
Abstract
Background Context
Several studies have shown that factors such as insurance type and patient income are associated with different readmission rates following certain orthopaedic procedures. The literature, however, remains sparse with regard to these demographic characteristics and their associations to perioperative lumbar spine fusion outcomes.
Purpose
The purpose of this study was to assess the associations between hospital type, insurance type, and patient median income to both 30-day complication and readmission rates following lumbar spine fusion.
Patient Sample
Patients who underwent primary lumbar spine fusion (n = 596,568) from 2010-2016 were queried from the National Readmissions Database (NRD).
Outcome Measures
Incidence of 30-day complication and readmission rates
Methods
All relevant diagnoses and procedures were identified using International Classification of Disease, 9th and 10th Edition (ICD-9, 10) codes. Hospital types were categorized as metropolitan non-teaching (n = 212,131), metropolitan teaching (n = 364,752), and rural (n = 19,685). Insurance types included: Medicare (n = 213,534), Medicaid (n = 78,520), private insurance (n = 196,648), and out-of-pocket (n = 45,025). Patient income was divided into the following quartiles: Q1 (n = 112,083), Q2 (n = 145,755), Q3 (n = 156,276), and Q4 (n = 147,289), wherein quartile 1 corresponded to lower income ranges and quartile 4 to higher ranges. Statistical analysis was conducted in R. Kruskal-Wallis tests with Dunn’s pairwise comparisons were performed to analyze differences in 30-day readmission and complication rates in patients who underwent lumbar spine fusion. Complications analyzed included infection, wound injury, hematoma, neurological injury, thromboembolic event, and hardware failure.
Results
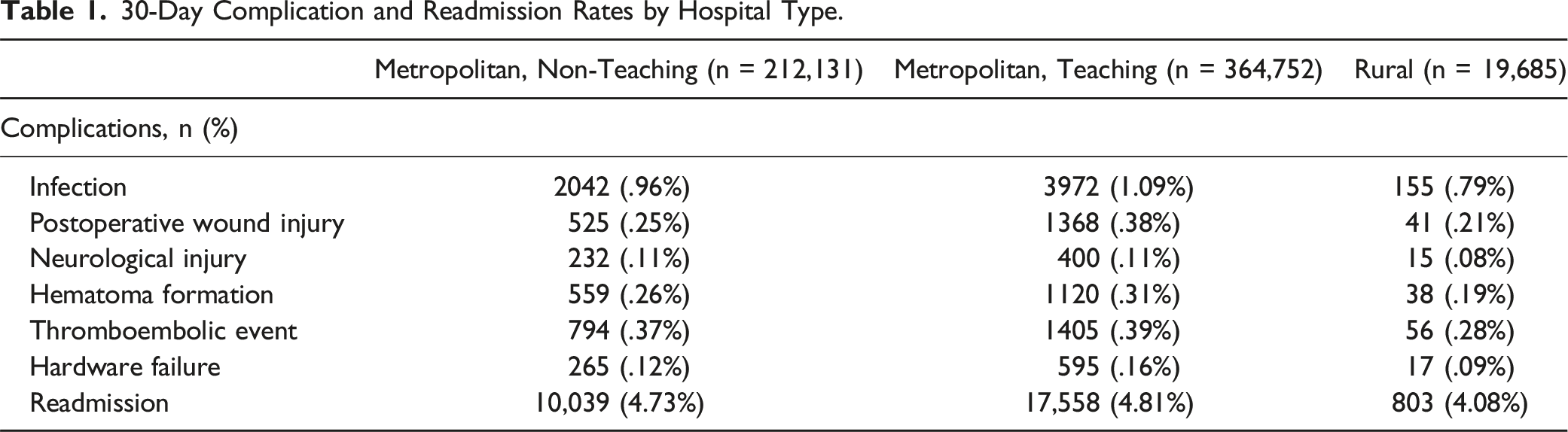
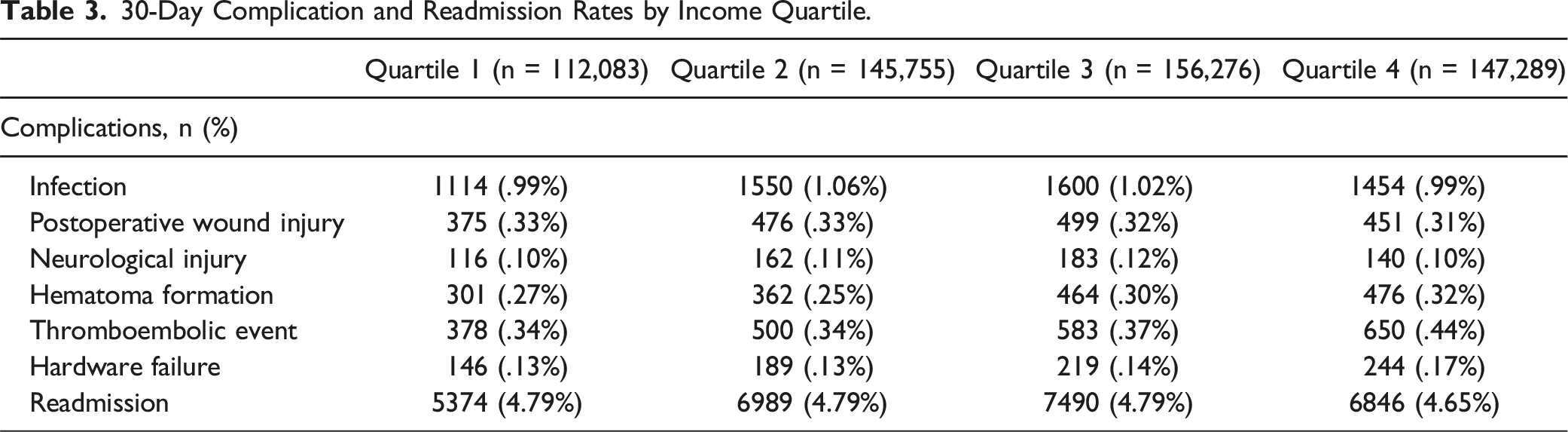
30-day readmission was significantly higher in metropolitan teaching hospitals compared to metropolitan non-teaching hospitals and rural hospitals (P < .05). Patients from metropolitan teaching hospitals had significantly higher rates of infection (P < .001), wound injury (P < .001), hematoma (P = .018), and hardware failure (P < .002) compared to those treated at metropolitan non-teaching hospitals. Privately insured patients were significantly less likely to be readmitted at 30 days than those paying with Medicare or Medicaid (P < .01). Patients with private insurance also experienced significantly lower rates of hematoma formation than Medicare beneficiaries and out-of-pocket payers (P < .01), postoperative wound injury compared to Medicaid patients and out-of-pocket payers (P < .005), and infection compared to all other groups (P < .001). Patients in Quartile 4 experienced significantly greater rates of hematoma formation compared to those in Quartiles 1 and 2 and were more likely to experience a thromboembolic event compared to all other groups.
Conclusion
Patients undergoing lumbar spine fusion at metropolitan non-teaching hospitals and paying with private insurance had significantly lower 30-day readmission rates than their counterparts. Complications within 30 days following lumbar spine fusion were significantly higher in patients treated at metropolitan teaching hospitals and in Medicare and Medicaid beneficiaries. Aside from a few exceptions, however, patient income was generally not associated with differential complication rates.
Introduction
Patient socioeconomic factors and demographic characteristics have been widely established as predictors of postoperative outcomes. Several studies have demonstrated the effect of lower patient socioeconomic status (SES) in precipitating additional financial burden, poorer patient outcomes, and increased complication rates following surgery.1,2 These associations arise from a complex, multifactorial interaction between patient-, provider-, and environmental-related factors ranging from obstacles in healthcare access to lower quality of care overall3,4.
Similar disparities in postoperative outcomes have also been described as a function of patient insurance type and even hospital characteristics. In a retrospective analysis of 103,290 patients undergoing shoulder arthroplasty, Li et al. found significantly increased risk of perioperative medical and surgical complications in Medicare and Medicaid/uninsured patients compared to age- and sex-matched patients with private insurance. 5 Regarding hospital characteristics, Sheetz et al found substantial differences and variation in risk-adjusted surgical outcomes across 87 hospitals listed on or affiliated with the 2018 US News and World Report Honor Roll. In their study, honor roll hospitals demonstrated lower failure to rescue rates but higher complication rates compared to network affiliates; within networks, failure to rescue and complication rates varied up to 4.9 and 4.3-fold respectively. 6
Such disparities in surgical outcomes have also impacted patients undergoing spine surgery. Using the 2003-2004 Spine End Results Registry, Hacquebord et al. found Medicare insurance status to be associated with a 1.68 times higher risk of incurring an adverse event compared to private insurance in patients undergoing any type of spine surgery. 7 In a study of cervical spine surgery patients using the 2002-2009 National Inpatient Sample (NIS), Fineberg et al. observed significantly increased length of stay (LOS), hospital costs, and mortality in teaching vs non-teaching hospitals. 8 Although these inequities in surgical outcomes have been broadly described throughout the spine literature, no studies have explored the relationship of both patient socioeconomic factors and hospital characteristics on postoperative outcomes in lumbar fusions. To address this paucity, the present study evaluates 30-day complication and readmission rates as a function of patient median income, insurance type, and hospital type in patients undergoing lumbar spine fusions.
Methods
A retrospective cohort analysis was performed using the Healthcare Cost and Utilization Project (HCUP) Nationwide Readmission Database (NRD) from 2010-2016. The NRD is an annually published database that provides de-identified information on each patient’s admission including diagnoses, procedures, inpatient demographics, hospitalization characteristics, and readmission data. The present study utilizes NRD discharge weights to allow for nationally representative readmission analysis. All hospital admissions are associated with unique patient linkages which allow for accurate patient tracking through each calendar year.
International Classification of Diseases, Ninth Revision (ICD-9) and Tenth Revision (ICD-10) codes were used to identify relevant information related to patient diagnoses and procedures at both admission and readmission.
Patient Selection and Analysis
ICD-9 and ICD-10 codes were used to identify 596,568 patients who underwent a lumbar fusion at index admission from 2010-2016. Three separate analyses were performed using hospital type, insurance type, and patient income quartile as independent variables. Hospital type included the following groups: metropolitan non-teaching (n = 212,131), metropolitan teaching (n = 364,752), and rural (n = 19,685). Insurance type was divided into 4 cohorts: Medicare (n = 213,534), Medicaid (n = 78,520), private insurance (n = 196,648), and out-of-pocket payers (n = 45,025). Similarly, patient income quartile also included 4 groups. Income quartile classifications were based on each patient’s income relative to the estimated median household income of their corresponding zip code. Patient income quartiles included Quartiles 1 (n = 112,083), 2 (n = 145,755), 3 (n = 156,276), and 4 (n = 147,289), with Quartile 1 corresponding to the poorest populations and Quartile 4 corresponding to the wealthiest populations. Primary outcome measures were 30-day complication and readmission rates. Complications of interest included infection, wound injury, hematoma, neurological injury, thromboembolic event, and hardware failure.
Statistical analysis was conducted using RStudio (Version 1.2.5042). Nonparametric Kruskal-Wallis testing, followed by Dunn’s pairwise comparisons were used to analyze differences in 30-day complication and readmission rates between cohorts. All statistical tests were two-sided with significance level set at α = .05. This study did not require Institutional review board (IRB) approval as patient data within the NRD is de-identified.
Results
Hospital Type
30-Day Complication and Readmission Rates by Hospital Type.
Insurance Type
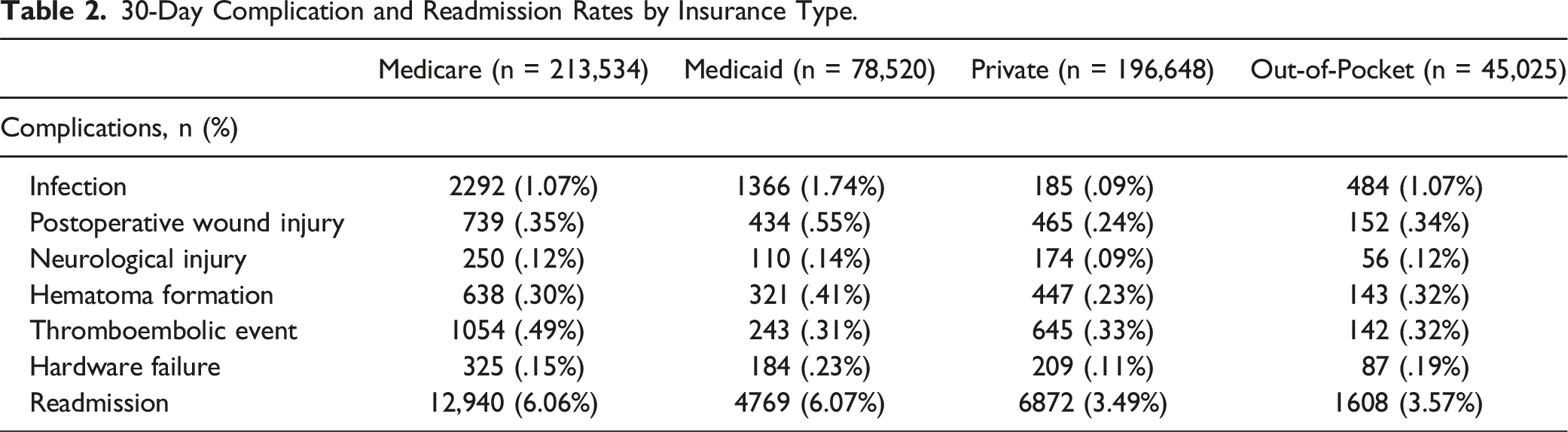
Privately insured patients experienced the lowest rates of complications across all complications of interest with the exception of thromboembolic events. Patients with private insurance experienced significantly lower rates of infection (.09% vs 1.07%), hematoma formation (.23% vs .30%), and thromboembolic events (.33% vs .49%) compared to Medicare beneficiaries (all P < .05). The private insurance cohort also demonstrated significantly reduced risk of infection (.09% vs 1.74%) and postoperative wound injury (.24% vs .55%) relative to Medicaid patients (all P < .001). When comparing privately insured patients with out-of-pocket payers, private insurance status was associated with significantly lower risk of infection (.09% vs 1.07%), postoperative wound injury (.24% vs .34%), hematoma formation (.23% vs .32%), and hardware failure (.11% vs .19%) at 30 days (all P < .01). Patients with private insurance (3.49%) were also significantly less likely to be readmitted compared to Medicare (6.06%) or Medicaid beneficiaries (6.07%) at 30-days (all P < .001).
30-Day Complication and Readmission Rates by Insurance Type.
Income Quartile
30-Day Complication and Readmission Rates by Income Quartile.
Discussion
Regarding hospital type, our results revealed that admission to metropolitan teaching hospitals for a lumbar spine fusion was consistently associated with higher rates of 30-day complications and readmission when compared to metropolitan non-teaching and rural hospitals. These findings are well-aligned with the literature, which has previously found admission to teaching hospitals to be associated with increased postoperative complication rates across various surgical specialties.9-11 This persistent finding, however, is likely attributable to the increased volume and magnitude of complex cases encountered at teaching hospitals, which often function as tertiary referral centers, rather than teaching status alone; several studies have confirmed the association between greater case complexity and admission to a teaching hospital.12-14 In the context of spine surgery, Fineberg et al. found a significantly greater number of multilevel fusions and increased use of posterior approaches, in teaching hospitals compared to their non-teaching counterparts when analyzing postoperative outcomes following cervical spine surgery. The increased risk of complications associated with these operative characteristics have been well-described and are likely responsible for increased complication rates observed in teaching hospitals. 8
Our study also found significant differences in complication rates across patient insurance types whereby privately insured patients were notably less likely to experience postoperative complications or readmission. These findings have been reaffirmed in numerous studies comparing postoperative outcomes in spine surgery patients who were either privately or publicly insured (Medicare or Medicaid).15-18 In a study evaluating insurance type and outcomes following surgery for spinal metastases, Dasenbrock et al initially observed significantly greater odds for in-hospital mortality and complications with Medicaid patients compared to privately insured patients on univariate analysis; but upon controlling for acuity of presentation at admission, mortality and postoperative complication rates were no longer different across groups. 19 Veltre et al. also found markedly higher complication rates following primary total hip arthroplasty (THA) in a matched cohort analysis of Medicare patients vs privately insured patients. 20 Disparities in outcomes between patients with government-sponsored insurance and private insurance are likely a consequence of SES differences or health inequities that were already present prior to admission.21,22
Finally, our study found significantly increased rates of hematoma formation, thromboembolic events, and hardware failure within 30 days in patients belonging to income quartile 4. These findings are in contrast to observations of previous studies, which have reported poorer surgical outcomes and increased mortality rates amongst low income patients.23,24 Although the results of the present study contradict the widely accepted notion that lower income patients generally fare worse, this understanding has been established largely on the premise of using insurance status as a proxy for patient income and SES.25,26 Patients who are uninsured, however, are disproportionately and predominantly low-income, which is represented by the lower income quartile groups in our study (i.e. Quartile 1, Quartile 2). 27 Bearing this in mind, paradoxically reduced readmission rates have been observed in uninsured patients across various contexts.28,29 Uninsured patients have significantly reduced access to care, consequent to limited health literacy, lack of confidence in receiving care, and high financial burden, leading them to often forgo appropriate care.30,31 The described phenomenon of low-income patients under-utilizing health resources is well-documented across many medical disciplines — as shown by Dickman et al, access to care remains a challenge in low-income populations as many patients continue to be uninsured despite implementation of the Affordable Care Act (ACA) in 2010. 32 In a well-cited study, Devoe et al. further established persistent barriers to care even amongst low SES patients who are insured. 33 Interestingly, other investigations have found that uninsured patients were significantly less likely to be readmitted while low-income patients were conversely more likely; the authors, however, interestingly reported that these discrepancies were specifically within the context of longer follow-up periods. 34 This phenomenon may explain why patients belonging to lower income quartiles in our study demonstrated lower rates of readmission for hematoma formation, thromboembolic events, or hardware failure within the short-term, 30-day postoperative period compared to patients belonging to income quartile 4.
Limitations
The present study has several limitations. Use of the NRD inherently confines our analysis to the binary nature of ICD-9 and ICD-10 coding. Consequently, our analysis is unable to characterize the severity of any given complication beyond its occurrence or nonoccurrence. Further, these nonspecific ICD codes preclude the current study from including more granular data elements in analysis of readmission and complication rates, including patients’ preoperative status, case complexity, and surgeon expertise. Additionally, our analysis did not control for demographic variables that may have been different across cohorts. In doing this, however, we sought to increase the extrapolability of our findings and the study’s external validity by including patient characteristics that are representative of their respective cohorts. For example, one of the principal eligibility criteria for Medicare is that patients are aged 65 or older, whereby 84.49% of Medicare enrollees were found to be age 65 or older from 2011-2016, 35 inevitably resulting in a higher mean age for this cohort. The objective of this study was to analyze disparities across patient demographics associated with different hospital types, insurance types, and income quartiles, rather than the single variable itself, to capture the complex interplay of socioeconomic and environmental factors associated with each group.
Conclusions
In summary, admission to a metropolitan teaching hospital for patients undergoing lumbar spine fusions was associated with increased rates of short-term postoperative complications compared to metropolitan non-teaching and rural hospitals. This finding is most likely attributable to the fact that teaching hospitals also commonly function as tertiary referral centers, and therefore receive higher complexity cases. Patient outcomes were also found to differ with varying insurance types, where patients who were privately insured were significantly less likely to experience postoperative complications or readmission than beneficiaries of government-subsidized insurance such as Medicare or Medicaid. These differences may be largely owed to pre-existing health inequities or socioeconomic disparities that ultimately lead to more advanced, complex disease presentation at admission; these cases have a significantly greater predisposition toward suboptimal surgical outcomes. Lastly, patients belonging to the highest income group, Quartile 4, paradoxically demonstrated higher rates of short-term postoperative complications relative to patients in lower income groups. While seemingly contradictory, these findings, however, can be explained by the disproportionally high prevalence of uninsured patients amongst lower income groups, in that uninsured patients are significantly less likely to utilize healthcare resources due to limited health literacy, inadequate care accessibility, and financial instability. Future studies should aim to identify specific socioeconomic factors responsible for fostering disparate, suboptimal outcomes and to define the magnitude of their negative impact on patient outcomes across different insurance types and income classes. Further understanding of how disparities in outcomes may arise from varying hospital types to differing demographic characteristics associated with various insurance types or income groups is essential in mitigating the factors that drive inequitable outcomes in patients undergoing lumbar spine.
Footnotes
Author’s Note
Matthew Chen, Andy Ton, Shane Shahrestani, Xiao Chen, Alexander Ballatori, have nothing to disclose. Jeffrey C. Wang has received intellectual property royalties from Zimmer Biomet, NovApproach, SeaSpine, and DePuy Synthes. Zorica Buser: Grants/ Research support: AO Spine (Paid directly to institution/employer); Nexus Spine (Paid directly to institution/employer), Medical Metrics (Paid directly to institution/employer); MiMedx (past, Paid directly to institution/employer), SBIR NIH (past, Paid directly to institution/employer); Medical Metrics (past, Paid directly to institution/employer); Next Science (past, Paid directly to institution/employer); Consultancy: Next Science (paid directly to institution/employer); Scientific Advisory Board: Medtronic, Medical Metrics, DePuy Synthes; Trips/Travel: AO Spine (Travel Expense Reimbursement, travel reimbursements for AO Spine Knowledge forum meetings and congresses), NASS (Travel Expense Reimbursement); Board of Directors: LSRS (Nonfinancial, Co-chair Program Committee); Committees: AO Spine Knowledge Forum Degenerative (Steering Committee Member); North American Spine Society: Research Project Management Committee (Vice chair), Section on Biologics & Basic Research (Co-chair), The Spine Journal Peer Reviewers (Committee member). Patents (issued): Biomarkers for painful intervertebral discs and methods of use thereof Institutional review board (IRB) approval was not required as no patient information was collected for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.