
Abstract
Study Design
Retrospective study.
Objective
To investigate the characteristics of newly developing Modic changes following discectomy and their impact on residual low back pain (LBP) in the early postoperative stage of lumbar disc herniation.
Methods
We included 96 patients who underwent microscopic discectomy. Through MRI, we assessed new developments of Modic changes and the progression of disc degeneration at the surgical level. The presence of cartilaginous endplates was evaluated using resected specimens, and the main outcome was assessed using the visual analog scale (VAS). Further, the prevalence and time course of Modic changes, and their effects on clinical outcomes in the early postoperative period were examined.
Results
A new development of Modic changes was detected in 28% of cartilaginous herniations at 6 months. Modic changes were observed more frequently in patients with cartilaginous herniation than in those without cartilaginous herniation postoperatively (P < .001). The VAS scores for LBP up to 6 months were greater in patients with Modic changes (P < .001) than those without; however, no significant differences were identified in the presence or absence of Modic changes over the year follow-up. The development of Modic changes was closely associated with residual LBP at 6 months (β:0.511, P < .001).
Conclusions
Modic changes develop predominantly in patients with avulsion-type herniation than in those with annular rupture at an earlier phase after discectomy. Furthermore, disc herniation with cartilaginous endplates may be associated with a slower decrease in LBP for up to 6 months, supporting the notion that newly developing endplate changes may cause residual LBP.
Introduction
Lumbar disc herniation is a risk factor for the development of endplate changes, which are known as Modic changes on magnetic resonance image (MRI). 1 These changes are characterized into 3 types and indicate different stages of the same pathologic process. Type 1 changes that are inflammatory phase progress to type 2 and type 3 changes over time, which constitute the degenerative phase. A new development of endplate changes following discectomy at the operated level has been described with varying prevalence from approximately 6-35%.2-6 Although histological characteristics of lumbar disc herniation have been described as the variable composition, research of anatomical failure sites in disc herniation indicated that endplate junction failure was more common than annulus fibrosus rupture. 7 Cartilaginous herniation, which may arise from the vertebral bone rupture, causes the failure of the endplate structure leading to an increase in the permeability of the endplate. 8 Consequently, the defect of the cartilaginous endplate from the vertebral body may facilitate the movement of biological agents from the disc to the vertebral body, resulting in a high prevalence of Modic changes. Furthermore, an avulsion-type herniation may cause Modic change development in the early postoperative period and endplate changes to a greater extent.
Patients with lumbar disc herniation usually undergo discectomy if they fail to respond to conservative treatment. Moreover, the outcomes of this procedure are good for lower back and radicular pain.9,10 Discectomy provides the most immediate relief from leg pain; however, it is challenging to predict improvement in low back pain (LBP) after surgery. Modic changes are reported to be associated with LBP, particularly type 1 changes.11,12 A few previous studies demonstrated that patients with Modic changes showed higher expression of proinflammatory cytokines, which are known mediators of the peripheral inflammatory response, possibly resulting in LBP.13,14 Furthermore, studies indicate that Modic changes are associated with spinal instability and hypermobility.15,16 Therefore, the presence of Modic changes at baseline and/or the appearance of new Modic changes following discectomy may affect the improvement of postoperative LBP in patients with lumbar disc herniation. However, previous studies have concluded that patients with or without Modic changes showed similar recovery of LBP score following discectomy at 1 year or more.2-5,17-19 The short-term period results indicated that the clinical outcomes of the preoperative presence of Modic changes exhibited less improvement compared with no presence of Modic changes postoperatively at 6 months. 20 Conversely, preoperative presence and/or postoperative persistence of Modic changes did not affect back pain assessed by visual analog scale (VAS) in the early postoperative period.20,21 Thus, the effect of Modic changes on lumbar disc herniation following discectomy remains controversial. This is because previous studies investigated patients with heterogeneous conditions, including both the presence of Modic changes preoperatively and newly developing Modic changes following discectomy and advanced disc degeneration. However, the characteristics of newly developed Modic changes in the lumbar disc herniation with or without cartilaginous endplate avulsion, its time course, and the association between endplate changes and clinical symptoms in the early period have not been investigated. Moreover, this information may be useful for predicting the postoperative clinical course of patients with lumbar disc herniation in an earlier postoperative phase.
This present novel study investigates the prevalence and time course of newly developing Modic changes focused on the anatomical failure of the disc and evaluates whether the new development of Modic changes affects the residual of LBP at an early postoperative period in patients with lumbar disc herniation.
Materials and Methods
Patient Population
This observational and retrospective study enrolled 111 patients who were surgically treated by single-level microscopic discectomy between January 2013 and December 2018; the period in which consecutive surgical samples were available. The inclusion criteria were lumbar disc herniation on MRI with corresponding radicular pain, failure of conservative treatment for 6 weeks or more, no spinal instability as assessed on functional radiographs, and a minimum 1-year follow-up following discectomy. Additionally, to reduce the effects of degenerative factors that can cause LBP following discectomy, patients without Modic changes, patients without severely degenerated intervertebral discs that were classified as grade ≤4 using the Pfirrmann grade system, 22 and patients <60 years of age at initial evaluation were included. The exclusion criteria were coexisting lumbar spinal canal stenosis, history of lumbar surgery, cauda equina syndrome, and insufficient collection of tissue samples. Eight patients were 60 years or older, 1 had concomitant lumbar spinal canal stenosis, 1 had a history of lumbar surgery, 1 had cauda equina syndrome, 2 had insufficient surgical specimens, and 2 were lost to follow-up. Consequently, 96 patients were included in this study.
The study was approved by the institutional review board at the Kyushu University Hospital (approval number: 30-225). The informed written consent was received from all patients.
Surgical Procedure and Histological Study
All surgeries were performed using the standard unilateral interlaminar fenestration technique by the same surgeon. If necessary, the procedure was combined with minimal exposure laminotomy. Although intraoperative dural tear was observed in 1 case, this complication did not affect postoperative outcomes. All the epidural and submembranous tissues of the extruded discs were excised. However, the intradiscal space was observed, and loose parts of the disc were resected.
Radiographic and MRI Assessment
To evaluate segmental instability at the operative level after discectomy, the posterior disc angle in the flexion position was measured at the final follow-up. The posterior disc angle at flexion was defined as lordosis (+) or kyphosis (−). Translation was measured using lateral flexion and extension radiographs. MRI was performed using a 1.5 Tesla scanner (Magnetom Symphony, Siemens Health care) at baseline, 6 months postoperatively, and at the final follow-up. We examined sagittal and axial T1-weighted spin-echo images (TR/TE, 540/12) and sagittal and axial T2-weighted fast spin-echo images (TR/TE, 2300/120) of each patient. The acquisition matrix was 320 × 224 mm for T1-weighted images and 330 × 280 mm for T2-weighted images. The slice width was 4 mm, and the interslice gap was 1 mm for both the sagittal and axial slices. The inversion recovery time for the T1-weighted images was 660 ms, and the number of excitations for both T1- and T2-weighted images was 4. All MRI analyses were conducted independently by 2 orthopedic surgeons (K.K. and G.K.) who were blinded to the clinical data of the patients. Modic change at the operated level was assessed based on Modic classification which was divided into 6 groups; type 0, type 1, type 2, type 3, and mixed type 1/2 and 2/3. 23 In addition, we quantified the extent of horizontal location of Modic changes as ≤33%, 34%–66%, and >66% of the anteroposterior, which was partially modified from previous reports. 24 Furthermore, the depth of Modic changes was assessed as the ratio of the largest cranio-caudal extension of endplate abnormalities to the vertebral height and classified into 4 types as follows: endplate only, ≤25%, 26%-50%, and >50%. 24 When an intensity change occurred on both sides, the larger cranial or caudal extent was used for further evaluation. Disc degeneration was assessed using the Pfirrmann grading system and divided into 2 groups based on whether disc degeneration had progressed to 1 or more grades.
Histological Analysis
The surgical specimens were fixed in a 10% formaldehyde and embedded in paraffin. The materials were cut into 4 μm thick slices with a microtome and stained with hematoxylin and eosin. A minimum of 5 consecutive sections with the largest cross-sectional areas were evaluated for each specimen. Two pathologists, who were blinded to the study participants, examined the specimens and reported the histological findings. They assessed the presence of a cartilaginous endplate in the herniated samples. The following criteria were used to discriminate between the cartilaginous endplate and other tissues. The structure observed in the specimens was composed of hyaline cartilage with an amorphous matrix and chondrocyte-like cells exhibiting a clearly visible perinuclear halo.
Clinical Outcomes
The severity of LBP and leg pain was evaluated using the VAS scores ranging from 0-100 at baseline, 6 weeks, 3 months, 6 months, and at the final follow-up. Additionally, we assessed health-related quality of life outcomes using the Rolland–Morris Disability Questionnaire (RDQ) preoperatively, 6 months postoperatively, and at the final follow-up. Furthermore, neurological status was evaluated using the Japanese Orthopaedic Association (JOA) lumbar score at 3 time points.
Statistical Analyses
Descriptive data are presented as mean with standard deviation or frequencies (%). The significance of differences between the groups was statistically analyzed using the unpaired t test, Mann–Whitney U test, and Chi-square test. A paired t test was used to examine the differences in clinical outcomes at follow-up points after discectomy in relation to the presence or absence of Modic changes. Multiple linear regression analysis was employed to determine the factors associated with residual LBP at 6 months after discectomy, controlling for age, sex, preoperative VAS score for LBP, newly developing Modic changes, progression of disc degeneration, and the presence of a cartilaginous endplate. The level of significance was set at P < .05.
Statistical analyses were performed using JMP software (version 15; SAS Institute, Cary, NC, USA). Intra- and interobserver reliability were assessed using Cohen’s kappa for nominal variables (type of Modic changes) and Cohen's weighted kappa for ordinal variables (width and depth of Modic changes and disc degeneration). The kappa values are interpreted as follows: 0-.20, poor; .21-.40, fair; .41-.60, moderate; .61-.80, good; .81-1.00, very good. 25
Results
Preoperative Patient’s Characteristics
Preoperative Characteristics in 96 Patients with Lumbar Disc Herniation.
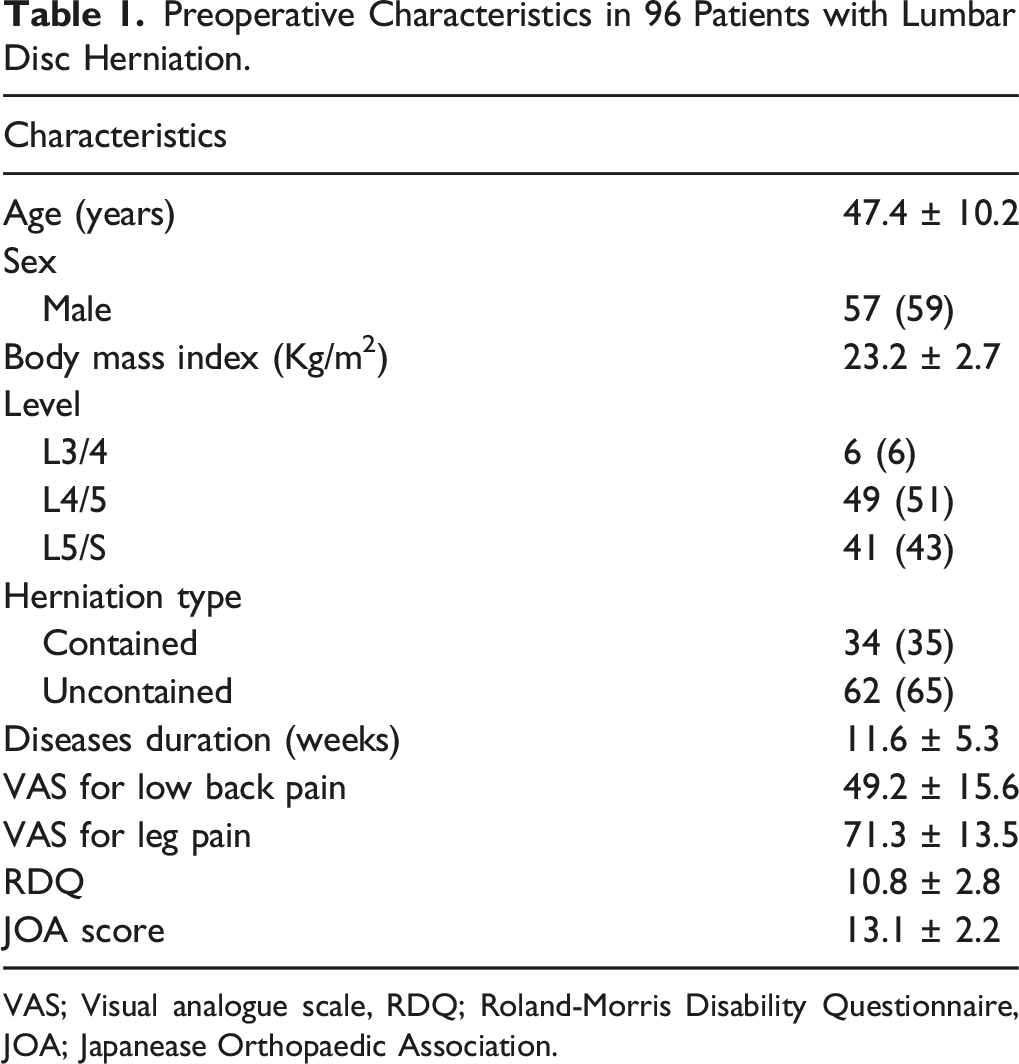
VAS; Visual analogue scale, RDQ; Roland-Morris Disability Questionnaire, JOA; Japanease Orthopaedic Association.
Reliability of MRI Assessment and Time Course of Modic Changes and Disc Degeneration
The intra-observer reliability for the type of Modic changes was considered as good with kappa values of .8. Regarding the depth and width of Modic changes, kappa values ranged from .66-.86 and .62-.76, respectively. The inter-observer reliability for the type was considered as good with kappa values of .74. For depth and width, kappa values ranged from .64-.8 and .62-.76, respectively. The reliability of the disc degeneration assessment was good, with a mean intra-observer kappa value of .74 and an inter-observer kappa value of .66.
Time Course of New Developing Modic Changes and the Progression of Disc Degeneration.
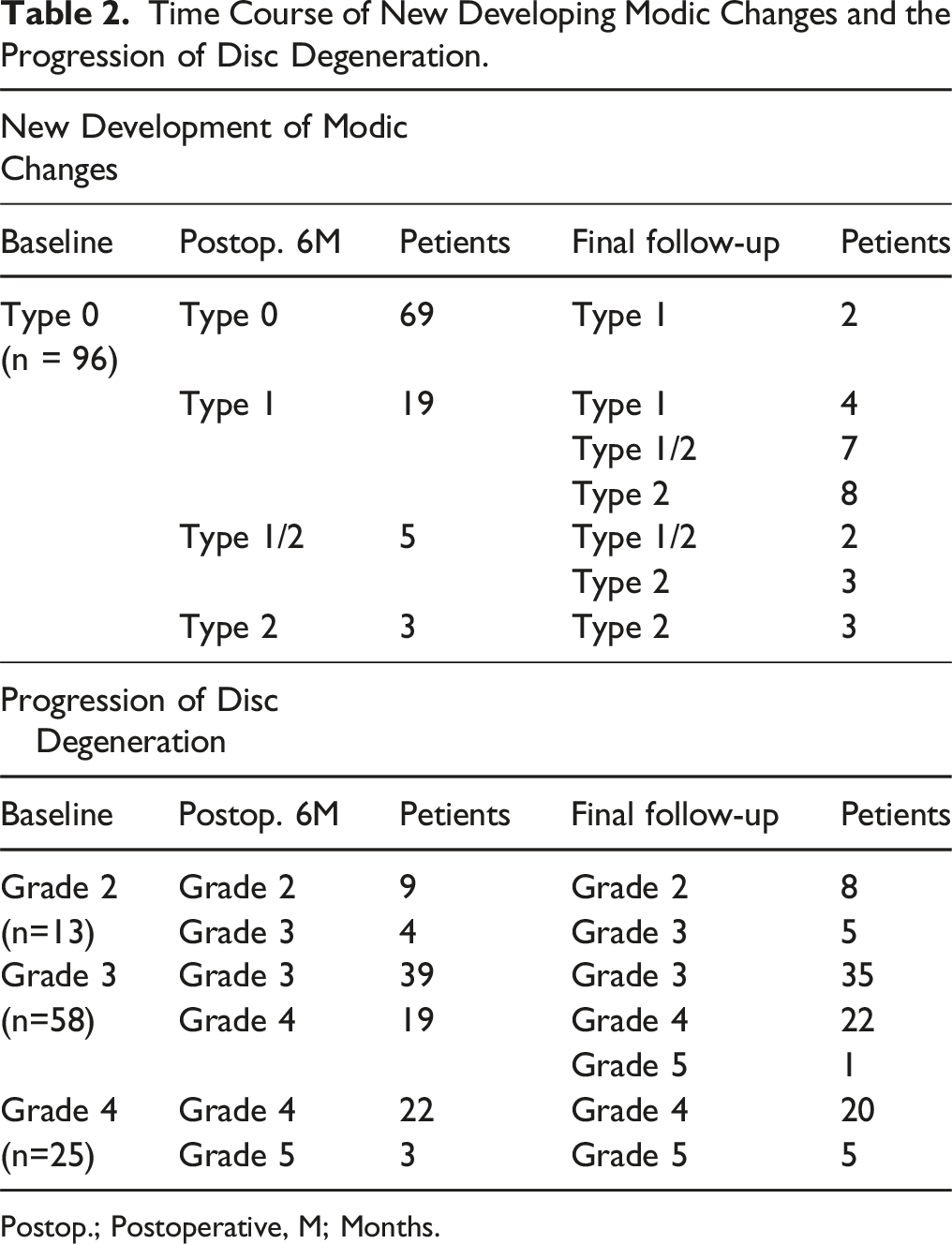
Postop.; Postoperative, M; Months.
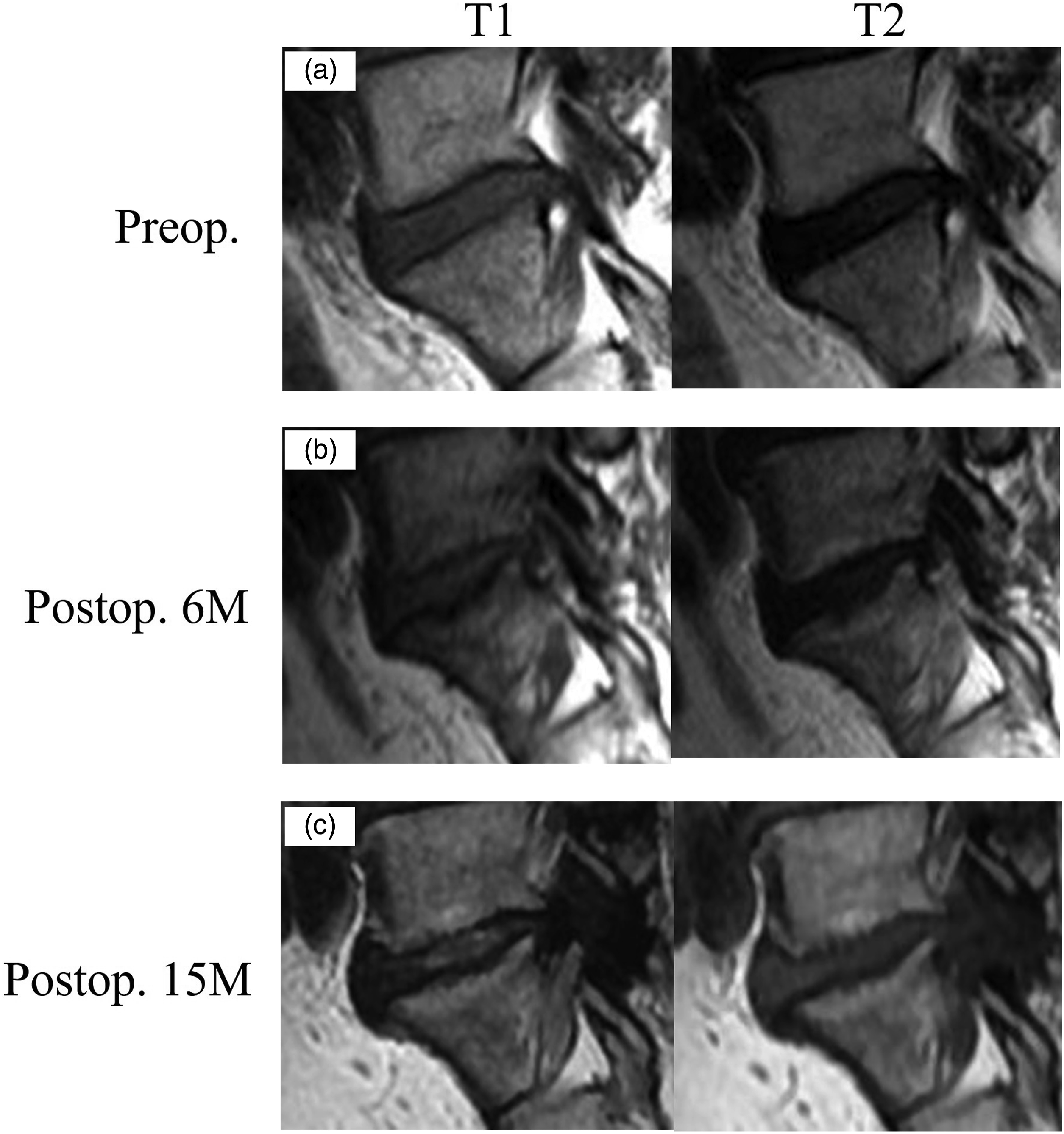
A 42-year-old man with L5/S disc herniation. (a) There are no Modic changes on the adjacent endplate of herniated level preoperatively. Microendscopic discectomy is performed, and cartilaginous endplate is observed in the resected disc (b) Modic type 1/2 changes are recognized in upper and lower endplates at postoperative 6 months. (c) Modic changes converted to type 2 at 15 months following discectomy. Preop., preoperative; postop., postoperative; M, months.
The Association of New Development of Modic Changes with Demographic and Imaging Data
Association of New Developing Modic Changes With Demographic and Imaging Findings.
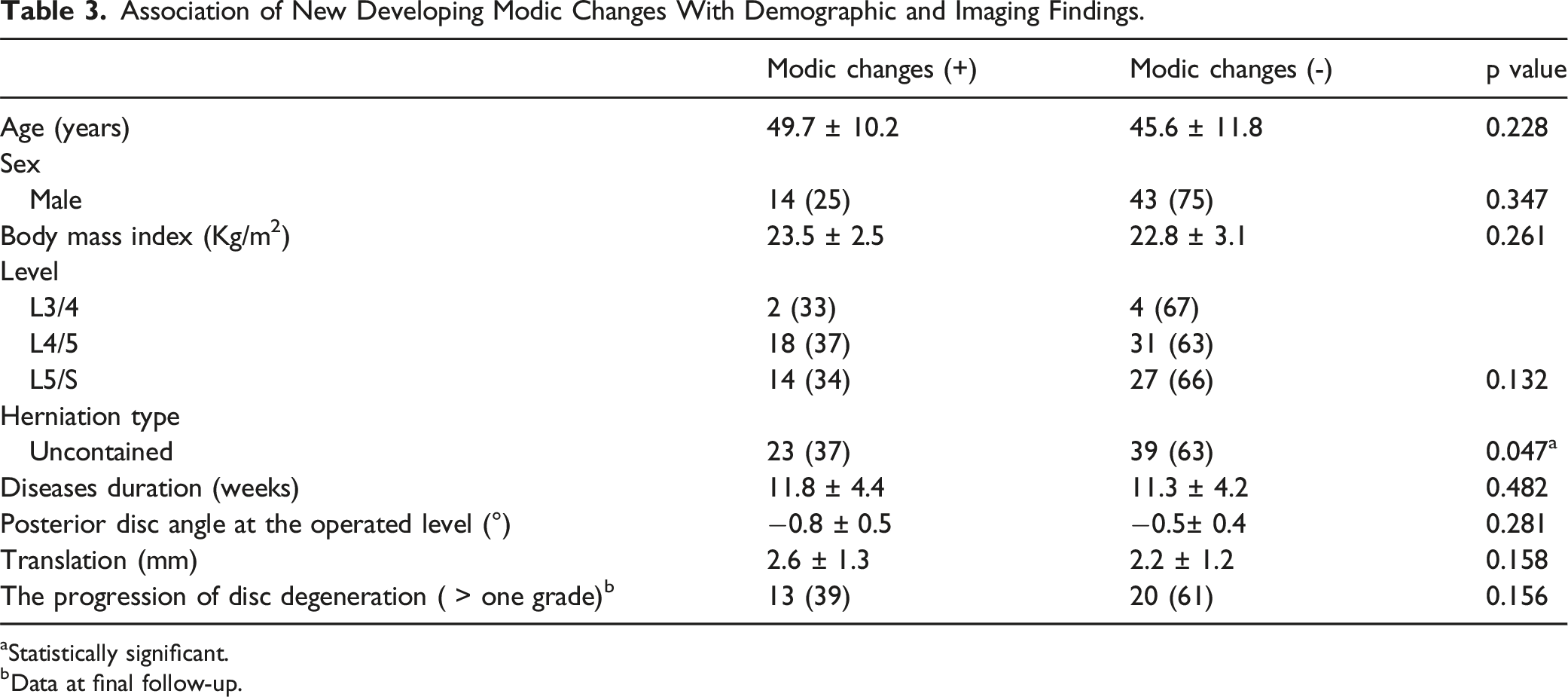
aStatistically significant.
bData at final follow-up.
The Prevalence of Cartilaginous Herniation and Their Association with MRI Findings
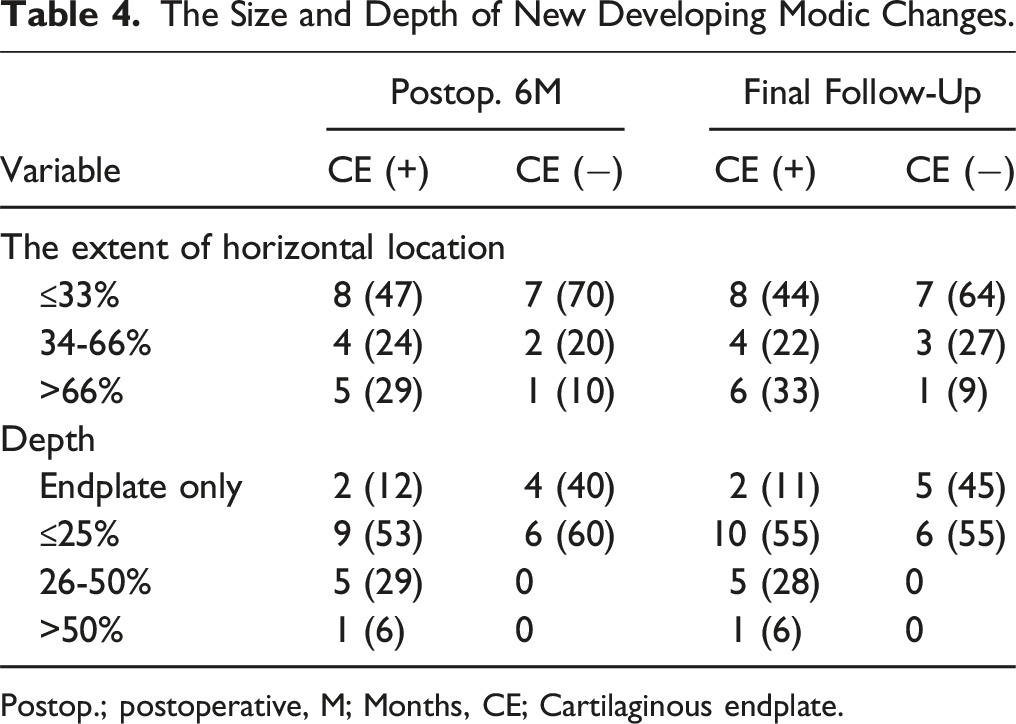
The presence of cartilaginous endplate in herniated specimens was observed in 33 (34%) of 96 patients. There was a significant association between cartilaginous herniation and new development of Modic changes at both postoperative 6 months (P < .001) and the final follow-up (P < .001) (Figure 2). Patients with cartilaginous endplate at both follow-up period showed a tendency for Modic changes with the depth >25% (Table 4). There was no significant association between cartilaginous herniation and the progression of disc degeneration. The association between the percentage containing cartilaginous endplate and new development of Modic changes (a) or the progression of disc degeneration (b) in the operated level. (a) Patients with cartilaginous herniation have a higher prevalence of newly developing Modic changes compared with those without cartilaginous herniation. (b) There is no association between cartilaginous herniation and the progression of disc degeneration. Postop., postoperative; M, months; FU, follow-up. The Size and Depth of New Developing Modic Changes. Postop.; postoperative, M; Months, CE; Cartilaginous endplate.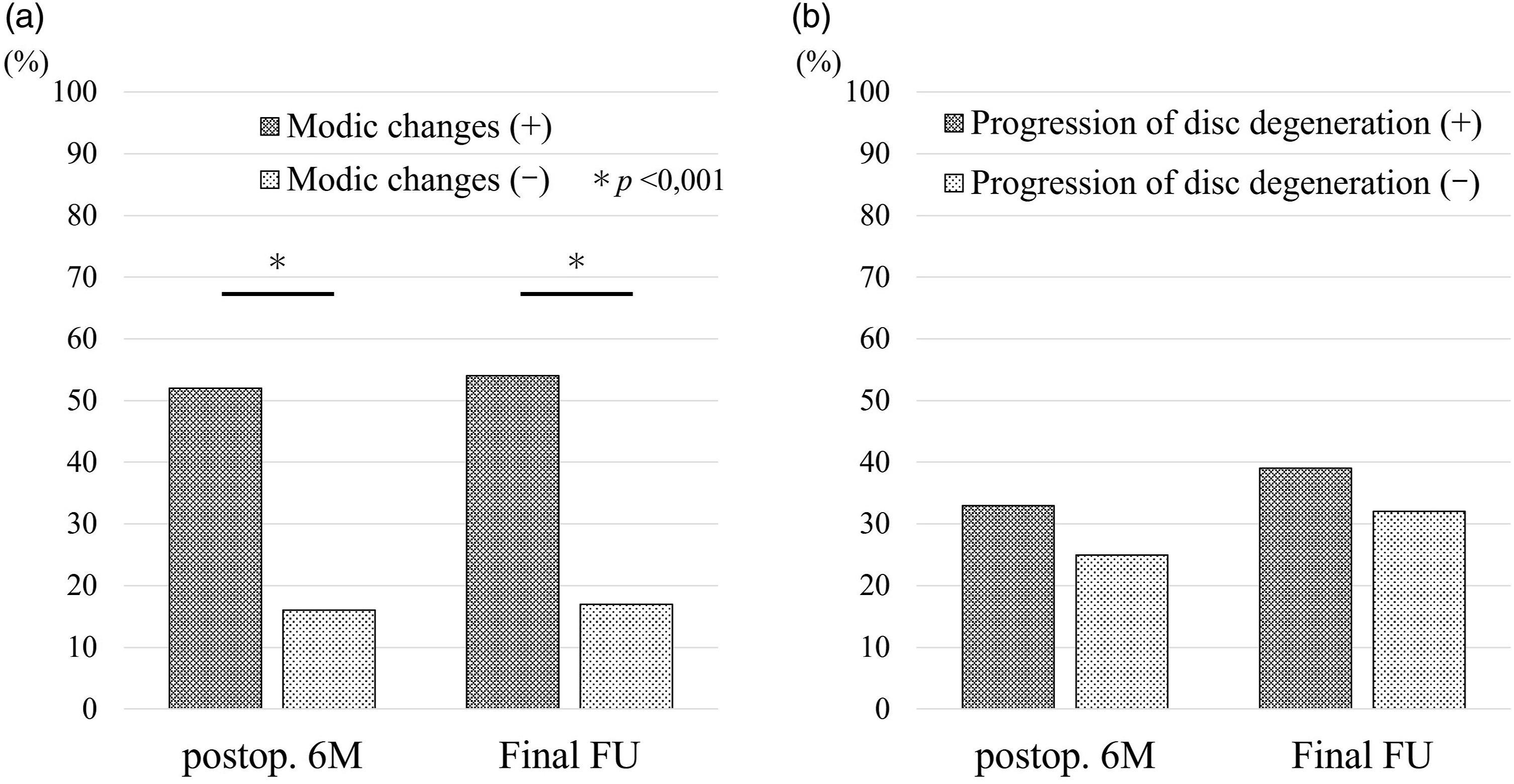
Influence of New Developing Modic Changes on Clinical Outcomes
The VAS scores for LBP at 6 weeks, 3 months, and 6 months were higher in patients with disc herniation with Modic changes than in those without Modic changes (P < .001, P < .001, P < .001, respectively); however, no differences were observed at the final follow-up (Figure 3a). The newly developed Modic changes had no significant effect on the VAS score for leg pain throughout the follow-up period (Figure 3b). Neither the RDQ nor the JOA scores were associated with the development of Modic changes at any time point (Figure 3c and d). VAS scores for low back pain (a) and leg pain (b) at baseline, 6 weeks, 3 and 6 months, and final follow-up, and RDQ (c) and JOA score (d) at baseline, 6 months, and final follow-up. Patients with new development of Modic changes have a higher VAS score for low back pain compared with those without Modic changes at 6 weeks (P < .001), 3 months (P < .001), and 6 months (P < .001), however, no differences are recognized at final follow-up. VAS for leg pain, RDQ, and JOA scores have no association with the presence or absence of Modic changes at any time point VAS, visual analog scale; RDQ, Roland–Morris Disability Questionnaire; JOA, Japanese Orthopaedic Association; preop., preoperative; W, weeks; M, months; FU, follow-up.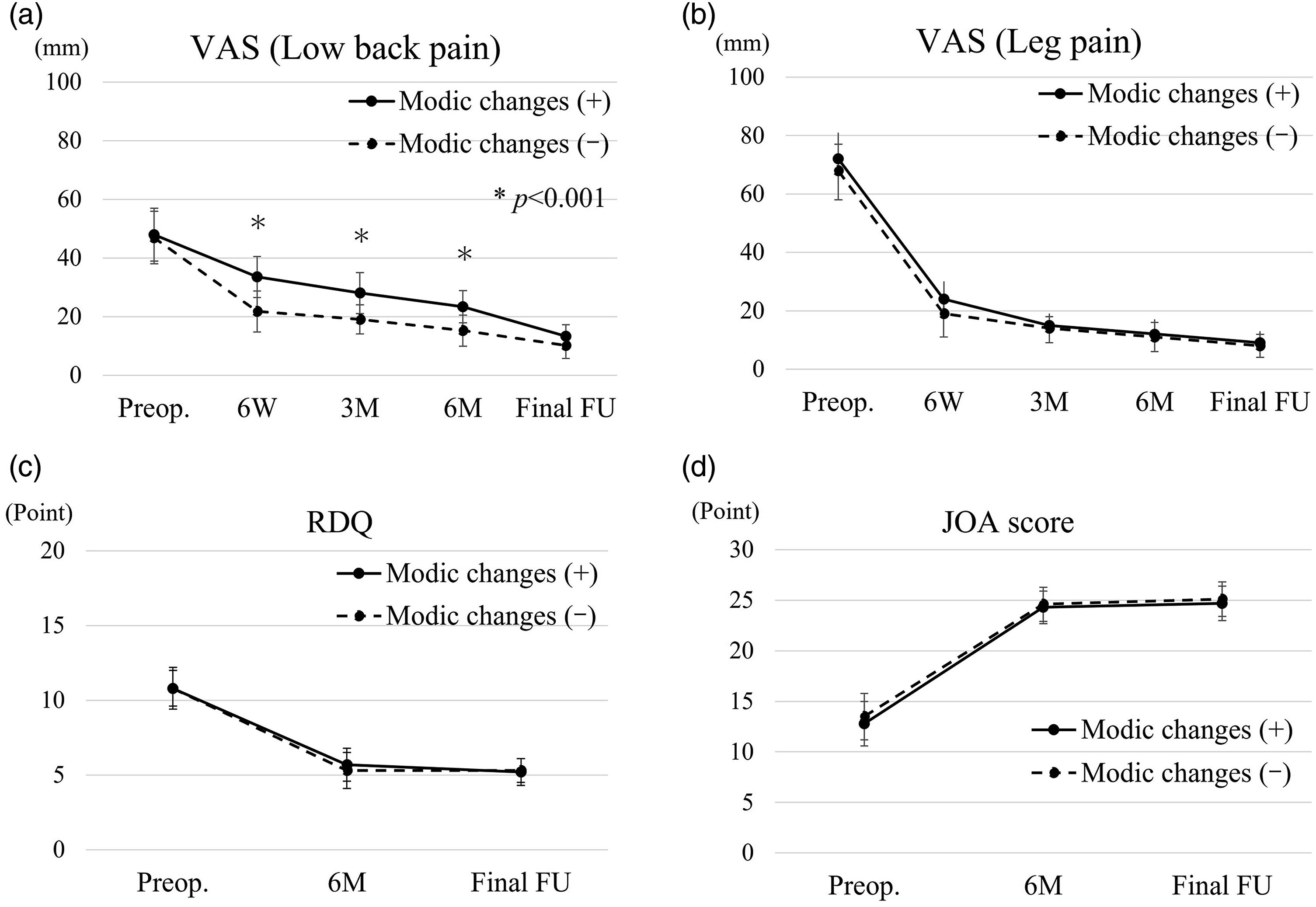
Multiple linear Regression Analysis Between the Variables and Residual Low Back Pain at Postoperative 6 Months.
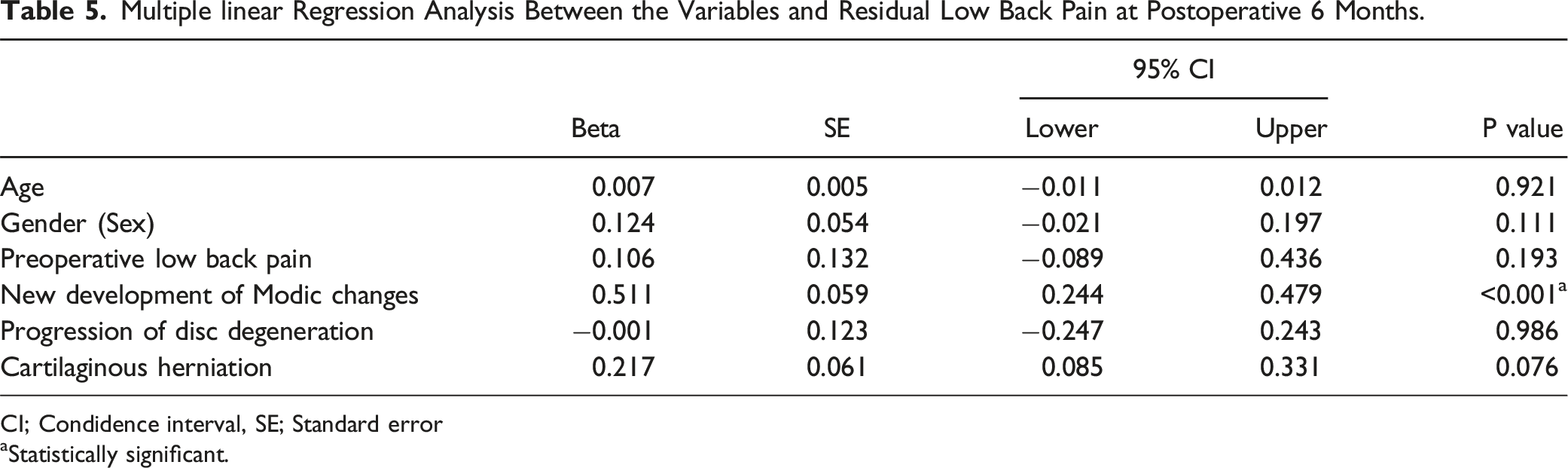
CI; Condidence interval, SE; Standard error
aStatistically significant.
Discussion
The principal aim of this study was to identify the characteristics of newly developed Modic changes postoperatively in lumbar disc herniation with or without endplate avulsion and assess the possible association between newly developed Modic changes and clinical symptoms in the early postoperative period. Our main results revealed that newly developed Modic changes had a higher occurrence in patients with cartilaginous endplates than in those without cartilaginous endplates. Additionally, a majority of them developed at an earlier stage following discectomy. Furthermore, the new occurrence of Modic changes was not associated with the clinical outcome at 1 year or more postoperatively; however, patients with Modic changes exhibited a slow recovery of LBP than those without Modic changes for up to 6 months. This indicates that the presence of cartilaginous endplate in a herniated disc may be related to residual LBP in the early postoperative period following discectomy and that the development of new Modic changes can partially explain this finding.
The endplate was identified as a potentially weak region in the disc, which was only loose connection between the cartilaginous endplate and the subchondral bone, thus increasing the risk of failure in this region.26,27 Rajasekaran et al stated that avulsion and rim fractures of the endplate junction were more frequent than annular rupture and proposed that lumbar disc herniation may be the result of endplate failure than annular rapture. 7 The hyaline cartilage endplate limits the movement of metabolites and water between bone marrow and disc. As the cartilaginous endplate is poorly regenerated, its loss causes failure of the effective barrier, resulting in greater migration of biological agents and stimulation of endplate degeneration.8,28 These changes may play a key role in the development of Modic changes, particularly in patients with cartilaginous herniation. Here, patients with disc herniation containing a cartilaginous endplate had a higher prevalence of newly developed Modic changes postoperatively compared with those without a cartilaginous endplate which is consistent with previous reports.29-31
Regarding the timing of the development of endplate changes at the operated level following discectomy, previous reports have demonstrated that these changes occur commonly during a few years postoperatively.4,11 In a previous study, endplate changes developed at the operated level within 6 months, with a 6 to 19% prevalence in patients with lumbar disc herniation. 6 Furthermore, an earlier report indicated that patients with type 1 and type 2 Modic changes increased about 35% within 1 year, 4 indicating that new development of Modic changes may develop frequently within the first 1 year postoperatively. In particular, focusing on the anatomical pattern of a disc failure, disc herniation with vertebral endplate avulsion may develop into Modic changes earlier than those with annulus fibrosus rupture because of extensive damage to the endplate structure as a barrier function. Our results indicated that newly developing Modic changes at the operated level had a greater prevalence in 17 of 33 patients with cartilaginous endplate avulsion (55%) at 6 months postoperatively compared with those without cartilaginous endplate (16%). These results suggest that cartilaginous herniation may be a risk factor for vertebral endplate changes in the early phase following discectomy.
Several studies have demonstrated the effect of Modic changes on the improvement of LBP after lumbar discectomy.2-5,15-21 For short-term outcomes, Chin et al demonstrated less improvement based on the Oswestry Disability Index (ODI) in patients with Modic changes at baseline than those without Modic changes at 6 months. 20 In the evaluation using the VAS for back pain, 2 previous studies indicated no influence of the presence of Modic changes in residual LBP at 6 months.20,21 However, in these studies, there were some heterogeneities, including differences in the timing of development of Modic changes and varying degrees of disc degeneration at baseline. Our study, which minimized this heterogeneity, demonstrated that lumbar disc herniation with newly developed Modic changes had a slow recovery process for LBP up to 6 months postoperatively, and were closely associated with residual LBP at 6 months postoperatively. These may be attributed to the new development of Modic changes as a cause of residual LBP at an earlier postoperative phase, caused by the stimulation of inflammatory cytokines such as interleukin-1β and tumor necrosis factor-α.13,32 Most studies reported that Modic changes were not associated with VAS and ODI scores at 1 year or more follow-up after discectomy, our results were also consistent with previous reports.2-5,17-19 Most Modic type 1 changes commonly convert into type 2 changes over time, that is, unstable inflammatory phase to stable chronic phase of degeneration.1,33 A previous study reported that there was an increased prevalence of Type 2 changes in patients following discectomy compared with those with non-surgical treatment. 34 Considering the time course of Modic changes, the effect of Modic changes on LBP may decrease over time. Early postoperative delayed recovery of LBP in patients with Modic changes is clinically important; if LBP persists in the early phase following discectomy, an evaluation using MRI and careful follow-up of these patients is preferred.
Avulsion-type disc herniation, which has greater fissures in the vertebral endplate, may indicate that inflammation has spread widely into the vertebral bone marrow, leading to severe degeneration of the vertebral endplate. An earlier study demonstrated that the extent of Modic changes after discectomy had a significant association with the severity of LBP and higher ODI. 15 On the contrary, Määttä et al suggested that the size of Modic type 1 changes is not directly associated with the clinical symptoms, however, the type of Modic lesion is more important., 35 the different measurement methods in these studies are considered to be the main reason for this contradictory conclusion and inconsistent results. Our results showed that cartilaginous herniation results in a larger area of Modic changes. No statistical advantage was observed because the patient groups were extremely small for a reliable analysis. Hence, further studies are required to confirm the influence of these factors on LBP intensity.
A previous study demonstrated that translational motion of lumbar segments increased in patients with type 2 Modic changes, whereas angular motion tended to increase in patients with Modic type 1 compared with those having Modic type 2 and type 3. This indicates that a disorder of the endplates may play a crucial role in spinal instability. 36 Similarly, another study supported that Modic type 1 was associated with segmental hypermobility and LBP. 37 In patients with lumbar disc herniation, severe endplate changes after discectomy lead to spinal instability, resulting in postoperative residual LBP.15,16 However, a previous study indicated that patients with Modic changes preoperatively did not show an increase in spinal hypermobility and the occurrence of transitional instability at 1 year following discectomy. 2 In this study, no stability changes after discectomy on postoperative flexion-extension radiography were observed at an average of 18 months postoperatively consistent with previous studies. This is explained by the assessment of patients with disc herniation who were younger, without a severely degenerative spine, and limited to a short follow-up period. Therefore, we believe that the stability and mobility of the spinal segments had little effect on the clinical symptoms in this study.
The current study has a few limitations. First, there were no assessments of other possible anatomical sources of LBP, such as the facet joint and myofascial pain. However, to avoid the influence of degenerative factors that cause LBP, we excluded patients with severe disc degeneration and endplate changes at baseline. Additionally, psychosocial and psychological factors are associated with postoperative clinical outcomes in patients with lumbar disc herniation, 38 however, our study did not include these factors. Second, the minimum follow-up period of 1 year was short for the clinical evaluation of lumbar disc herniation, and the number of patients was small. Third, smaller fragments may have been missed during surgical removal and subsequent histopathological preparation. To minimize variance, herniated fragments were excised using the same surgical procedure and at least 5 consecutive sections of the cross-sectional area were evaluated for each specimen. Finally, we did not investigate the natural course of Modic changes and their influence on clinical symptoms in the conservative treatment group because this study only included patients who underwent surgery. Conservative treatment is an alternative approach for patients with lumbar disc herniation having sciatica symptoms; therefore, examination of this group is important. Hence, further studies with longer follow-up periods, including non-surgical treatment groups, and evaluation of other factors related to LBP should be conducted to confirm our results.
Conclusion
Our results demonstrated that newly developed Modic changes in patients with cartilaginous endplate avulsion indicated a higher prevalence than in those without cartilaginous endplate avulsion in lumbar disc herniation, and also occurred in the early postoperative period. Furthermore, the majority of patients treated by discectomy have a substantial pain reduction by approximately 1 year or more; however, patients with newly developed Modic changes may imply a slower initial decrease in LBP. These results indicate that avulsion-type herniation may be associated with persistent LBP early after discectomy, related to newly developing Modic changes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.