
Abstract
Study Design:
Retrospective cohort study.
Objective:
The influence that race has on mortality rates in patients with spinal cord tumors is relatively unknown. The aim of this study was to investigate the influence of race on the outcomes of patients with primary malignant or nonmalignant tumors of the spinal cord or spinal meninges.
Methods:
The Surveillance, Epidemiology, and End Results (SEER) Registry was used to identify all patients with a code for primary malignant or nonmalignant tumor of the spinal cord (C72.0) or spinal meninges (C70.1) from 1973 through 2016. Racial groups (African-American/Black vs. White) were balanced using propensity-score (PS) matching using a non-parsimonious 1:1 nearest neighbor matching algorithm. Overall survival (OS) estimates were obtained using the Kaplan-Meier method and compared across non-PS-matched and PS-matched groups using log-rank tests. Associations of survival with clinical variables was assessed using doubly robust Cox proportional-hazards (CPH) regression analysis.
Results:
There were a total of 7,498 patients identified with 648 (6.8%) being African American. African-American patients with primary intradural spine tumors were more likely to die of all causes than were White patients in both the non-PS-matched [HR: 1.26, 95% CI: (1.04, 1.51), P = 0.01] and PS-matched cohorts [HR: 1.64, 95% CI: (1.28, 2.11), P < 0.0001]. On multivariate CPH regression analysis age at diagnosis [HR: 1.03, 95% CI: (1.02, 1.05), P < 0.0001], race [HR: 1.82, 95% CI: (1.22, 2.74), P = 0.004), and receipt of RT [HR: 2.62, 95% CI: (1.56, 4.37), P = 0.0002) were all significantly associated with all-cause mortality, when controlling for other demographic, tumor, and treatment variables.
Conclusions:
Our study provides population-based estimates of the prognosis for patients with primary malignant or nonmalignant tumors of the spinal cord or spinal meninges and suggests that race may impact all-cause mortality.
Introduction
While there have been significant strides toward improving access to specialty care across racial and socioeconomic groups, inconsistencies in equitable surgical outcomes are still evident among various specialties.1-7 Specifically in spine surgery, African American race has been associated with inferior outcomes with disproportionately increased complications and 30-day readmission rates,8,9 longer hospital stays, 10 and greater healthcare costs. 11 Analogously, increased mortality rates following spine surgery is no exception. In a retrospective, 10-year analysis using the Nationwide Inpatient Sample (NIS) of 803 949 adult patients undergoing lumbar spine surgery, Poorman et al demonstrated that Black race was significantly associated with increased mortality rates with an odds-ratio (OR) of 1.40. 12 Therefore, a better understanding of how racial disparities impact mortality rates within spinal surgery is necessary for improving overall quality of patient care and bridge the disparities gap.
In spine oncology, primary spine tumors comprise of less than 10% of central nervous system (CNS) tumors, with most common primary intradural spine tumors are schwannoma, meningioma, and glioma.13-16 Despite improved overall survival in recent periods, the 5-year mortality rate for these tumors remains eminent with reported rates up to 40.3%. 17 Previous studies have identified various factors affecting mortality such as age at diagnosis, 18 tumor grade, 19 and extent of surgical resection. 20 However, there continues to be varying evidence on the impact that race has on mortality within different intradural pathologies. In a population-based cohort study of 346 patients with primary intramedullary spinal cord lymphoma (PISCL), Yang et al demonstrated that White race was a significant independent predictor of tumor-related survival (OR: 1.69). 18 Whereas in an analysis of 1,721 patients with primary spinal cord astrocytoma (SCA) or ependymoma (SCE) captured by Surveillance, Epidemiology, and End Results (SEER), Milano et al found that race was not a significant independent predictor of survival. 19 The varying results underscores the need for further investigation of comparative disparities in mortality outcomes within the primary intradural spine tumor population.
The aim of this study was to investigate whether race is an independent predictor of all-cause mortality for patients diagnosed with a malignant or nonmalignant tumor of the spinal cord or spinal meninges.
Methods
Data Source and Patient Population
We used the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) Program database, a nationwide registry covering approximately 34.6% of the United States population between 1975 and 2016. 21 We queried the SEER 18 registry, with chemotherapy and radiation therapy data included, for cases including information on patient demographics, tumor histology, treatment, and mortality. This registry captures patients from 18 regions across the United States including the Alaskan Native Tumor Registry, Connecticut, Detroit, the Georgia Center for Cancer Statistics, the Greater Bay Area Cancer Registry, Greater California, Hawaii, Iowa, Kentucky, Los Angeles, Louisiana, New Mexico, New Jersey, Seattle-Puget Sound, and Utah. Follow-up for patients in the SEER Program is tracked monthly and an 80% follow-up rate is maintained for all analytical patients from the SEER cancer registry reference date.
Tumor histology was recorded using the World Health Organization (WHO) International Classification of Diseases for Oncology (ICD-O) 3 rd Edition. We performed a retrospective analysis of patients diagnosed with primary tumors of the spinal cord (C72.0) or spinal meninges (C70.1) available in the SEER registry described above. Cauda equina (C72.1) was not included given the high risk of cauda equina syndrome which confounds the urgency and treatment approach which may confound the analysis. Institutional Review Board was deemed exempted due to the deidentification of patients in the SEER database.
Data Collection
Patient demographic, tumor, and treatment information was collected for each patient case listing queried. Demographic information included age for patients 18 years and older, sex (male or female), and race (white or African American). Patients with a race not listed as white or African American were excluded from analysis (e.g., other). Tumor characteristics included tumor behavior (benign, borderline, or malignant) and tumor size, which was defined as the greatest dimension of the tumor measured in millimeters from 1 to 986 mm. The most common histologic types of neoplasms were summarized by racial category. Procedural information was organized by receipt of a surgical procedure, chemotherapy, or radiation therapy. Surgical procedure was dichotomized into resection and no resection categories, where resection was further categorized as gross total resection or partial resection, and No Resection was further categorized as diagnostic procedure (e.g., excisional biopsy), no surgical procedure, or missing/unknown procedure. Chemotherapy was dichotomized as either received or not received. Radiation therapy was dichotomized as received or not received and further categorized by modality (e.g., beam radiation alone) and chronicity (radiation after surgery or radiation prior to surgery).
Univariate Analysis
Categorical variables were described using counts and percentages. Continuous variables were summarized using means and standard deviations (SD), if normally distributed, and median with interquartile range [IQR], if skewed. D’Agostino and Pearson’s test for normality was performed on normalized continuous variables to determine whether a variable was normally distributed. 22 Comparison between the groups was conducted by χ2 tests for categorical variables and 2-sided independent t-tests for continuous normally distributed variables or Mann-Whitney rank tests for continuous skewed variables.
Propensity Score Matching
Unbalanced cohorts with a nonrandom distribution of patients between the cohorts was accounted for by using propensity score (PS) matching. We created a non-parsimonious logistic regression model to derive propensity scores using age, sex, behavior, and therapy, including receipt of resection or radiation. Histologic type was not included in the PS-matching, due to the large number of categories with low counts (n < 5), that may have introduced instability or overfitting into the model. Tumor size and receipt of chemotherapy were also not included in the PS model due to sparsity. The matching algorithm used for this study was 1:1 nearest neighbor greedy matching algorithm without replacement, in which African American patients were matched to unique White patients. The optimal caliper width was determined by calculating 0.2 of the standard deviation of the logit of the propensity scores of all patients, as described elsewhere. 23 The adequacy of the model was validated by comparing the standardized mean difference of propensity scores between the pre- and post-matched data sets. After PS-matching, all variables were compared again using univariate hypothesis test between the African American and PS-matched White cohorts to determine whether the PS-matching algorithm yielded balanced comparison groups.
Survival Analysis
We constructed Kaplan-Meier (KM) survival curves for the 2 race cohorts (White and African American) both before and after PS-matching. The KM curves were compared by calculating median survivals, hazard ratios (HRs) with 95% confidence intervals (95% CIs), and P-values using log-rank (Mantel-Cox) tests. We then constructed a doubly robust multivariate ordinal Cox Proportional Hazards (CPH) regression on All-Cause Mortality, using a combined cohort including African American patients and PS-matched White patients. This CPH model was adjusted for age at diagnosis, sex, behavior category, treatment, and tumor size. The model yielded HRs, 95% CIs, and P-values. The concordance probability was calculated for the final CPH model to measure its discriminative capacity.
All values with n < 10 were withheld from tables and analysis to preserve patient anonymity. A P-value of less than α = 0.05 was determined to be statistically significant for all univariate tests described above. The final doubly robust multivariate CPH model was adjusted for multiple comparisons using the Bonferroni correction procedure, where the adjusted P-value threshold was adjusted to α/N = 0.05/9 ≈ 0.0056 where N is the number of comparisons. Data queries were performed using SEER*Stat, version 8.3.5. 21 Statistical analysis was performed using Python, version 3.8.0 and Prism, version 8.21.
PS matching yielded 648 well-matched White and African American pairs (1,296 patients); the remaining 6,202 White patients were discarded from the analysis. The mean standard differences of propensity scores before and after matching were 0.348 and 2.90 × 10−6, respectively. The optimized caliper width used for the matching algorithm was 0.07. The demographic, tumor, and treatment variables were all balanced after PS-matching, with P > 0.05 for all univariate comparisons, Tables 1 and 2.
Patient Demographics and Tumor Characteristics.
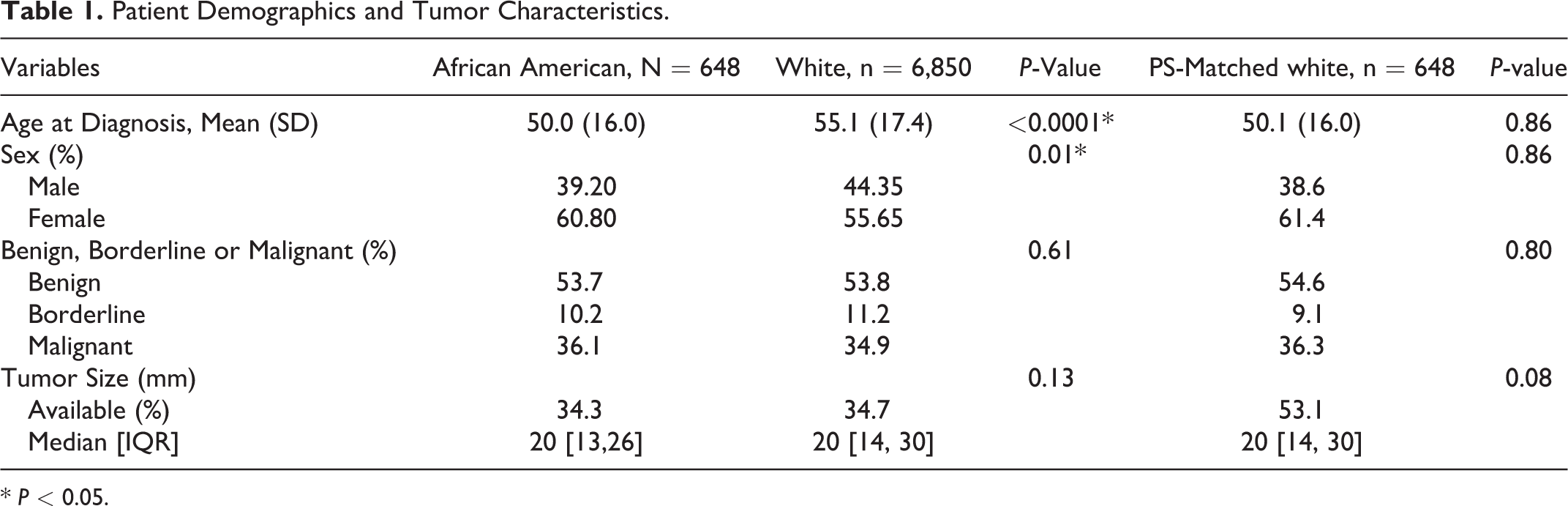
* P < 0.05.
Surgery, Chemotherapy, and RT for Primary Intradural Spine Tumors.
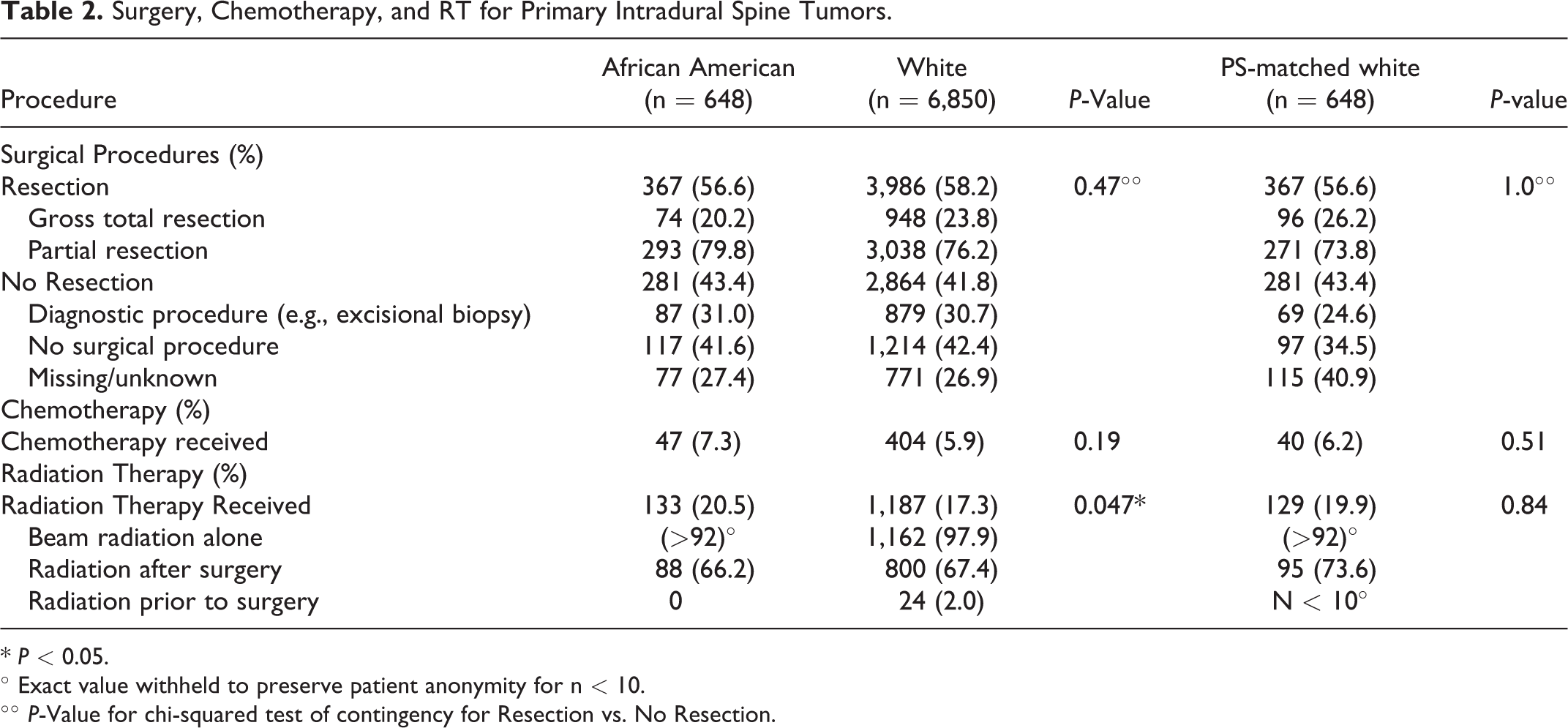
* P < 0.05.
° Exact value withheld to preserve patient anonymity for n < 10.
°° P-Value for chi-squared test of contingency for Resection vs. No Resection.
Results
Patient Demographics and Tumor Characteristics
There were 7,498 patients identified with a malignant or nonmalignant tumor of the spinal cord or spinal meninges, of which 648 (8.6%) were African American and 6,850 (91.4%) were White, Table 1. The African American cohort tended to be younger (African American: 50.0 ± 16.0 years vs. White 55.1 ± 17.4 years, P < 0.0001), Table 1. Both cohorts were comprised of a majority of benign tumors (African American: 53.7% benign vs. White: 53.8% benign, P = 0.61), with approximately one-third of the tumors in each cohort being malignant (African American: 36.1% malignant vs. White: 34.9% malignant, P = 0.61), Table 1. The most common histologic types were similar between the African-American and White cohorts, Figure 1. The 7 most common histologic types comprised 76.2% and 80.9% of all tumors in the White and African-American cohorts, respectively. The 3 most prevalent tumor histological types between White and African-American cohorts were meningiomas (26.4% vs 30.1%), nerve sheath tumors (16.0% vs 18.4%), ependymomas and anaplastic ependymomas (16.1% vs 13.2%), Figure 1.
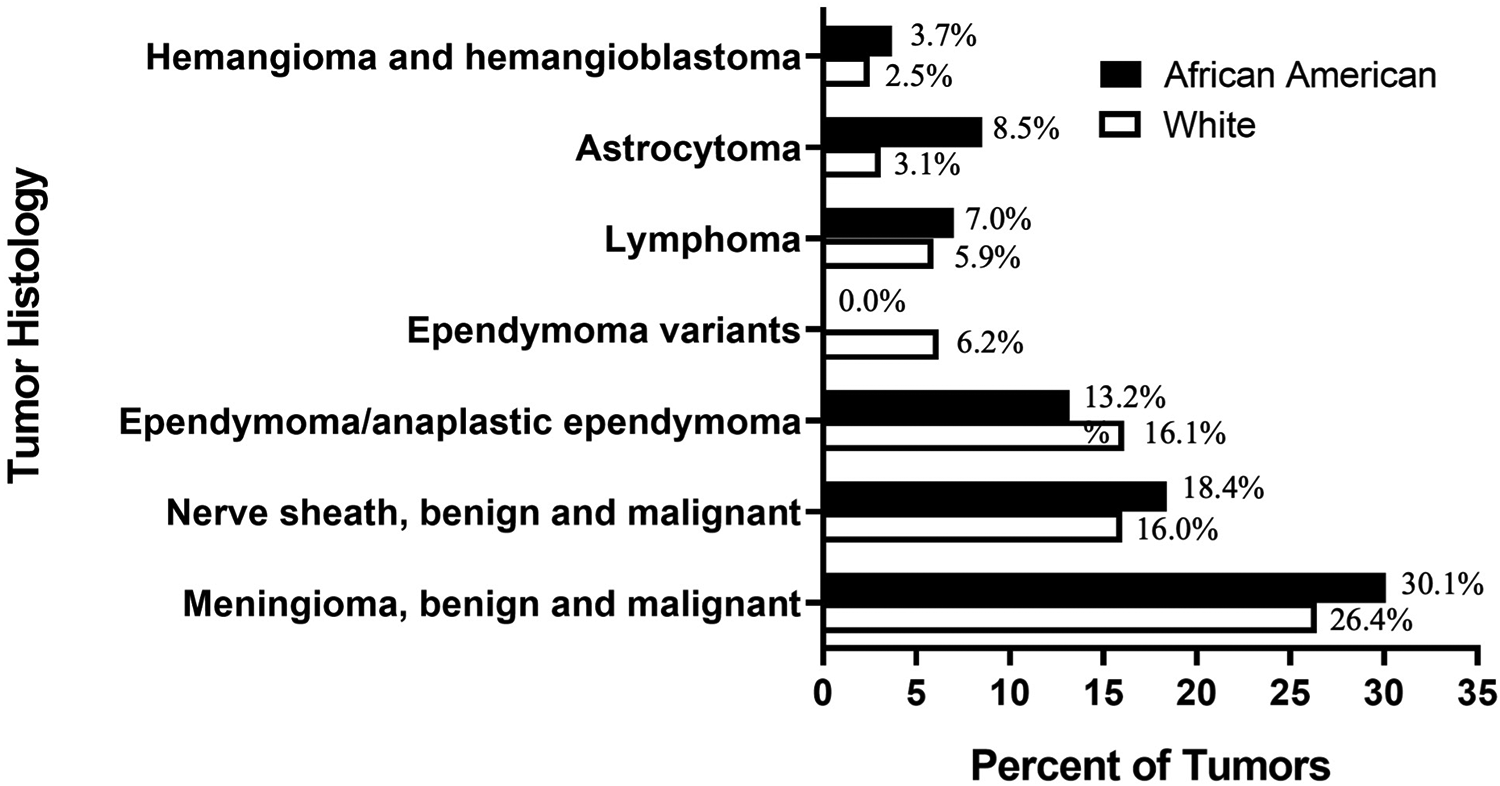
Most prevalent histology categories of spinal neoplasms by race.
Treatment Characteristics
The relative proportion of patients who received gross total or partial resection was similar between cohorts (African American: 56.6% resection vs. White: 58.2% resection, P = 0.47), Table 2. Of the patients who received resection, a majority in each cohort received partial resection, rather than gross total resection (African American: 79.8% partial resection vs. White: 76.2% partial resection, P = 0.47), Table 2. African American patients had a slightly greater proportion of patients who underwent radiation therapy (RT) than were White patients (African American: 20.5% RT vs. White: 17.3% RT, P = 0.047), Table 2.
Survival Analysis
African American patients survived a median of 71 months (5.9 years) shorter than White patients (African American: 218 months vs. White: 289 months) [HR 1.26, 95% CI: (1.04, 1.51), P = 0.01], Figure 2A. After PS matching on race, white patients survived a median of 76 months (6.3 years) longer than African American patients (African American: 224 months vs. PS-matched White: 300 months) [HR 1.64, 95% CI: (1.28, 2.11), P < 0.0001], Figure 2B. Patients who received RT survived a median of 221 months (18.4 years) shorter than patients who did not receive RT (RT: 350 months vs. No RT: 129 months) [HR: 2.78, 95% CI: (2.43, 3.18), P < 0.0001], Figure 2C. After PS matching on race, patients who received RT survived a median of 245 months (20.4 years) shorter than patients who did not receive RT (RT: 372 months vs. No RT: 127 months) [HR: 3.15, 95% CI: (2.36, 4.19), P < 0.0001), Figure 2D.
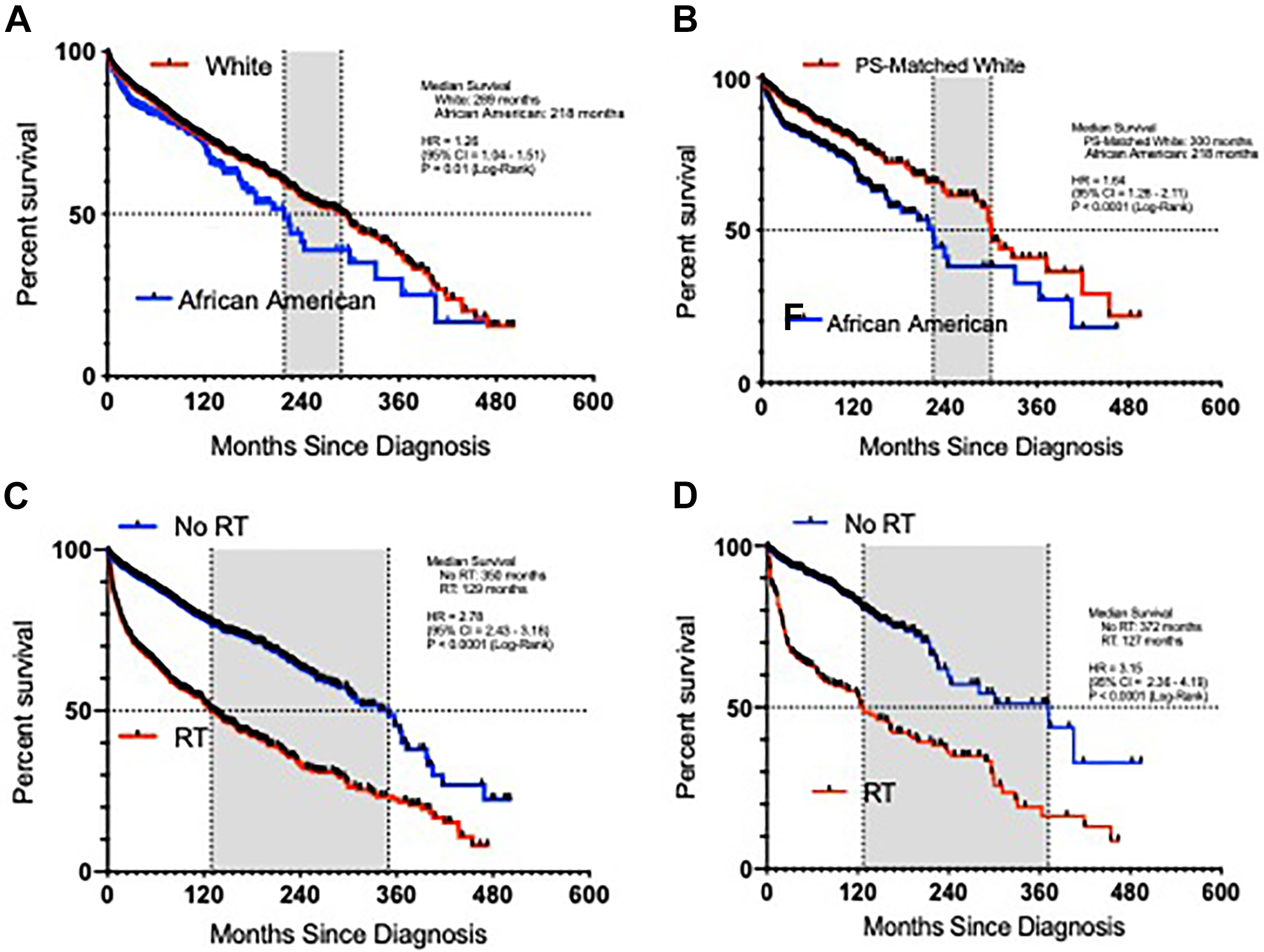
Kaplan-Meier survival curve for all-cause mortality. A, White patients versus African American patients. B, Propensity score (PS)-matched white patients versus African American patients. C, No radiation therapy (RT) versus RT. D, No RT versus RT in the composite African American with PS-matched white cohort.
Cox Proportional Hazards Regression Survival Analysis
The concordance probability of the doubly robust CPH regression model on all-cause mortality on PS-matched cohorts was 0.77, indicating good discrimination of the global CPH model. 24 In this model, 3 covariates met the threshold of significance: age at diagnosis, African American race, and receipt of RT, Table 3 and Figure 3. Controlling for other factors, patients who were older were significantly more likely to die from all causes than were younger patients [HR: 1.03, 95% CI: (1.03, 1.05), P < 0.0001], Table 3 and Figure 3. Likewise, patients who were of African American race were more likely to die of all causes than were patients of white race [HR: 1.82, 95% CI: (1.22, 2.74), P = 0.004], Table 3 and Figure 3. Patients who received RT were also more likely to die of all causes than were patients who did not receive RT [HR: 2.62, 95% CI: (1.56, 4.37), P = 0.0002], Table 3 and Figure 3.
Doubly Robust Cox Proportional-Hazards Regression Survival Analysis for All-Cause Mortality on Propensity Score-Matched Cohorts of Patients With Primary Intradural Spine tumors.*
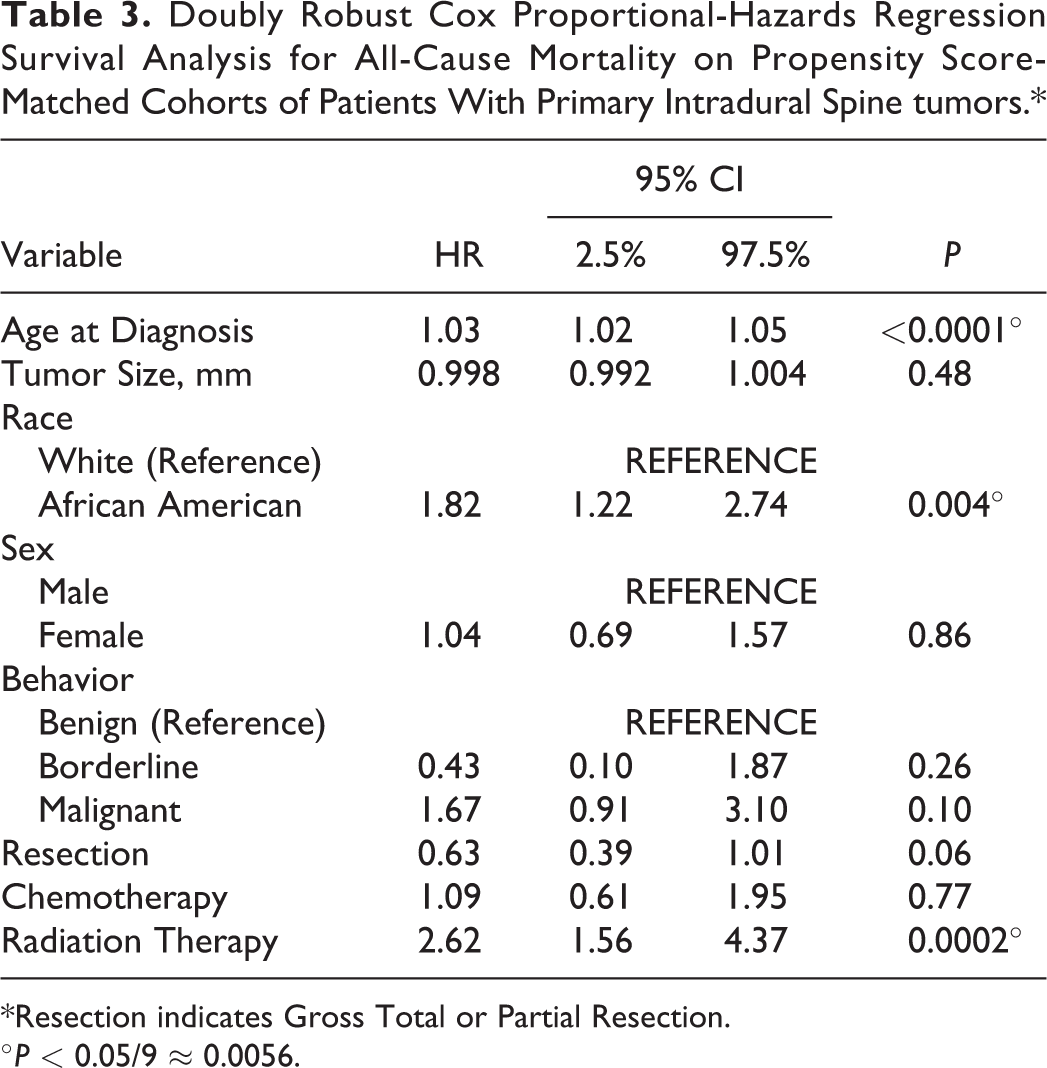
*Resection indicates Gross Total or Partial Resection.
°P < 0.05/9 ≈ 0.0056.
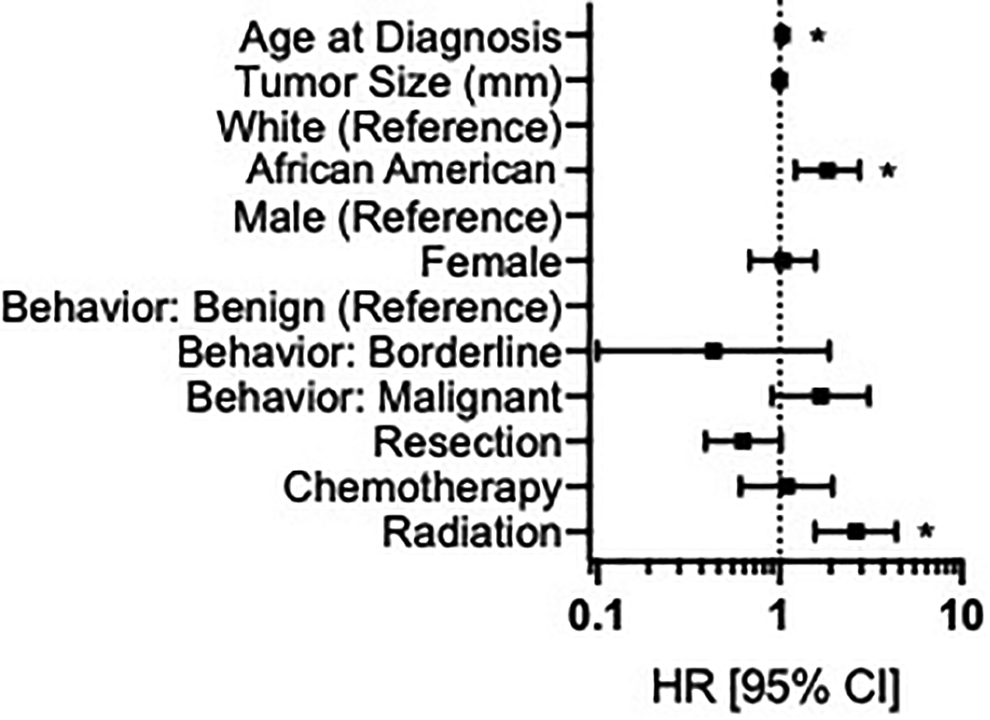
Forest plot representing results of doubly robust Cox proportional hazards regression on all-cause mortality for propensity score-matched cohorts. *P < 0.05/9 ≈ 0.0056.
Discussion
In this retrospective, PS-matched cohort analysis of 7,498 patients with a primary malignant or nonmalignant tumor of the spinal cord or spinal meninges, we demonstrate race is an independent risk factor for mortality, with African American patients experiencing nearly a 2-fold HR for mortality compared to White patients.
Previous studies have demonstrated that African American patients may have lower incidence rates of primary spinal cord tumors compared to White patients. In a retrospective cohort study of 3,226 patients diagnosed with a primary spine cord tumor, Schellinger et al demonstrated that White patients (incidence rate of 0.79/100 000 person-years) were at significantly higher risk of developing tumors than African American patients (incidence rate of 0.45./100 000 patient years), with the most common pathology being meningiomas. 13 Similarly, in a retrospective study utilizing the Central Brain Tumor Registry (CBTR) of 6,989 patients diagnosed with primary spinal schwannoma, Tish et al found that the incidence rate was approximately twice as high for White patients than for African American patients, with an incidence rate roughly twice as high. 25 Further studies are necessary better characterize the differential incidence rate as well as identify underlying genetic predispositions among different racial groups for the occurrence of a primary spinal cord tumors.
Within the literature, there has been varying evidence on racial differences in tumor characteristics of patients with primary spinal cord tumors. In the Duong et al NPCR and SEER study, the authors found that after adjusting for age that malignant rates were significantly higher in Whites than other racial groups. 26 However, in a retrospective cohort study utilizing the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) of 991 patients with intradural extramedullary spinal cord tumors, Bhimani et al demonstrated that race was not found to be associated with the proportion of malignant tumors. 24 Similarly, in a retrospective cohort utilizing the National Cancer Database (NCDB) of 287 patients with WHO grade II or III spinal meningioma, Wright et al showed that African American and White patients had similar tumor grades upon diagnosis. 27 Analogous to the aforementioned studies, our study did not find significant differences the tumor characteristics before or after propensity matching. Further studies are indicated to determine whether tumor characteristics differ between racial cohorts in order to better risk-stratify patients and treatment plans.
Along with tumor characteristics, there have been efforts to identify similar racial differences in treatment modalities. In retrospective NCDB cohort study of 753 adult patients diagnosed with spinal myxopapillary ependymomas, Scarpelli et al showed that African American race was significantly associated with decreased use of radiation therapy. 28 Whereas, in another NCDB study of 10 458 patients with spinal meningiomas, Yolcu et al found that African American race did not influence the decision for radiation only, but was an independent predictor of any radiation plus surgery (OR: 2.19) or adjuvant radiation (OR: 2.05). 29 Interestingly, in a retrospective cohort study of 183 patients diagnosed with spinal cord gliomas, Abdel-Wahab et al demonstrated that race was not significantly associated with use of surgery only or postoperative receipt of radiation for patients with ependymoma or astrocytoma. 30 Additional studies are necessary to determine if there exists an underlying racial disparity in standardized treatment approaches in hopes to provide a more equitable patient care.
A number of studies have reported an association between race and mortality among patients with primary spinal cord tumors. Similar to the findings of the Yang et al study, in the Abdel-Wahab et al study of 183 patients with spinal cord gliomas, the authors demonstrated that White race was significantly associated with improved 15-year progression free survival for patients with ependymoma. 30 In the Deb et al national retrospective cohort study of 1,904 patients with primary osseous spinal neoplasms, the authors demonstrated that non-White race was associated with significantly shorter survival time (HR: 1.744). 31 Analogous to the aforementioned studies, upon propensity-score matching, our study found that African American race was a significant independent predictor of all-cause mortality (HR: 1.82). Further, well-controlled prospective studies are necessary to understand and control for various factors that may be causing these disparities in mortality rates to occur.
Conversely, there have been other studies that demonstrate a lack of association between race and survival. In a population-based study of 561 patients with low-grade spinal cord astrocytomas (SCA) captured by the SEER database, Diaz-Aguilar et al found that race (White, African American, or Asian or Pacific Islander) was not significantly associated with overall survival. 32 Similarly, in a retrospective cohort study of 133 patients with primary intradural spinal hemangioblastoma, Westwick et al showed no difference between racial cohorts with respect to mortality. 33 Likewise, in a retrospective cohort study of 131 patients with intradural intramedullary astrocytomas in the SEER database, Khalid et al demonstrated that race had no statistically significant association with survival in either uni- or multivariate analysis. 34 These studies demonstrate the need for further investigation on the impact of racial disparities has on mortality in order to improve the overall quality of care provided for non-White patients.
Along with assessing racial disparities on mortality following diagnosis of primary spinal cord tumors, there have been efforts to identify similar disparities in other healthcare proxy metrics. In a retrospective NIS cohort study of 18 297 adult patients undergoing spinal surgery for a primary benign intradural spine tumor, Kalakoti et al demonstrated that African American race was a significant independent predictor of cardiac complications (OR: 3.04), incidence of DVT (OR: 2.73), prolonged LOS (OR: 1.74), high-end hospital charges (OR: 1.57), and unfavorable discharge disposition (OR: 1.69). 35 Similarly, in another NIS study of 15 545 patients undergoing surgery for spinal cord tumor, Sharma et al found that African American race was significantly associated with increased adverse discharge dispositions and hospital costs. 36 In a national retrospective cohort study of 19 017 patients undergoing resection of a spinal cord tumor, Patil et al demonstrated that, compared to White patients, African American patients were at increased risk of prolonged LOS (OR: 1.6) and post-operative complication (OR: 1.9) which increased mean hospital chargers by over $10 000 per complication. 37 As risk stratification calculators and models are being created, assessing the influence that race has on all hospital metrics may be necessary to accurately optimize perioperative and post-discharge patient quality care. Our study provides insight to a potentially modifiable disparity among the management and treatment of patients with spine tumors. While our findings do not identify the cause of the all-cause mortality between the cohorts, our results do spark inquiry for further investigations. These inquiries include determining how racial differences in the temporal delay of presentation, diagnosis and surgical intervention effect overall survival. Further investigations are warranted to better elucidate where and why racial disparities may exist in health systems and clinical practices.
This study has several limitations that may impact its interpretation. First, the variables and outcomes were reviewed retrospectively and based solely on data available in the SEER database, which may have been affected by reporting bias, coding bias, loss to follow-up or attrition, and other weaknesses in causal inference associated with all retrospective database studies. Secondly, differences have been demonstrated between results gathered from the SEER database and other similar national cancer databases for primary central nervous system neoplasms, which may limit the generalizability or comparability of our results. 38 Third, we pooled mortality into “all-cause mortality” and did not account for disease- or tumor-specific mortality. Furthermore, tumors of the cauda equina were not included given the risk of cauda equina syndrome which may have implications in our findings. Lastly, our study is limited by the definition of race provided by SEER, which is inherently administrative and is not nuanced to the important variability present in personal and cultural conceptions of race and ethnicity. We acknowledge that race is an inherently cultural and administrative construct, and not a biological entity. 39 Despite these limitations this study demonstrates that racial disparities may exist in survival for patients with malignant or nonmalignant tumor of the spinal cord or spinal meninges.
Conclusion
Our study suggests that African American patients diagnosed with a malignant or nonmalignant tumor of the spinal cord or spinal meninges may have a higher risk of all-cause mortality compared to White patients. Further studies are necessary to elucidate the underlying perpetual factors contributing to the racial disparities in mortality for patients diagnosed with spinal cord tumors in order to better overall quality and equality of patient care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.