
Abstract
Study Design
Reliability analysis.
Objectives
Vertebral pelvic angles (VPA) are gaining popularity given their ability to describe the shape of the spine. Understanding the reliability and minimal detectable change (MDC) is necessary to determine how these measurement tools should be used in the manual assessment of spine radiographs. Our aim is to assess intra- and interobserver intraclass correlation coefficients (ICC) and the MDC in the use of VPA for assessing alignment in adult spinal deformity (ASD).
Methods
Three independent examiners blindly measured T1, T4, T9, L1, and L4PA twice in ASD patients with a 4-week window after the initial measurements. Patients who had undergone hip or shoulder arthroplasty, fused or transitional vertebrae, or whose hip joints were not visible on radiographs were excluded. Power analysis calculated a minimum sample size of 19. Both intra- and interobserver ICC and MDC, which denotes the smallest detectable change in a true value with 95% confidence, were calculated.
Results
Out of the 193 patients, 39 were ultimately included in the study, and 390 measurements were performed by 3 raters. Intraobserver ICC values ranged from .90 to .99. The interobserver ICC was .97, .97, .96, .95, and .92, and the MDC was 5.3°, 5.1°, 4.8°, 4.9°, and 4.1° for T1, T4, T9, L1, and L4PA, respectively.
Conclusion
All VPAs showed excellent intra- and interobserver reliability, however, the MDC is relatively high compared to typical ranges for VPA values. Therefore, surgeons must be aware that substantial alignment changes may not be detected by a single VPA.
Introduction
Treatment decisions in the management of ASD must consider regional and global spinal malalignment in both the sagittal and coronal planes. 1 Various radiographic spinopelvic parameters have been proposed to assess malalignment severity in ASD patients, such as the sagittal vertical axis (SVA) and T1 spinopelvic inclination.2-6 These radiographic parameters are widely utilized in the treatment of ASD patients, as determining the precise focal target correction angle is critical to properly plan for ASD correction surgery. Nevertheless, the accuracy of measurement can still be influenced by different factors. For instance, positional compensation at the hip joint can impact SVA. 7 This occurs because even if the severity of the spinal deformity is identical, the SVA may change due to different amounts of compensation with a retroverted pelvis. On the other hand, the T1 pelvic angle (T1PA), which measures the angle between a line drawn from the center of the femoral head axis to the center of the T1 vertebral body and another line to the middle of the S1 endplate,8,9 is suggested as a more reliable global spinal alignment parameter for treatment planning and clinical outcomes in ASD.9-11 The T1PA can take into account positional compensation in the position of the pelvis,8,12,13 and unlike the SVA, it does not require calibration of radiographs. 7
Other VPAs have been proposed to describe spinal alignment.12,14,15 The VPA is defined as the angle formed between two lines drawn from the center of both femoral heads to the center of a vertebral body and to the superior S1 endplate (Figure 1).
12
Although measurements of the other VPAs have been used to evaluate clinical outcomes in ASD surgery, their reliability has been understudied compared to the T1PA.
12
This is of concern because, for example, the mean baseline L1PA in ASD patients was approximately half the mean T1PA (9.3° vs 18.8°), which may double the sensitivity to measurement error if both parameters have the same minimal detectable change (MDC).
12
On the other hand, VPAs may be more reliable than traditional spinopelvic angles measured using the Cobb angle technique, such as lumbar lordosis (LL) or thoracic kyphosis (TK), because VPAs do not require precise identification of the endplate, which is commonly challenging in preoperative ASD patients.
16
The aim of this study is to determine the intra- and interrater reliability and MDC of various VPAs measured from the T1, T4, T9, L1, and L4 vertebrae in ASD patients. As shown for the T1PA, we hypothesize that the T4PA, T9PA, L1PA, and L4PA angles are reliable measures of spinal alignment. Vertebral pelvic angle (VPA) defined as the angle formed between lines drawn from the center of the femoral head to the center of the T1, T4, T9, L1 and L4 vertebral bodies and to the midpoint of the superior S1 endplate.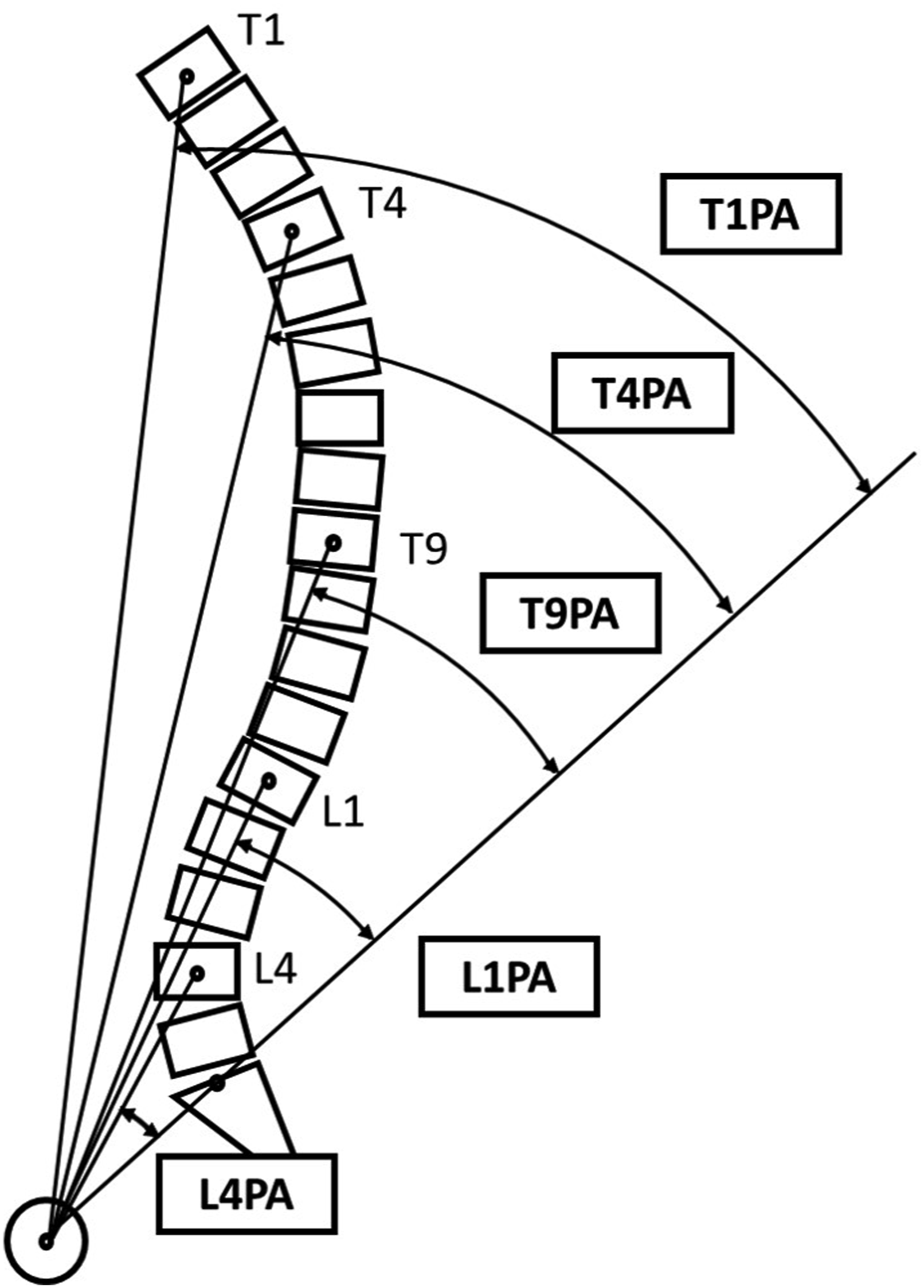
Methods
Patient Selection
Preoperative radiographs of ASD patients aged >18 years were retrospectively analyzed from the pooled dataset of ASD patients. Study approval was obtained from the institutional review board of our hospital (IRB number 2018-1142), and all patients provided written informed consent. ASD was confirmed by at least one of the following: coronal Cobb angle ≥20°, SVA ≥ 5 cm, pelvic tilt (PT) ≥ 25°, or thoracic kyphosis (TK) ≥ 60°, as previously reported.12,17 Only patients without a history of spinal fusion and with full spine lateral radiographs showing bilateral hip joints were included. Posteroanterior radiographs were used to assess coronal deformities and confirm transitional vertebrae. Patients with prior hip and/or shoulder arthroplasty, lumbosacral transitional vertebrae (ie, sacralization of L5 or lumbarization of S1) and/or vertebrae that were fused due to prior surgery or arthritis, including ankylosing spondylitis, were excluded. Patients with a body mass index (BMI) > 35 were excluded to avoid measurement interference from poor image quality due to thick fat tissue.
The Reliability Assessment of Measuring Different VPA
Three independent raters, including an attending orthopedic spine surgeon (OS) and two research engineers (RE1 and RE2) measured the T1PA, T4PA, T9PA, L1PA, and L4PA on every radiograph. All raters were trained in measuring VPAs in at least 20 cases and were trained in measuring traditional spinopelvic parameters in over 100 cases before data collection. To evaluate intraobserver reliability, each radiograph was remeasured after a 4-week interval while blinded to the previous results to minimize potential recall bias.
All radiographs were uploaded to the system and measured using a picture archiving and communication system (PACS) application, Sectra IDS7 version 24.1 (Sectra, Linköping, Sweden). The measurements were carried out on computers and monitors that are routinely used in clinical practice. The hip joints are marked with a circle on the software tool, and their centers are automatically identified by the software. The midpoint of the superior S1 endplate is also detected automatically by the software once the endplate is traced, as illustrated in Figure 2. Then, the VPA was measured by two lines drawn from the center of both femoral heads to the center of a vertebral body and to the midpoint of the superior S1 endplate. The hip joints are marked with a circle on the software tool and their centers are automatically identified on the PACS system. The center of the superior S1 endplate is also automatically detected by the software once the endplate is traced.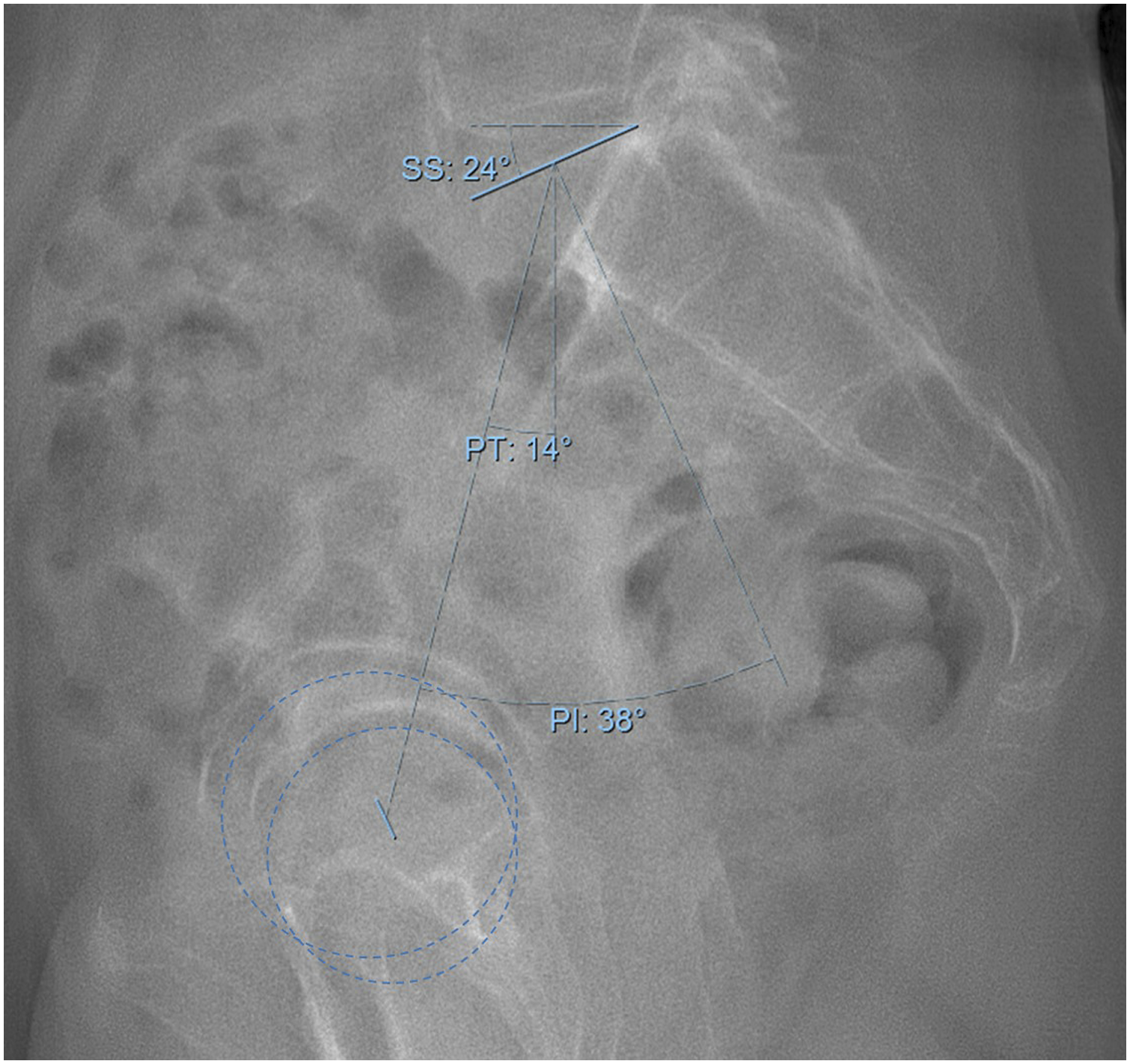
Statistical Analysis
The ground truth (GT) measurement was defined as the mean of two values measured by the OS, and the absolute difference between the GT and the values measured by the two REs was calculated. The intraclass correlation coefficient (ICC) was calculated to assess inter- and intraobserver reliability. The ICC refers to correlations within repeated measurements and is calculated by taking the ratio of the variance of interest to the total variance. ICC scores range from 0 to 1.0, with scores of 1.0 indicating perfect reliability between measurements. ICC values less than .5, between .5 and .75, between .75-.9, and greater than .90 are indicative of poor, moderate, good, and excellent reliability, respectively. 18 Assuming that the ICC for VPA measurements is similar to that of T1PA, we estimated the expected ICC for VPAs to be .95 based on a previous study of T1PA measurements. 7 Subsequently, the minimum sample size for the power analysis was 19 with an expected ICC of .95, a minimum acceptable ICC of .85, a significance level (P value) of .05, and a power (1-β) of 80%. 19 The standard error of measurement (SEM) and MDC were also calculated to describe the degree of measurement error for each VPA. The MDC represents the minimum amount of change that is considered to be true change with 95% confidence, meaning that differences within the MDC value are considered to be within the measurement error: MDC = 1.96 × √2 × SEM. 20 Analysis was performed using SAS version 9.4 (SAS, Inc., Cary, NC, USA).
Results
Demographics and Spinopelvic Parameters of the 39 Patients.
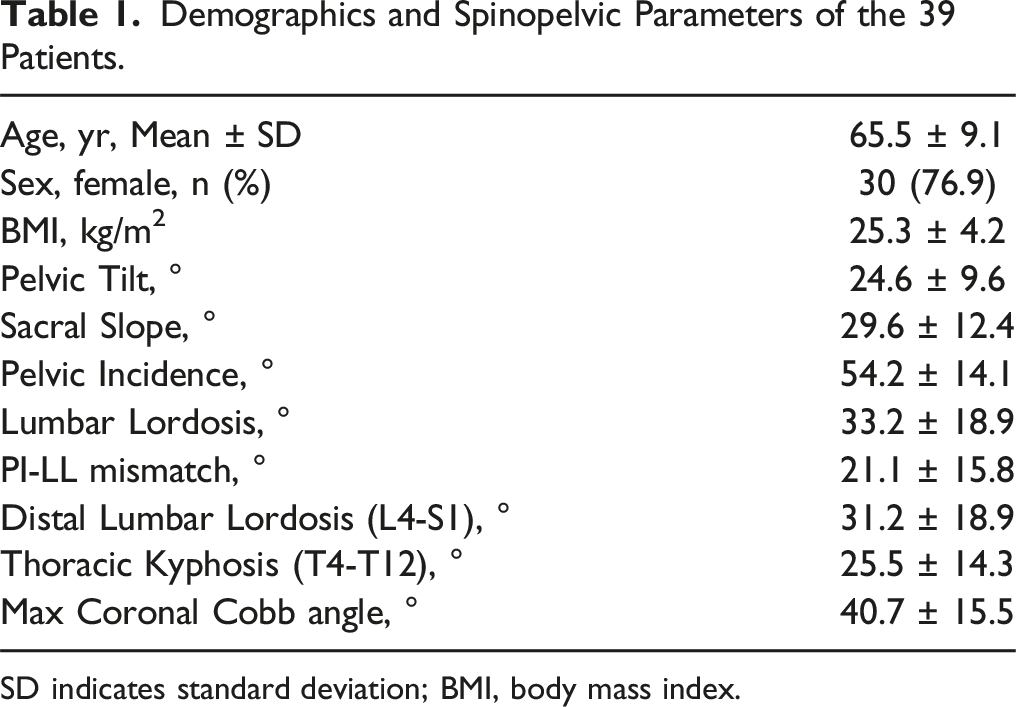
SD indicates standard deviation; BMI, body mass index.
Intra- and Interrater Reliability of VPA Measurements
The Absolute Error to GT for VPA.
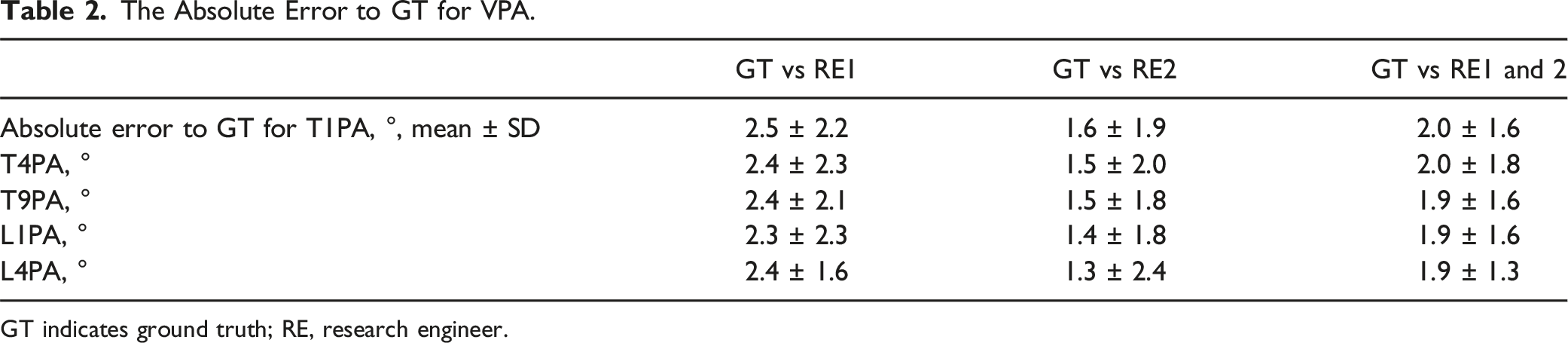
GT indicates ground truth; RE, research engineer.
Intrarater ICC for VPA Measurements.
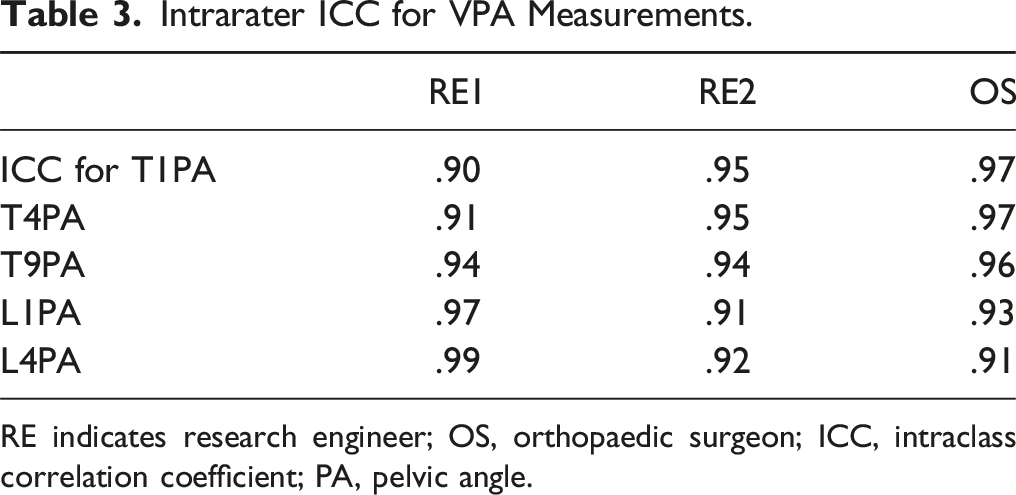
RE indicates research engineer; OS, orthopaedic surgeon; ICC, intraclass correlation coefficient; PA, pelvic angle.
Interrater ICC for VPA Measurements.
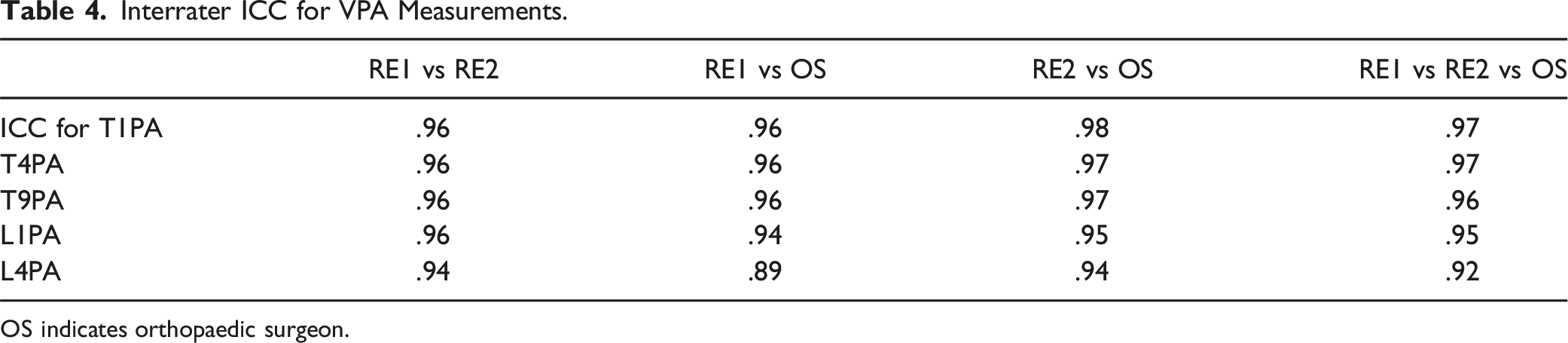
OS indicates orthopaedic surgeon.
MDC for VPA measurements
The mean values for each VPA in our patient cohort were 22.2 ± 10.6°, 18.9 ± 10.0°, 14.2 ± 9.2°, 10.4 ± 7.7°, 10.0 ± 5.3°, and the MDC were 5.3°, 5.1°, 4.8°. 4.9°, 4.1° for T1PA, T4PA. T9PA, L1PA, L4PA respectively. The T1PA exhibited the smallest MDC/mean ratio, suggesting greater robustness of measurement with respect to the impact of the smallest true change over measurement error relative to the mean value (Table 5).
Discussion
The MDC Value for Each VPA.
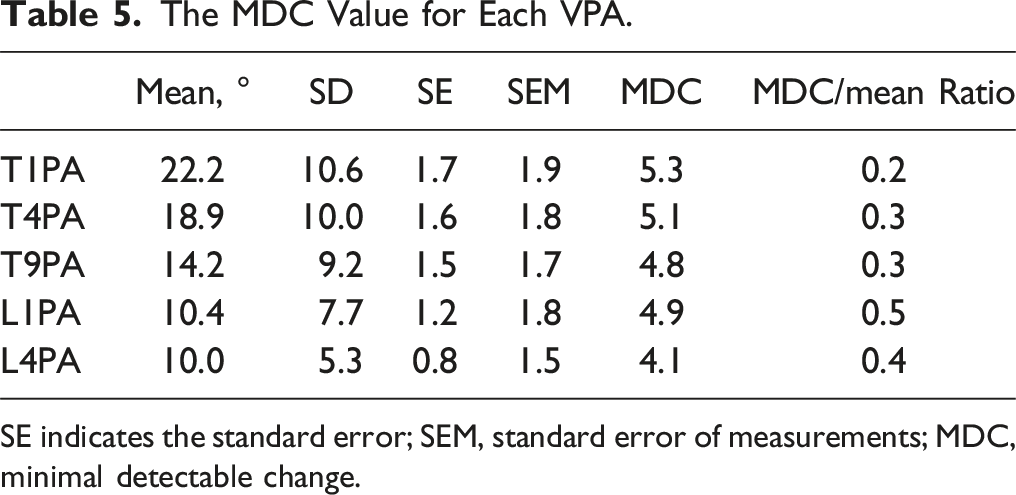
SE indicates the standard error; SEM, standard error of measurements; MDC, minimal detectable change.
Proper measurement of spinopelvic parameters in ASD patients is critical in directing deformity correction and defining the confines of realignment. To be effective measurements, VPAs must exhibit comparable or superior reliability to the traditional Cobb angle technique. Pruijs et al. conducted a study on Cobb angle reliability in 10 scoliosis patients, finding an MDC of 5° for the Cobb angle which closely aligns with our results with an MDC range of 4.1-5.3°. 21 Additionally, Briggs et al. reported on the reliability of the Cobb angle for thoracic spines with or without deformity, with an interrater ICC range of .83-.99 and an intrarater ICC range of .98-.99. 22 In terms of the reliability of traditional sagittal spinopelvic parameters, Vidal et al. conducted a study on the reliability of measuring LL in adolescent idiopathic scoliosis. 23 They found that the intrarater ICC ranged from .911 to .953, and the interrater ICC was .843. Lafage et al. conducted a study on measuring sagittal spinal alignment in ASD patients. The interrater ICC values for LL, TK, pelvic incidence (PI), and pelvic tilt (PT) were found to be .872, .900, .909, and .978, respectively. 24 The reliability of VPA measurement may be comparable to or possibly slightly better than that of LL or TK. This can be attributed to the inherent difficulty of identifying the endplates to measure those angles in patients with spinal deformity.
Reliability of T1PA, the most established VPA in the current literature, was validated by Plachta et al. 7 They assessed the reliability of the T1PA measurement in 7 examiners and 50 healthy adult volunteers in three pelvic rotational positions (neutral, anterior, posterior). The ICC for both intra- and interobserver agreements ranged from .83-.99. Moreover, the accuracy of each measure compared to their gold standard fell within a range of 2°. Though our measurements exhibited marginally better reliability, our results closely mirrored these reported results. Protopsaltis et al. also found comparable reliability in their five-observer T1PA measurements of 20 ASD patients with an intraobserver ICC of .936 and interobserver ICC of .965. 12 They also reported an intraobserver ICC of .906 and interobserver ICC of .961 for L1PA, which was consistent with our results. 12 In contrast, Vaynrub et al. found a much wider ICC range in their four-observer VPA measurements of 20 ASD patients using intraoperative radiographs. They found the ICC ranges for intraobserver agreement to be .31-.86, .43-.83, .49-.81, and .65-.81 and the ICC for interobserver agreement to be .68, .93, .84, and .84 for T1PA, T4PA, T9PA, and L1PA, respectively. 14 This discrepancy may have been due to the poor resolution of the intraoperative radiographs or lack of adequate prior VPA measurement training for two of their raters, which was valued and implemented in this study. Regarding L4PA, this study appears to be the first to report its reliability, which was found to be excellent in both intra- and interrater reliability.
The high reliability and robustness of VPAs demonstrated in this study can be attributed to several reasons. By relying on vertebral body centroid identification, the measurement allows for greater variation in the angle line while remaining accurate to the true value. As illustrated in Figure 3A, the angle line for T1 or L4 can fall between the dotted boundaries and still reliably obtain an accurate measurement compared to the GT. Furthermore, as the angle line travels proximally from the femoral head axis, a larger variation is acceptable due to the geometric nature of angles, which can be seen when comparing the T1 boundary lines to the L4 boundary lines. This fact may explain why L4PA had the lowest interrater reliability. Figure 3B and 3C also emphasize that clearly identifying vertebral endplates, which is needed for the Cobb angle, is unnecessary in VPAs, allowing again for acceptable variation in measurement while remaining accurate. This feature of VPAs is of great importance when it comes to ASD patients whose vertebral endplates may not be clearly visible or defined due to scoliosis, advanced kyphosis, or severe spondylosis. (A) A description of how the distance between the target vertebral body and the center of the hip joint affects the area where the measurement error ±2° (dotted line) from the ground truth (GT, black line) can be obtained. The acceptable range for the T1 vertebral body is larger than that for the L4 vertebral body. (B) The magnified image of Figure 2A focused at the level of the T1 vertebral body. (C) Compared to the acceptable range of ±2° measurement error for the line used for T1PA, the acceptable range of ±2° measurement error for the line along the superior endplate used for the Cobb angle technique of the T1 vertebral body is narrow.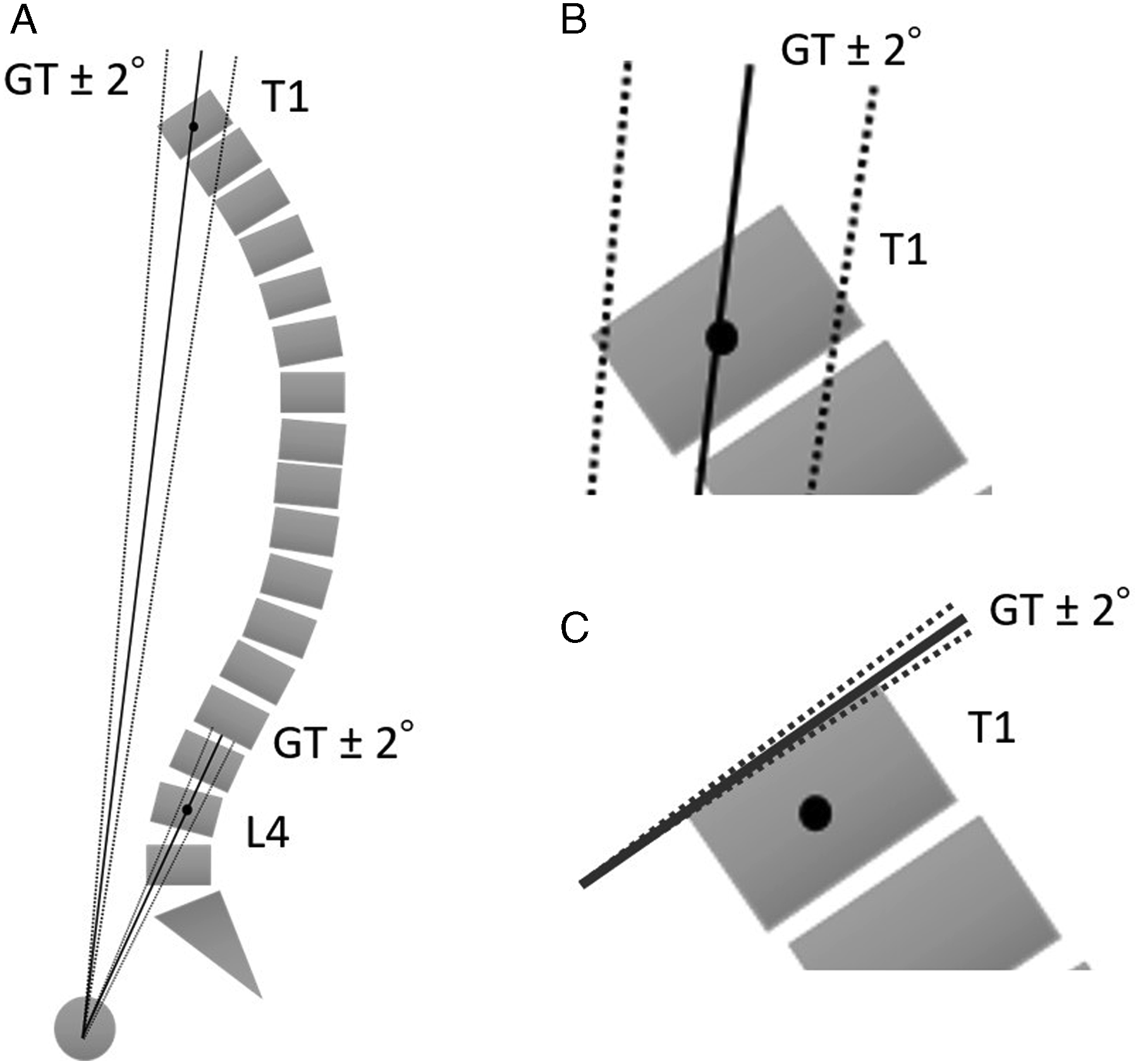
We found that the typical MDC for VPAs is approximately 5 degrees. The average pelvic incidence is approximately 51 ± 10° according to the most recent literature. 25 Per Hills et al, the formula for an “ideal” L1PA is PI × .5 - 20°. 26 Therefore, the range of ideal L1PA in an asymptomatic population is approximately 0-10°. Considering that we found 5 degrees as the approximate MDC for L1PA, this poses a potential clinical problem when using L1PA to determine intraoperative or postoperative corrections. Substantial clinical changes in alignment (eg, changing the lumbar alignment in a patient with a PI of 40° from 5 to 0°) may not be detectable using a single VPA alone. Therefore, we recommend that surgeons assess changes in alignment using more than just a single VPA. Using Cobb angles or adding other VPAs (ie, L4PA or a UIV-PA) may help avoid over- or under-estimating corrections due to measurement error.
Limitations to this study do exist. First, utilization of the measurement tool available on the PACS software, which automatically determines the center between the bilateral hip joints, may lead to better measurement reliability than without the use of the software tool. Second, the examiners included in the study were trained to measure VPA, including the measurement of other spinopelvic parameters prior to the actual measurement. Thus, it may be not appropriate to generalize the findings to non-trained examiners. However, these values were obtained by training the REs in only 20 cases for VPA measurement, suggesting that the learning curve would not be a major issue for surgeons. Third, the strict selection criteria of the radiographs allowed for proper vertebral visualization, but not all measurements of ASD patients will be without joint arthroplasty and prior spinal surgical history. Future studies should investigate the influence of these artifacts on the reliability of VPA measurements.
Conclusion
All VPA measurements performed by trained examiners showed excellent intra- and interobserver reliability in ASD patients. This study is the first to provide a pragmatic MDC for VPA, which was calculated to be approximately 5° for all VPA. This study suggests that the VPA appears to be at least as reliably measured as the traditional spinopelvic alignment. Additionally, VPA can be theoretically more reliable than Cobb angles, especially in cases where the endplate is challenging to identify. Thoracic VPAs may be more stable than lumbar VPAs theoretically due to the greater distance of the target vertebral body from the hip joints.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: No direct funding was received for this study. However, the study used REDCap (Research Electronic Data Capture) hosted at Weill Cornell Medicine Clinical and Translational Science Center supported by the National Center For Advancing Translational Science of the National Institute of Health (NIH) under award number: UL1 TR002384.
HSS Approved IRB Number
2018-1142