
Abstract
Study Design
Cadaveric anatomical studies.
Objective
This study aims to investigate the anatomical relationship between bony landmark “V point”, dural sac, nerve roots, and intervertebral disc for improving operative outcomes and decreasing post-operative complications in posterior endoscopic cervical foraminotomy or discectomy (PECF or PECD).
Methods
10 soft adult cadavers were studied. We measured the distance of the V point to the lateral margin of dural sac, V point to the inferior border of intervertebral disc, and the inferior border of cervical nerve root to the inferior border of intervertebral disc. Then we calculated the mean of distance from V point to the inferior border of cervical nerve root.
Results
The mean distance from the V point to the lateral margin of dural sac from C3/4 to C7/T1 ranged from 3.1 ± 1.38 mm to 3.37 ± 1.46 mm. The mean distances from V point to the inferior border of intervertebral disc from C3/4 to C7/T1 were .19 ± 1.16 mm at C3/4, .45 ± 1.23 mm at C4/5, .43 ± 1.01 at C5/6, −.43 ± 1.86 mm at C6/7 and −1.5 ± 1.2 mm at C7/T1. The mean distance between V point and the inferior border of cervical nerve root from C3/4 to C7/T1 showed all positive value, ranging from .06 ± 1.18 mm to 4.45 ± 2.57 mm, increasing caudally.
Conclusion
In performing PECF or PECD, a 3-4 mm radius of bone removal should be enough for exposure and neural decompression at C3/4 to C5/6. At C6/7 and C7/T1 a more extensive bone cut of more than 4 mm is recommended, especially in cranial direction.
Introduction
Surgical procedures for cervical radiculopathy have been performed by either an anterior or posterior approach. Although the anterior approach to the cervical spine has received the most attention in recent years, problems associated with instrumentation and fusion have led to the adoption of motion preservation surgery. The posterior approach was developed to improve surgical outcome and decrease postoperative complication related to anterior approach and has been historically proven as an effective and safe method for selected cervical pathologies.1-3 Conventional posterior approaches to the cervical spine require extensive subperiosteal stripping of the paraspinal musculature, leading to postoperative morbidities due to higher surgical trauma. Presently, the development of minimally invasive spine surgery (MISS) using a full endoscopic system enables spine surgeons to avoid approach-related complications or extensive tissue damages of open surgeries. Posterior endoscopic cervical foraminotomy or discectomy (PECF or PECD) is a well-established, minimally invasive surgery for cervical radiculopathy. However, PECF or PECD may be associated with postoperative complications owing to limited surgical visual field, surgeons’ experience, and operation technique.2,4,5
The important bony anatomical landmark for PECF or PECD is the “V point”. This landmark is formed by the inferior border of the upper laminae, the superior edge of the inferior laminae, and the medial point of the facet joint.6,7 The 3 bony structures converges forming a V-shape, serving as a landmark for starting decompressive bone work during the surgery (Figure 1). The radius of decompressive bone work proposed in many literatures often refer to the distance relative to this “V point”.6,7 To safely perform PECF or PECD, it is essential to understand the anatomical relationship between the V point, neural structures, and compressive intervertebral disc pathology. However, anatomic studies on these cervical anatomical landmarks have not been well elucidated. The “V-Point” is formed by the inferior border of the upper laminae, the superior edge of the inferior laminae, and the medial point of the facet joint. The 3 bony structures converges, forming a V-shape, serving as a landmark for starting decompressive bone work during the surgery.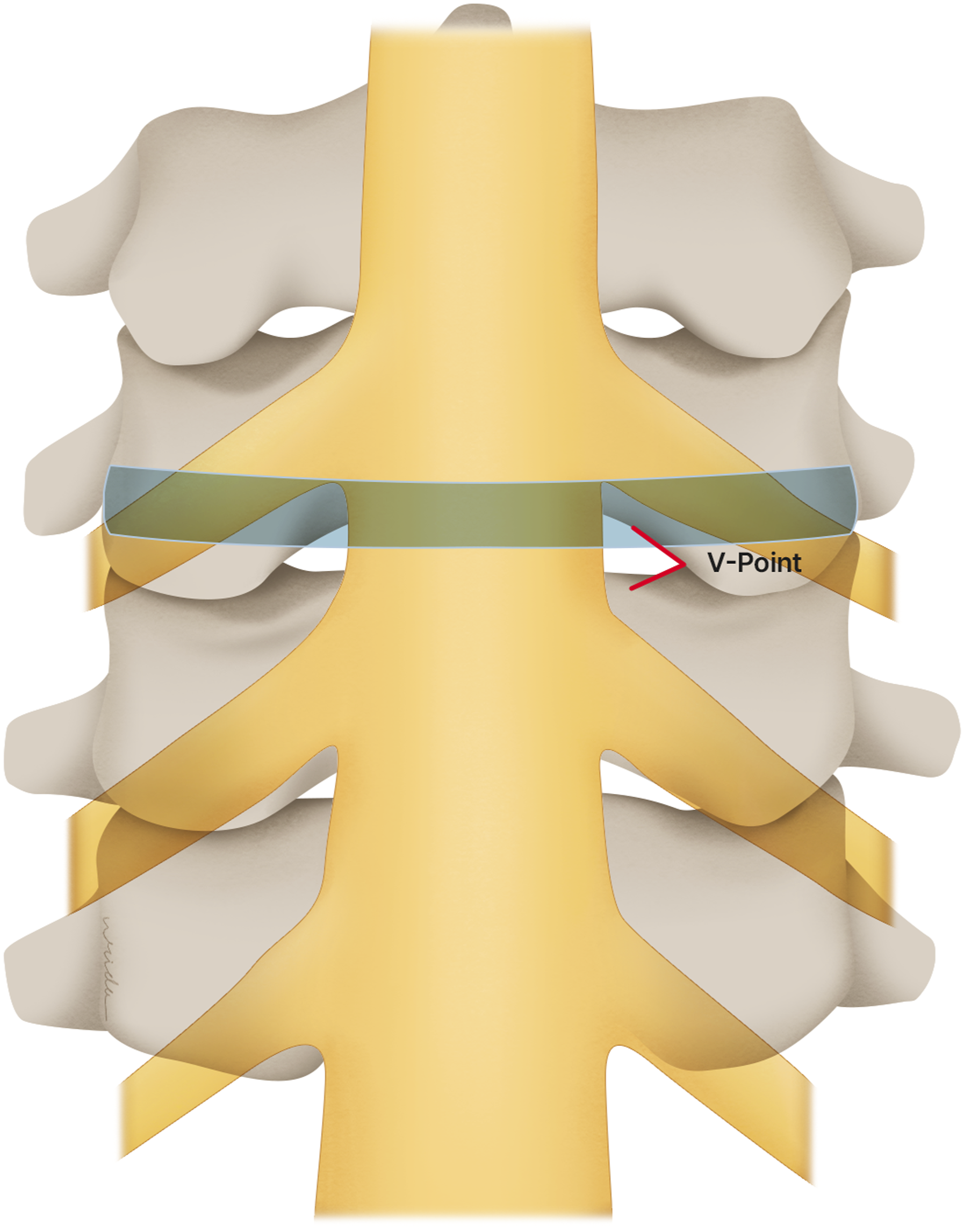
The objective of this study is to define the anatomical relationship between landmarks V point, dural sac, cervical nerve roots and intervertebral disc. This knowledge should improve operative outcomes, safety, and decrease postoperative complications of PECF and PECD.
Materials and Methods
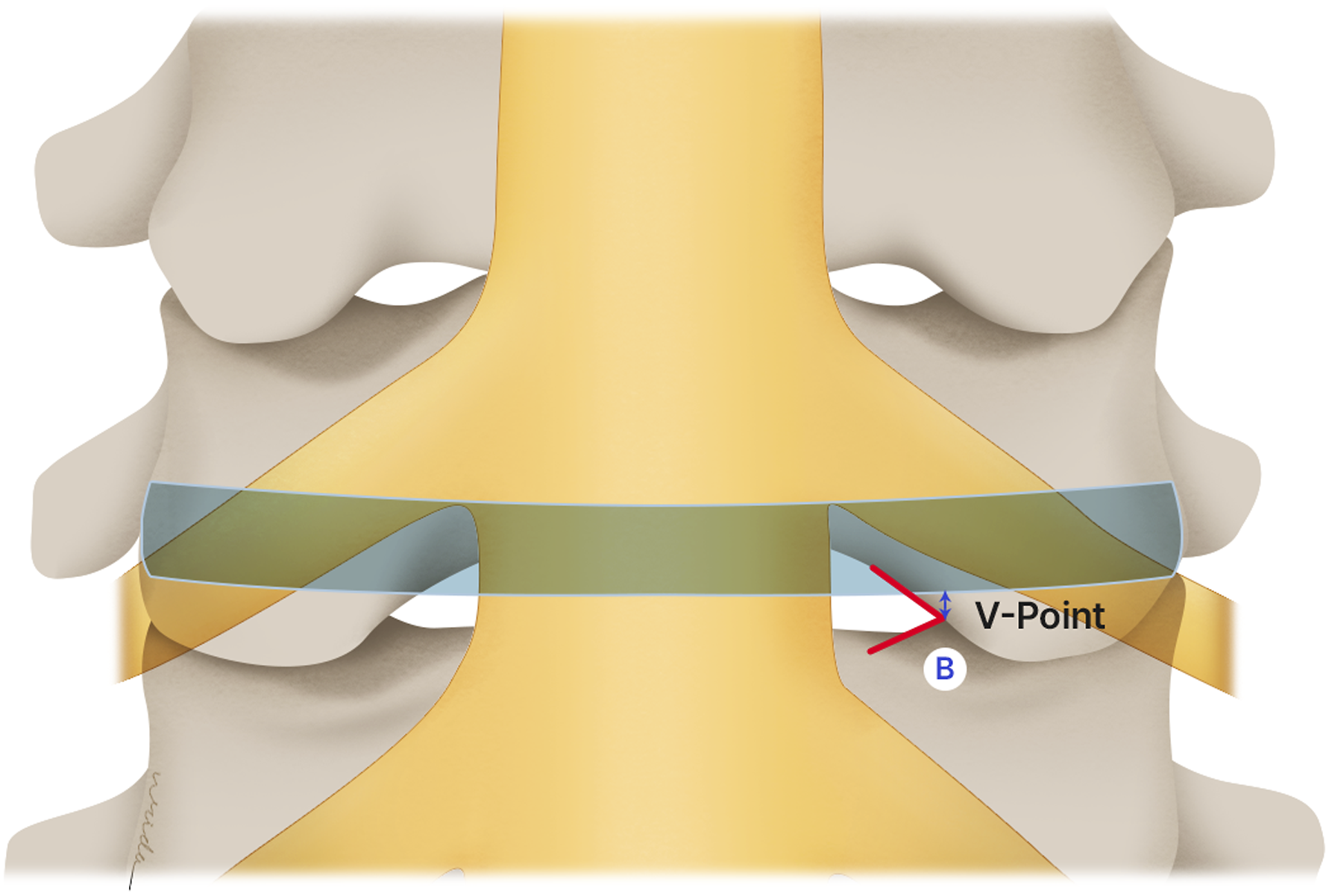
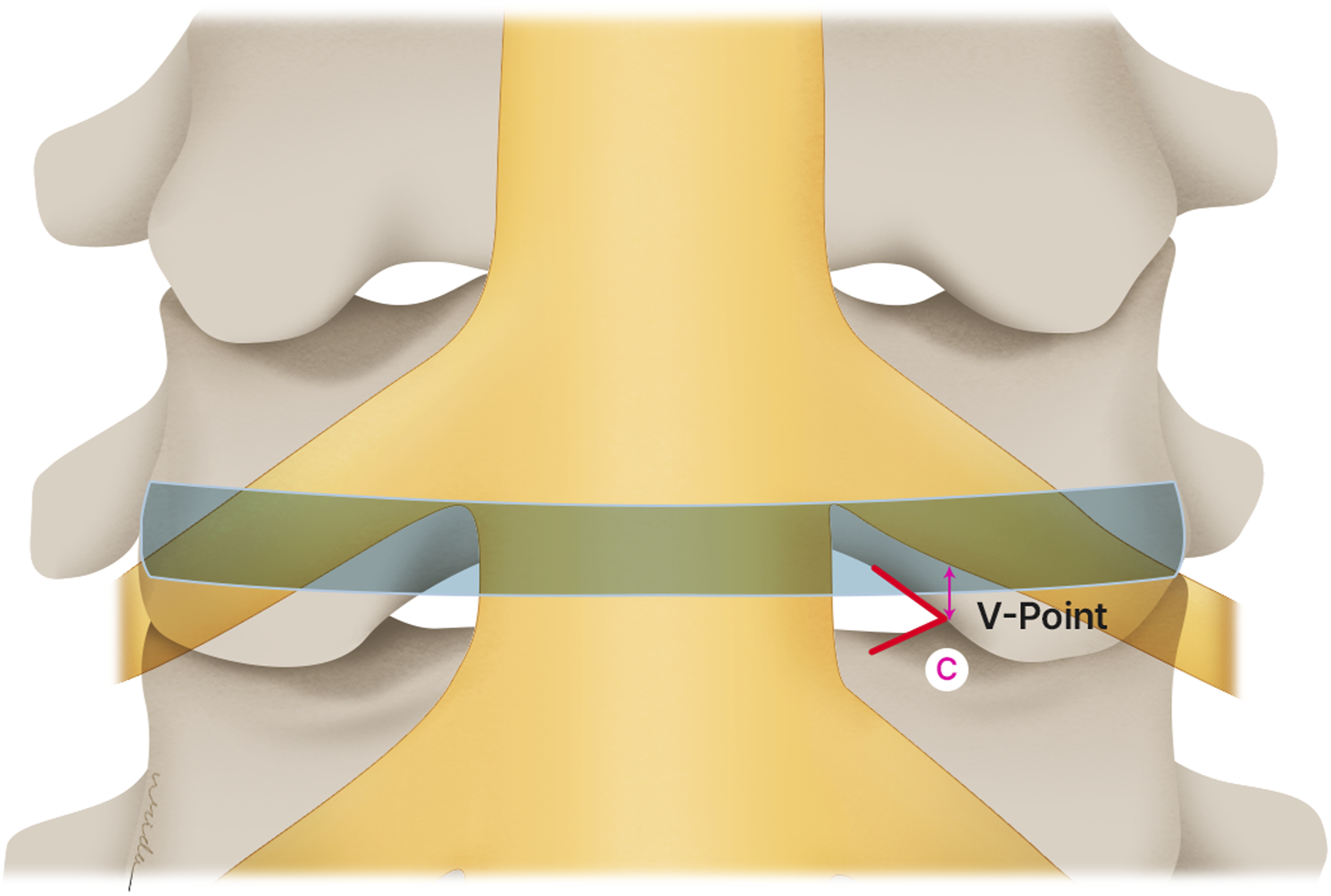
10 soft adult cadavers (5 men and 5 women), ages at death ranging from 59 to 95 years (mean, 76 years) were used in this study. The cadaveric specimens of the cervical spine from the occipital bone to the first thoracic vertebra were obtained. Cadavers with history of cervical spine trauma, metastasis, infection, and previous cervical spine surgery were excluded. These cervical spines were positioned neutral in sagittal plane and cleaned thoroughly of all the posterior soft tissues. V point was identified and marked level by level. Partial Laminectomy was done by high-speed burrs and Kerrison rongeur. The tip of bony V point was preserved until the complete exposure of lateral margin of dural sac. The distance between V point to lateral margin of dural sac was measured (A) at C3/4 to C7/T1 level on both sides (Figure 2). Consequently, the inferior border of each intervertebral disc was identified from C3/4 -C7/T1. The distance between inferior border of intervertebral disc and V point was measured (B) in vertical plane (Figure 3). Subsequently, 2 mm Kerrison rongeur was used to remove laminar bone to expose the cervical nerve root C3 to C8 on both sides. The distance between inferior border of nerve root and inferior border of intervertebral disc was measured (C) in vertical plane (Figure 4). Because the exposure of nerve roots causes damage to V point, the distance between V point and cervical nerve root was measured indirectly by calculation of distances between V point to inferior border of the disc and V point to inferior border of nerve root. (Distance of V point to inferior border of cervical nerve root = (Nerve root to Intervertebral disc) – (V point to Intervertebral disc)). The distance between the V point to lateral margin of dural sac was measured (A). The distance between inferior border of intervertebral disc and V point was measured (B) in vertical plane. The distance between inferior border of nerve root and inferior border of intervertebral disc was measured (C) in vertical plane.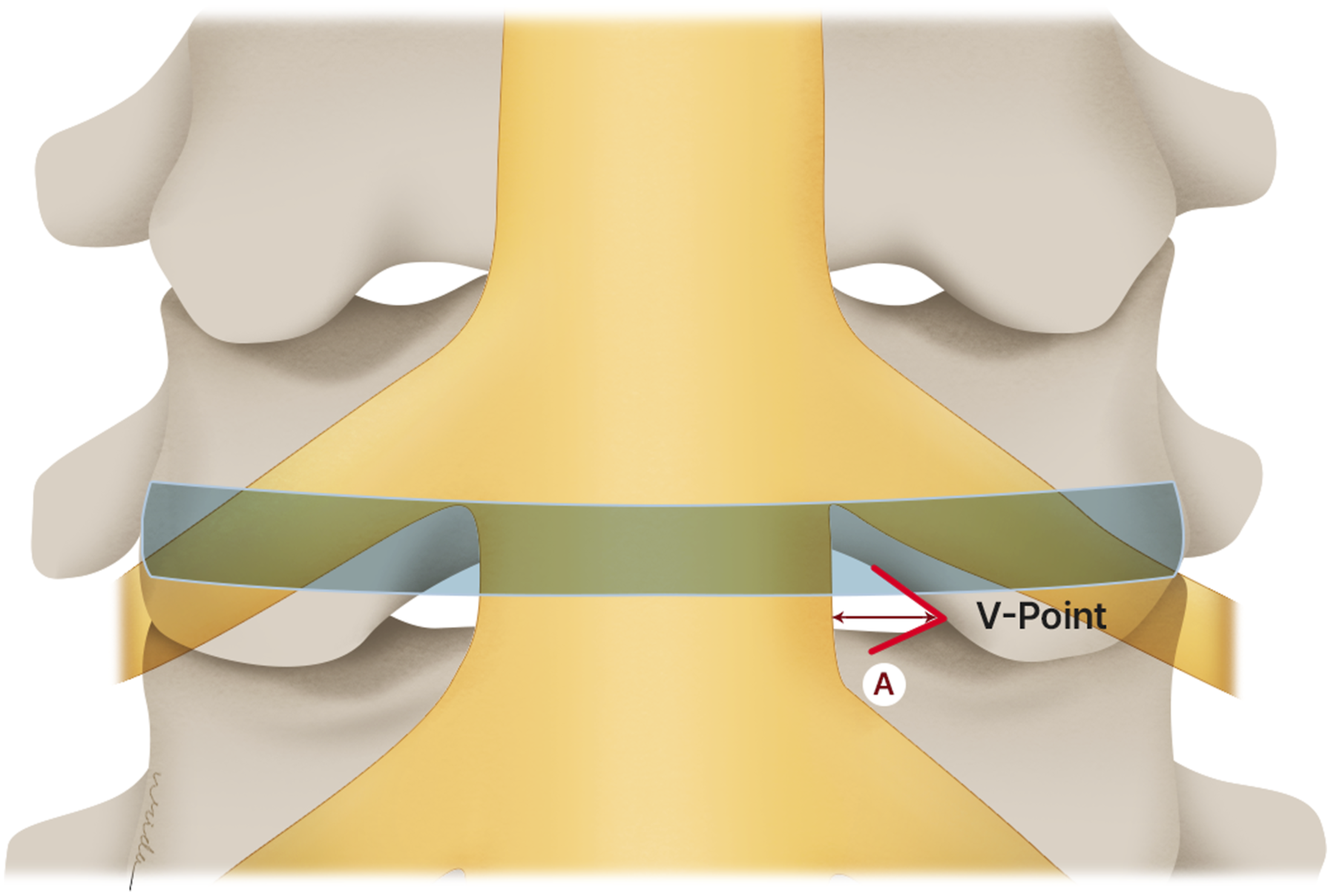
All parameters were measured 2 times by the senior spine surgeon and spine fellow, and the mean was used as the final value. All measurements were made using Vernier Caliper.
Statistical Analysis
Statistical analyses were performed using PASW Statistics ver. 18.0 (SPSS Inc., Chicago, IL, USA). All parameters are continuous data. We calculated the means and standard deviations (mean ± standard deviation)
Result
The Anatomic Relationship Between the V Point and the Lateral Margin of Dural Sac.
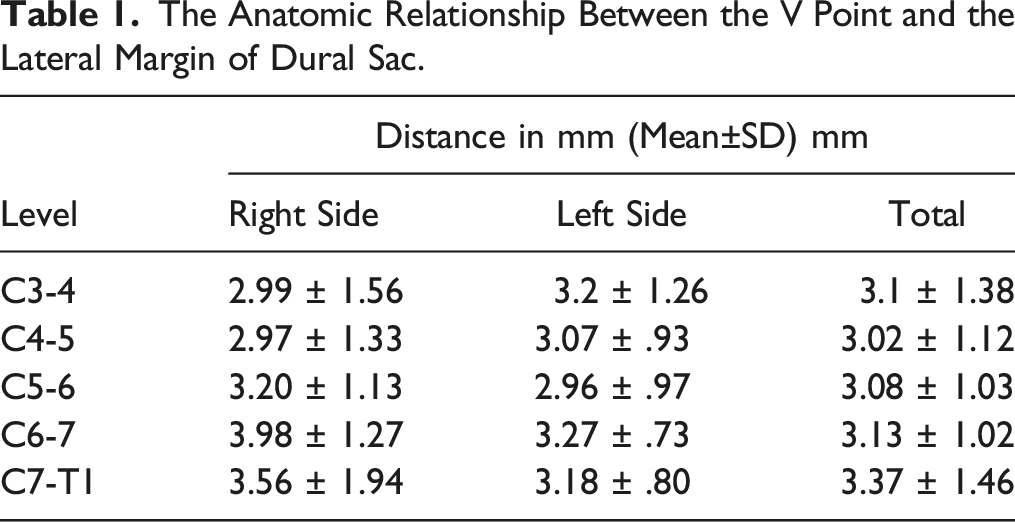
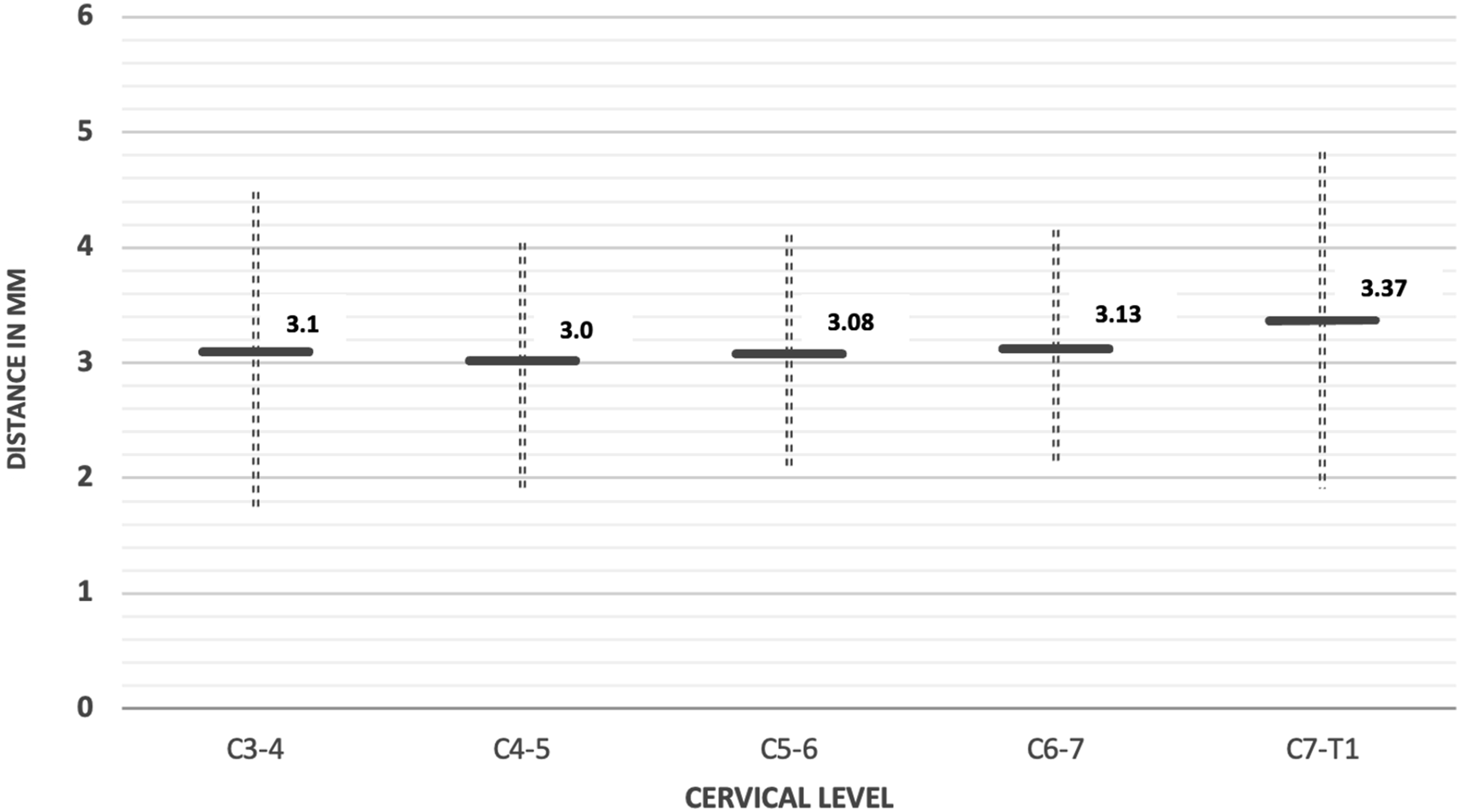
The anatomic relationship between the V point and the lateral margin of dural sac. Distance is presented as mean +/− SD of the average of the left and right sides.
The Anatomic Relationship Between the V Point and the Inferior Border of Intervertebral Disc.
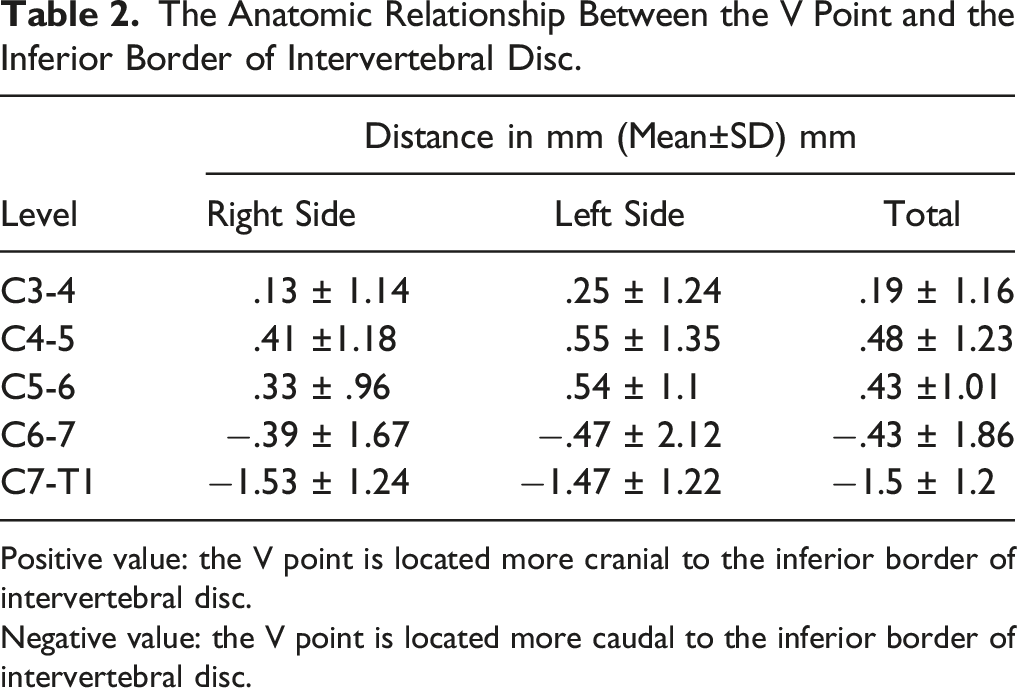
Positive value: the V point is located more cranial to the inferior border of intervertebral disc.
Negative value: the V point is located more caudal to the inferior border of intervertebral disc.
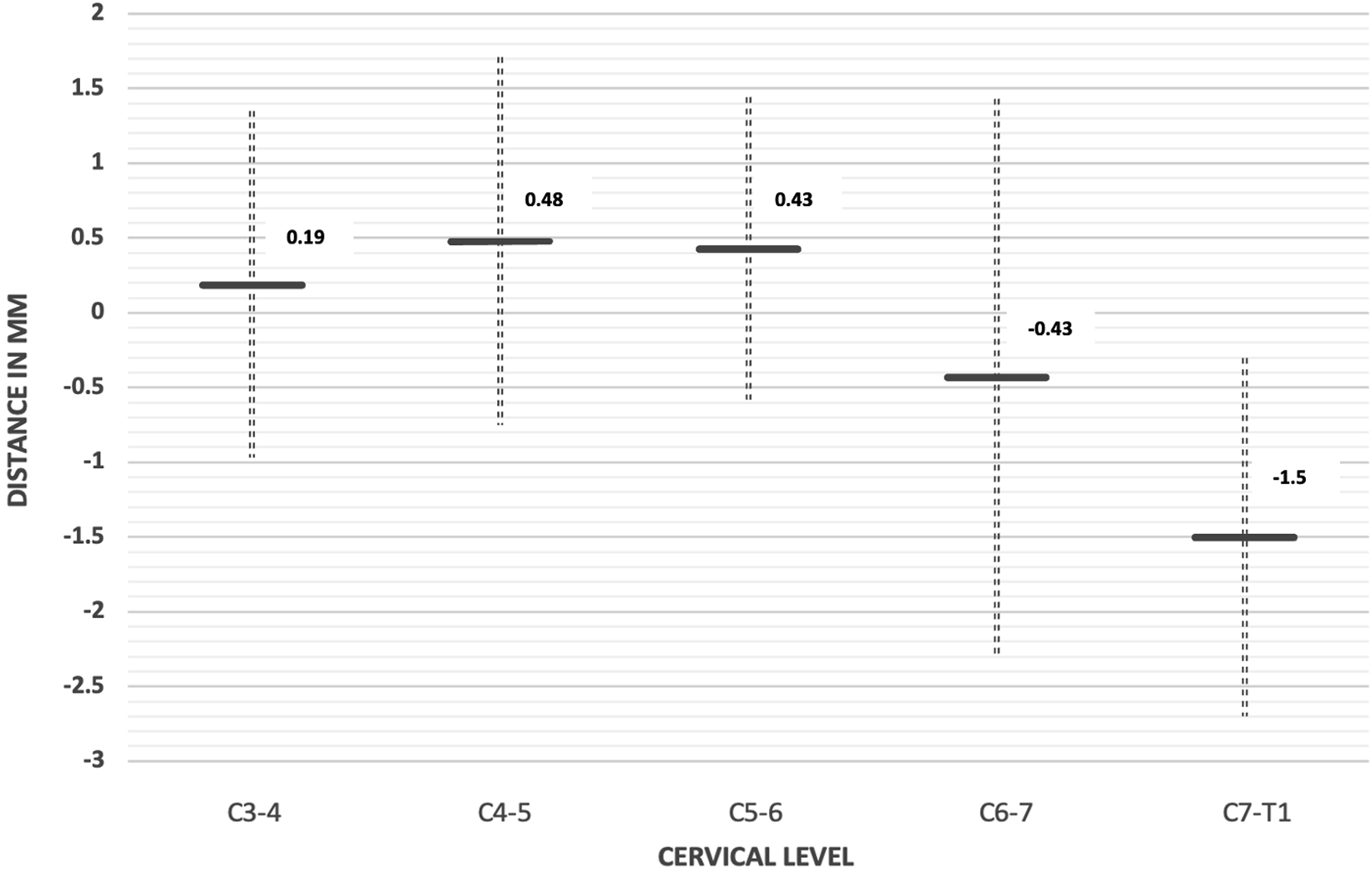
The anatomic relationship between the V point and the inferior border of intervertebral disc. Distance is presented as mean +/− SD of the average of the left and right sides. Positive value: the V point is located more cranial to the inferior border of intervertebral disc. Negative value: the V point is located more caudal to the inferior border of intervertebral disc.
The Anatomic Relationship Between the Inferior Border of Cervical Nerve Root and the Inferior Border of Intervertebral Disc.
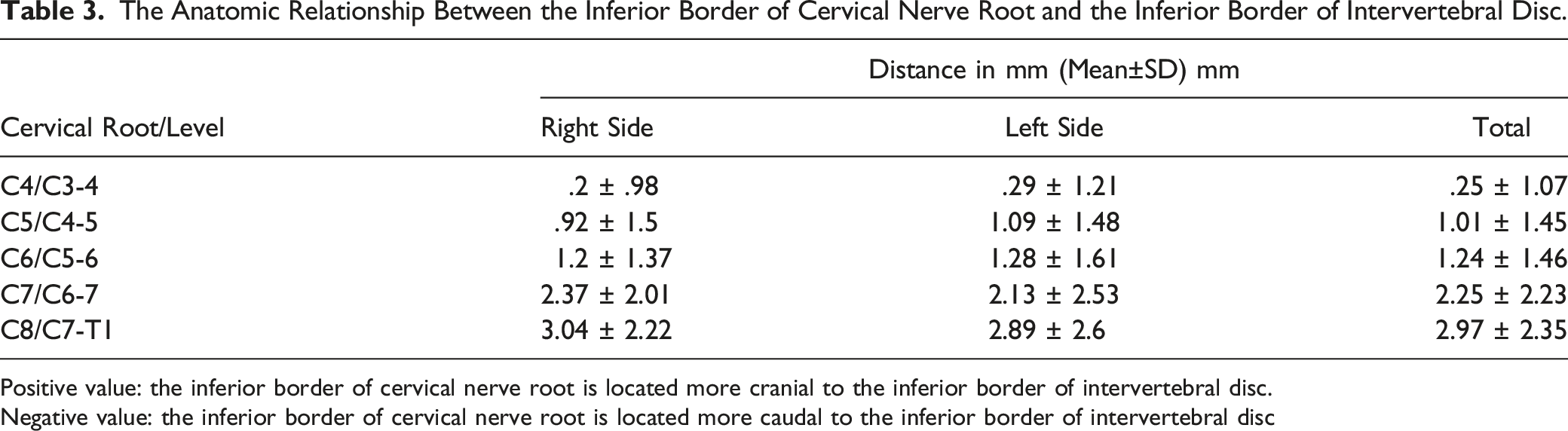
Positive value: the inferior border of cervical nerve root is located more cranial to the inferior border of intervertebral disc.
Negative value: the inferior border of cervical nerve root is located more caudal to the inferior border of intervertebral disc
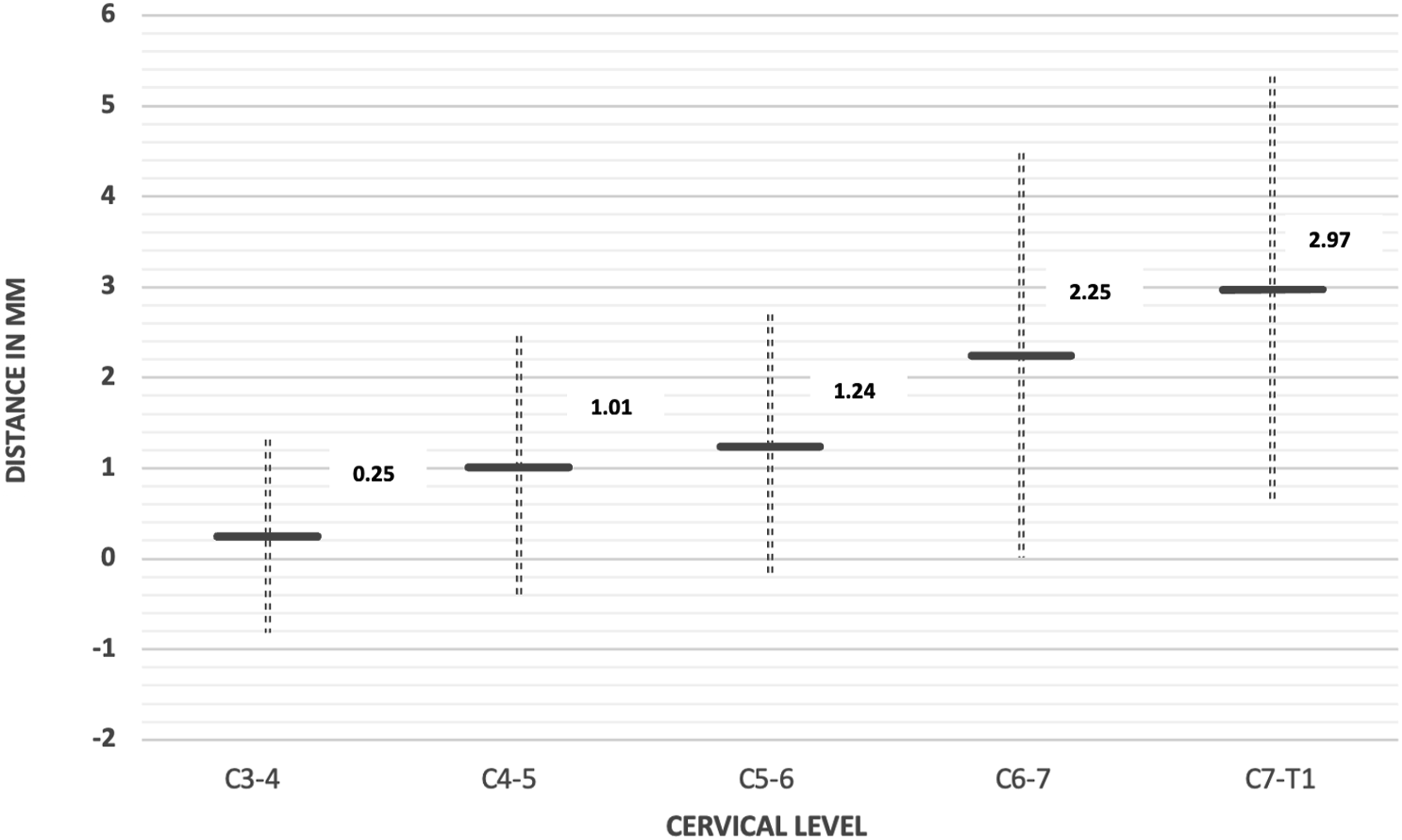
The anatomic relationship between the inferior border of cervical nerve root and the inferior border of intervertebral disc. Distance is presented as mean +/− SD of the average of the left and right sides. Positive value: the inferior border of cervical nerve root is located more cranial to the inferior border of intervertebral disc. Negative value: the inferior border of cervical nerve root is located more caudal to the inferior border of intervertebral disc.
The Anatomic Relationship Between the Inferior Border of Cervical Nerve Root and the V Point.
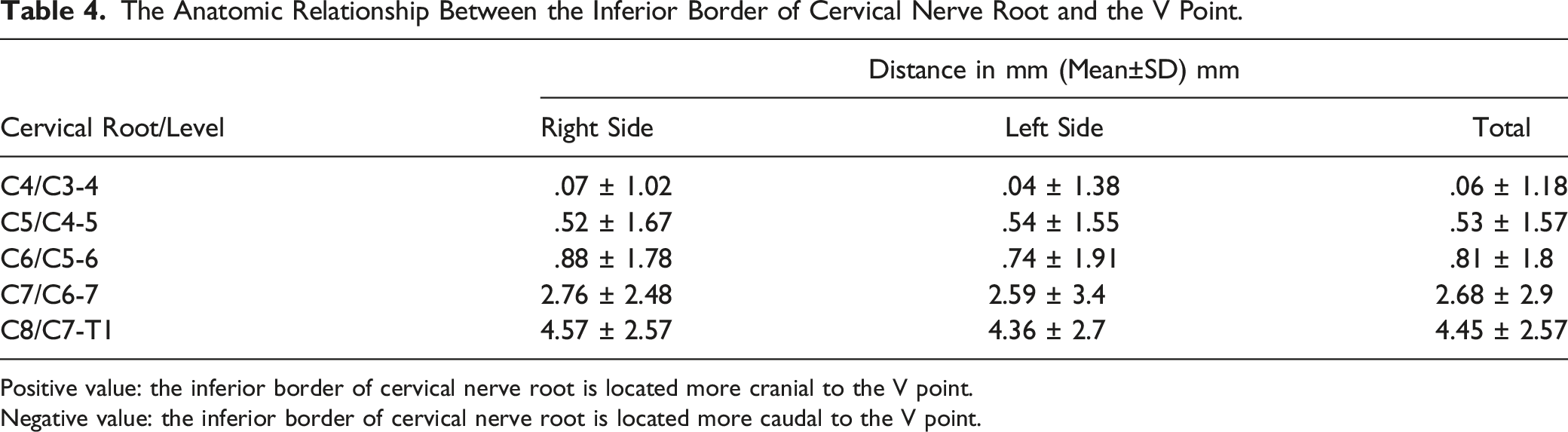
Positive value: the inferior border of cervical nerve root is located more cranial to the V point.
Negative value: the inferior border of cervical nerve root is located more caudal to the V point.
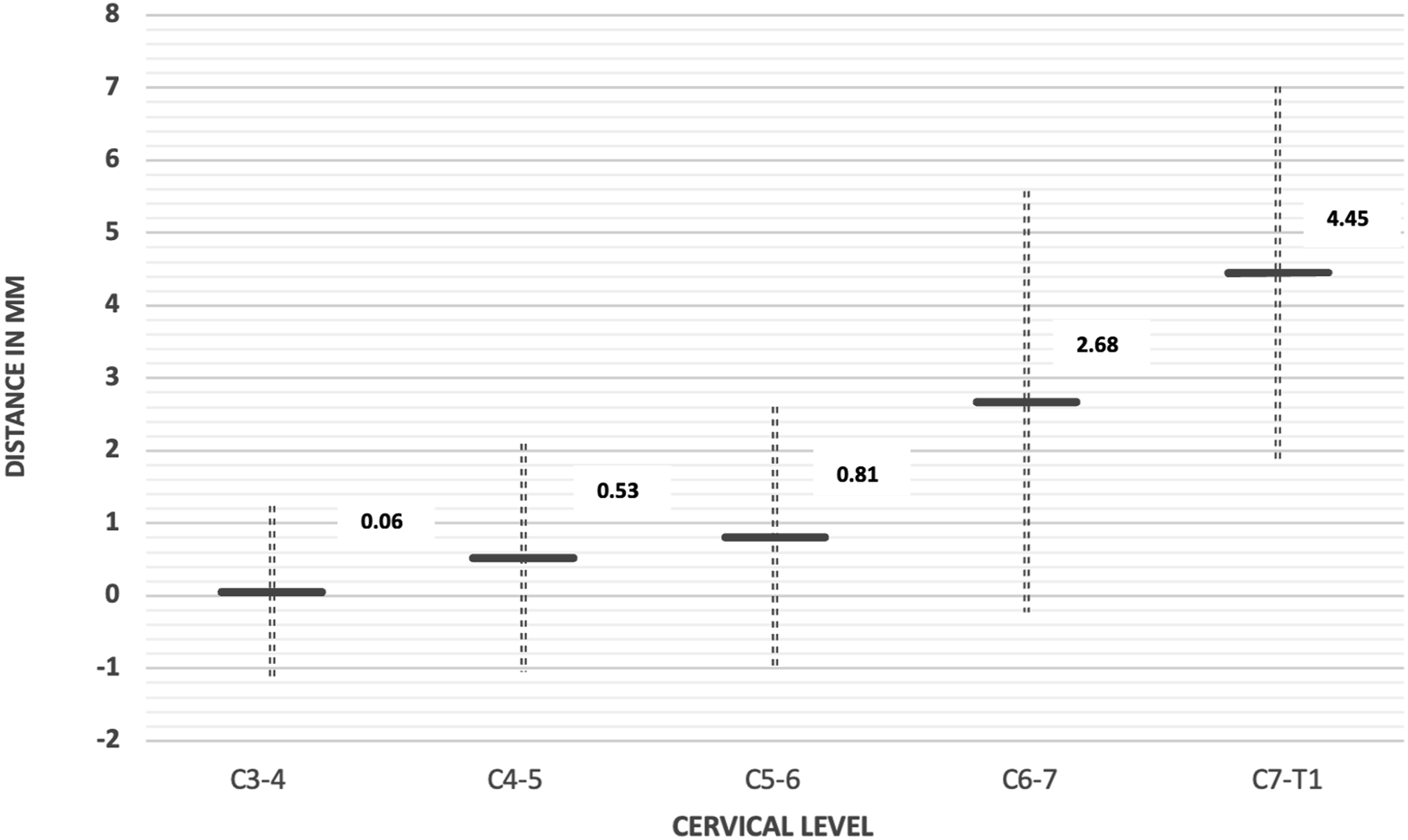
The anatomic relationship between the inferior border of cervical nerve root and the V point. Distance is presented as mean +/− SD of the average of the left and right sides. Positive value denotes that the inferior border of cervical nerve root is located more cranial to the V point. Negative value denotes that the inferior border of cervical nerve root is located more caudal to the V point.
Discussion
Minimally invasive spine surgery has been developed for the treatment of spinal diseases with minimized surgical trauma. It was wildly used for the lumbar spine surgery and gained more popularity in the cervical spine area. Cervical radiculopathy caused by either lateral disc herniation or foraminal stenosis can be treated by minimally invasive spinal decompression procedures using wide range of instruments including microscope, microendoscope, tubular retractor, or full endoscopic spine surgery systems. These techniques have been proven to yield similar clinical outcomes when compared with conventional open techniques while allowing for less post-operative complications.8-13
Posterior endoscopic cervical foraminotomy or discectomy (PECF or PECD) is amongst the novel procedures accepted as a safe and efficient treatment of cervical radiculopathy. Similar to other minimally invasive surgical modalities, PECF or PECD is limited by the narrow surgical visibility. Thus, anatomical knowledge and spatial orientation of critical structures are crucial to safely performing PECF or PECD.
Ahn et al recommend structuring the surgical steps of PECF and PECD into 3 distinct stages. 11 Firstly, the full-endoscopic surgical instrument is precisely position on the laminar-facet junction. Secondly, foraminal unroofing is performed using endoscopic burrs and punches (endoscopic foraminotomy). Thirdly, a thorough disc and nerve root decompression under endoscopic visualization (full-scale endoscopic decompression).
In the second stage, exposure of the bony structures can be performed by removing soft tissues with radiofrequency coagulator and cutting forceps from the laminae and medial facet joint. The overlying tissues are removed until the medial junction of superior and inferior facet joints creating a “V point”, which is an important landmark for beginning of bone drilling, is clearly exposed. The post-operative complications of posterior percutaneous endoscopic cervical discectomy is reported as 3%–48%.
7
The adverse events such as nerve or dural injury, intraoperative bleeding, persistent symptom and segmental instability after surgery might be caused by poor surgical technique and the lack of knowledge about location of crucial anatomical structures in relation to the visible landmarks. Currently, the understanding of relationship between the V point and surrounding spinal and neural structures is still lacking. The insight from our study is summarized as shown in Figure 9 and should provide helpful information for preoperative planning and could possibly allow for better outcomes and less complications, including iatrogenic instability or inadequate decompression. 3D CT reconstruction of the estimated locations of V points, inferior border of intervertebral disc, and cervical nerve roots. The mean distance from nerve roots to inferior border of discs and V point were positive from C3-T1, suggesting a superior position of nerve roots. The distance increases from cranial to caudal level. Only V point of C6/7 and C7/T1 were located caudal to the disc.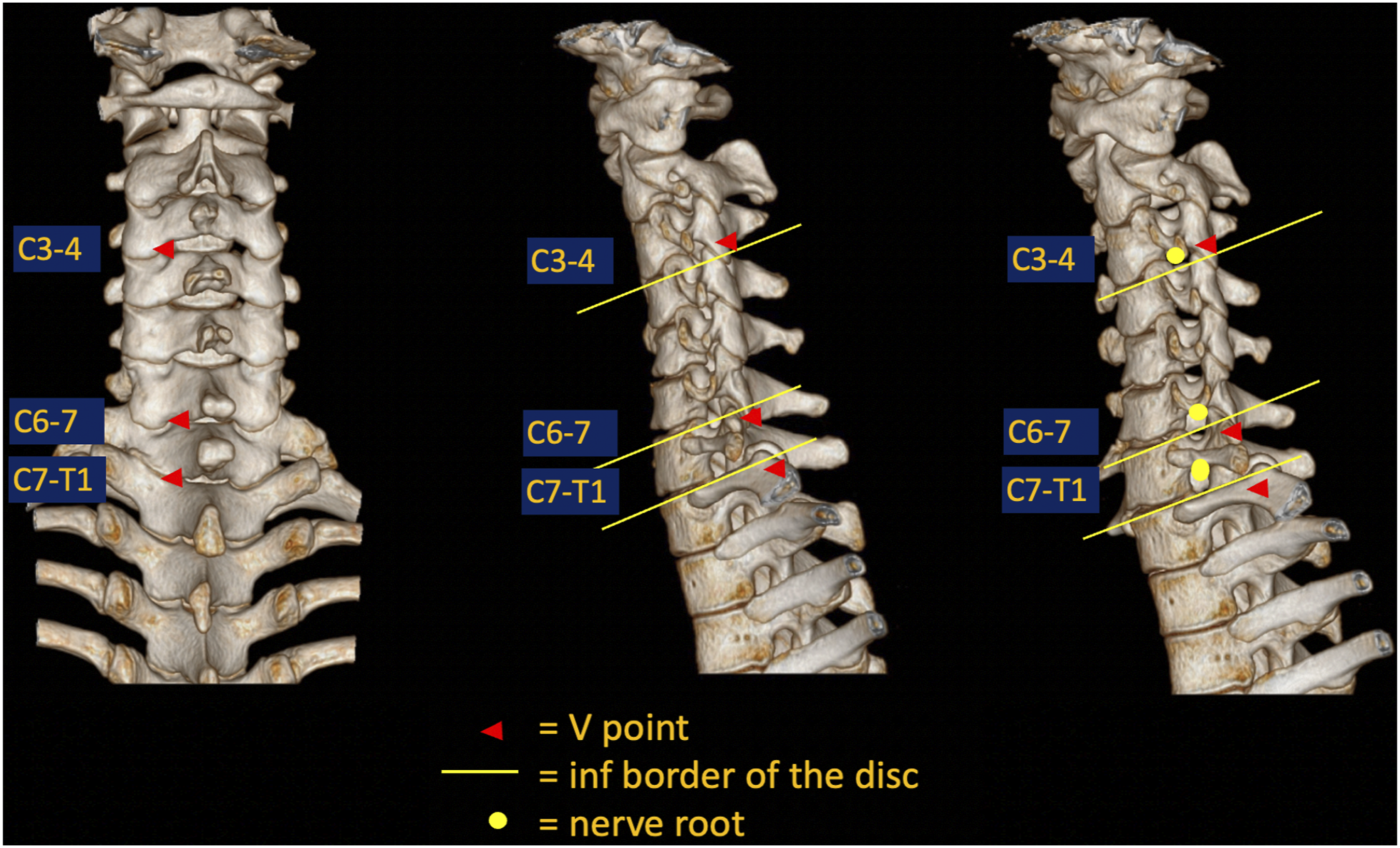
Barakat M et al 14 reported the horizontal distance from the medial part of facet joint to neural tissue after laminectomy to be ranging from 5.1 to 7.1 mm, increasing from C3/4 to C6/7. Thus, they recommended the removal of bone about 4-5 mm from the superior and inferior lamina to obtain good visibility of the dura. Furthermore, another 4-5 mm bony removal, laterally, from the lateral mass is needed to provide adequate exposure of the exiting nerve root for decompression and removal of herniated disc. Similarly, Kim CH et al suggested to remove about 3-4 mm radius of bone from the V point to adequately exposure nerve root, dural sac and intervertebral disc. 12 Both recommendations were comparable to our findings that the distance between the V point and the lateral margin of dural sac C3-4 to C7-T1 ranged from 3.1 ± 1.38 mm to 3.37 ± 1.46 mm. Thus, by removing a 3-5 mm radius of bone from the V point, surgeons should be able to adequately reach the lateral border of dural sac in mediolateral plane at all cervical levels.
The result in another imaging study was different from ours. Kim JY et al 15 studied relationship of the lateral dural edge and the V-point in 80 patients from MRI and CT scan. This study revealed that the location of the lateral edge dura in the relation to the V-point may have an age-related discrepancy due to the degenerative changes associated with aging. The author suggested that loss of disc height and loss of lordotic alignment leads to a narrowed anteroposterior diameter of the spinal canal, causing the lateral edge of dural and nerve root to be shifted more laterally. This effect is further enhanced in C5/6 and C6/7 levels and in patients aged in the 70s. Hence, the authors recommended a more extensive bony removal especially when performing PECF or PECD in in the more caudal cervical levels and in the older patients. We hypothesize that this contrary could be due to the shrinkage of neural and dural tissue in our study when compared with those of the living subjects. Nevertheless, the mentioned 3 studies did not evaluate the relation between the medial point of facet or the cervical nerve root with the intervertebral disc level.
In cranio-caudal plane, our result revealed that lower border of the nerve root is usually located cranially to V point. At C3/4 to C5/6, the lower border of the nerve root is located less than a millimeter cranial to the V point. At C6/7 and C7/T1, this interval is increased to about 2.5 to 4.5 mm. Tanaka N et al performed a cadaveric study of the cervical intervertebral foramina, nerve roots, and intradural rootlets under a surgical microscope. 16 They classified the anatomic relation between roots and the discs into 4 types; shoulder: when the disc is proximal to the root; anterior: when the disc is located just anteriorly to the root; axillary: when the disc is distal to the root; and no contact: when the disc does not have contact with the root. The shoulder and anterior types were identified more frequently at C5 and C6 roots, whereas the axillary and no contact types were more common at C7 and C8 roots. There was no axillary and no contact type at C5 root, and no shoulder and anterior type at C8 root. These observations are similar to that of our study. In our results, relation of the C4, C5 and C6 roots and the intervertebral disc are similar to shoulder or anterior type of Tanaka’s study. Furthermore, the location of C7 and C8 roots relative to the disc is similar to the axillary or no contact type. Finally, to adequately expose cervical nerve roots, we recommend removing the inferior part of the upper lamina further than the superior edge of the inferior lamina as the V point is located inferiorly to the nerve root and intervertebral disc. This is especially highlighted at the C6/7 and C7/T1 levels where the nerve roots might be totally covered by the upper laminar bone.
Nevertheless, the present study also has some limitations. Firstly, the number of cadaveric samples was limited. Secondly, the size and locations of neural structures may be affected by loss of body fluid in cadavers relative to that of the living subjects. Thirdly, the severity of degenerative changes in cadaveric samples are difficult to evaluate. Furthermore, the result illustrated is obtained from a neutral neck position. The presented distances and relationships may alter when surgery is performed in a flexed neck position. Thus, the application of the result of this study should be exercised with caution in the real-world patients, concerning for the anatomical relationship changes caused by neck position and anatomical alteration due to degenerative changes. Furthermore, the V point is a useful anatomic landmark as the starting point of decompressive bone work in which our study portrays the relationship of cervical nerve roots and intervertebral discs to this particular point. The treatment of radiculopathy can only be achieved when the bony removal is completed until the underlying nerve root is decompressed. At the same time, all attempts must be made to preserve 50 percent of the facet joint to prevent creating iatrogenic instability.
Conclusion
This study investigated the anatomical relationship between bony landmark “V point”, dural sac, cervical nerve roots and intervertebral disc. In the horizontal plane, a 3 to 4 mm bone removal radius from the V point is sufficient for the surgical exposure and adequate decompression of the neural structures. In the vertical plane, a 3 to 4 mm radius of bone removal should be enough at C3/4 and C5/6 levels. At C6/7 and C7/T1, a more extensive foraminotomy is recommended, with radius larger than 4 mm. Furthermore, surgeons should consider removing the inferior part of the upper lamina further than the superior part of the inferior lamina to obtain adequate exposure and neural decompression for cervical radiculopathy. This knowledge should be beneficial in enhancing outcomes and reducing complications in PECF and PECD where surgical visibility is limited, and a steep learning curve is required.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.