
Abstract
Study Design
Retrospective Cohort Study.
Objectives
Although the optimal timing of surgical intervention for traumatic spinal cord injury (TSCI) is controversial, early intervention has been recognized as being beneficial in several studies. The objective of this study was to evaluate the socioeconomic factors that may delay time to surgical fixation in the management of TSCI.
Methods
The present study utilized the Trauma Quality Improvement Program (TQIP) dataset to identify patients aged greater than 18 undergoing spinal fusion for TSCI from 2007-2016. Patients were divided into subgroups based on race and insurance types. Multivariable linear regression was used to compare time to procedure based on race and payer type while adjusting for demographic and injury-specific factors. Significance was set at P < .05.
Results
Using multivariable analysis, Hispanic and Black patients were associated with significantly increased time to fixation of 12.1 h (95% CI 5.5-18.7, P < .001), and 20.1 h (95% CI 12.1-28.1, P < .001), respectively compared to White patients. Other cohorts based on racial status did not have significantly different times to fixation (P > .05). Medicaid was associated with an increased time to fixation compared to private insurance (11.6 h, 95% CI 3.9-19.2, P = .003).
Conclusions
Black and Hispanic race and Medicaid were associated with statistically significant increases in time to fixation following TSCI, potentially compromising quality of patient care and resulting in poorer outcomes. More research is needed to elucidate this relationship and ensure equitable care is being delivered.
Introduction
High income North America has the highest standardized incidence and prevalence of traumatic spinal cord injuries (TSCIs). 1 Traumatic spinal cord injuries are often debilitating as they historically result in poor functional outcomes for patients. 2 The management of TSCI requires prompt evaluation and may necessitate urgent intervention to preserve neurologic function. Thus, time to procedure is critical to reduce spinal cord ischemia and optimize post-surgical outcomes. 3
Socioeconomic disparity refers to the unequal distribution of economic resources, opportunities, and access to essential services among different individuals or groups within a society. This disparity is often measured in terms of income, education, employment opportunities, and overall social and economic well-being. Socioeconomic disparity within medicine exacerbates health inequalities by limiting access to quality healthcare for individuals with lower socioeconomic status (SES). This disparity often results in unequal distribution of resources, leading to disparities in health outcomes and exacerbating existing societal inequalities. Because of the urgency and often time-sensitive nature of managing traumatic injuries, it is essential to have a complete understanding of the barriers to receiving appropriate care. Several studies have incompletely identified differences in hospital wait times, treatment plans, and patient outcomes based on SES and race.4-7 Srikumaran et al revealed that Black patients had a longer time to surgery following hip fracture as compared to similarly matched White patients. 8 Moreover, another study found that, in patients undergoing anterior cervical discectomy and fusion (ACDF), Black and Hispanic race, low household income, and Medicare insurance were all associated with extended length of stay following surgery. 4 Specifically, in patients hospitalized for traumatic cervical spinal cord injury, one study found that low SES and Black race were associated with fewer discharges home and higher rates of in-hospital mortality.5,6
Although these studies suggest a difference in management for patients based on socioeconomic factors, there is currently a lack of research looking at potential biases in time to spinal fixation following TSCI. The present study utilized a national trauma database to assess time to spinal fixation based on insurance status and race for patients undergoing surgical fixation of TSCI. We hypothesized that White patients and private insurance will be associated with the shortest time to fixation in surgical management of TSCI.
Methods
Data Source
The present study utilized the Trauma Quality Improvement Program (TQIP) dataset to collect patient records from 2007-2016. This dataset incudes patients across the United States pooled from 875 participating trauma centers. Patients aged 18 and older undergoing spinal fusion for TSCI were included. Patients designated as polytrauma were excluded from the analysis. Patients were divided into subgroups based on race, consisting of White, Black, other, and unknown. The “Other” category consisted of Asian, Native Hawaiian/Pacific Islander, American Indian, and patients who identified as “other.” In addition, patients were grouped into a cohort based on whether or not ethnicity was recorded as Hispanic. If race/ethnicity was not listed, the patient was placed in the unknown category. Furthermore, patients were categorized by payer type into 8 groups: Private/Commercial, Medicare, Medicaid, Government/military, Workers Comp/Automotive, Self-Pay, Unknown and Not Billed.
Informed Consent and IRB Approval
The information in the TQIP database does not contain any personal identifiers. Therefore, this study is deemed exempt from informed consent and IRB approval by the Johns Hopkins Medicine Human Research Protection Program.
Outcomes
Demographics (n = 8773).
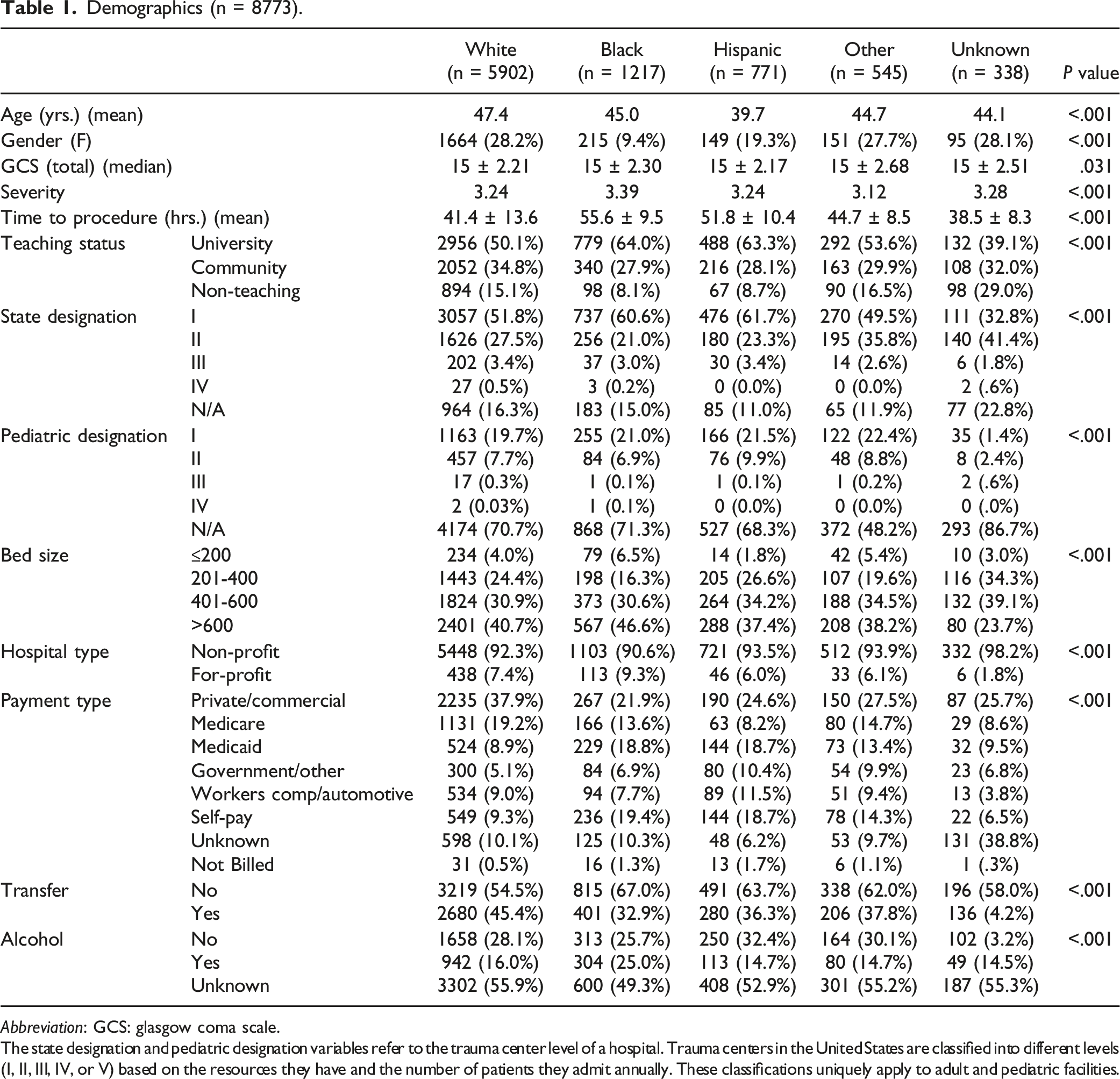
Abbreviation: GCS: glasgow coma scale.
The state designation and pediatric designation variables refer to the trauma center level of a hospital. Trauma centers in the United States are classified into different levels (I, II, III, IV, or V) based on the resources they have and the number of patients they admit annually. These classifications uniquely apply to adult and pediatric facilities.
Statistical Analysis
ANOVA and Pearson’s Chi-Square χ2 testing were used to determine if there was a difference in continuous and categorical demographics, respectively, among primary race groups. Univariate and multivariable linear regression analysis were used to compare time to procedure based on patient primary race and payer type while adjusting for patient demographics, hospital teaching and profit status, levels involved, region of the spine fixed, severity of TSCI, and emergency room disposition. Significance was set at P < .05. All statistical testing was performed on SPSS (IBM Corp. Released 2020. IBM SPSS Statistics for Macintosh, Version 27.0. Armonk, NY: IBM Corp).
Results
Demographics
Demographics.
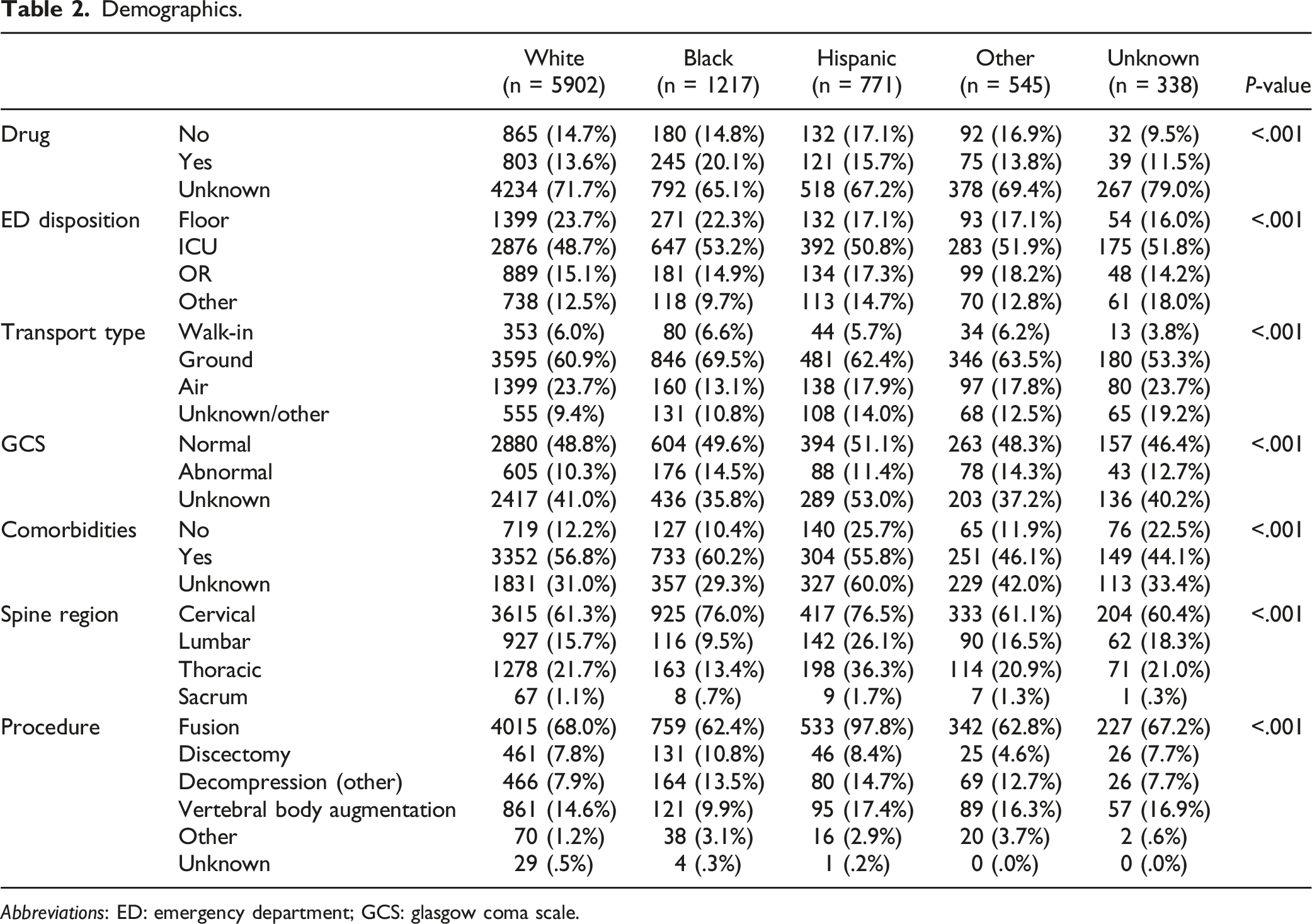
Abbreviations: ED: emergency department; GCS: glasgow coma scale.
Time to Fixation by Race
Time to Procedure (Hours): Adjusted Linear Regression Analysis.
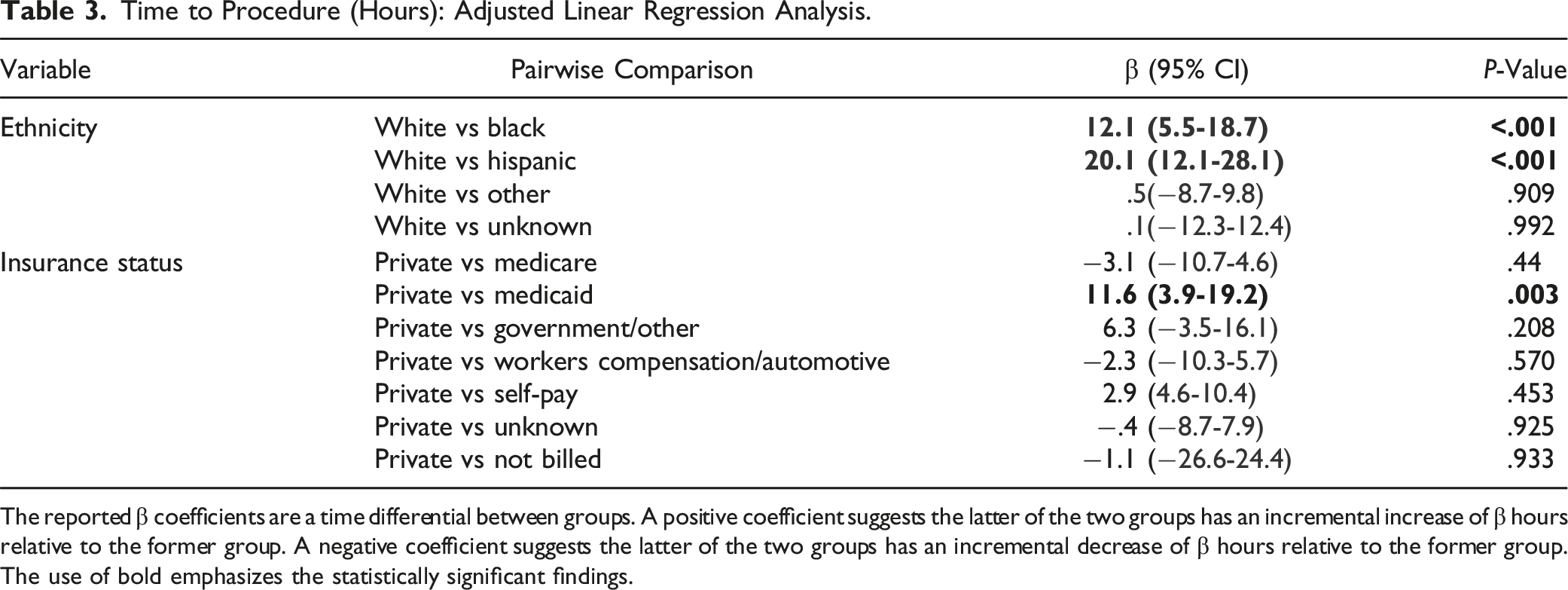
The reported β coefficients are a time differential between groups. A positive coefficient suggests the latter of the two groups has an incremental increase of β hours relative to the former group. A negative coefficient suggests the latter of the two groups has an incremental decrease of β hours relative to the former group.
The use of bold emphasizes the statistically significant findings.
Time to Fixation by Insurance
Univariate analysis showed that Medicare, Medicaid, government and military-based insurances, and self-pay were all associated with significant increases in time to fixation compared to private insurance (P < .05). However, following multivariable analysis, only Medicaid was associated with a statistically significant increased time to fixation when compared with private insurance (11.6 h, 95% CI 3.9-19.2, P = .003). Workers’ compensation was not associated with a significantly significant time to fixation compared to privately insured patients in either univariate or multivariable analysis (P > .05) (Table 3).
Discussion
It is well-recognized that differences in patient outcomes exist based on SES and race.4-7 The present study aims to assess whether implicit bias in terms of race and insurance affects time to spinal fixation in the management of TSCI. The results, presented as beta coefficients, offer valuable insights into the association between different demographic groups and the time required for spinal fixation. When compared to White patients, both Black and Hispanic individuals exhibited statistically significant increases in time to fixation. Specifically, Black patients were associated with a substantial increase of 12.1 h (95% CI 5.5-18.7, P < .001), while Hispanic patients faced an even greater delay, with an increase of 20.1 h (95% CI 12.1-28.1, P < .001). These beta coefficients provide a quantitative measure of the time differential, emphasizing the considerable impact of race on the timeliness of surgical intervention for TSCI. The study found that patients with Medicaid were associated with a significant increase of 11.6 h compared to those with private insurance. These findings underscore critical issues in healthcare access and highlight potential barriers that certain demographic groups encounter in receiving prompt and equitable care for TSCI. Our results suggest healthcare outcomes due to SES and race stem from healthcare delivery--timely fixation of traumatic injuries being one of many examples.
In other studies of racial disparities, Black and Native American patients had greater 30-day postoperative complications following spine surgery compared to Caucasian (White) patients. 9 In a study of patients with hip fractures undergoing surgery at Johns Hopkins regional hospitals, Black patients had the longest median time to surgery, followed by Asian patients, White patients, and patients of other races. 8 Similar results have been found in studies of breast cancer patients and lung cancer patients receiving surgical treatment,10,11 but there is a gap in the literature within the field of spine surgery.
The results of the present study suggest that, compared to White patients, both Black race and Hispanic ethnicity are associated with significantly longer times to procedure for spinal fixation following TSCI. The delay in time to surgery for certain racial groups could contribute to disparities in postoperative outcomes, as earlier surgery following TSCI has been associated with greater improvements in motor function postoperatively. 12 However, the optimal timing of surgery following TCSI is controversial and is dependent on many factors including pattern of injury, co-morbid injuries, and need to stabilize patients in critical condition. For these reasons, it is difficult to determine the true causes of the delayed time to fixation seen among Black and Hispanic patients. One potential explanation is that non-White patients have higher rates of comorbidities that may be preclude emergent surgery before the patient can be stabilized.13-17 Another possibility includes the location or site at which these patients initially present to, which, if in an area lacking sufficient resources, may necessitate a transfer to a better equipped center, further delaying fixation. As the present study was primarily focused on analyzing time to surgery, further research is needed to evaluate the exact causes of delayed surgery and the effects on postoperative outcomes in Black and Hispanic patients.
This study also demonstrated a significantly longer time to procedure for patients with Medicaid compared to patients with private health insurance. No significant differences in time to surgery were observed for patients with Medicare, government/other insurance, worker’s compensation/automotive, or self-pay compared to patients with private health insurance. Previous studies have shown a similar relationship between Medicaid and adverse postoperative outcomes. In a study of patients undergoing surgical fixation for lumbar spinal stenosis, patients with Medicaid had greater health care resource utilization after their index procedure as measured by initial length of stay and complication rates. They also had higher rates of ED visits, readmissions, and medication prescription in the immediate postoperative period. 18 In the same study, privately insured patients had significantly higher rates of reoperation at one and two years-potentially indicating that patients with Medicaid were going without beneficial procedures in the long-term (although patient-specific radiographic and clinical data was not available in this particular study to verify this hypothesis). Differences in time to surgery and healthcare utilization can be seen outside of spine surgery, as well. In a study of patients undergoing bariatric surgery, both Medicaid and Medicare patients had significantly longer times to surgery compared to privately insured patients. 19 These authors hypothesized that this was a result of increased insurance-related requirements and a lengthy approval process before surgery, and the need for greater patient education, both of which may have prolonged the interval from initial consultation to procedure. This hypothesis is less relevant to the current paper due to the emergent nature of fixation for TSCI and lack of initial insurance approval. However, there is other evidence that may suggest a system-level bias towards patients of a particular insurance status. Unlike morbidity and mortality, which can be influenced by underlying psychosocial factors and medical comorbidities, insurance status should, theoretically, play a minimal role in healthcare utilization in an emergent setting such as traumatic injury. Despite this, a study released by the Institute of Medicine found that uninsured patients with traumatic injuries were less likely to be admitted to a hospital, more likely to receive fewer services once admitted, and more likely to die when compared with insured trauma victims. 20 Another study found that, following traumatic injury, publicly insured patients had longer risk-adjusted length of stay than privately insured patients, possibly reflecting difficulty in arranging a safe discharge. 21 Such results support the hypothesis that publicly insured or uninsured patients face system-level biases when being managed for emergent traumatic injury.
Another important factor to consider in interpretation of these results is the role of implicit bias among healthcare providers. Implicit bias has been recognized as having a negative influence on patient provider relationships in several studies.22-25 Hoffman et al conducted two studies in which White adults with and without medical training were surveyed on their beliefs surrounding false biological differences between Black and White patients and their associated treatment recommendation for pain management. 25 50% of participants with medical training (students and residents) endorsed at least one false belief. They also found a positive relationship between endorsement of false beliefs and inaccuracy of management recommendations, implying that the maintenance of false beliefs about a patient based on race can directly lead to improper management. Although the results of the current study can neither support nor refute an influential role of implicit bias, it is nevertheless an important potential factor to consider.
This study provides valuable information regarding disparities in access to care, specifically time to spinal fixation surgery following TSCI. A patient’s race or insurance status is significantly associated with delays in care following TSCI that, potentially, could have significant negative impacts on their perioperative and postoperative outcomes. Identifying and further understanding the discrepancies and inequity in healthcare is paramount to provide equal access and quality care for all.
Strengths and Limitations
Because of the TQIP database’s large size and inclusion of 875 centers across a geographically diverse area, the results have a high degree of generalizability to the US population. Nevertheless, the present study has several limitations that should be considered when interpreting its findings. First, due to the limitations of the database, the study did not capture all possible disparities that could be affecting access to care. The data was acquired and selected from the TQIP database, and there is always the potential for coding errors in the creation of the original database or in the selection of the relevant aspects of the database for this study. The database does not include a hospital identifier to determine the proportion of different races served at a hospital. Therefore, it was not possible to determine if different outcomes were a result of hospital historically serving higher proportions of minorities compared to those who are lower serving. In addition, variables such as severity of initial injury, surgical technique, and intraoperative factors were not available and could not be taken into account. Finally, only patients who underwent spinal fixation surgery were included in the analysis, and therefore selection bias is inherent. While acknowledging the presence of these limitations, this study provides useful insight into the effect of demographic factors on timeliness in the administration of surgical intervention for patients with a TSCI.
Conclusions
Black and Hispanic race and Medicaid were associated with statistically significant increases in time to fixation following TSCI, potentially compromising quality of patient care and resulting in poorer outcomes. More research is needed to elucidate this relationship and ensure equitable care is being delivered.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Hamid Hassanzadeh is a paid consultant, paid presenter or speaker, and has stock/stock options for Nuvasive. Dr Hamid Hassanzadeh is a paid presenter/speaker and receives research support from Orthofix, Inc.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.