
Abstract
Study Design:
Prospective cohort study.
Objective:
Endplate lesions though have been implicated in the genesis of lumbar disc herniation (LDH), very little is known regarding their clinical course. Thus, the present study is aimed to investigate the incidence and types of endplate failure (EPF) in LDH and its correlation with the clinical symptoms and prognosis.
Methods:
Clinical and magnetic resonance imaging (MRI) features of 66 patients with isolated single level LDH were studied. Three-dimensional fast spoiled gradient (3D FSPGR) MRI and computed tomography scans were used to identify the bony and cartilaginous EPF. Twenty-five patients were operated on and 41 patients were treated conservatively. Changes in the pain score, function and neurology were noted at 3, 6, 12, 24, and 36 weeks.
Results:
Endplate lesions were observed in 64 patients (96.9%), including bony endplate failure (bony failure) in 47 patients (71.2%) and isolated cartilaginous endplate lesions in 17 patients (25.7%). Bony failure group had similar pain and functional scores but more severe neurological deficit at the initial evaluation. Clinical parameters improved in all groups, but the recovery was lesser in conservatively treated bony failure patients.
Conclusion:
Endplate lesions are commonly associated with symptomatic LDH. Presence of bony failure can increase neurological deficit and reduce the chance of recovery with conservative management. The 3D FSPGR sequence of MRI can be successfully used for detection of the endplate lesions in the herniated disc.
Keywords
Introduction
Lumbar disc herniation (LDH) is the most common cause of low back pain affecting 1 to 5 per 1000 population per year. 1 Yet there is hardly any disease, where the opinions vary so widely regarding the pathogenesis and management. 2 –5 The discogenic back pain is multifactorial in origin arising from mechanical compression, neurophysiological changes, ischemia, inflammatory, and/or immunologic mechanisms. 6,7 Previously, the nucleus pulposus was being implicated for most of the symptoms, but now the role of other structures are increasingly being recognized. 2,3,6 –11
Lying between the vertebral body and intervertebral disc, the endplate provides strength and nutrition to the disc. 12 –14 Because of its location between stiff bone and resilient disc, it is the weakest portion of vertebral-disc complex, predisposing it to mechanical failure. 15 It is also the site where structural changes of degeneration are most eveident. 10,16 Though some previous cadaveric studies and one in vivo study have highlighted the role of endplate failure (EPF) in LDH, none of them have described its significance in clinical symptamatology. 6 –9,17 –19 Most of these previous studies used computed tomography (CT) scan to evaluate EPF, which can increase the radiation and cost. 9,20 –24
Initially, Kakitsubata et al 25 used the fat-suppressed 3-dimensional fast spoiled gradient (3D FSPGR) magnetic resonance imaging (MRI) in cadavers to delineate the normal anatomy of cartilage endplate and morphological changes in discovertebral junction. Schmid et al 6 then used marrow signal intensity and vertebral corner defect in MRI to predict the presence of cartilaginous components in the extruded disc. Subsequently, a few authors used ultrashort echo time (UTE) or 3D fast low angle shot (3D FLASH) MRI sequences to study the endplate cartilage. 26 –29
The present study is aimed to evaluate the incidence and pattern of endplate lesions in LDH and their implications in clinical presentation and prognosis. It also aims to evaluate the usefulness of 3D FSPGR MRI sequence to detect the EPF.
Material and Methods
The present study is a prospective cohort series of the patients with single-level LDH presented to the clinic between February 2014 and May 2015. Prior to the study, an approval was taken from the ethics committee of the institute. Patients included in the study were between 20 and 50 years of age, with nerve root tension signs and/or neurological deficit. Exclusion criteria included kyphoscoliosis, previous lumbar spinal surgery, cauda equina syndrome, spinal canal stenosis, multilevel disc prolapse, spondylolisthesis, or spondylodiscitis.
During MRI, additional 3D FSPGR sequence along with the routine T1 and T2 sequences were used to study the status of the endplate (1.5-T Optima GEM MRI, GE Healthcare, Buckinghamshire, UK). Sixty-six patients formed the study group and their MRI evaluations included level, position (central, paramedian, or lateral), and stage of herniations (protrusion, extrusion, or sequestration). Detail status of nucleus pulposus, annulus fibrosus, and endplate were noted and the LDH were classified as per Rajasekaran et al 9 (Table 1). However, unlike the previous study, here the classification was primarily based on MRI features. Additionally, CT scan (16 slice CT scan, GE Healthcare, Buckinghamshire, UK) was also done in 44 cases to study the bony component of the endplate failure. All the radiological assessments were done by the third and fifth authors. Differences regarding the classifications were sorted out by a common consensus.
Rajasekaran Classification of Endplate Junction Failure.
The patients were initialy treated conservatively with analgesics, muscle relaxants and physiotherapy programme. The indications for surgery were presence of neurological deficit, no improvement after 6 weeks of conservative treatment or worsening of the symptoms and deficit. However, as some of the patients had received adequate conservative management elsewhere without much relief, they were considered directly for surgery from the beginning. Discectomy through fenestration was done in all cases except those with massive disc prolapse and severe canal encroachment where laminectomy was considered. After exposure, the protruded discs were observed for any rupture of annulus fibrosus and then the nucleus pulposus was removed with care not to damage the endplates. In extruded and sequestrated discs, only the loose fragments were removed. The herniated materials were then observed, palpated with fingers especially to detect any cartilage or bony pieces and sent for histopathological examinition.
Patients were then followed up at 3, 6, 12, 24, and 36 weeks and improvement of the symptoms were evaluated by changes in neurodeficit, straight leg raising (SLR), visual analogue score (VAS), and Oswestry disability index (ODI). All the data was recorded and analysed by SPSS 21 (IBM Corp, Armonk, NY, USA). Comparision among the groups were done by Mann-Whitney U test and Fisher’s exact test.
Results
A total of 66 patients (50 males and 16 females) with isolated single level LDH were recruited for the study. As per 3D FSPGR sequence, 45 patients had bony endplate failure (bony failure) and were grouped as group 1. CT scan detected bony failure in 2 more patients taking the total number in group 1 to 47 (71.2%). All patients with bony failure had associated cartilaginous component, but then the classification was done on the basis of bony lesions. Out of these, 19 patients had type 1A failure (Figure 1), 14 had type 1B failure (Figure 2), 5 had type 1C failure (Figure 3), and 9 had type 1D failure (Figure 4). The 3D FSPGR sequence was found to have excellent specificity (100%) and sensitivity (92%) for detection of bony failure. In contrast the routine T1- and T2-weighted sequences could detect only 33.3% of bony failures missing most of the type 1A and 1B endplate failure. Nineteen patients (28.8%) had type 2 endplate failure and were grouped as group 2, of which 17 patients had cartilaginous endplate failure (cartilaginous failure) (Figure 5) and 2 patients had only annulus fibrosus tear (Figure 6).
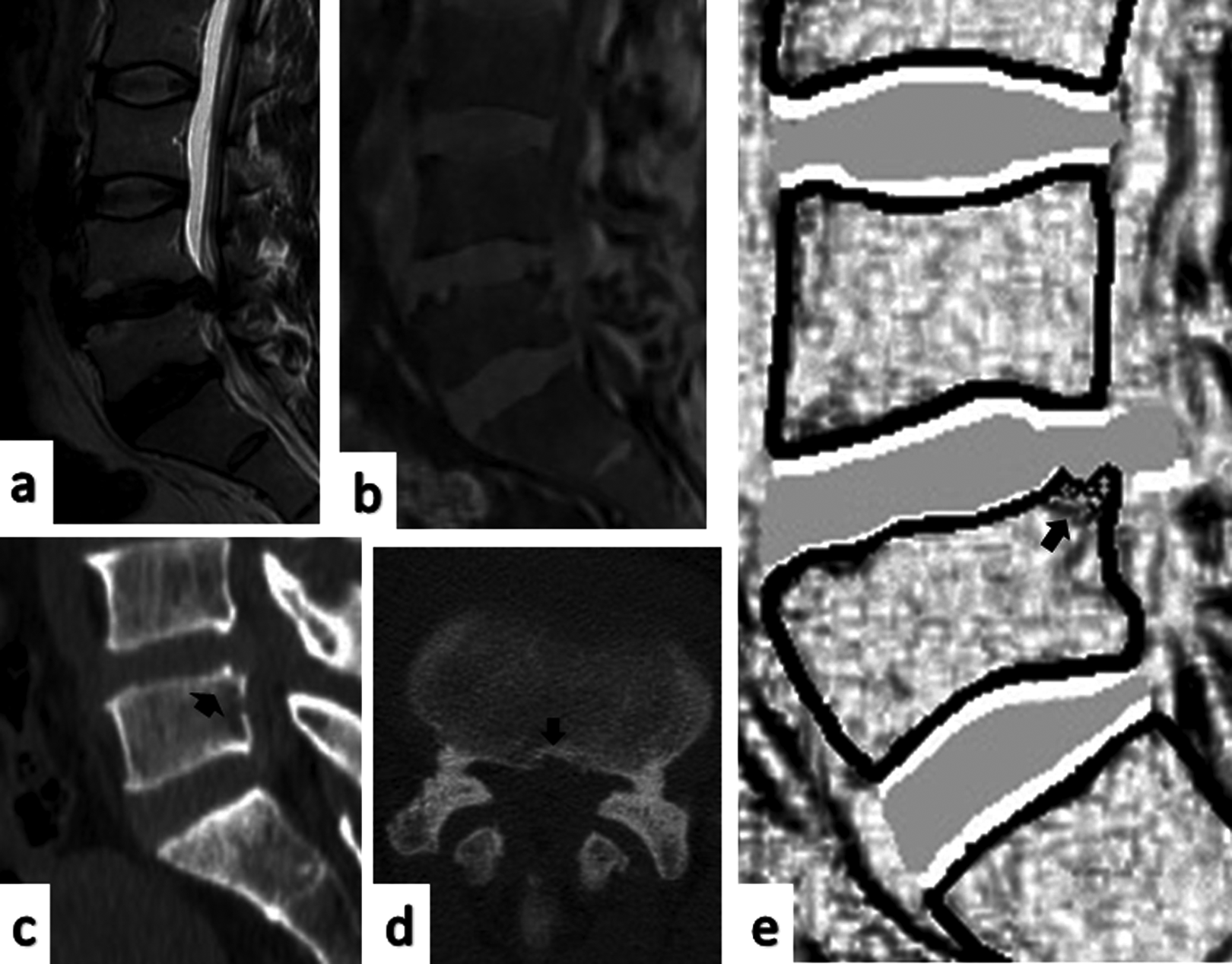
Type 1A herniation: (a) T2 image with L4-5 LDH, (b) 3D FSPGR image, (c, d) CT scan images, (e) sketch of the 3D FSPGR. Black arrow—bony irregularity at posterior superior corner of L5. LDH, lumbar disc herniation; 3D FSPGR, 3-dimensional fast spoiled gradient; CT, computed tomography.
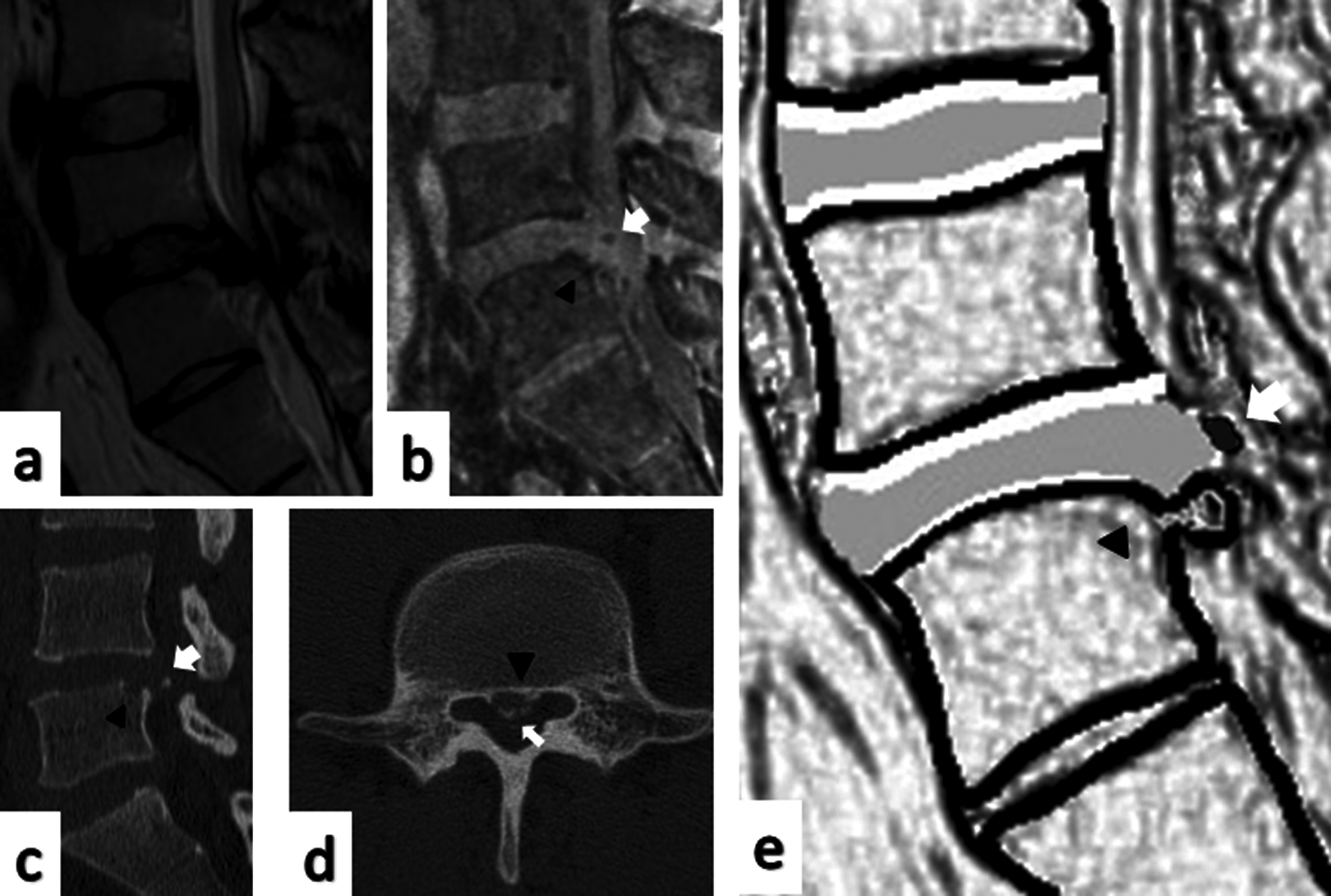
Type 1B herniation: (a) T2 image with L4-5 LDH, (b) 3D FSPGR image, (c, d) CT scan images, (e) sketch of the 3D FSPGR. White arrow—avulsed bony fragment, black arrowhead—site of end plate failure. LDH, lumbar disc herniation; 3D FSPGR, 3-dimensional fast spoiled gradient; CT, computed tomography.
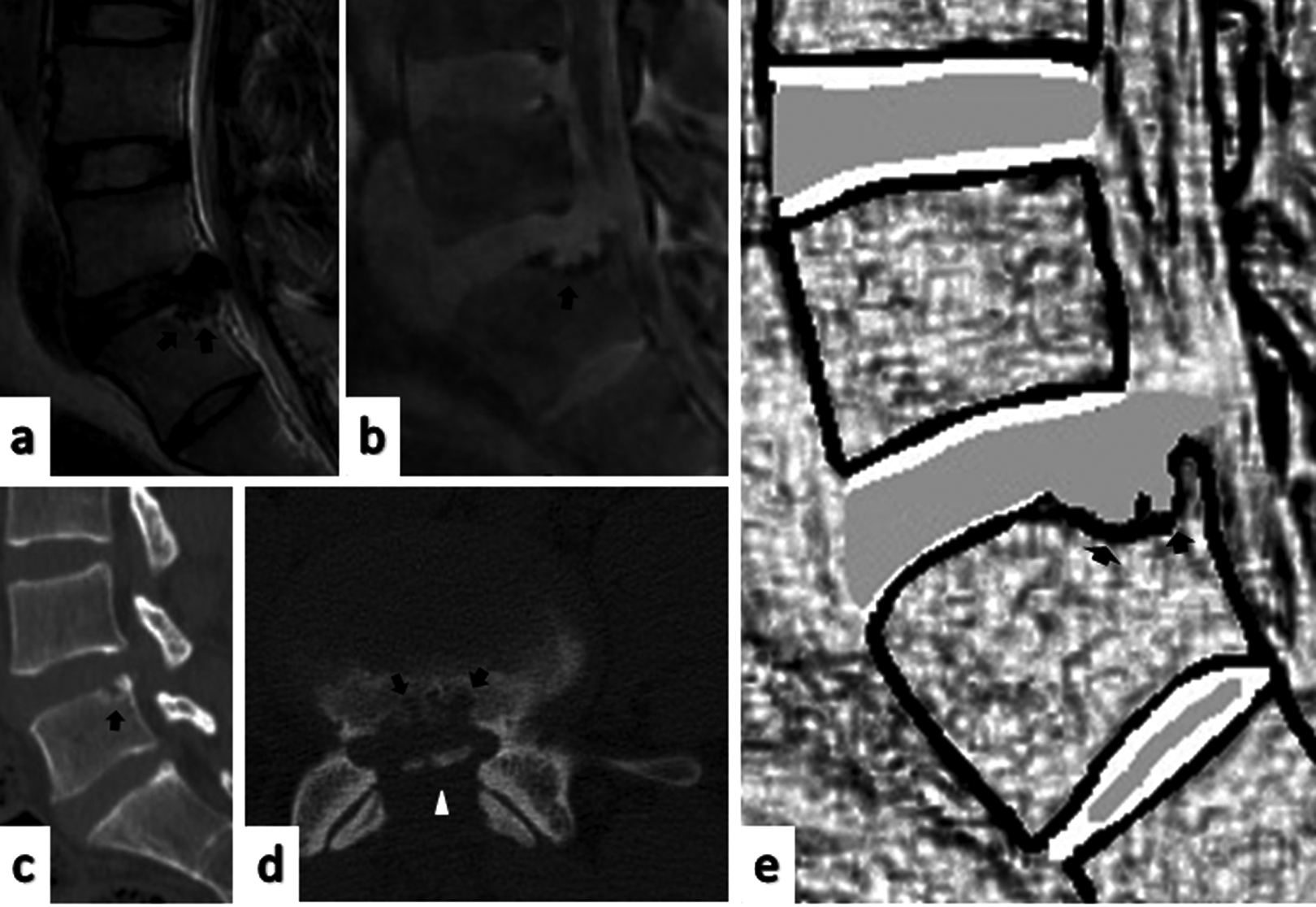
Type 1C herniation: (a) T2 image with L4-5 LDH, (b) 3D FSPGR image, (c, d) CT scan images, (e) sketch of the 3D FSPGR. Black arrows—defect in the inferior endplate along with subchondral sclerosis, white arrowhead—avulsion of underlying bony endplate. LDH, lumbar disc herniation; 3D FSPGR, 3-dimensional fast spoiled gradient; CT, computed tomography.
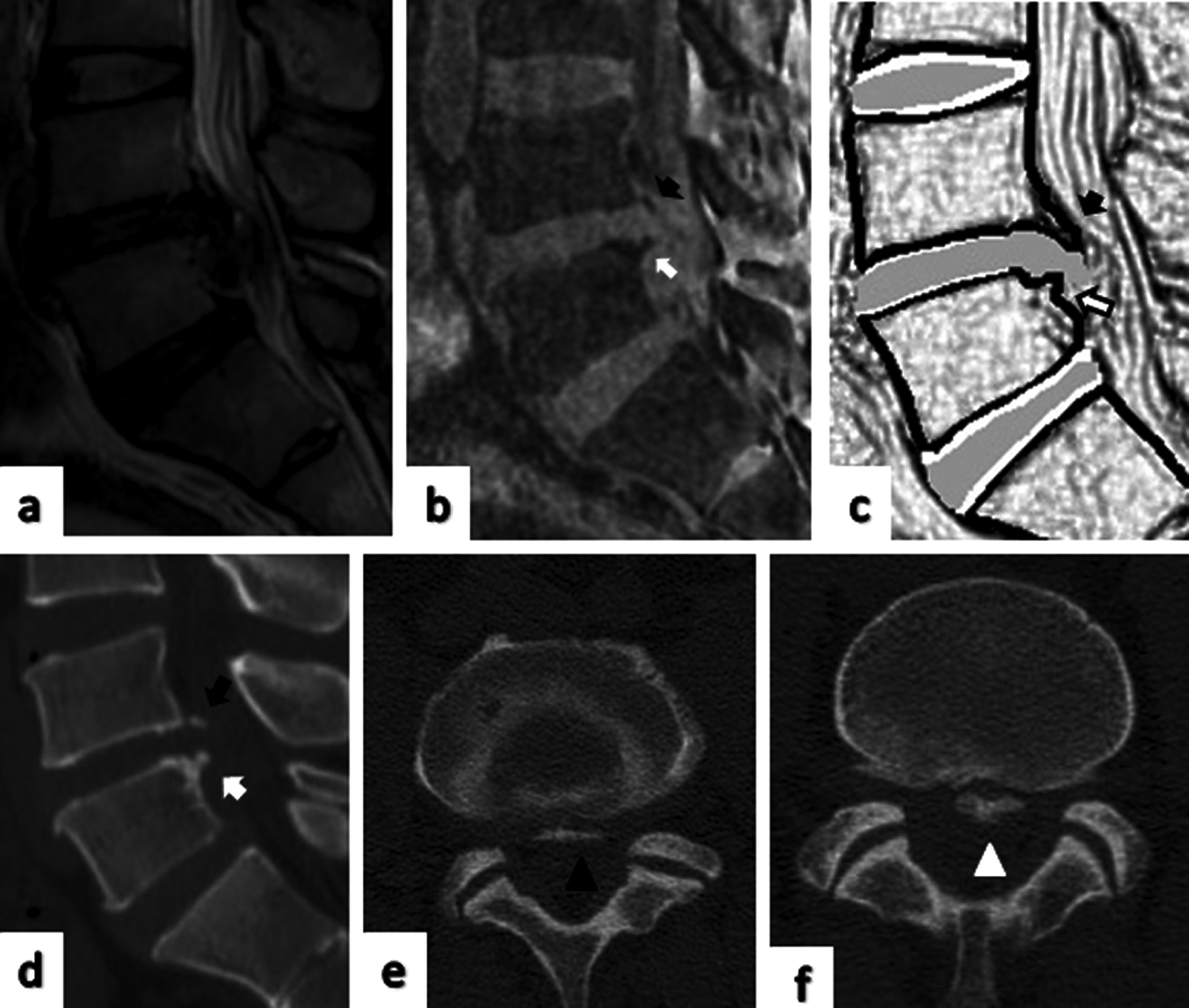
Type 1D herniation: (a) T2 image with L4-5 LDH, (b) 3D FSPGR image, (c) sketch of the 3D FSPGR, (d) mid-sagittal CT scan, (e) axial CT scan at upper endplate level, (f) axial CT scan at lower endplate level. Black arrows—disruption of superior endplate, white arrows—disruption of inferior endplate, arrowheads—avulsed bony fragments at superior (black) and inferior (white) levels. LDH, lumbar disc herniation; 3D FSPGR, 3-dimensional fast spoiled gradient; CT, computed tomography.
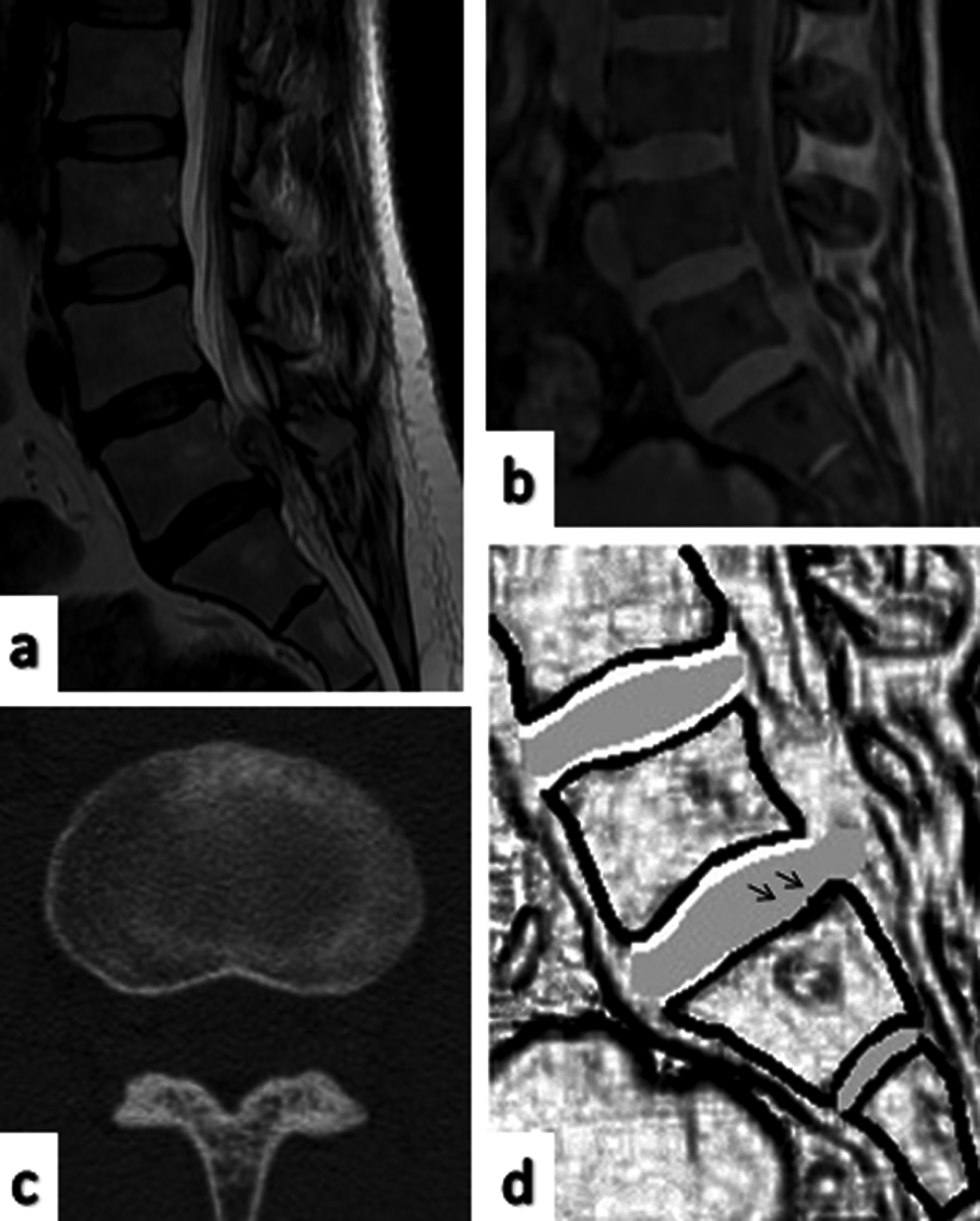
Type 2 herniation with cartilaginous endplate failure: (a) T2 image with L5-S1 LDH, (b) 3D FSPGR image, (c) axial CT scan image, (d) sketch of the 3D FSPGR. Arrows—absence of hyperintense line of inferior cartilaginous endplate. LDH, lumbar disc herniation; 3D FSPGR, 3-dimensional fast spoiled gradient; CT, computed tomography.
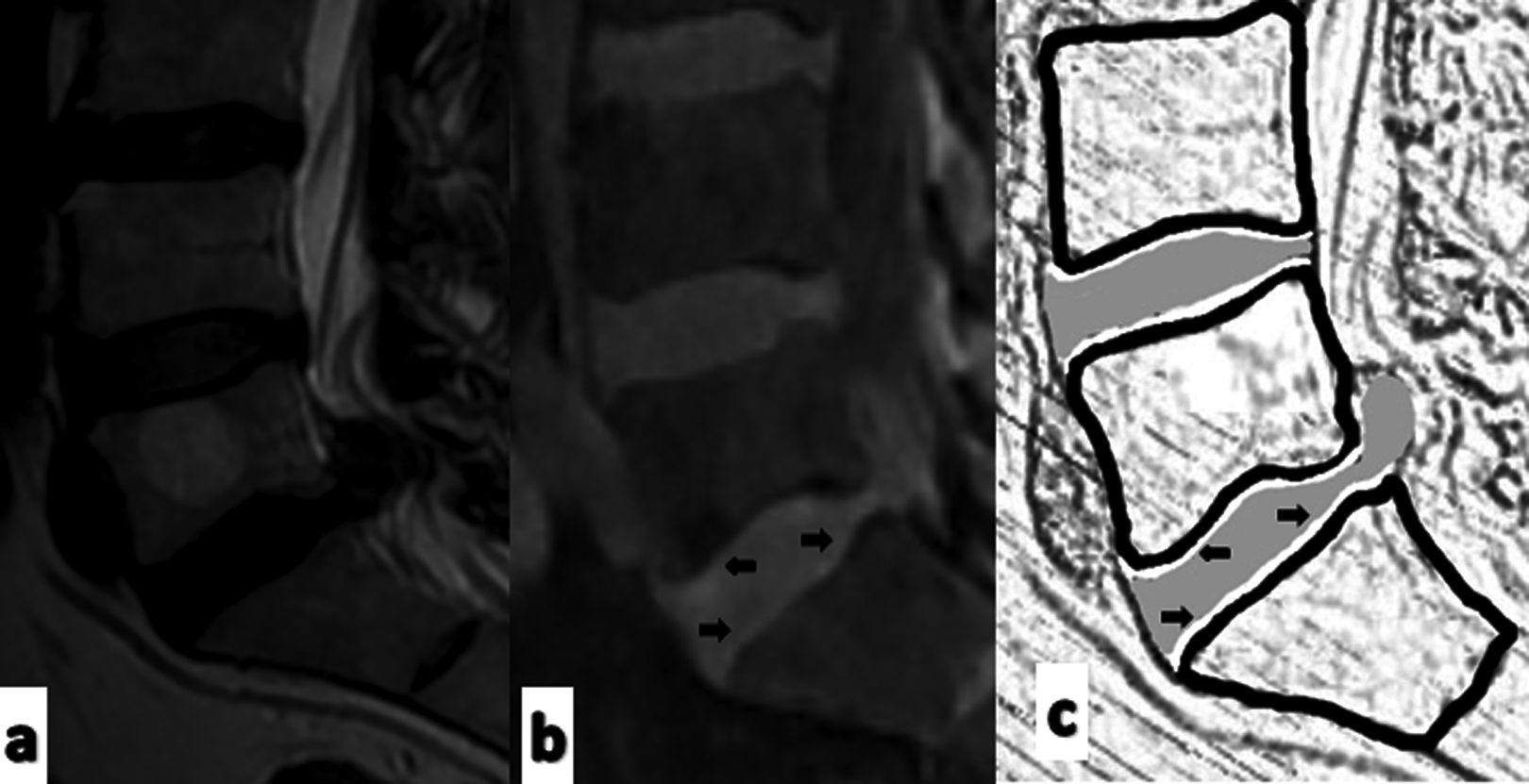
Type 2 herniation without endplate failure: (a) T2 image, (b) 3D FSPGR image, (c) sketch of 3D FSPGR image. Arrows—hyperintense line between disc and vertebra depicting the intact cartilaginous endplate. 3D FSPGR, 3-dimensional fast spoiled gradient.
Eleven patients in group 1 and 6 patients in group 2 had cartilaginous failure at levels additional to LDH level. Four patients in group 1 had bony failure at levels other than the LDH. In all these 4 patients, the L3-4 was the herniated level while L4-5 had the bony failure without herniation. The failure of the endplate was significantly associated with the herniated discs than the lumbar discs without herniation (odds ratio 12.29, P < .01).
The mean duration of back pain was 6.22 ± 3.6 months in group 1, which was significantly higher than that of group 2 (3.03 ± 2 months). In all patients, the low back pain was associated with leg pain with unilateral radiation in 48 patients and bilateral radiation in 18 patients. Eleven patients had neurological deficit (all in group 1) with absence of ankle jerk in 2 of them. Complete loss of fine touch was observed in 2 patients (all in group 1) and hypoesthesia in 48 patients (33 of group 1 and 15 of group 2). Both the groups were similar in terms of sex distribution (Fisher exact test, P = .90), level of herniation (Table 2), stage of disc herniation (Table 3), and canal diameter (Table 4). Fifteen patients had migration of the herniated material of whom 11 had inferior (10 of group 1, 1 of group 2) and 4 had superior (1 of group 1, 3 of group 2) migration.
Distribution of Level of Lumbar Disc Herniation (LDH).

Distribution of Stages of Lumbar Disc Herniation (LDH).

Comparison of the Groups in Terms of Age and Canal Diameter.
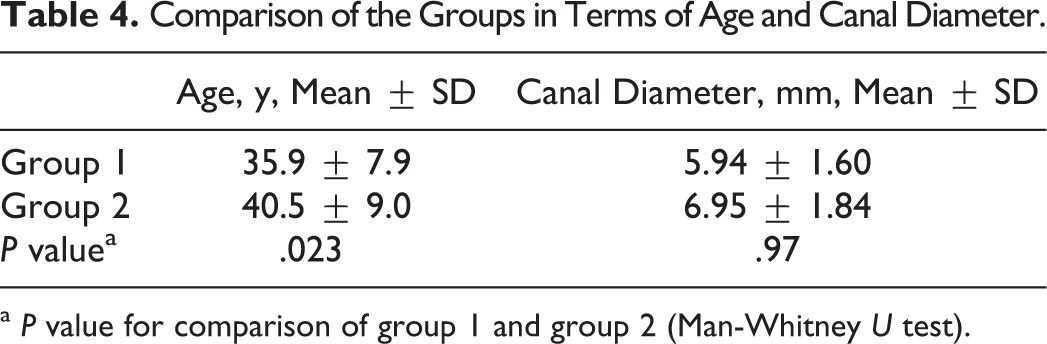
a P value for comparison of group 1 and group 2 (Man-Whitney U test).
A total of 25 patients were operated (23 in group 1 and 2 in group 2) while 41 patients (24 in group 1 and 17 in group 2) were treated conservatively. Nine patients from group 1 were initially planned for conservative management but later operated as the symptoms did not improve. Eight patients (3 in group 1 and 5 in group 2) were planned for surgery, but treated conservatively due to their unwillingness. One patient from group 1 developed discitis in the postoperative period, which was treated with initial intravenous antibiotics and later considered for posterior instrumented fusion. There were no other major complications related to the surgery. The paresthesia and neurological status improved in all but one patient from group 1. In this patient, the discectomy was difficult owing to the hardness of the disc.
The mean initial SLR was 27.1° ± 14.2° in group 1 and 33.1° ± 19.1° in group 2. The initial SLR was comparable among the groups and all groups showed improvement during follow up period. While there was no difference between the surgically treated patients in both groups, the improvement of SLR was significantly lower in the group 1 patients treated conservatively. This difference was evident at 6 weeks and remained thereafter (Figure 7a). Initial mean VAS was 7.2 ± 0.87 in group 1 and 5.6 ± 0.96 in group 2, while the initial mean ODI was 46.9 ± 11.9 in group 1 and 28.7 ± 7.5 in group 2. Though at the beginning VAS and ODI were significantly worse in group 1 patients than group 2, later all patients showed improvement (Figure 7b and c).
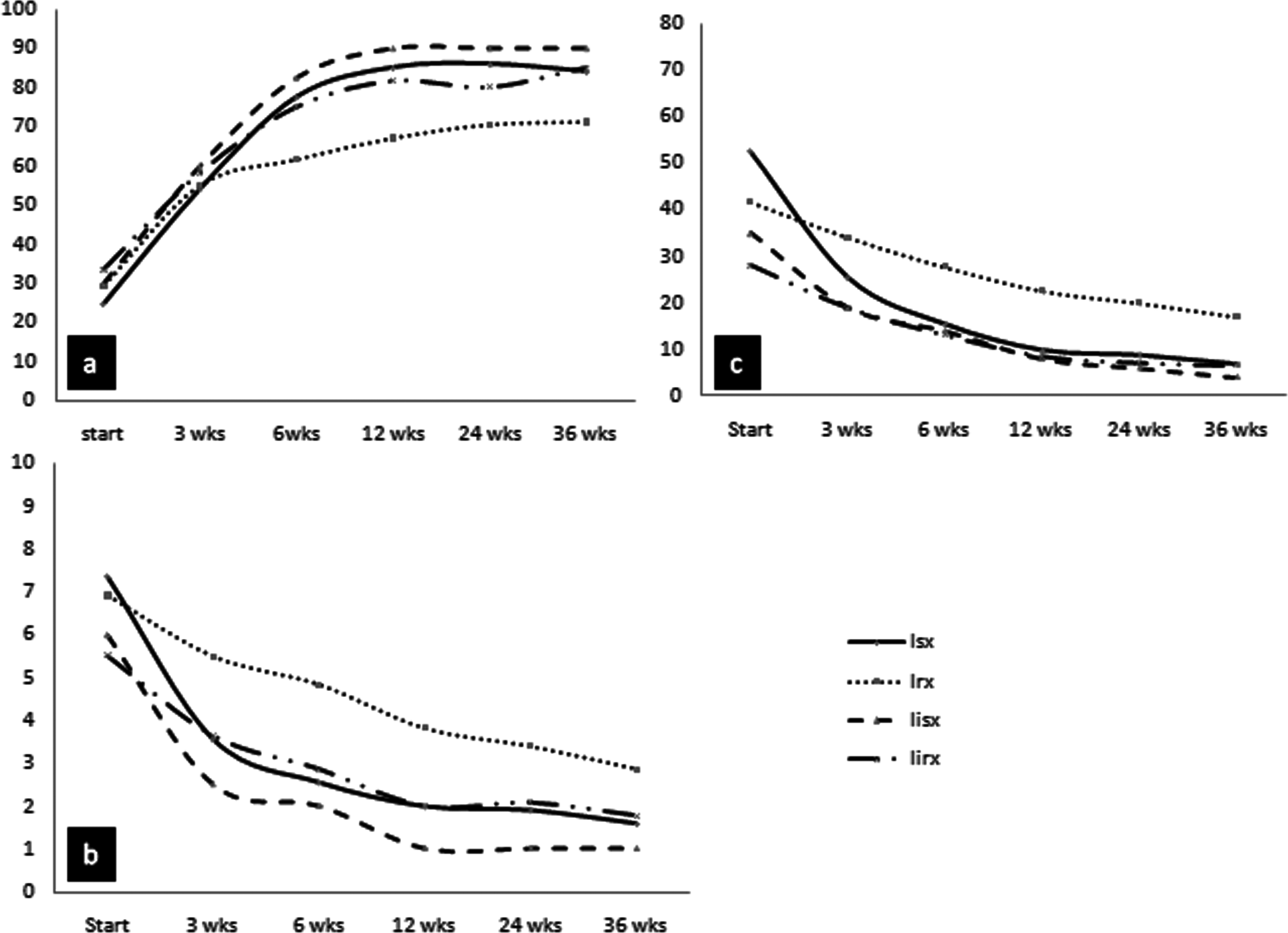
Change of clinical parameters during follow-up: (a) change of SLR, (b) change of ODI, (c) change of VAS. Wks—weeks, Isx (solid line)—mean value of patients with bony EPF and were operated, Irx (dotted line)—mean value of patients with bony EPF and were treated conservatively, IIsx (dashed line)—mean value of patients without bony EPF and were operated, IIrx (dash dot line)—mean value of patients without bony EPF and were treated conservatively. SLR, straight leg raising; ODI, Oswestry disability index; VAS, visual analogue score; EPF, endplate failure.
Discussion
The present study used MRI to assess and classify the endplate failure and correlate it with the clinical picture. Though few previous authors have observed fracture of vertebral rim in the pathogenesis of LDH, 21 –25 Rajasekaran et al 9 first classified the endplate junctional failure associated with LDH. In this study, we used the 3D FSPGR sequence to evaluate the endplate cartilage and found it to have excellent sensitivity and specificity for detection of endplate failure.
In this study, patients with bony failure were found to be younger (Table 4). This is probably because of the fact that, at younger age, annulus fibrosus is stronger than endplate junction. Thus, when loaded in pure compression or torsion along with axial compression and flexion, the endplate fails before annulus fibrosus. 30 –32
In the present study, 47 patients (71.2%) had bony failure and 17 patients (25.7%) had cartilaginous failure. As all bony failures were also associated with cartilage endplate lesions, 97% of patients had some cartilaginous components in the herniated materials, which is higher than most of the previous studies. However, most of the previous reports had used histopathology to evaluate the bony or cartilaginous components where there were chances of missing smaller fragments during surgical removal and subsequent histopathological preparations. 2,6 –8 Anatomical variations in the annulus also can contribute to the pattern of EPF. As the cartilage endplate does not extend beyond the mid annulus, the peripheral portion of annulus is directly attached to the vertebral bone by strong collagen (Sharpey’s) fibers and may pull off bone fragment from posterior corner of the vertebral body. 8,33 –35 In the middle region of annulus, the collagen fibers are thickest and attached to the cartilage endplate at a distance away from bone. Because of the strong bonding between the bony and cartilaginous endplates here, the displaced cartilage may sometimes take fragments of subchondral bone along with it resulting in an erosion of the bony endplate. 8,13,36 This explains the genesis of most common patterns of EPF. Near the inner annulus cohesive strength between central cartilaginous endplate and the adjacent bone is weak. Thus, even with modest force, the nucleus-cartilaginous endplate can easily be pulled off the bone resulting in an isolated cartilaginous failure. 4,20
Both erosion and avulsion type of disc herniations are common in those of a younger age, with larger herniations and substantial migrations. 6,17,35,36 As the patients in our study were relatively younger, this might have contributed to the higher occurrence of type 1A and 1B EPF.
Four patients had bony failure at other levels, all at L4-L5 when the LDH was at L3-L4. Considering the fact that bony endplate fracture may take many months to progress to LDH, it is possible that these other level bony failures may be the initiating pathology for future disc herniation. 9,12,20,24 This may provide a window of opportunity for intervention to prevent progression and ultimate herniation. 9
In the present study, regardless of treatment, clinical parameters improved in all groups. However, in the bony failure group, conservative management resulted in significantly lesser improvement than surgery. This was most probably owing to hardness of discs in bony failure that can produce significant compression. Such a compression can only be relieved by surgical means. 7 –9 We also had difficulty in removal of the disc in 1 patient. When associated with large bony fragment, it may be difficult to remove the herniated disc with fenestration alone. These patients would be better benefitted with a wider laminectomy. One patient had residual weakness even after surgery. This was probably due to high contact pressure between the herniated material and nerve root resulting in ischemia and demyelination. 7,37,38 Another patient with bony failure developed discitis after surgery. Free movement of bacteria after the defect created due to bony failure and the anaerobic environment around the herniation could have prompted this infection. 8,39
Previous studies had stated that presence of cartilage endplate in the extruded material impedes the neovascularization and resorption, resulting in a poorer prognosis of LDH. 7,8,40 –43 Interestingly in the present study patients with isolated cartilaginous failure showed good clinical improvement with conservative management. We do not have much literature that explains this phenomenon, but propose a few possibilities. The MRI sequences used in this study could only identify the presence of cartilage endplate lesion, but could not quantify the amount of cartilage in the herniated materials. Considering the wide variations in cartilage content, the prognosis may thus be affected. 7,34,44 As the severity of neurodeficit was much lesser in isolated cartilaginous failure, probably these patients had minimal amount of cartilage in the herniated material. 7 Willburger et al 7 have observed that higher hyaline cartilage content can make the herniation heavier resulting in inferior migration. This was seen only in 1 out of 17 patients among cartilaginous failure group of the present study.
Our study had few limitations. First, our center being a tertiary referral center, we often get patients having severe symptoms with longer duration or unrelieved by conservative therapy given elsewhere. This might have influenced the incidence of the bony and cartilaginous failures. Second, the number of surgically treated patients in group 2 was very small for any statistical calculation. Also with 3D FSPGR sequence it was very hard to differentiate between cartilaginous failure associated with LDH and loss of cartilage endplate due to degeneration. Finally, we have used the 1.5-T MRI that was available to us. An MRI of 3.0-T or higher could have given a better resolution.
Conclusion
This study demonstrates that endplate lesions especially the bony failures are very common in symptomatic lumbar disc herniation. It also strengthens the evidences, that the endplate rather than the annulus is the primary site of pathology. Identification and classification of the endplate failure has implications in the prognosis, as the involvement of the bony component increases the need for surgery. This study also provides the evidence that the 3D FSPGR sequence can be successfully used for identification and classification of the endplate failure, thus reducing the need for CT scan.
Footnotes
Acknowledgments
We thank Dr Alok Sood, Professor of Orthopaedics, Lady Harding Medical College, New Delhi and Dr Ritesh Bhoot, Neurosurgery Consultant, Vivekananda Hospital, Bhubaneswar for their valuable help in preparation of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been funded by the AO Spine Asia Pacific research grant. One or more authors have received Fellowship Support from AO Spine Asia Pacific previously not related to this research.