet fracture involvement, and both end plate fractures, were collected and assessed in a retrospective manner for all patients at the initiation of the study. In order to evaluate the extent of pain alleviation and improvement in daily activities in both groups, we measured the visual analogue score (VAS) and Oswestry disability index (ODI) at the beginning and at regular intervals of 6 months, 1 year, and 2 years during the follow-up period. The study also examined the number of patients in both groups who required surgical intervention for pain relief due to failed medical therapy with new-onset neurodeficit, pseudoarthrosis, or non-union. The non-union diagnosis was confirmed by identifying a vertebral cleft or abnormal movement at the location of the fractured vertebra on the lateral sitting and lateral supine radiographs. If Non union was established or the need for surgical intervention was seen in patients taking only bisphosphonates, they were all asked to begin teriparatide for a period for 18 months.
Outcome scores were calculated for VAS by using the formula 100 * (preoperative VAS score minus postoperative VAS score minus preoperative VAS score/pre operative VAS). Similarly done for ODI = 100 * (preoperative ODI score - postoperative ODI score/preoperative ODI score). The results were subsequently categorised as exceptional (≥75%), good (≥50%), and average (<50%).
The inclusion criteria encompassed patients who visited our spine outpatient department (OPD) between 2016 and 2020, and met the following conditions: having an osteoporotic vertebral compression fracture (OVCF) below the sixth thoracic vertebrae level, seeking medical attention within 1 week after their fall, being above 55 years of age, and being willing to undergo medical management with antiresorptive/TTPD treatment.
The exclusion criteria for this study were as follows: patients who did not consent to undergo treatment with bisphosphonates or teriparatide, patients below the age of 55, patients with fractures above the sixth thoracic vertebrae level, patients with a diagnosed kummels lesion prior to starting treatment, patients who presented after 2 weeks of a vertebral compression fracture, patients with a history of previous use of antiresorptive treatment, patients with acute neurodeficit following a fracture, patients with fractures caused by other secondary factors such as infectious pathology, metastasis, or multiple myeloma, patients without follow-up or currently on steroid treatment, and patients with uncontrolled hypertension, renal/hepatic impairment, chronic tobacco use, or other significant medical conditions such as cancer.
Statistical Analysis
The variables were quantified as numerical values or percentages and analysed using either the chi-square or Fisher exact test. The results from both groups were compared using the Studentt test. For each attribute in both groups, we computed the mean values and standard deviations. An ANOVA test was conducted to assess treatment changes in both groups throughout all follow-up periods. The statistical analyses were conducted using SPSS 20.0, with a significance level of 0.05.
Results
The study comprised a total of 194 participants and was categorised into two cohort groups based on the treatment administered to the patients. At the conclusion of a 2-year follow-up period, demographic and statistical data were accessible for all patients, with the exception of two patients from Group A and 1 patient from Group B who were no longer being monitored. Group A, consisting of 104 individuals, received treatment with bisphosphonates alone, while Group B, consisting of 87 individuals, received treatment with Teriparatide and bisphosphonates.
Demographics.
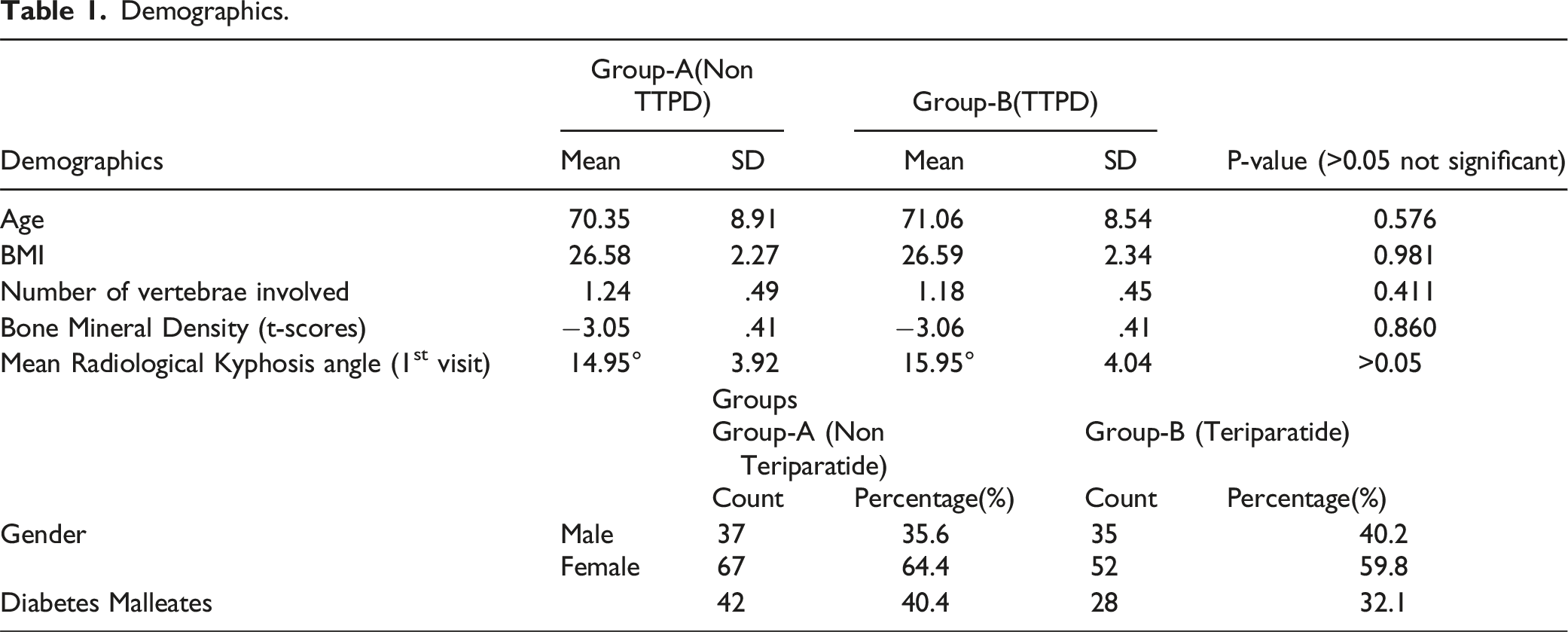
Group A, which received bisphosphonates alone, consisted of 37 male patients and 67 female patients. In contrast, Group B contained 35 male patients and 52 female patients. The group of patients taking bisphosphonates had a diabetes prevalence rate of 40.4%, whereas the group of patients on teriparatide had a diabetes prevalence rate of 32.1%. The proportion of vertebral body collapse was computed in both groups and assessed (Table 1). Group A (Non TTPD) consisted of 35.6% males and 64.4% females, whereas Group B (TTPD) contained 40.2% males and 59.8% females. No statistically significant differences were seen when comparing all demographic data. (P-value >0.05).
Incidence of Facet Fractures and Involvement of Both Endplate Fractures.

Variables VAS, ODI – Timeline after Initiating Treatment.

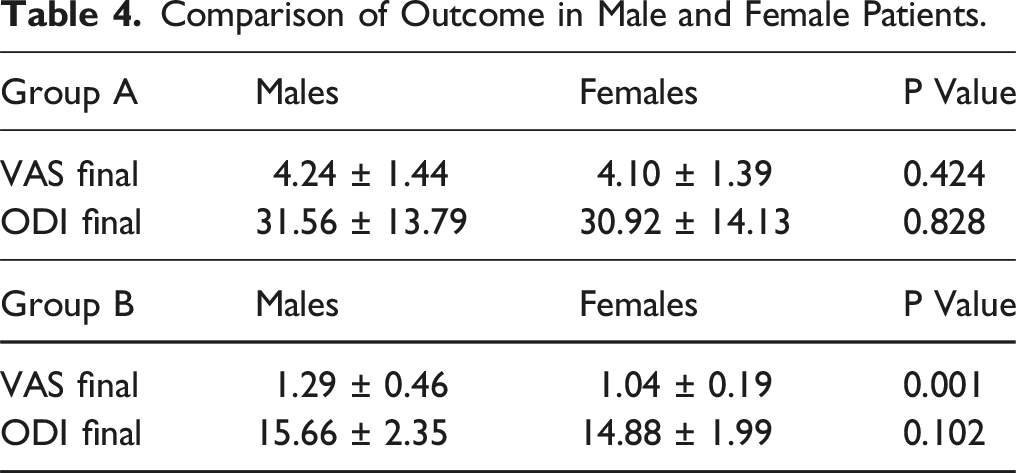
Comparison of Outcome in Male and Female Patients.
Radiological Comparison of Union/non-union.
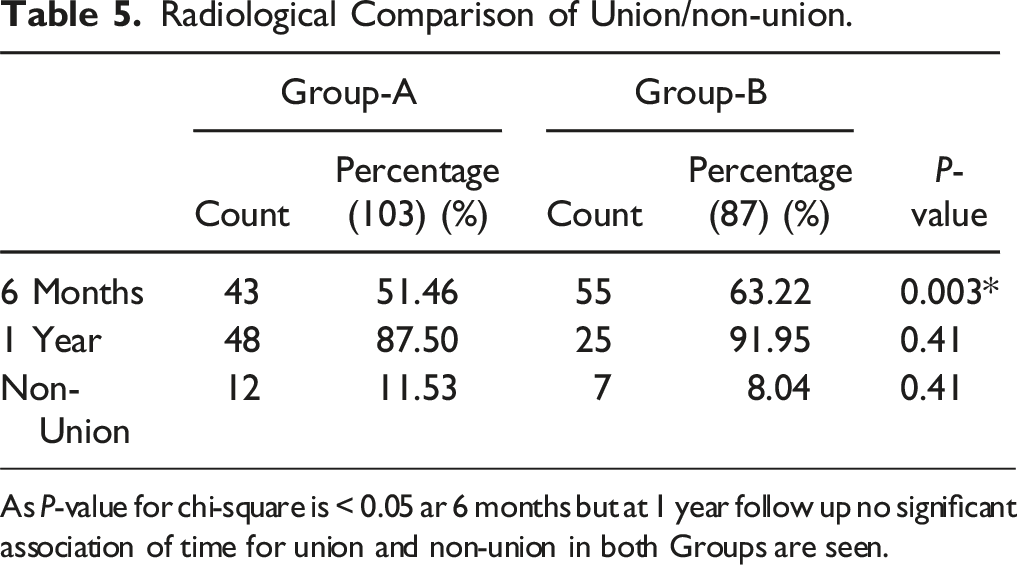
As P-value for chi-square is < 0.05 ar 6 months but at 1 year follow up no significant association of time for union and non-union in both Groups are seen.
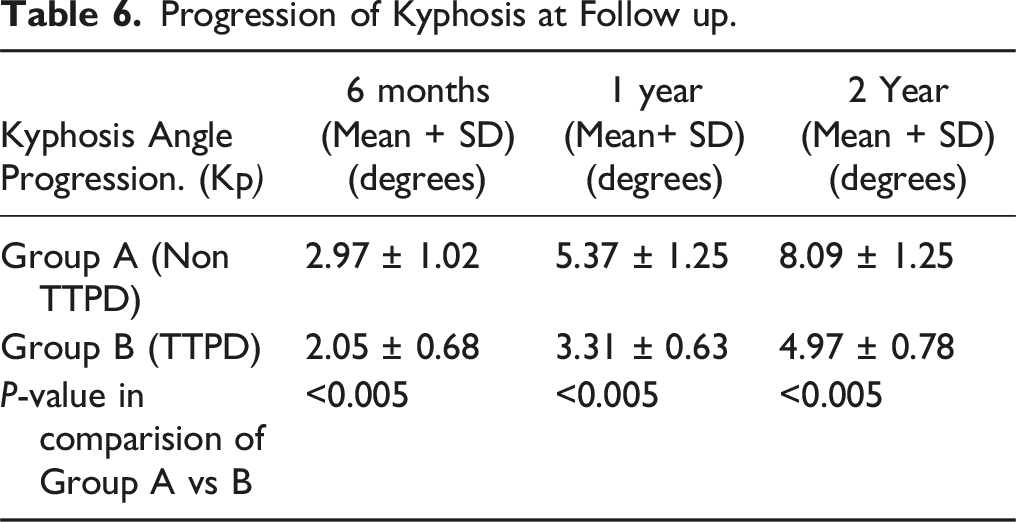
Progression of Kyphosis at Follow up.
SURGICAL INTERVENTIONS in BOTH GROUPS.

Discussion
The occurrence of non-union is a well-established phenomenon in the field of orthopaedics. Non-union is a complex condition affected by multiple factors, including the biology of healing, mechanical instability, and extrinsic factors such as osteoporosis, smoking, alcohol, and drug misuse. Pertaining to osteoporotic spine, most crucial factor is the biology of a non-healing fracture. Non-union in the osteoporotic spine has resulted in considerable impairment and has prompted the identification of teriparatide, a medication that has lately received great interest for its capacity to stimulate bone turnover markers through its anabolic actions. In a 2016 trial, teriparatide was compared to a placebo to assess its impact on bone biomarkers. The study revealed that teriparatide had favourable anabolic effects on bone turnover markers, potentially accelerating the healing process of fractures. 11
Both Group A and Group B demonstrated a positive overall impact in alleviating pain, as evidenced by a considerable reduction in VAS scores during the last follow-up assessment. Patients who receive treatment with anabolic and antiresorptive medications often experience a reduced occurrence of acute back pain exacerbation.
12
Chenz et al conducted a comparative analysis of pain scores between two groups: a control group and a group that was administered teriparatide. The group receiving teriparatide exhibited a notable decrease in pain levels as compared to the control group.
13
A study shown that 12 months of teriparatide treatment effectively reduced the bone mineral density (BMD) scores of the spine in 19 patients with osteoporotic fractures, from an initial average of 3.23 ± 0.24 to a final average of 2.88 ± 0.24.
14
Figure 1 Follow up X-rays of Group A(non-teriparatide) at 6 months, Follow up X-rays of Group A(non-teriparatide) at 1 year, Follow up X-rays of Group A(non-teriparatide) at 2 year.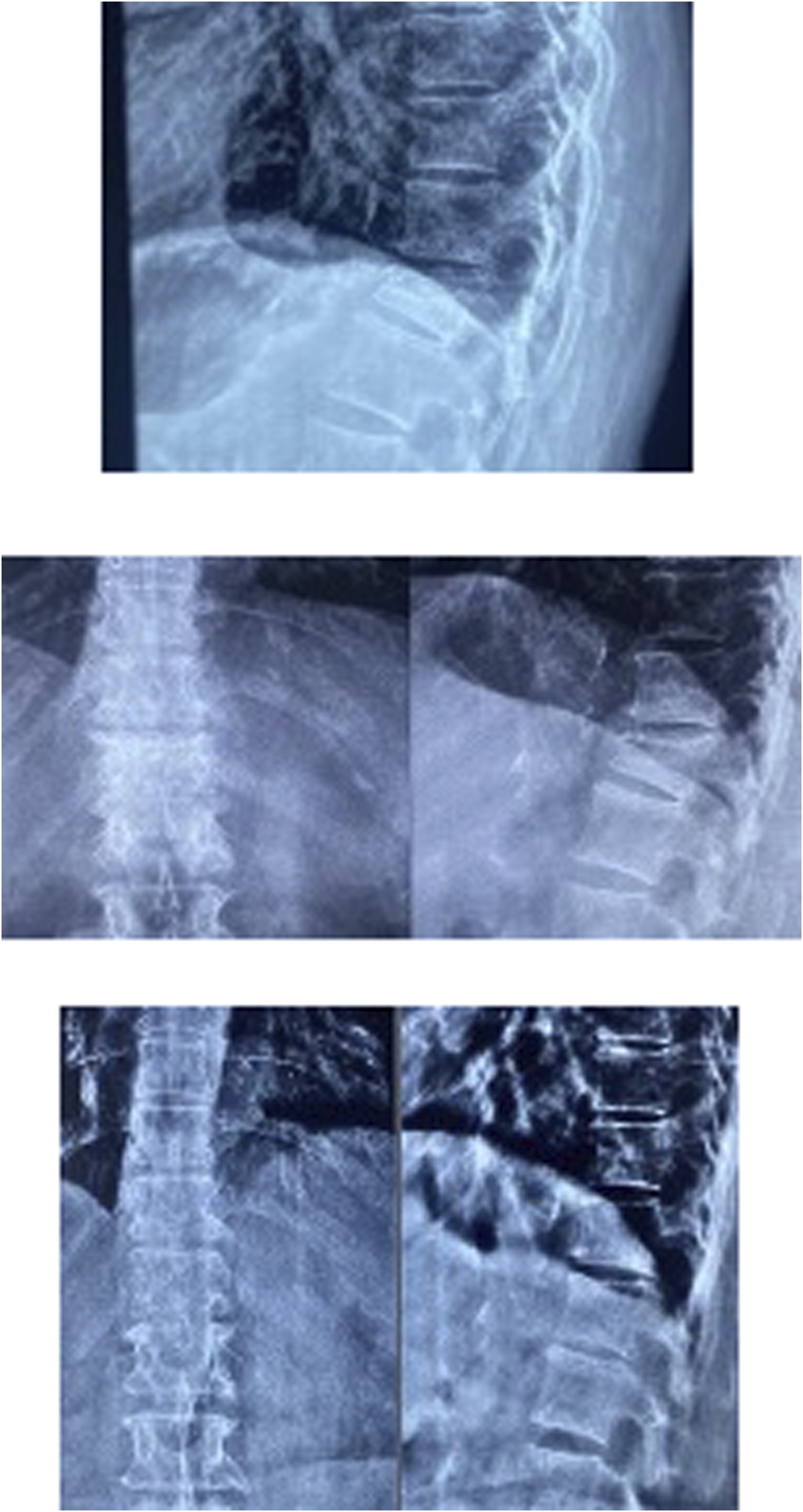
The main focus in this study comes to the prevention of surgical intervention in patients that are affected with osteoporotic vertebral compression fracture. Surgery is indicated in patients with intractable pain due to non-union and increase in local kyphosis resulting in high risk of neurological injury. A retrospective study done in 2021 on OVCF patients treated with teriparatide and alendronate showed that the area of bone mineralization in the teriparatide group (54.28%) was significantly higher than that of patients treated with alendronate (35.57%).
15
A meta-analysis done in 2021 showed that teriparatide was very superior to only Bisphosphonates in increasing BMD scores and was also helpful for postmenopausal women in the short- and long-term treatment of osteoporosis.
16
Many such studies have shown the efficacy of teriparatide in the fracture healing process. In patients treated with teriparatide (Figure 2), we are able to appreciate that there is good union seen radiologically at 2 years of follow-up and also a minimal Kp Figure 3. Follow up Xrays of Group B (Teriparatide) Xray images at 1st visit, Follow up Xrays of Group B (Teriparatide) Xray images at 1 Year, Follow up Xrays of Group B (Teriparatide) Xray images at 2 Years. Classic Non-union (kummels lesion) seen at 6 months in patient from Group A(non-teriparatide), Classic Non-union (kummels lesion) seen at 6 months in patient from Group A(non-teriparatide).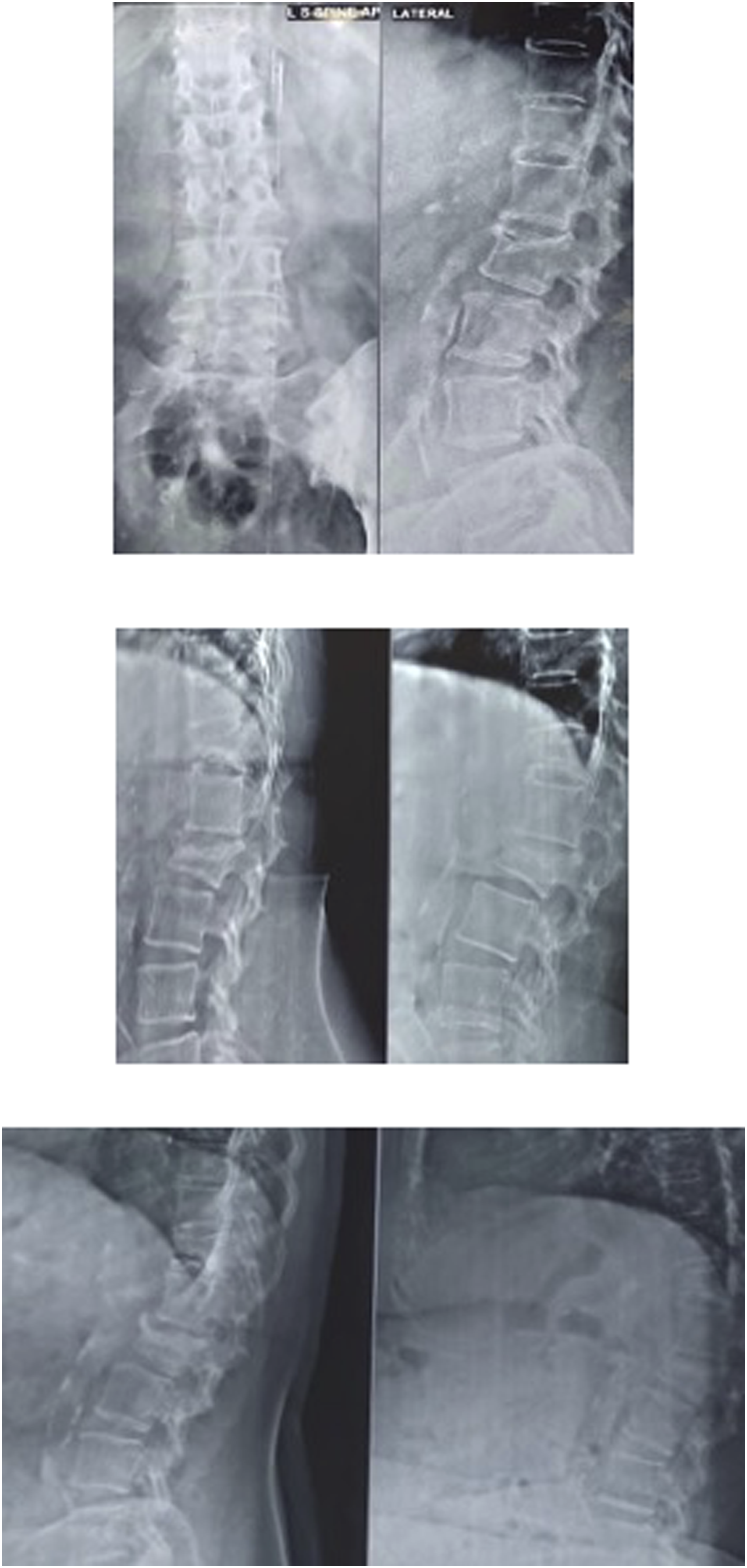
In our trial, we found that teriparatide medication resulted in faster rates of bone union. Specifically, only 5.75% of patients in the teriparatide group experienced non-union (also known as Kummels disease), compared to 10.68% in the bisphosphonate group. Preventing non-union (Kummels disease) is the primary treatment approach for patients with osteoporotic vertebral compression fractures (OVCF). Patients who develop non-union experience challenges in treatment, necessitating surgical interventions that may include extensive fixing of segments and the use of bone grafts or vertebroplasty. Patients suffering from non-union have persistent and unmanageable agony as a result of a fracture that does not heal. 17 Past investigations have consistently demonstrated that treatment with vertebroplasty or kyphotic correction produces favourable outcomes in patients with kummels disease. 18 Our study found that group A (Non TTPD) had an average outcome score in 29% between pre-treatment and last follow-up, 66% had a good score, and 5% had excellent. In contrast, group B (TTPD) had an average result score in 5.74%, 29.89% good, and 64.36% had an excellent score. (Figure 4) ODI results showed a similar trend, with group A (Non TTPD) scores of 24.30% average, 70.90% good, and 4.85% excellent. However, group B (TTPD) had just 4.60% average outcomes, 91.92% good outcomes, and 3.44% exceptional outcomes. (Figure 5).
Additionally, numerous studies have demonstrated the advantageous effects of TTPD in facilitating osseous fusion following spinal fusion or corrective surgery.8–10 Given its demonstrated efficacy in enhancing fusion following corrective spine procedures, further investigation is warranted to explore its potential for preventing the necessity of surgical intervention. Our study found that during the initial visit, the kyphosis angles in both groups were similar. However, during the regular monitoring with x-rays, the degree of Kyphosis progression was assessed at 6 months, 1 year, and 2 years. The results indicated that patients in Group A, who had just Bisphosphonates treatment, experienced a greater degree of progression. (Table 5). Patients who received teriparatide treatment experienced considerably reduced advancement in the local kyphosis angles. It has been established that progressive kyphosis can have specific repercussions on the patient, including the development of adjacent-level fractures and back pain for the patient. 19
The duration of our study included a 2-year follow-up period and this has provided insights into the fact that the early administration of teriparatide can enhance the likelihood of bone union and reduce the occurrence of a Kummels lesion. Operative intervention was necessary for complete resolution of pain in all patients with Kummels lesions. A 2020 study comparing teriparatide vs operational treatment for osteoporotic vertebral compression fractures (OVCF) demonstrated comparable clinical outcomes. However, teriparatide was deemed preferable due to its significant cost benefit over the operative approach. 19
All patients in both groups adhered to the treatment regimen, and there were no instances of treatment discontinuation in either the bisphosphonates or teriparatide groups. The limitations of our study include the inability to track bone turnover biomarkers and the absence of a Bone Mineral Density (BMD) examination to demonstrate the anabolic benefits of both groups. The scope of our research is restricted to a single centre. Therefore, doing a multicentre study with a long-term follow-up could offer a more comprehensive viewpoint.
Teriparatide has demonstrated a clear reduction in the necessity for surgical intervention in individuals with osteoporotic vertebral compression fractures (OVCF). Although literature discusses teriparatide primarily in the context of preventing secondary fractures, this study provides a clear annotation that early and primary treatment with teriparatide can enhance the rates of bone union and reduce the necessity for surgical intervention in elderly individuals with osteoporotic vertebral compression fractures.
Conclusion
The use of bisphosphonates as a standalone therapy regimen for osteoporosis is evidently ineffective due to its lack of inherent anabolic properties. However, if osteoporosis progresses to the point of a fracture occurring due to a minor injury, it is advisable to initiate early teriparatide treatment to potentially avoid the necessity of surgical intervention.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.