
Abstract
Study Design
Systematic review.
Objective
To compare the efficacy of the posterior approach and combined anterior-posterior approach in the treatment of ankylosing spondylitis (AS) with cervical spine fracture by meta-analysis.
Methods
The databases PubMed, Web of Science, Embase, and Cochrane Library were searched for studies on the comparison of the posterior approach group and the combined anterior-posterior approach group in the treatment of ankylosing spondylitis combined with cervical spine fracture from database establishment to August 2023. The procedure time, intraoperative blood loss, the rates of neurological improvement, mean change in the postoperative neurological function, complication rates, rates of revised surgery, and mortality were extracted. Meta-analysis was performed using RevMan 5.4 software provided by Cochrane Library.
Results
A total of 11 retrospective cohort studies with a total of 215 patients were included in this study. The posterior approach group had lower intraoperative blood loss than the combined anterior-posterior approach group [Mean difference (MD) = -146.05, 95%CI(-187.40,-104.69), P < .00001]; the operation time was significantly less in the posterior approach group than in the combined anterior-posterior approach group [MD = -95.34, 95%CI(-113.13,-77.55), P < .00001]. There were no statistically significant differences in the neurological improvement rates, mean changes in postoperative neurological function, complication rates, modified surgery rates, and mortality rates.
Conclusion
Both the posterior approach and combined anterior and posterior approach can achieve good results. Clinicians should develop an individualized approach based on the patient's fracture type, degree of spinal cord injury, fracture stability, fracture dislocation, general condition, and underlying disease.
Keywords
Introduction
Ankylosing spondylitis (AS) is a common chronic inflammatory autoimmune disease characterized by the involvement of axial joints such as the spine and sacroiliac region. The condition of AS continues to progress, eventually leading to bamboo-like changes in the whole spine, spinal flexibility disappeared, accompanied by osteoporosis and increased bone fragility, and slight external force can cause spinal fracture and dislocation. According to the literature, the incidence of spinal fracture and dislocation in patients with AS ranges from 5% to 15%, which is four times that of the average person, 81% of which occurs in the cervical spine, especially in the lower cervical spine and cervicothoracic junction.1,2 According to the current mainstream view in the world, for the treatment of patients with ankylosing spondylitis combined with cervical spine fracture, surgical treatment is superior to conservative treatment in terms of efficacy and life expectancy. 3
The surgical treatment of ankylosing spondylitis combined with cervical spine fracture mainly includes decompression, reduction, fusion, and internal fixation.4,5In terms of surgical approach, although anterior approach surgery alone has the advantages of high safety, short operation time, less blood loss, and low incidence of infection, it is not widely used due to its disadvantages of limited available segments for fixation, postoperative vertebral instability, and high reoperation rate. 6 Currently, the posterior approach and combined anterior-posterior approach are widely used, but which of the two approaches is the best remains controversial. This study intends to perform a meta-analysis and systematic review of the posterior approach and combined anterior-posterior approach in the treatment of ankylosing spondylitis combined with cervical spine fracture from the aspects of intraoperative indicators, postoperative neurological changes, complication rate, reoperation rate, and mortality, to guide clinical practice.
Methods
This study was completed following the Systematic reviews and meta-analyses in spine surgery, neurosurgery, and orthopedics: guidelines for the surgeon scientist and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for reporting.7,8 Because this study was a systematic review, patient informed consent and ethics committee approval were not required.
Search Strategy
Studies comparing the efficacy of posterior approach and combined anterior-posterior approach in the treatment of ankylosing spondylitis combined with cervical spine fracture were searched from PubMed, Web of Science, Cochrane Library, and Embase databases until August 2023. The search strategy was as follows: ((ankylosing spondylitis) AND (cervical spine fracture)) AND ((combined anterior-posterior approach) OR (posterior approach) OR (approach)). In addition, we searched the references of some relevant review articles to identify additional eligible studies.
Selection Criteria
The inclusion criteria for this systematic review and meta-analysis were as follows: (1) retrospective clinical study of posterior approach and combined anterior-posterior approach surgery for ankylosing spondylitis combined with cervical spine fracture; (2) results included at least two of the following indicators: procedure time, intraoperative blood loss, the rates of neurological improvement, mean change in the postoperative neurological function, complication rates, rates of revise surgery, rates of death in the group, and fracture healing time in each study.
The exclusion criteria for this systematic review and meta-analysis were as follows: (1) animal experiments or in vitro/biomechanical studies; (2) studies included only posterior approach or combined anterior-posterior approach; (3) meeting, expert opinion, or case report; (4) literature that could not obtain the full text.
Literature Selection
We first screened the literature using NoteExpress software (Version 3.3) to eliminate duplicates. Subsequently, two investigators independently completed literature screening according to the inclusion and exclusion criteria and checked the screening results and the disagreement between them in some studies needed to be resolved in discussion with a third investigator.
Data Extraction and Assessment of Study Quality
Data extraction was performed by two investigators and required data included the first author, publication year, country, study design method, number of patients, mean age, preoperative and postoperative American Spinal Injury Association (ASIA) grade, preoperative and postoperative Frankel grades, operation time, intraoperative blood loss, complications, reoperation rate, and mortality. In the included literature, ASIA or Frankel scores were used for the evaluation of preoperative and postoperative neurological function. In order to evaluate the neurological improvement after surgery more objectively, we specifically introduced the neurological improvement rate and mean postoperative neurological changes. Neurological improvement rate was defined as the number of patients with postoperative neurological improvement divided by the total number of patients undergoing surgery; mean postoperative neurological changes were defined as the sum of postoperative neurological improvement grades divided by the total number of patients undergoing surgery. Discrepant data were resolved by discussion with a third investigator. The retrospective cohort study used the Newcastle-Ottawa Quality Assessment Scale (NOS) to assess the quality of the literature.
Statistical Analysis
The extracted data were analyzed using RevMan 5.4 software. Heterogeneity was tested using the χ2 test and inconsistency index statistics (I 2 ), and a random-effects model was used if there was significant heterogeneity (I 2 > 50% and P < .1), and a fixed-effects model was used if there was homogeneity (P ≥ .1 and I 2 ≤ 50%). Mean difference (MD) and odds ratio (OR) were used as effect analysis statistics (95% CI) for continuous and binary variables, respectively.
Results
Study Selection and Characteristics
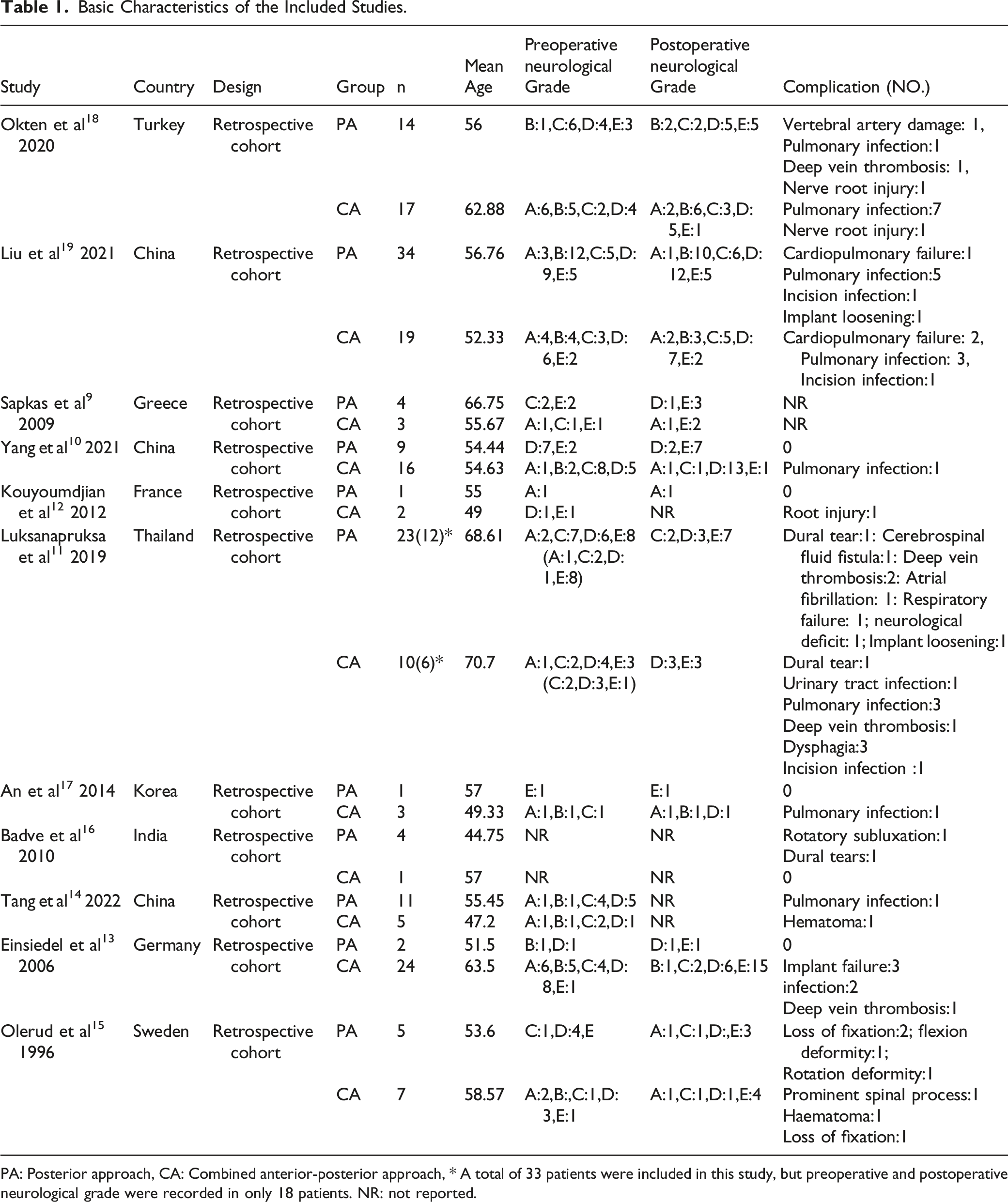
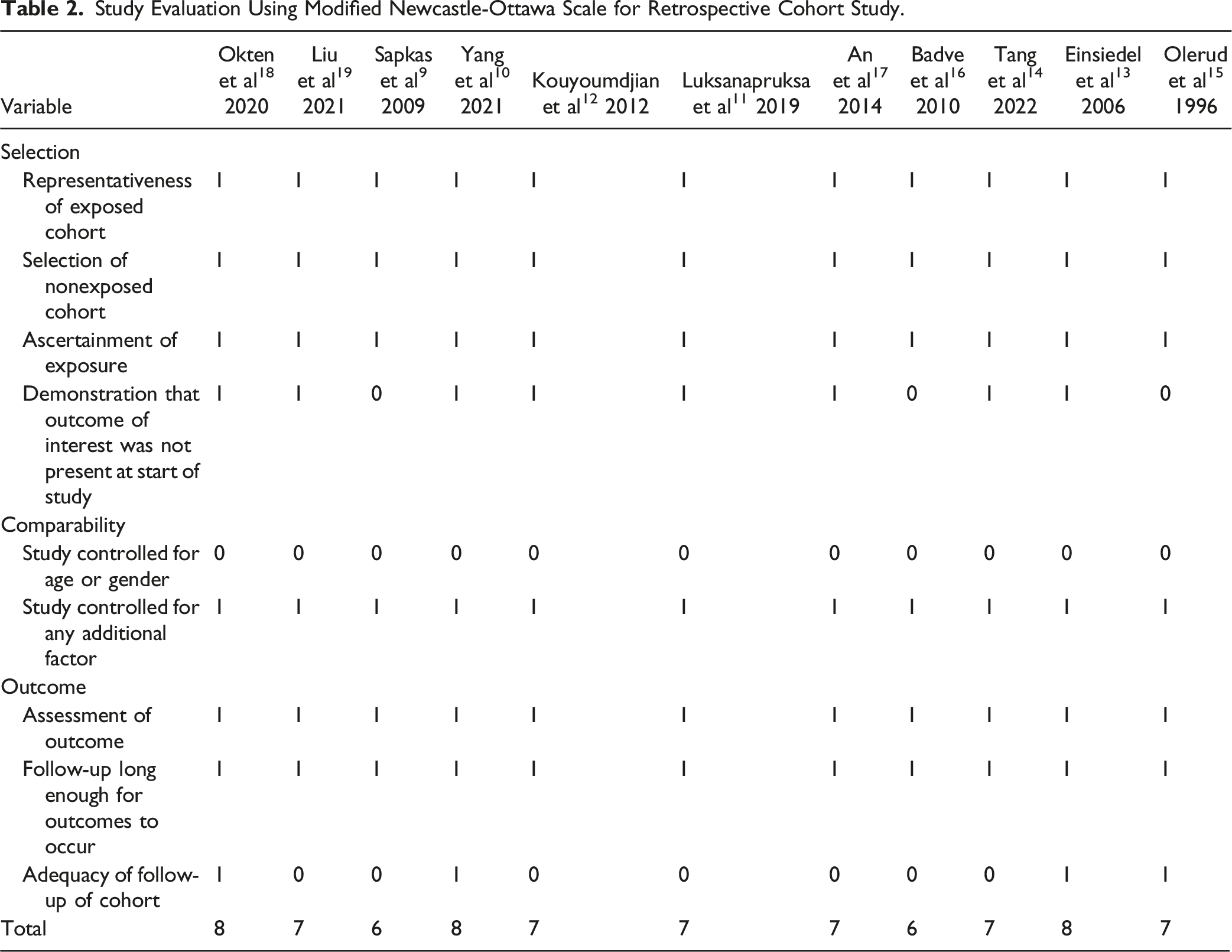
A total of 299 papers were obtained from the preliminary search, 201 duplicate published papers were eliminated by NoteExpress software (Version 3.3) software, and 68 papers that did not meet the inclusion criteria were screened by reading the title and abstract content,19 papers were excluded by a careful reading of the full text of the remaining 30 papers, and 11 papers9-19 were finally included in this study. The screening process is shown in Figure 1. A total of 215 patients were included in this study, including 108 patients in the posterior approach group and 107 patients in the combined anterior-posterior approach group. Further information on the included studies is presented in Table 1. The quality assessments for the retrospective studies using the Newcastle-Ottawa scale (score range, 6-8, with 6 positive responses considered to indicate a good quality study) are listed in Table 2. This study was registered on the International Prospective Register of Systematic Reviews (PROSPERO) (ID: CRD42023408281). Flowchart of search strategy and results. Information: 11 articles were filtered out from 299 original literatures. Basic Characteristics of the Included Studies. PA: Posterior approach, CA: Combined anterior-posterior approach, * A total of 33 patients were included in this study, but preoperative and postoperative neurological grade were recorded in only 18 patients. NR: not reported. Study Evaluation Using Modified Newcastle-Ottawa Scale for Retrospective Cohort Study.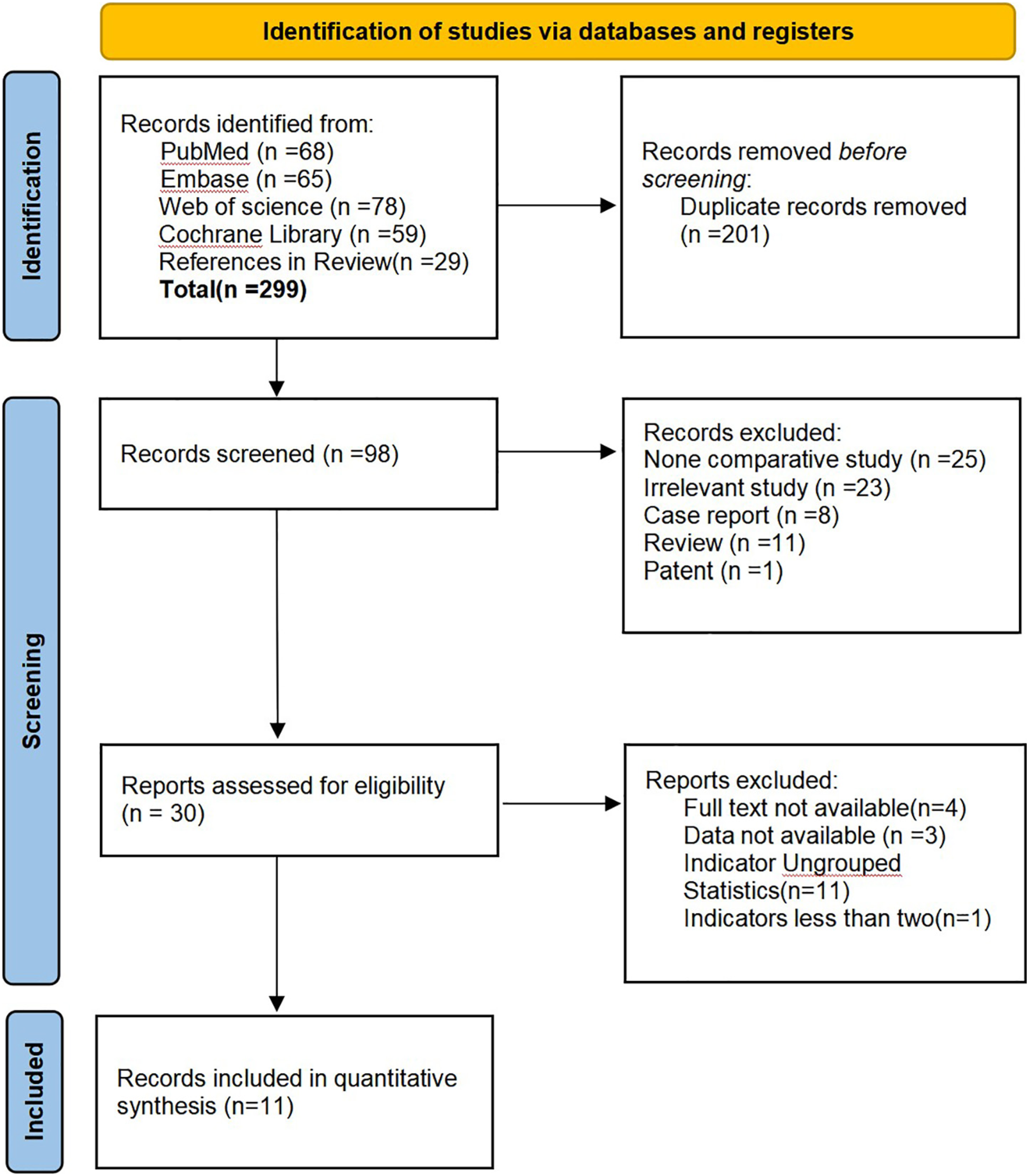
Meta-Analysis Results
Intraoperative Blood Loss
Three studies counted intraoperative blood loss, including 43 cases of the posterior approach group and 31 cases of the combined anterior-posterior approach group, with no significant heterogeneity among various studies(P = .23, I
2
= 32%). A meta-analysis of intraoperative blood loss using a fixed-effects model showed that the amount of bleeding was significantly less in the posterior approach group than in the combined anterior-posterior approach group[MD = −146.05, 95% CI (−187.40, −104.69), P < .00001, Figure 2]. Forest plot of intraoperative blood loss. PA: Posterior approach, CA: Combined anterior-posterior approach.
Operation Time
Four studies counted operation time, including 48 cases of the posterior approach group and 37 cases of the combined anterior-posterior approach group, with no significant heterogeneity among various studies(P = .45, I2 = 0%). A meta-analysis of operation time using a fixed-effects model showed that the operation time was significantly less in the posterior approach group than in the combined anterior-posterior approach group[MD = −95.34, 95% CI (−113.13, −77.55), P < .00001, Figure 3]. Forest plot of operation time. PA: Posterior approach, CA: Combined anterior-posterior approach.
Neurological Function Improvement Rate
A total of 107 cases in the posterior approach group and 105 cases in the combined anterior-posterior approach group, in 10 studies, had reported the neurological function improvement rate, with no significant heterogeneity among various studies (P = .98, I
2
= 0%). Meta-analysis of the neurological function improvement rate using the fixed effects model showed that the neurological function improvement rate in the posterior approach group was slightly lower than that in the combined anterior-posterior approach group[OR = .76, 95% CI (.41, 1.42), P = .39, Figure 4], suggesting that there was no statistically significant difference in neurological function improvement rate between the two groups. Forest plot of neurological function improvement rate. PA: Posterior approach, CA: Combined anterior-posterior approach.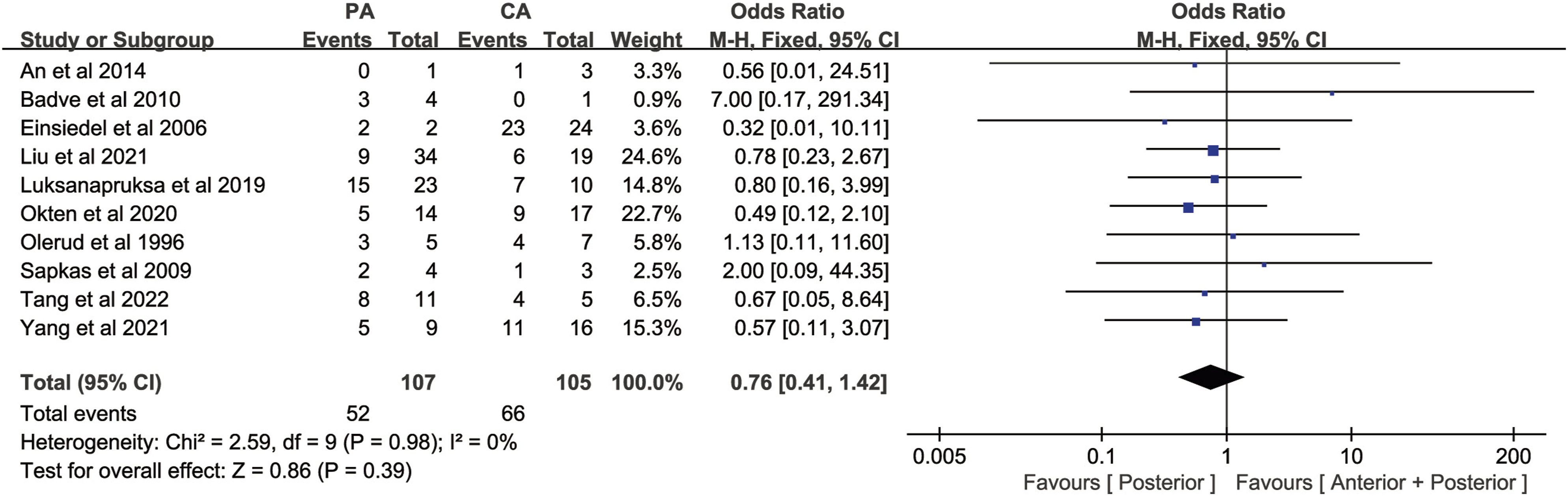
Mean Change in neurological Function after Surgery
A total of 81 cases in the posterior approach group and 94 cases in the combined anterior-posterior approach group, in 8 studies, had reported the mean change in neurological function after surgery, with no significant heterogeneity among various studies(P = .87, I
2
= 0%). Meta-analysis of the mean change in neurological function after surgery using the fixed effects model showed that the mean change in neurological function after surgery in the posterior approach group was lower than that in the combined anterior-posterior approach group[MD = −.17, 95% CI (−.35, .02), P = .07, Figure 5], suggesting that there was no statistically significant difference in mean change in neurological function after surgery between the two groups. Forest plot of mean change in neurological function after surgery. PA: Posterior approach, CA: Combined anterior-posterior approach.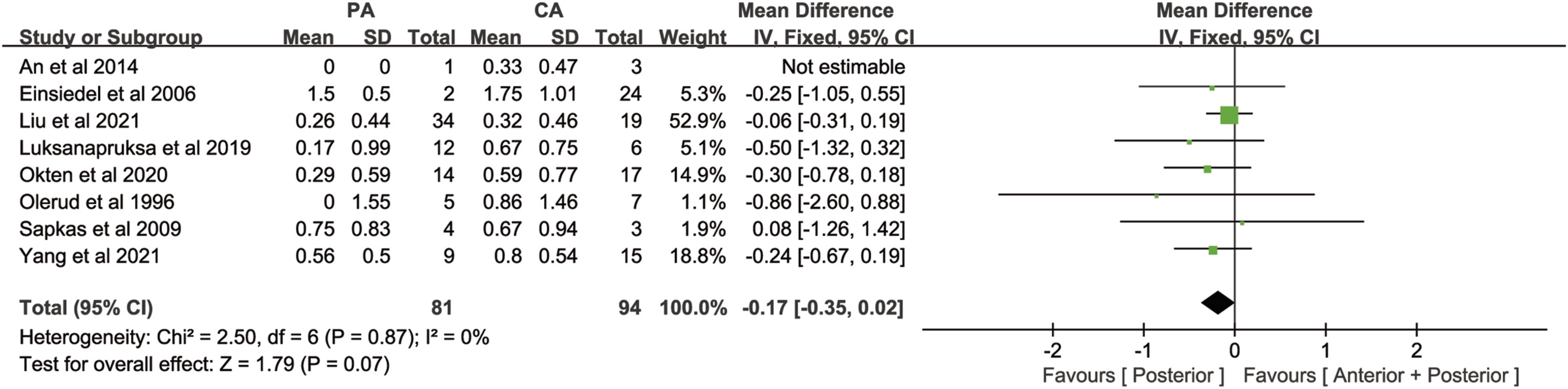
Complication
Ten studies counted complications, including 104 cases of the posterior approach group and 104 cases of the combined anterior-posterior approach group, with no significant heterogeneity among various studies(P = .56, I
2
= 0%). Meta-analysis of the complication rate using the fixed effects model showed that the complication rate in the posterior approach group was slightly lower than that in the combined anterior-posterior approach group[OR = .65, 95% CI (.34, 1.25), P = .20, Figure 6], suggesting that there was no statistically significant difference in complication rate between the two groups. Forest plot of complication. PA: Posterior approach, CA: Combined anterior-posterior approach.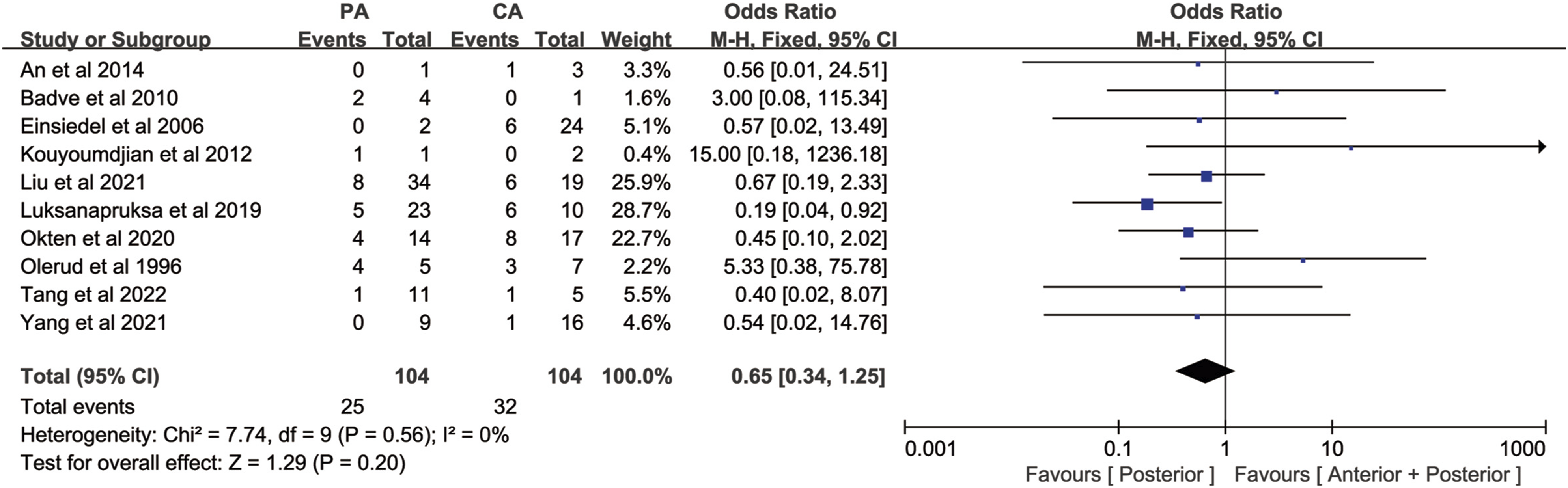
Revision Surgery Rate
Three studies counted revision surgery, including 11 cases of the posterior approach group and 32 cases of the combined anterior-posterior approach group, with no significant heterogeneity among various studies (P = .87, I
2
= 0%). Meta-analysis of the revision surgery rate using the fixed effects model showed that the revision surgery rate in the posterior approach group was slightly higher than that in the combined anterior-posterior approach group[OR = .77, 95% CI (.15, 4.15), P = .76, Figure 7], suggesting that there was no statistically significant difference in revision surgery rate between the two groups. Forest plot of revision surgery rate. PA: Posterior approach, CA: Combined anterior-posterior approach.
Mortality
Eight studies counted the number of deaths, including 92 cases of the posterior approach group and 96 cases of the combined anterior-posterior approach group, with no significant heterogeneity among various studies (P = .67, I
2
= 0%). Meta-analysis of the mortality using the fixed effects model showed that the mortality in the posterior approach group was slightly higher than that in the combined anterior-posterior approach group[OR = .59, 95% CI (.22, 1.60), P = .76, Figure 8], suggesting that there was no statistically significant difference in mortality between the two groups. Forest plot of mortality. PA: Posterior approach, CA: Combined anterior-posterior approach.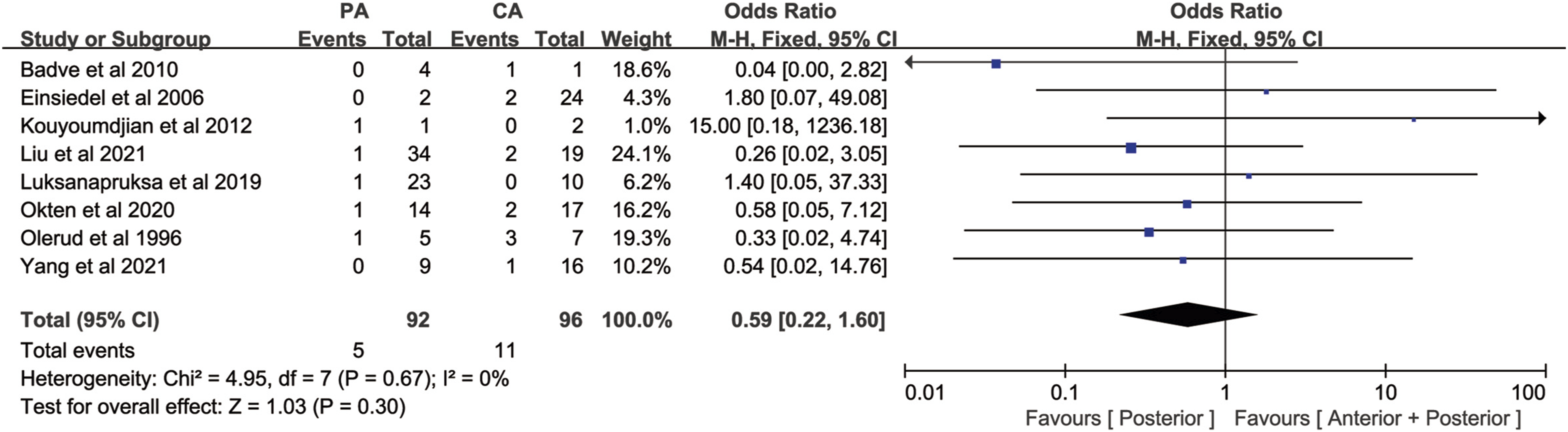
Sensitivity Analysis and Publication Bias
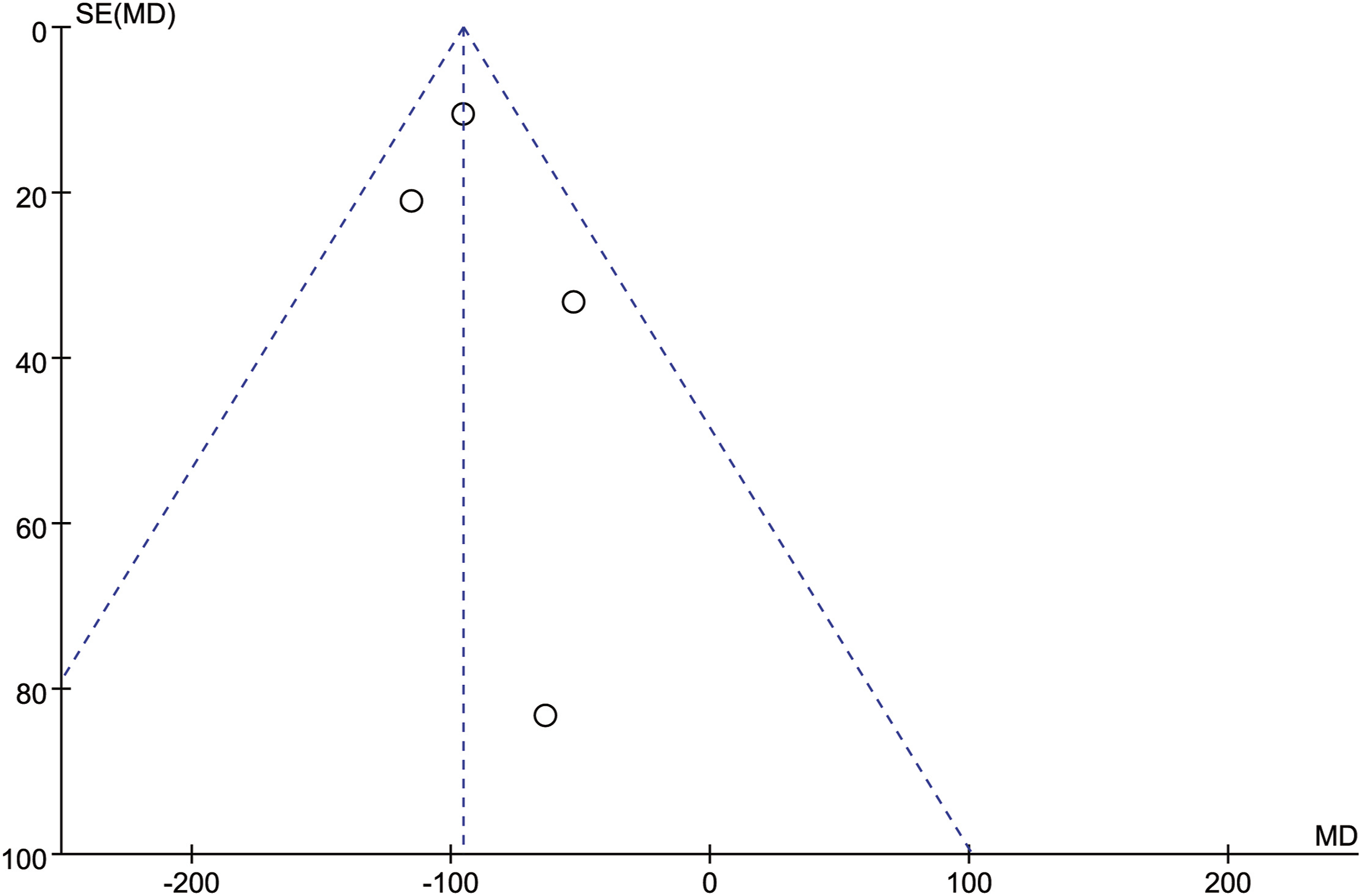
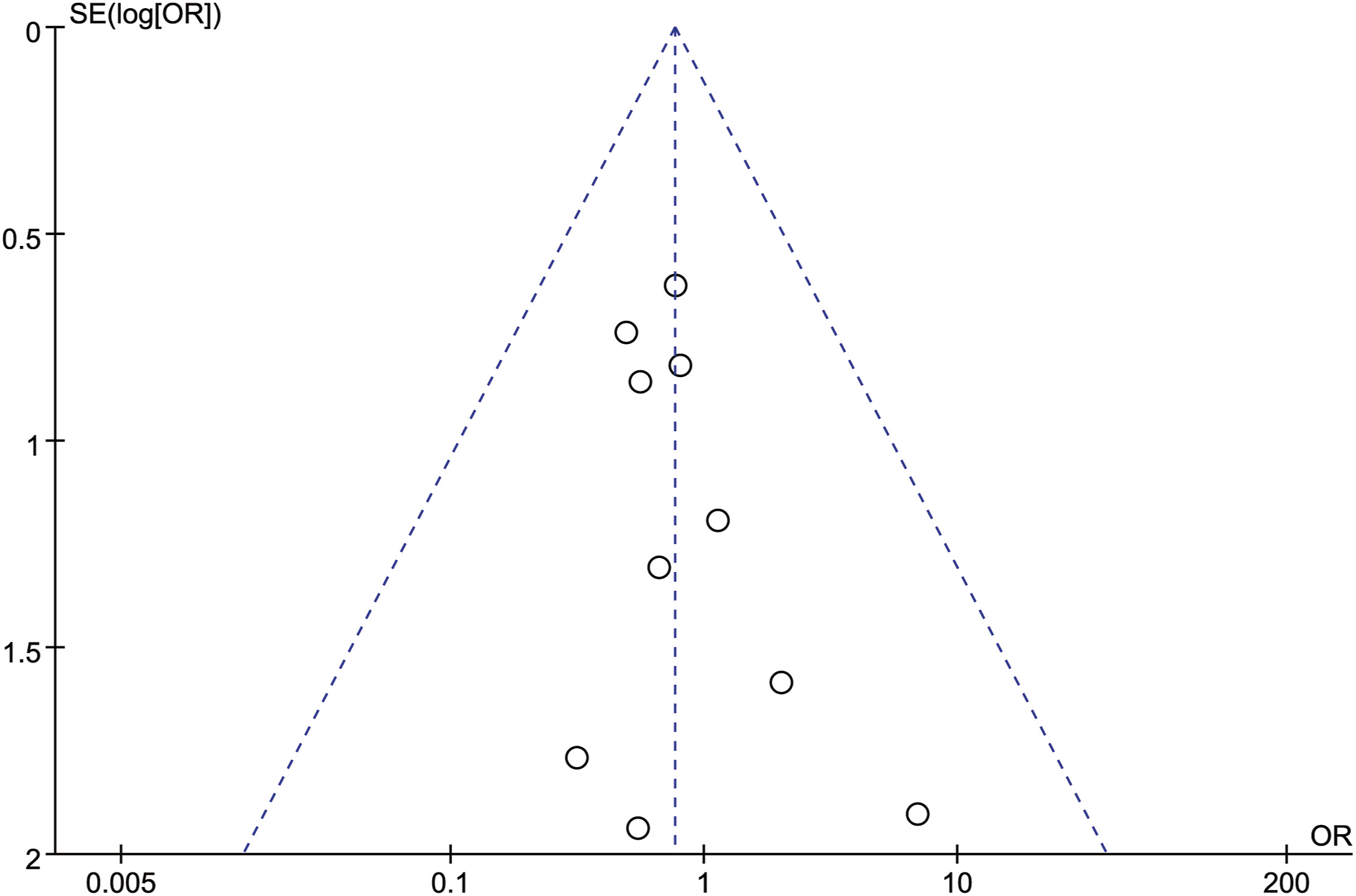
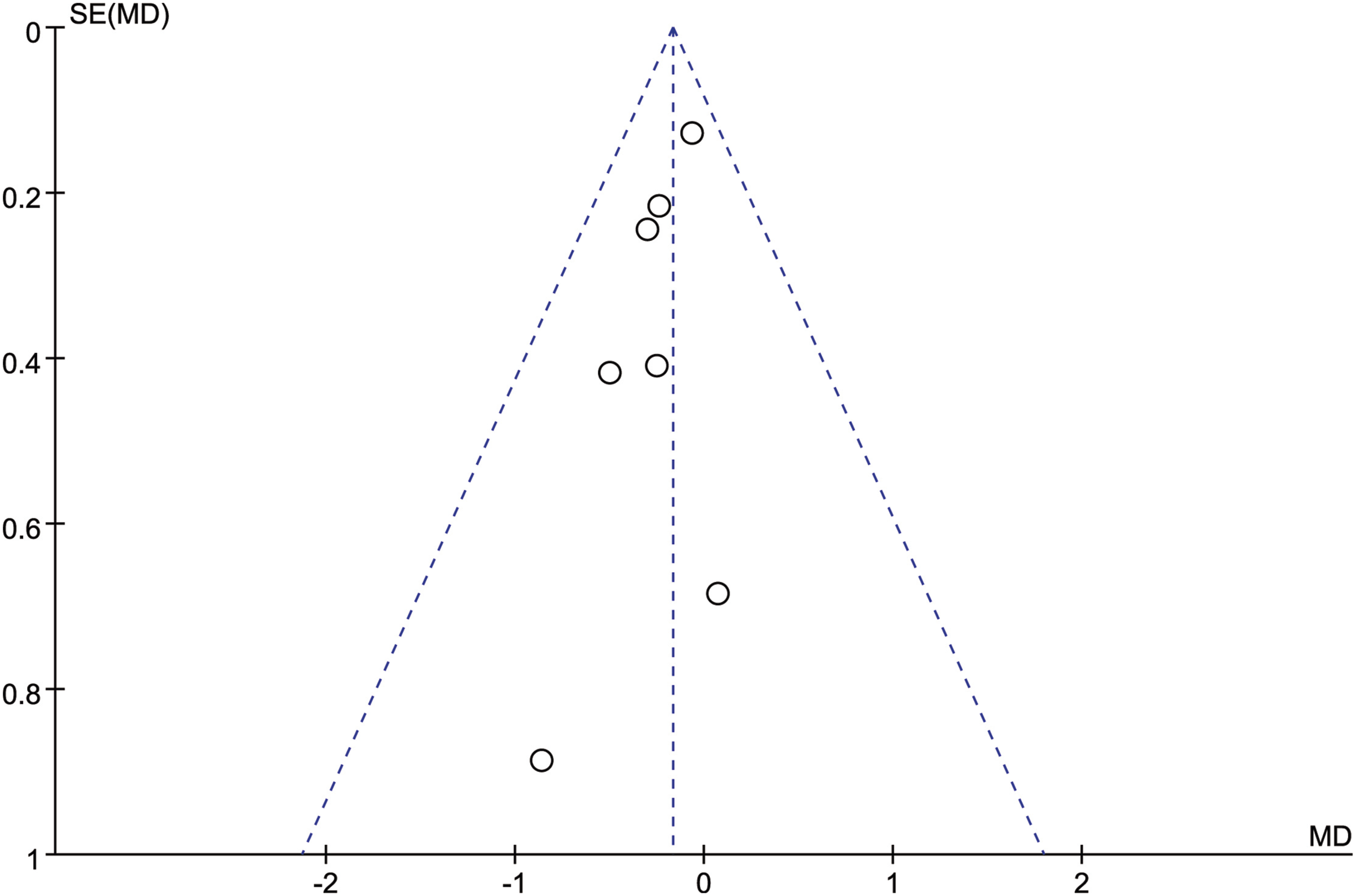
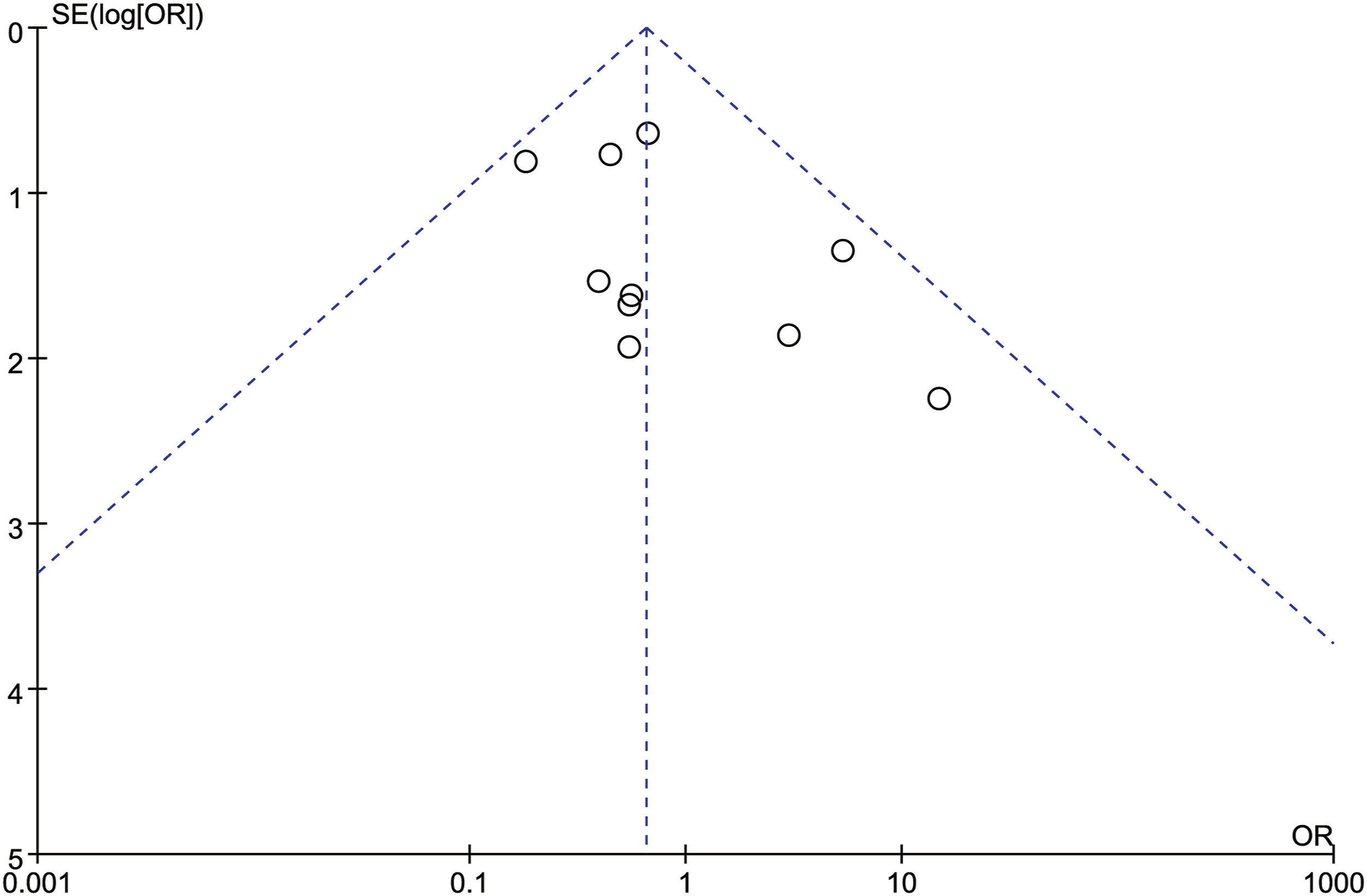
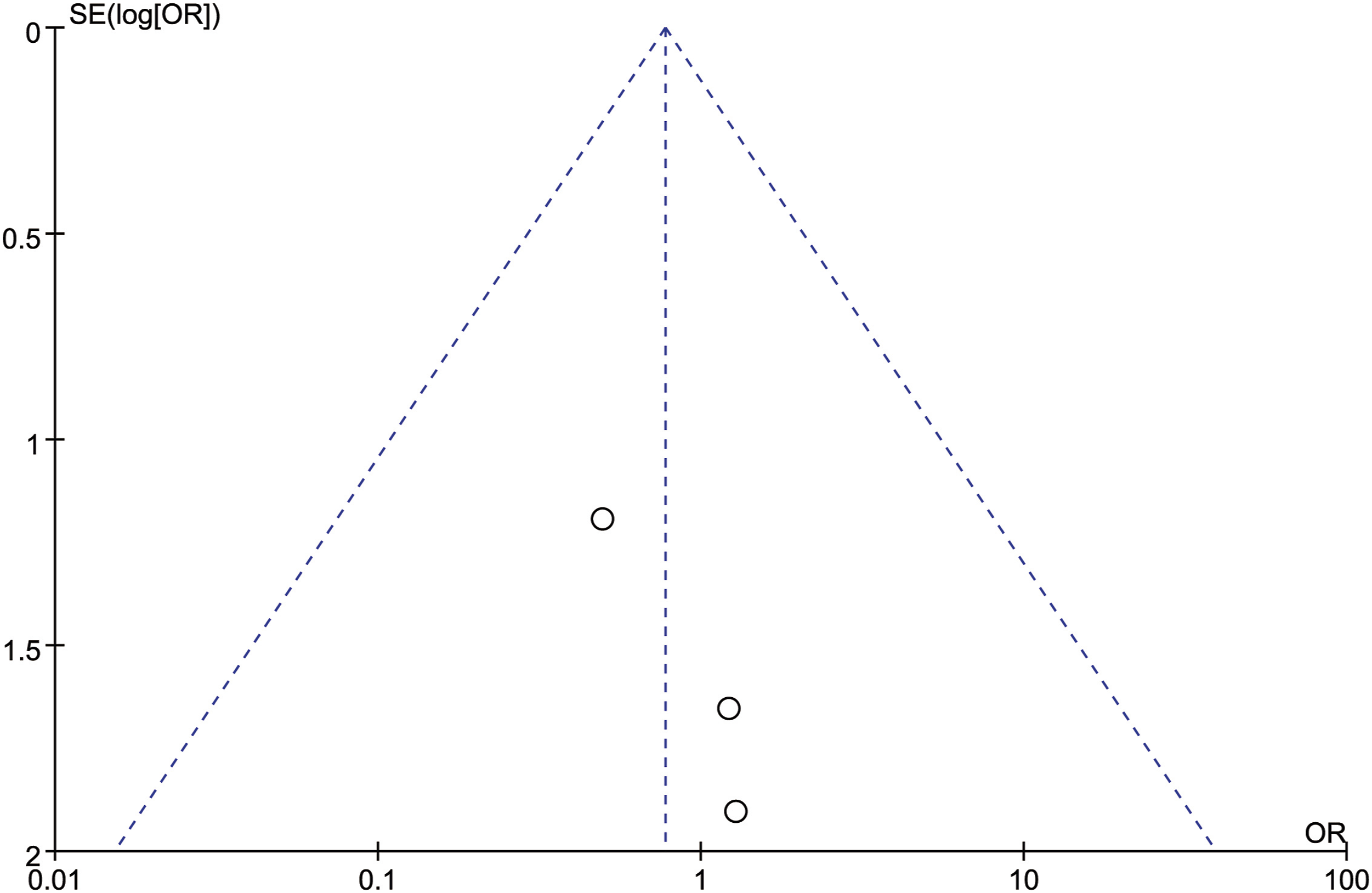
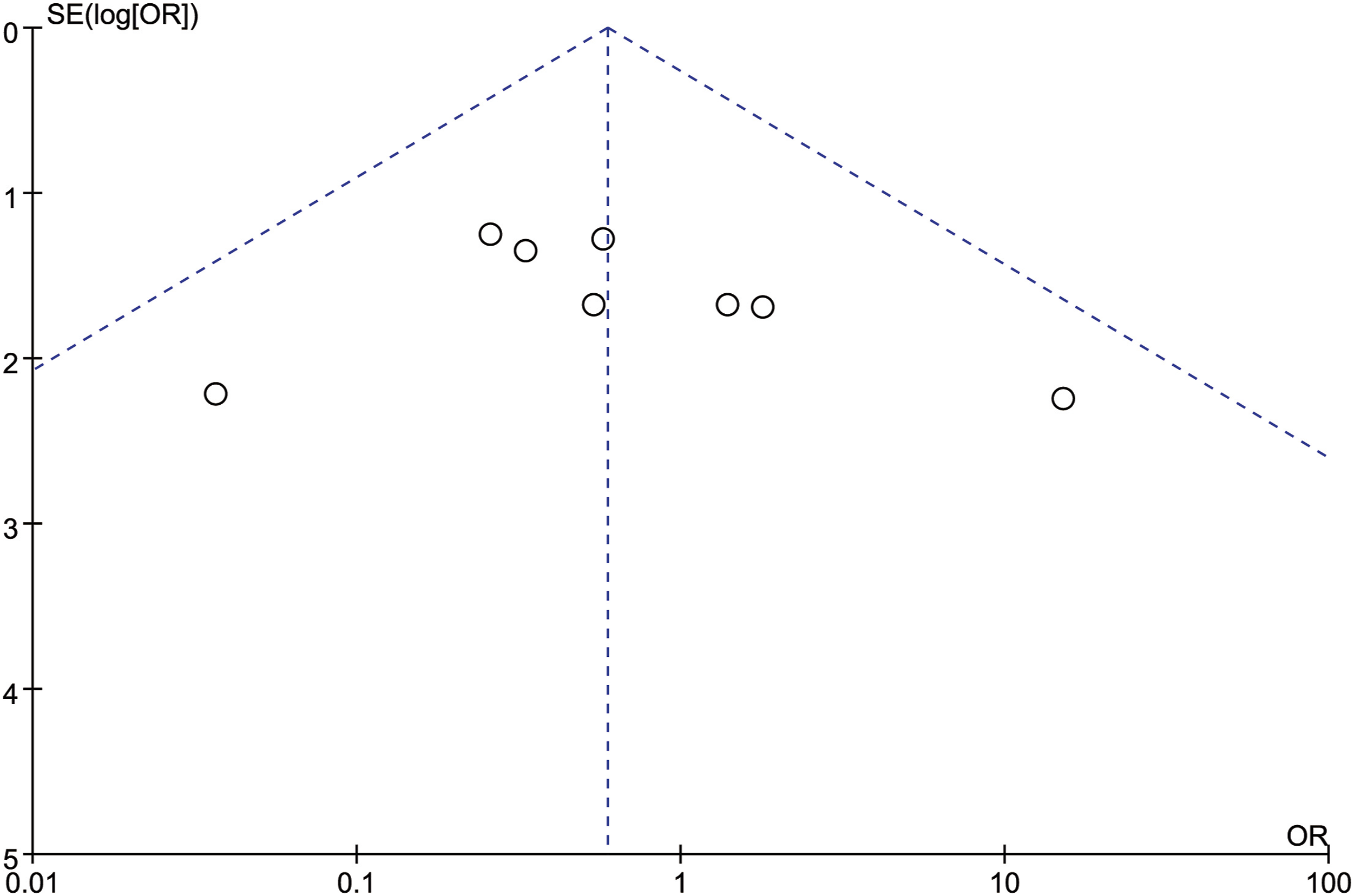
In order to test the reliability of the above analysis results, we changed the fixed-effect model used for all the above indicators to a random-effect model, sequentially excluding the studies with the largest and smallest weights, and no significant difference was observed compared with the fixed-effect model results, which indicated that our results were reliable. A total of 11 articles were included in this study. All outcome measures were tested for publication bias. It could be seen that the funnel plot of each outcome measure was visually basically symmetrical, suggesting that there was a small possibility of publication bias (Figures 9–15). Funnel plot of publication bias for intraoperative blood loss. Funnel plot of publication bias for operation time. Funnel plot of publication bias for neurological function improvement rate. Funnel plot of publication bias for mean change in neurological function after surgery. Funnel plot of publication bias for complication. Funnel plot of publication bias for revision surgery rate. Funnel plot of publication bias for mortality.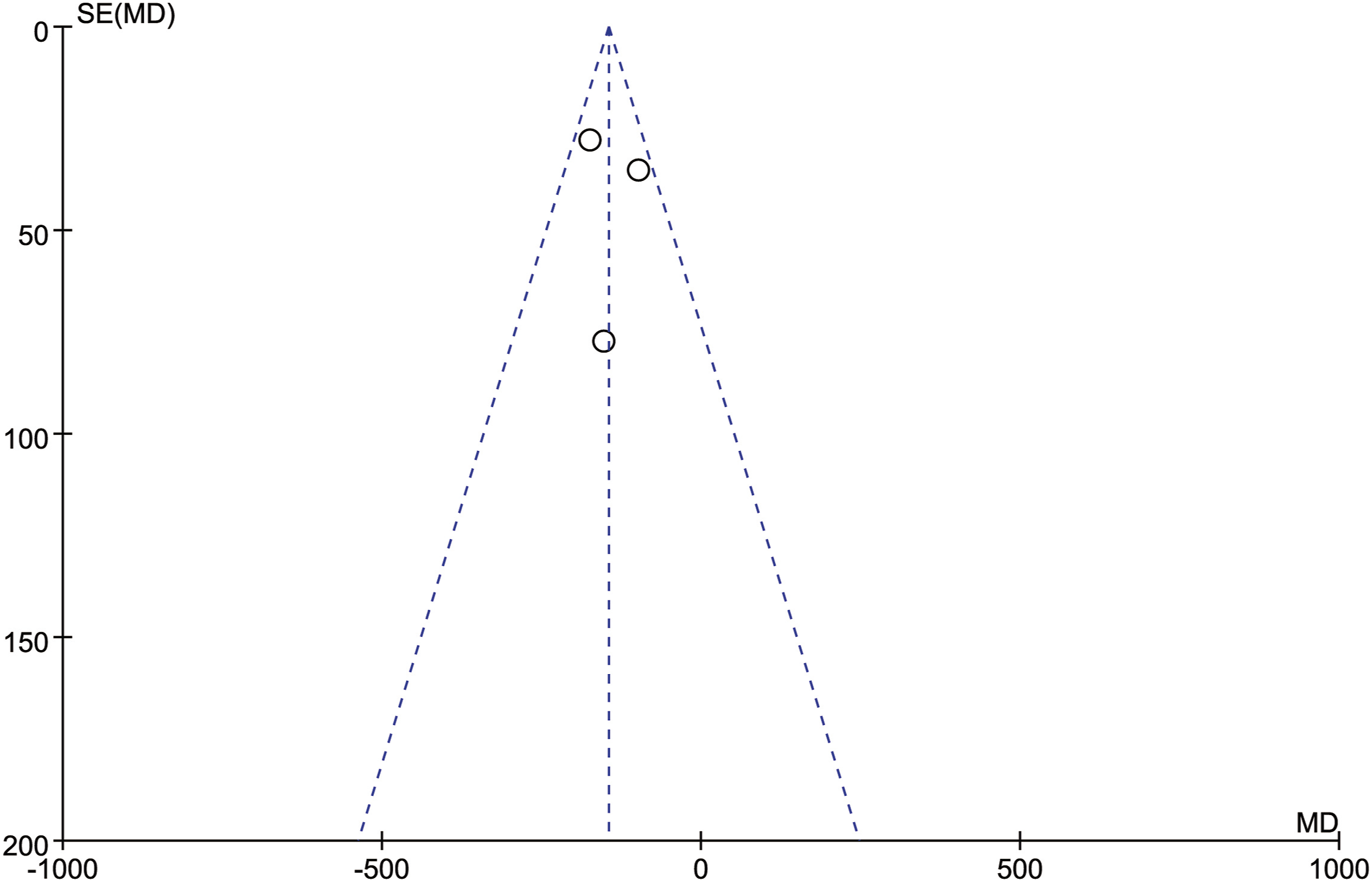
Discussion
AS is a chronic systemic autoimmune disease of unknown etiology that usually starts in the sacroiliac joint and is characterized by inflammation, hyperplasia, osteoporosis, and bony fusion of the sacroiliac joint, followed by an invasion of the paravertebral ligaments, facets, and peripheral joints along the central axis of the spine.20,21 With the continuous progress of the disease, it will eventually lead to bamboo-like changes in the whole spine and loss of spinal flexibility, accompanied by osteoporosis and increased bone fragility, slight external force can cause spinal fracture and dislocation.22,23 Ankylosing spondylitis with a spinal fracture is most common in the cervical spine easy to complicate cervical spinal cord injury, and leads to serious nerve injury in patients.24,25
The diagnosis of ankylosing spondylitis combined with cervical spine fracture is a significant issue that cannot be overlooked. Most cases of ankylosing spondylitis combined with cervical spine fracture are caused by minor trauma. The presence of chronic pain symptoms due to AS and the fact that most patients are receiving corticosteroids may mask the symptoms of fractures.12,26,27 In Shetty's study, four patients presented to the hospital with neurological symptoms several days after a trauma despite having intact neurological function immediately after trauma. 28 Simultaneously, changes in spinal anatomy, ligament ossification, and artifacts resulting from the development of long-term AS conditions may cause X-ray imaging of the cervical spine to fail to identify fractures in a timely manner. 29 In Kouyoumdjian and Sapkas' study, 36% and 60% of patients failed to accurately diagnose cervical spine fracture in the initial radiographic findings, resulting in delayed diagnosis and increased risk of neurological complications.9,12 Therefore, CT scan and MRI scan should be used to increase the sensitivity of the first radiological assessment to reduce the occurrence of missed diagnosis as well as delayed diagnosis, especially when there is an interval between trauma and neurological symptoms or neurological image deterioration, the formation of an epidural hematoma should be excluded by MRI scan. At the same time, strict external fixation and other necessary precautions are recommended throughout the diagnosis and before definitive treatment to avoid fracture dislocation or secondary nerve injury. 30
Woodruff et al 31 first reported the case series of ankylosing spondylitis combined with cervical spine fracture in 1963, its therapeutic principles have undergone several updates. Before 1989, conservative treatment was considered the gold standard for the treatment of ankylosing spondylitis combined with cervical spine fracture due to the high mortality rate of surgical treatment.32-35 However, the risks of local kyphosis aggravated by conservative treatment, nonunion caused by shear forces, neurological deterioration, bedsores and respiratory complications caused by prolonged bed rest, and skin damage caused by long-term brace wear have increasingly aroused the attention of clinicians. 28 At the same time, with the continuous improvement of surgical techniques, internal fixation provides better reduction and maintains stability during bone healing, and also has advantages in relieving spinal cord compression and reducing the time of bed immobilization, Gradually, conservative treatment has been gradually replaced by surgical treatment. 30 Current literature regarding ankylosing spondylitis combined with cervical spine fracture management has established that surgical treatment is superior to conservative management in terms of efficacy and life expectancy, but the ideal approach for surgical treatment remains controversial. 3 Anterior surgery alone has the advantages of a short operation time, less blood loss, fewer incision-related complications, and direct anterior decompression, but due to the disadvantages of limited anterior fixation levels, postoperative vertebral instability, and high reoperation rates, many researchers recommend the use of posterior approach or combined anterior-posterior approach to replace anterior surgery alone. 4
The results of this meta-analysis showed that the usage rate of posterior approach and combined anterior-posterior approach is essentially the same in ankylosing spondylitis combined with cervical spine fracture patients (108 vs 107). Compared with the combined anterior-posterior approach group, the posterior approach group had shorter operation times and less intraoperative blood loss, and the difference was statistically significant. There were no statistically significant differences between approaches in neurological improvement, complications, reoperations, and mortality. Olerud et al 15 first explored the approach for ankylosing spondylitis combined with cervical spine fracture in 1995, they concluded that the risk of initial nerve injury after fracture is high, and the risk of secondary neurological deterioration is substantial, so combined anterior-posterior approach is recommended to provide more secure fixation to reduce postoperative complications. However, our meta-analysis results showed that there was no statistical difference in postoperative complications between the combined anterior-posterior approach and posterior approach, whereas posterior approach was slightly superior to combined anterior-posterior approach in terms of postoperative complications, mortality, and reoperation rate. combined anterior-posterior approach require anterior and posterior incisions for reduction and internal fixation, which certainly increases the operation time and intraoperative blood loss, while patients with ankylosing spondylitis are usually accompanied by kyphosis and tilt deformity, 9 which are extremely difficult to operate when performing anterior surgery at the cervicothoracic junction, which in turn further increases the operation time, intraoperative blood loss and the chance of wound infection. Most AS patients suffer from cardiovascular and pulmonary diseases caused by restrictive rigidity of the thoracic cavity, 9 and the increase in operation time and intraoperative blood loss is bound to increase the burden on the heart and lungs and cause cardiopulmonary complications. According to our statistics of complications, cardiopulmonary complications occurred in more patients in the combined anterior-posterior approach group than in the posterior approach group (15.7% vs 9.3%). Therefore, we suggest that posterior approach should be preferred in the choice of surgical approach for patients with cardiopulmonary disease and restrictive rigidity of the thoracic cavity.
For patients with ankylosing spondylitis combined with cervical spine fracture, the improvement of postoperative neurological function is an important indicator to evaluate surgical methods. However, according to the statistical results of our included literature, combined anterior-posterior approach improved neurological function slightly better than posterior approach, but the difference was not statistically significant, which may be due to the limited number of patients included in the existing literature. In Panya et al's 11 study, it was clearly stated that the combined anterior-posterior approach group showed a higher rate of postoperative neurological improvement than the posterior approach group and that two patients in the posterior approach group experienced postoperative neurological deterioration. Similarly, the results of Okten et al 18 showed that the mean neurological improvement rate after surgery in the combined anterior-posterior approach group was significantly better than that in the posterior approach group, and the difference was statistically significant. According to our analysis, this may be related to the more reliable fixation provided by the combined approach. Posterior long-segment fixation may be an effective method to increase fixation stability in posterior surgery. Cornefjord et al 36 found that long levels of posterior fixation could provide more reliable fixation. Therefore, the appropriate addition of fixed levels when using a posterior approach can effectively improve the stability of fixation.
In summary, The degree of postoperative neurological recovery is closely related to the degree of cervical spinal cord injury and the presence or absence of diagnostic delay. The choice of surgical approach is only to obtain more adequate decompression and more reliable fixation, thus providing a good in vivo environment for the recovery of nerves. The authors concluded that combined anterior and posterior surgery is suitable for patients with poor cervical bone quality, severe destruction of all three columns, difficulty in reduction of fracture dislocation, and compression of the anterior and posterior spinal cord, while posterior surgery alone is suitable for fractures with good axial weight-bearing function of the anterior column, especially for patients with facet joint locking at the fracture dislocation. In addition, we recommend that posterior approaches be favored when selecting approaches for patients with underlying cardiopulmonary disease and poor general conditions.
This study remains subject to several limitations: 1) All articles included in this study were retrospective cohort studies and the number of patients included was small. More cases and prospective or multicenter studies may yield more convincing results. 2) We tried to collect information about patients' preoperative underlying cardiopulmonary disease in the included literature, but unfortunately, it was not documented, so the conclusion that the combined approach increases the burden on patients' heart and lungs with underlying cardiopulmonary disease and thus causes cardiopulmonary complications is less persuasive.
Conclusions
Overall, this article discusses the efficacy of combined anterior and posterior approach vs posterior approach alone in the treatment of patients with ankylosing spondylitis and cervical spine fractures. There was no statistically significant difference between the two surgical methods in terms of prognostic indicators. We concluded that AS combined with cervical spine fracture should consider the general condition of patients and the severity of spinal cord injury, fully assess the local deformity, displacement and bone defect of the fracture individualized selection of surgical methods.
Supplemental Material
Supplemental Material - Comparison of Posterior Approach and Combined Anterior-Posterior Approach in the Treatment of Ankylosing Spondylitis Combined With Cervical Spine Fracture: A Systematic Review and Meta-Analysis
Supplemental Material for Comparison of Posterior Approach and Combined Anterior-Posterior Approach in the Treatment of Ankylosing Spondylitis Combined With Cervical Spine Fracture: A Systematic Review and Meta-Analysis by Cong Peng, Haopeng Luan, Kai Liu, and Xinghua Song in Global Spine Journal
Footnotes
Author Contributions
CP, HPL, KL, and XHS developed the research questions and scope of the study. CP, HPL, and KL conducted data screening and data charting. CP drafted the manuscript and prepared tables, and figures with HPL’s contribution. CP, HPL, and XHS developed the literature search strategies in collaboration with the other authors. CP, HPL, and XHS contributed to the organization, analysis, and interpretation of the results. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (82172454).
Data Availability Statement
The data sets generated and analyzed during the current study are not publicly available but can be obtained from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.