
Abstract
Study Design
Retrospective cohort study.
Objective
Geriatric vertebral compression fractures are the most common fracture associated with osteoporosis. Using a large national database, the current study aimed to examine and characterize bracing trends for geriatric thoracic/lumbar compression fracture management.
Methods
The current study utilized the PearlDiver database from 2015-2021. Patients who suffered thoracic/lumbar compression fractures (fifth thoracic to the fifth lumbar vertebra [T5-L5]) were identified. Exclusion criteria included patients less than 65 years old or an indication of infection or neoplasm. Patients who received a brace within 90-days after the initial diagnosis of thoracic/lumbar compression fracture were abstracted and characterized overall and by fracture level. Multivariable logistic regression was performed to assess for correlation with bracing trends.
Results
In total 290 388 patients met inclusion criteria and suffered a thoracic/lumbar compression fracture (greatest incidence at the thoracolumbar junction). Of these, bracing was only prescribed for 4263 (1.5%), with the greatest variance of 1.5% by level. Independent predictors of bracing were geographic region (relative to northeast, west WE odds ratio [OR] 1.31, Midwest OR 1.20), younger age (OR 1.27 per decade), female sex (OR 1.17), and ECI (OR 1.02 per 2-point increase) (P < .05 for each).
Conclusion
Overall, the current study examined over a quarter of a million patients who suffered a T5-L5 compression fractures and found that only 1.5% of patients were braced. This low percentage, and that greatest predictor for bracing was non-clinical (geographic region), highlight the inconsistency of this practice and may be useful for developing treatment algorithms.
Introduction
Geriatric thoracic/lumbar compression fractures (VCFs) are common injuries that typically result from low-energy mechanisms and are most common in individuals with decreased bone density.1-3 These are the most common fractures associated with osteoporosis and impact approximately 1.5 million people in the United States annually, 4 with increasing rates in older cohorts. 5
Nonoperative treatment is the mainstay of treatment for managing VCFs.6,7 This may include physical therapy, 8 bed rest, 9 orthosis/bracing, 9 and management of underlying osteoporosis.10,11 Some of these fractures may be considered for cement augmentation12,13 or surgical stabilization. 14
With regard to bracing, Ohana et al examined a cohort of patients who suffered lumbar compression fractures and found no radiographic differences in patients who were treated with bracing vs no bracing with at least 12 months of follow-up. 15 Furthermore, Kim et al compared outcomes between patients who received no bracing, soft bracing, and rigid bracing and found no difference in Oswestry Disability Index scores, back pain, or progression of anterior body compression between the 3 groups after 12 weeks of follow-up. 16 Weitzman et al examined stable thoracolumbar fractures all treated without bracing with a 3.6-year follow-up. Weitzman et al found increased deformity in 10% of patients and no patients required further treatment. 17 A systematic review by Giele et al found that there was no evidence for the usefulness of bracing for thoracolumbar fractures. 18 Other studies have, also, shown that bracing does not improve pain and mobility in patients after compression fractures.16,19,20
However, Pfeifer et al examined a small cohort of 32 patients with 32 controls and found that wearing a brace for 6 months was associated with increased back extensor strength and abdominal flexor strength, and a decrease in the body sway, pain, and limitations of daily living. 21 Other studies have shown that bracing increases patient comfort, 22 and gait improvement, 23 and is associated with less muscle fatigue. 24 That being said, there is a gap in the literature regarding how often bracing is used in patients who suffer from a thoracic/lumbar compression fracture. There is a further gap in examining the variables associated with the use of bracing or not for geriatric compression fractures.
With different management options for VCF management, there is a paucity of literature evaluating the usage trends of bracing with the management of thoracic/lumbar compression fractures. The current study aimed to utilize a large, national, administrative dataset to examine and characterize the bracing/orthosis trends for thoracic/lumbar (fifth thoracic vertebra to the fifth lumbar vertebra [T5-L5]) compression fracture management.
Materials and Methods
Data Source/Study Population
The current study used the M157 PearlDiver database from 2015-2021. Based in the United States, PearlDiver is a large, national, administrative, and multi-insurance database; its use in similar studies has become well-established in orthopaedic/spine literature.25-29 The Yale University Institutional Review Board has exempted studies using PearlDiver from review and requiring informed consent because its data is output in aggregated and de-identified form.
Geriatric patients (age >65 years old) who suffered a T5-L5 compression fracture were identified using initial fracture visit International Classification of Disease (ICD) – 10th revision fracture codes. These included ICD-10-D-S22050A, ICD-10-D-S22060A, ICD-10-D-S22070A, ICD-10-D-S22080A, ICD-10-D-S32010A, ICD-10-D-S32020A, ICD-10-D-S32030A, ICD-10-D-S32040A, and ICD-10-D-S32050A. Exclusion criteria included an indication of infection or neoplasm within the 90-days before the compression fracture.
These levels were selected (T5-L5), as they are the levels likely to sustain thoracic/lumbar fracture and are most amenable to bracing. Like the current study, prior studies have also chosen to examine patient cohorts who suffered a compression fracture from T5-L5.30-33
Patient variables were abstracted including fracture level and patient age, sex, Elixhauser Comorbidity Index (ECI- a marker of overall comorbidity burden,34,35 and geographic regions (Northeast [NE], South [So], Midwest [MW], and West [WE]). The geographic regions are based on the definition by the U.S. Census Bureau. 36
Bracing Trends
Patient bracing was identified based on Current Procedural Terminology (CPT) codes. These included CPT-L0450, CPT-L0452, CPT-L0454, CPT-L0455, CPT-L0456, CPT-L0457, CPT-L0458, CPT-L0462, CPT-L0464, CPT-L0466, CPT-L0467, CPT-L0468, CPT-L0469, CPT-L0470, CPT-L0472, CPT-L0480, CPT-L0482, CPT-L0484, CPT-L0486, CPT-L0488, CPT-L0490, CPT-L0491, and CPT-L0492.
Patients who received a brace within 90-days after the initial diagnosis of thoracic/lumbar compression fracture were abstracted. The bracing vs non-bracing trends were characterized based on vertebral level with ICD-10 coding.
Data Analysis
To characterize the variables that are associated with bracing trends a univariable analysis. To examine the association with each variable independently a multivariable logistic regression was performed.
The PearlDiver Bellwether software was used for both the data collection and statistical analysis. The figures were created using Excel 16.74. Significance was defined as P < .05.
Results
Study Population
In total 290 388 patients who met the inclusion/exclusion criteria and suffered a compression fracture in the T5-L5 vertebrae were identified. Of these, 286 125 (98.5%) did not receive a brace within 90-days after diagnosis, and 4263 (1.5%) did receive a brace (Figure 1). This figure shows the breakdown of bracing trends from 2015 through 2021. In black is the group which received a brace and in grey is the group that did not receive a brace after compression fracture.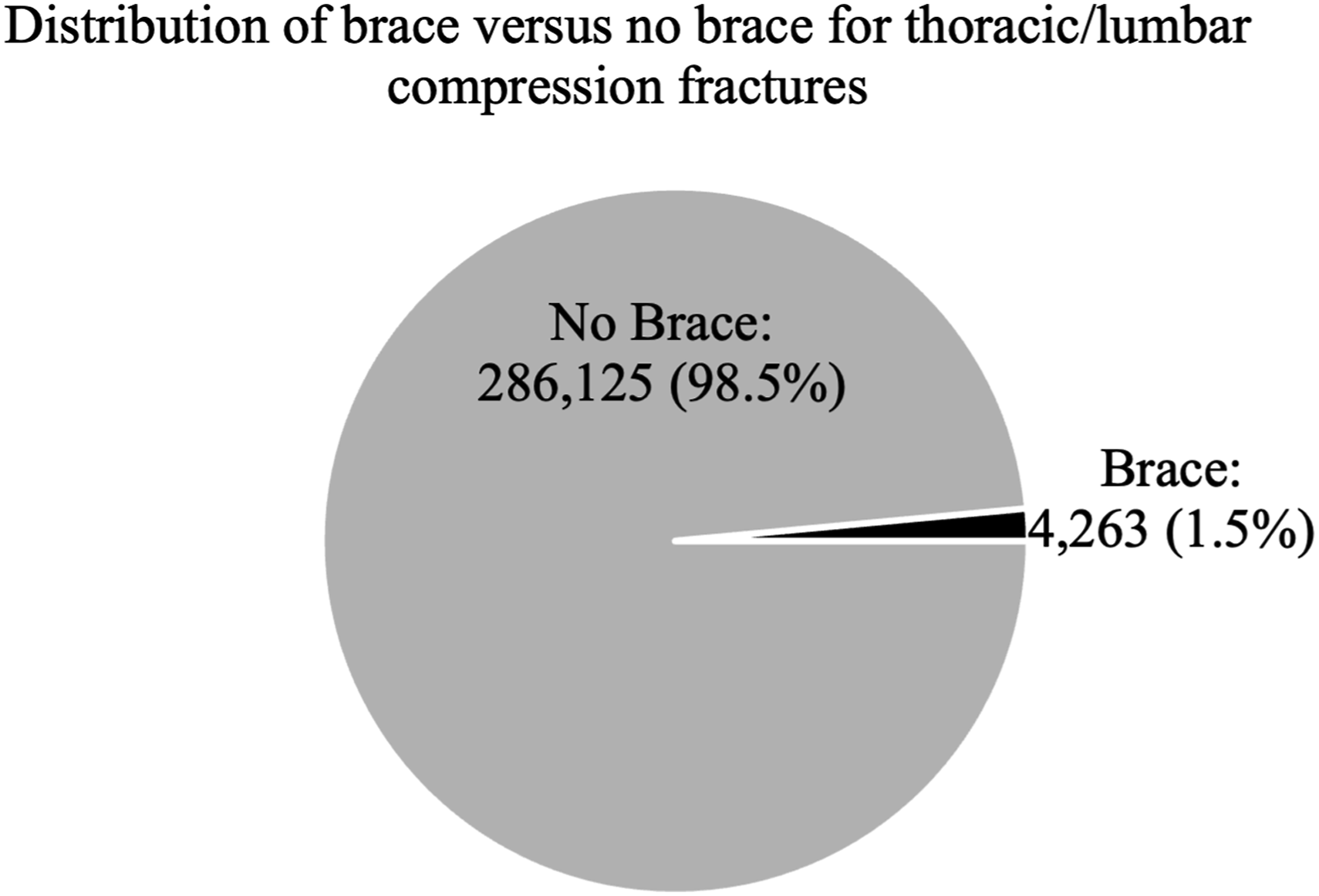
The fracture distribution of the study population is shown in Figure 2. The most common location of injury was at the thoracolumbar junction of T11/12-L1. This horizontal bar graph shows the frequency of compression fractures that occur at each level from T5-L5.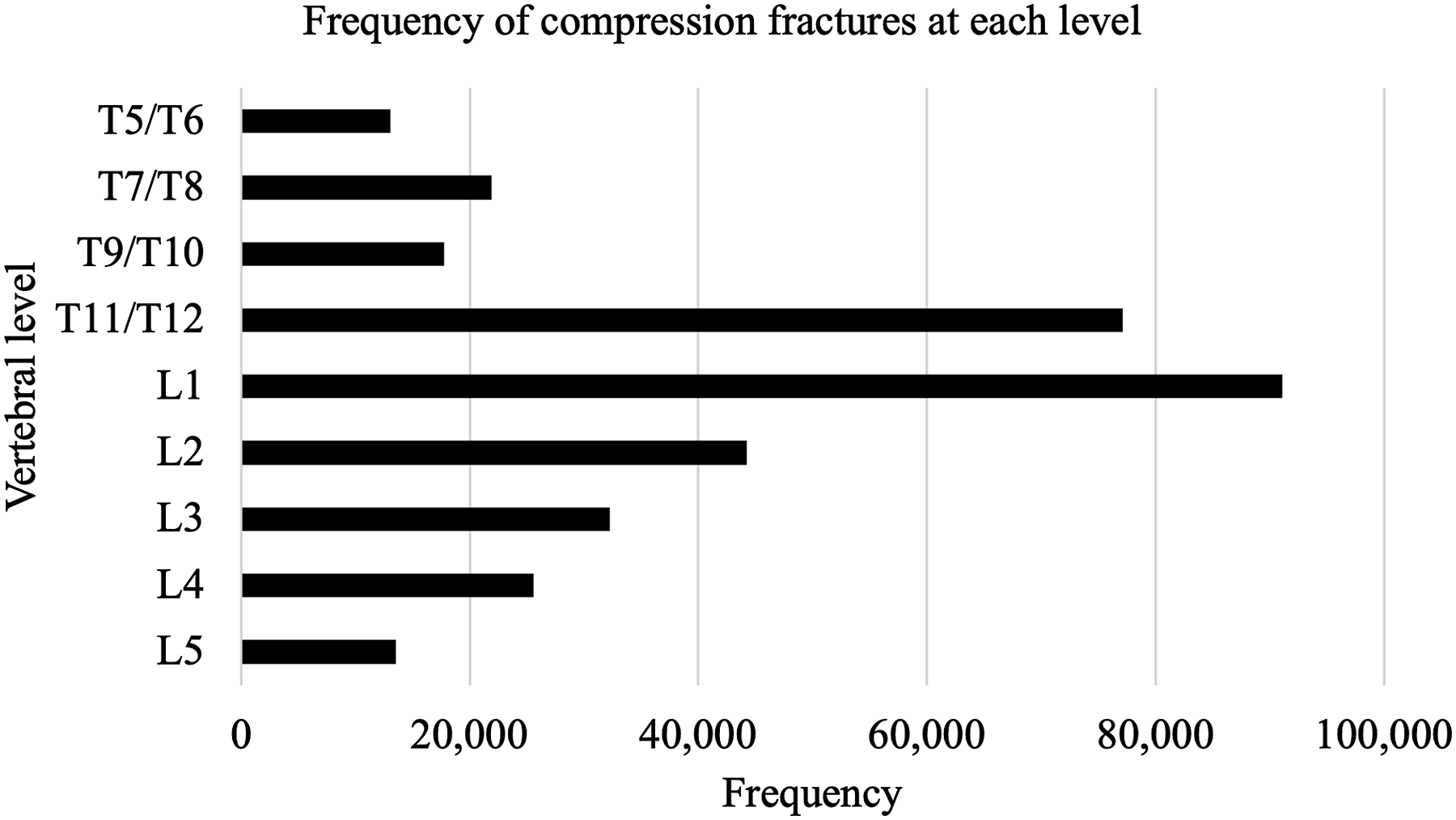
Bracing by Fracture Level
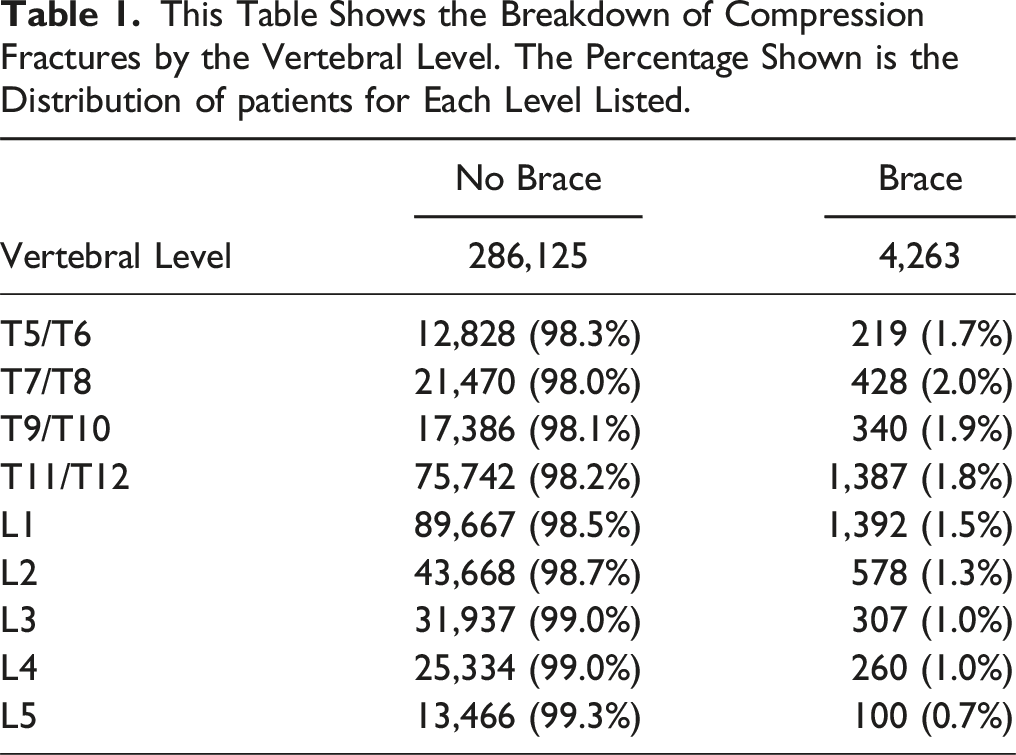
This Table Shows the Breakdown of Compression Fractures by the Vertebral Level. The Percentage Shown is the Distribution of patients for Each Level Listed.
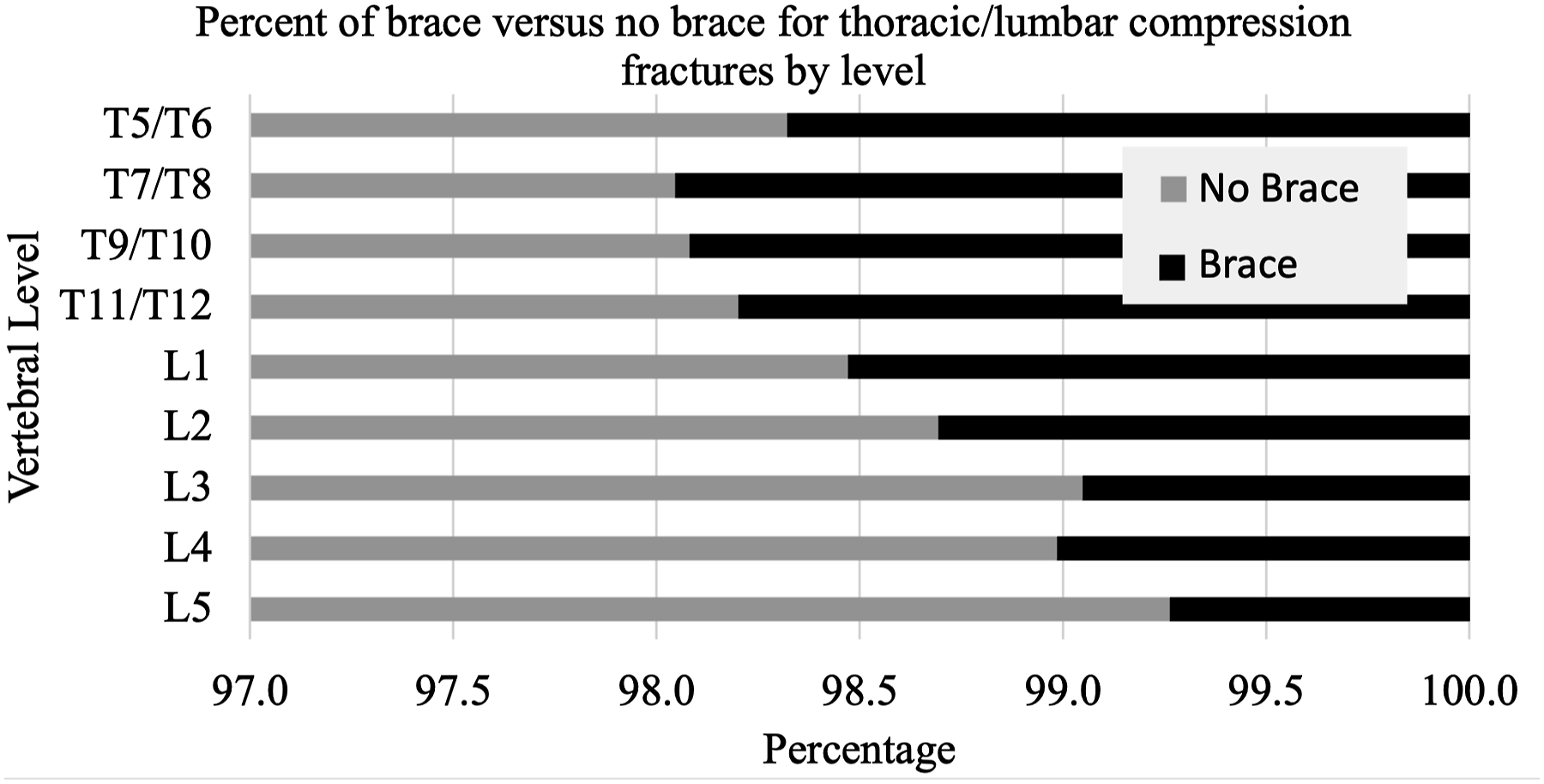
This stacked horizontal bar graph shows visually the percentage of brace (black) vs no brace (grey) by vertebral level from Table 1.
By levels, bracing was utilized for: T5/T6 (brace: 219 [1.7%]; no brace: 12 828 [98.3%]), T7/T8 (brace: 428 [2.0%]; no brace: 21 470 [98.0%]), T9/T10 (brace: 340 [1.9%]; no brace: 17 386 [98.1%]), T11/T12 (brace: 1387 [1.8%]; no brace: 75 742 [98.2%]), L1 (brace: 1392 [1.5%]; no brace: 89 667 [98.5%]), L2 (brace: 578 [1.3%]; no brace: 43 668 [98.7%]), L3 (brace: 307 [1.0%]; no brace: 31 937 [99.0%]), L4 (brace: 260 [1.0%]; no brace: 25 334 [99.0%]), and L5 (brace: 100 [.7%]; no brace: 13 466 [99.3%]).
Associations with Bracing
Univariable and Multivariable Logistic Regression Comparing Factors Associated With Receiving a Brace Versus Not Receiving One After Suffering a Compression Fracture.
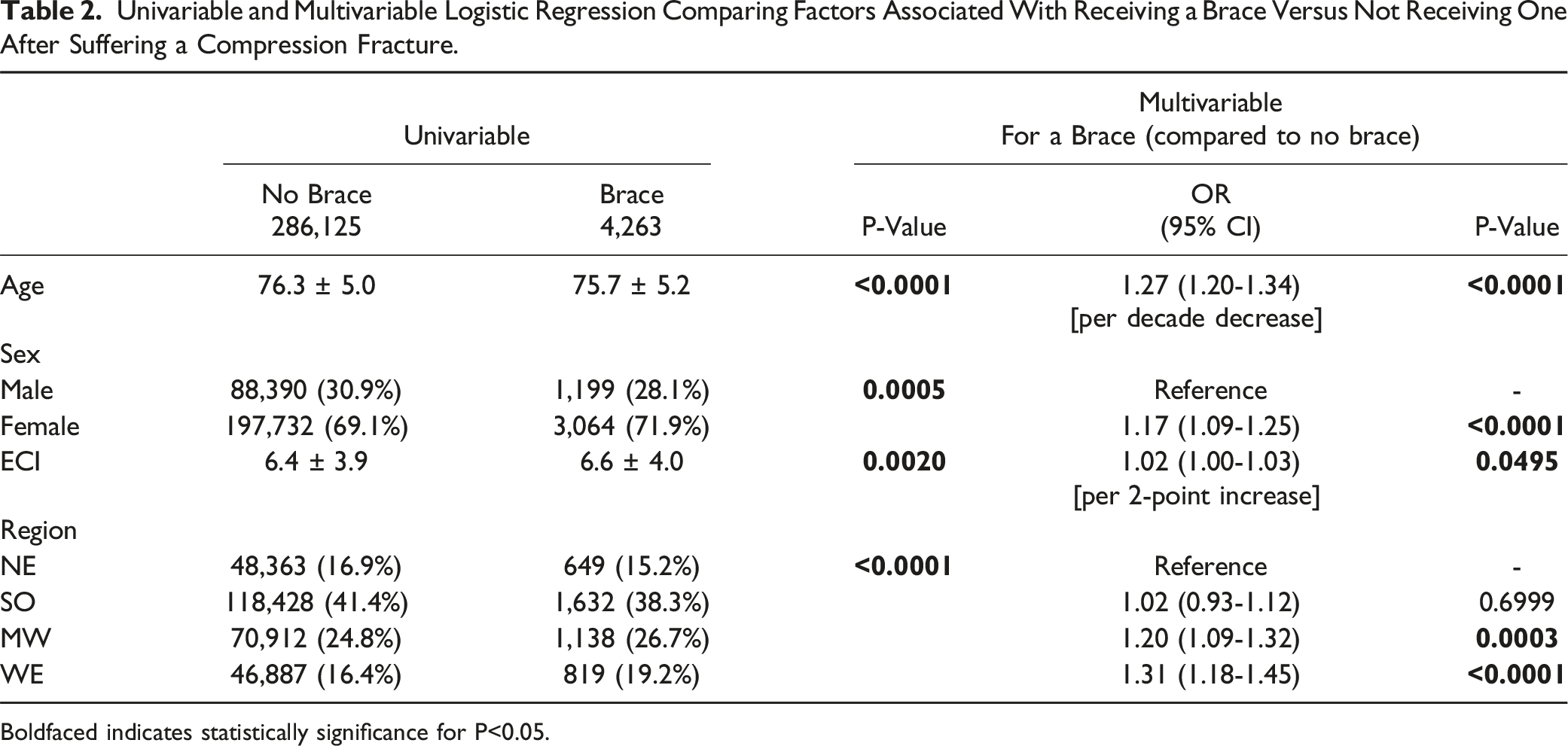
Boldfaced indicates statistically significance for P<0.05.
Multivariable logistic regression for patients who received a brace (compared to those who did not receive one) revealed the following statistically significant variables: WE region (Odds ratio [OR] 1.31 [P < .0001] relative to NE), age (OR 1.27 per decade decrease [P < .0001]), MW region (OR 1.20 [P = .0003], female sex (OR 1.17 relative to male sex [P < .0001]), and ECI (OR 1.02 per 2-point increase [P = .0495]).
Discussion
Geriatric vertebral compression fractures are the most common type of fracture associated with osteoporosis. While bracing may be considered, its use is variable and trends for utilization had not previously been characterized. The current study identified over a quarter million patients with such fractures and characterized the low percentage of patients who were braced.
In examining the distribution of thoracic/lumbar compression fractures by vertebral level, the current study found that over 60% of compression fractures occurred from Tl1-L2. This is consistent with prior literature which demonstrates osteoporotic compression fractures to be most likely at the thoracolumbar junction.37,38 The susceptibility of this area to fracture has been related to its transition from a rigid thoracic spine with associated ribs to a more flexible lumbar spine. 39
In terms of bracing, only 1.5% of the study population was braced for their thoracic/lumbar fracture. Further, this did not vary much by fracture level, and there was not more than a 1.5% variance in bracing by level. As reviewed in the introduction, the evidence for bracing is mixed, and it is of interest that such a low percentage were braced in the current cohort. The low bracing rate may be based on the significant literature finding no difference in patient outcomes with or without a brace after VCF.15-20 Further, there is currently no literature examining the rates of the utilization of bracing after suffering a compression fracture.
Several factors were found to be independently associated with the use of bracing for thoracic/lumbar fractures. One of these was that younger patients were more likely to be braced. This aligns with prior literature which has shown that younger patients tolerate bracing better than older patients. 7 Also female patients and those with higher ECI were slightly more likely to be braced; the reason for these associations was not clear.
Interestingly, the factor most associated with bracing was geographic region, where patients in the Midwest and West were more likely to receive a brace compared to patients in the Northeast. Geographic trends in bracing have not been previously examined; possible reasons for these differences include physician training location and patient preference. This highlights that non-clinical factors play a role in bracing trends suggesting a lack of clinical criteria for bracing.
There are limitations to the current study. As with other retrospective studies based on administrative data, it is limited based on study design and coding limitations. Also, fracture characteristics could not be specifically defined, or clinical factors and outcomes could not be assessed. Lastly, additional factors like osteoporosis treatments, treatment failures, orthoses compliance, and a measure of successful treatment were not able to be assessed.
Conclusion
Overall, the current study examined over a quarter of a million patients who suffered a T5-L5 compression fractures and found that only 1.5% of patients were braced. This low percentage, and the fact that the greatest predictor for bracing was non-clinical (geographic region), highlight the inconsistency of this practice and may be useful for developing treatment algorithms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Scott J Halperin (Jane Danowski Weiss Family Foundation Fund); Meera M Dhodapkar (Richard K. Gershon, M.D. Fund at Yale University School of Medicine, Associate Editor Visual Abstracts North American Spine Society Journal); Jonathan N Grauer (North American Spine Society Journal Editor-in-Chief).