
Abstract
Study design
Scoping review.
Objective
To identify which markers are used as surrogates for malnutrition in metastatic spine disease and which are the most studied outcomes associated with it.
Methods
A scoping review was performed by searching the PubMed/Medline, EMBASE, and Web of Science databases up to July 2022. We searched for articles exploring markers of malnutrition in spine oncology patients including but not limited to albumin, body weight, weight loss, and nutrition indices. A narrative synthesis was performed.
Results
A total of 61 articles reporting on 31,385 patients met inclusion criteria. There were 13 different surrogate markers of nutrition, with the most common being albumin in 67% of studies (n = 41), body weight/BMI in 34% (n = 21), and muscle mass in 28% (n = 17). The most common studied outcomes were survival in 82% (n = 50), complications in 28% (n = 17), and length of stay in 10% (n = 6) of studies. Quality of life and functional outcomes were assessed in 2% (n = 1) and 3% (n = 2) of studies, respectively. Out of 61 studies, 18% (n = 11) found no association between the examined markers and outcome.
Conclusion
Assessment of nutritional status in patients with spinal metastases is fundamental. However, there is lack of a comprehensive and consistent way of assessing malnutrition in oncologic spine patients and therefore inconsistency in its relationship with outcomes. A consensus agreement on the assessment and definition of malnutrition in spine tumor patients is needed.
Introduction
Malnutrition affects 30 – 85% of cancer patients.1,2 Inadequate nutrition is known to impact the tolerability of chemotherapy, 3 radiation, 4 and surgery, 5 and it is also associated with shorter survival.6,7 Nevertheless, malnutrition is a multi-dimensional condition and diagnosing it can be challenging. Surrogate markers that are oftentimes used include hypoalbuminemia, weight loss, low body mass index (BMI), low muscle mass, and others. 8 To overcome this heterogeneity in assessment and diagnosis, leading nutrition societies in the United States and Europe have developed tools to standardize the definition of malnutrition and include items such as insufficient energy intake, weight loss, and loss of muscle mass. 9 However, implementation and adoption can be challenging given the multi-dimensional nature of these questionnaires/forms and the time-consuming factor.
The spine is the third most common site for metastatic spread after the lung and liver. By the year 2040, the World Health Organization estimates an incidence of 29 million cancer cases, out of which an estimated 16% (4.6 million patients) will develop symptomatic metastatic spine disease. 10 Patients with metastatic spine disease represent a unique and challenging sub-population of cancer patients given the predisposition to back pain, limited mobility, neurological deficits, and overall lower activity levels. The real prevalence of malnutrition in this population is unknown, but has been reported to be as high as 90%. 11 While studies have found significant associations between malnutrition and higher risk of complications and shorter survival,11,12 there remains a need for a consensus agreement on how best to define it and how it uniquely affects metastatic spine tumor patients.
Thus, the purpose of this scoping review was to: (1) Identify which markers are most used as surrogates for malnutrition in metastatic spine disease, and (2) describe the most studied outcomes associated with malnutrition in metastatic spinal tumor patients.
Materials and Methods
The current study was performed in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines. 13 This study did not require institutional review board approval since it is a review of the literature and not considered human subjects research. No informed consent was needed either.
Literature Search
An online search was performed by author RDLGR on July 26, 2022 in the PubMed/Medline, EMBASE, and Web of Science databases. No limits on publication dates or languages were applied. Initial searches were performed using a combination of keywords derived from the National Cancer Institute’s Nutrition in Cancer Care website – “malnutrition”, “weight loss”, “albumin”, “sarcopenia”, “muscle mass”, “cachexia”, “anorexia”, “visceral fat”, “subcutaneous fat” and “spinal metastasis”. 8 Specific search algorithms are shown in Supplementary Table 1.
Inclusion and Exclusion Criteria
Eligible studies included patients with metastatic spine disease. Studies investigating nutritional status and its association with clinical outcomes were included. Markers of nutritional status included nutritional screening tools or other health markers such as body weight, body mass index (BMI), weight loss, albumin, prealbumin, sarcopenia, muscle mass, and visceral fat. 8 The following type of studies were excluded: performance assessments, external validations, and comparisons of previously developed scoring systems; abstracts; case reports; editorials or commentaries; systematic reviews; and narrative reviews.
Study Selection
The study algorithm is shown in Figure 1. All retrieved studies were downloaded to an Endnote X9 (Clarivate, London, United Kingdom) libraries and duplicates were removed. Studies were first screened based on their title and abstract for potential eligibility based on our inclusion criteria. All potentially relevant studies were downloaded, and full texts reviewed. Any potential disagreements were resolved by consensus among authors RDLGR, JHS, CRG, RCM, and MHW. Study selection algorithm.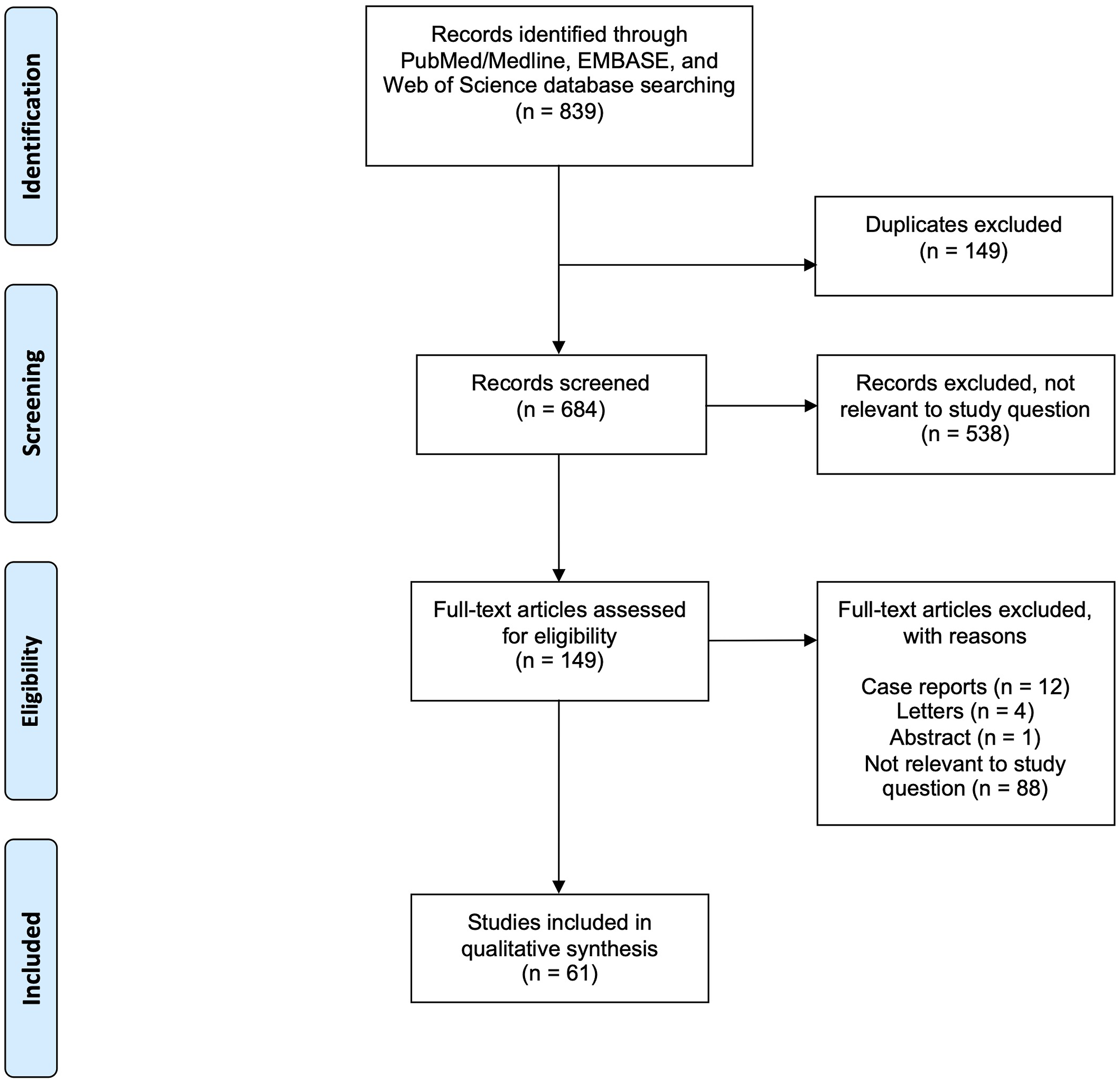
Primary and Secondary Questions
The primary question addressed which markers are most used as surrogates of malnutrition in patients with metastatic spine disease. The secondary question addressed which were the most common outcomes associated with malnutrition in patients with metastatic spine disease (such as survival, complications, length of hospital stay, and others).
Analysis
Explorative data analysis with descriptive statistics and a narrative review were performed. Levels of evidence were assigned based on the North American Spine Society guidelines.
Results
Characteristics of Included Studies.

Utilized Nutritional Markers
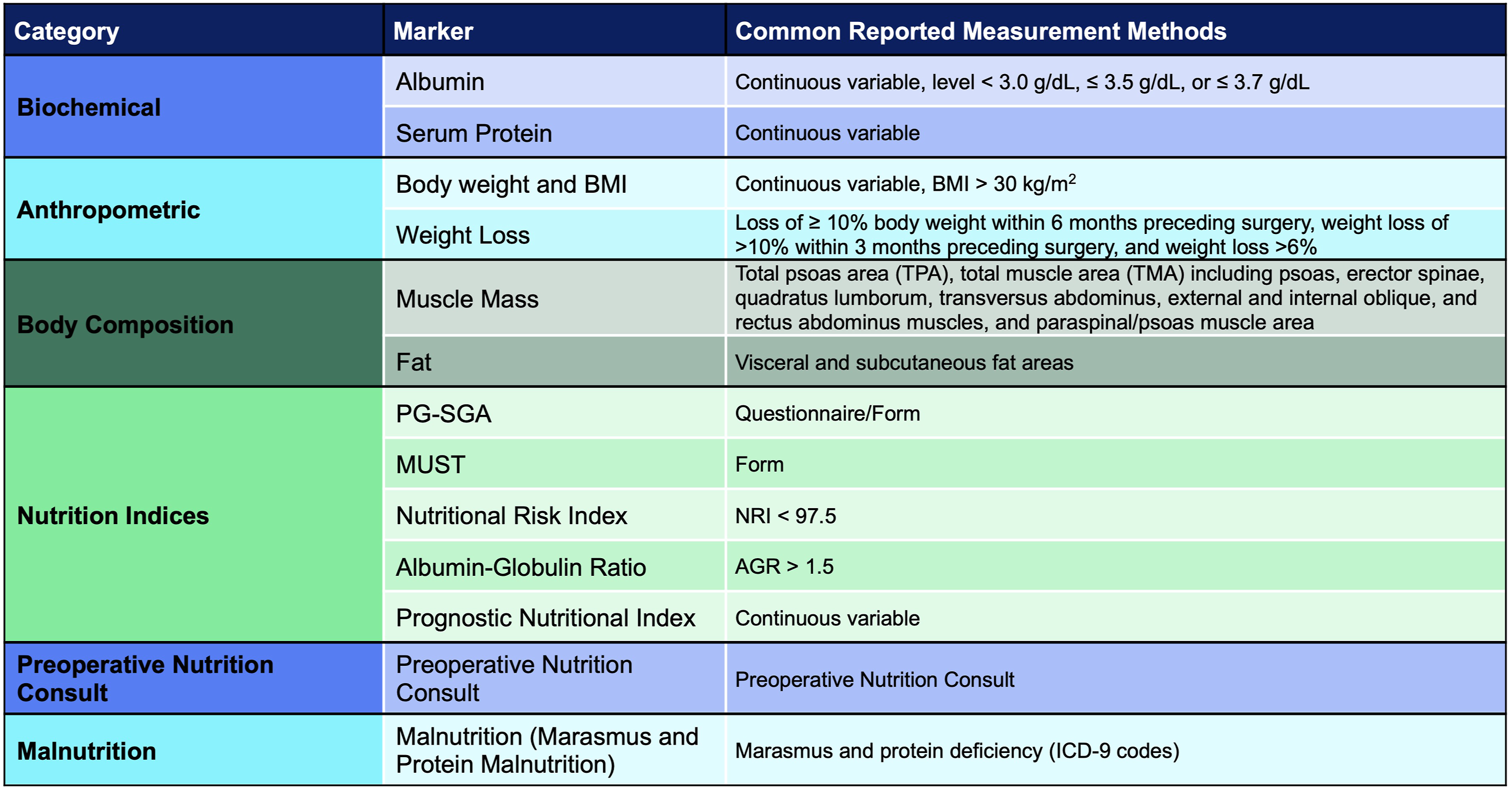
Data extraction revealed 13 different surrogate markers of nutrition (Figure 2); the most common was serum albumin in 67% of studies (n = 41),12,14,18-22,24,25,27-30,33-41,43-49,53-57,59,62,68,70-73 followed by body weight/BMI in 34% (n = 21),15,16,19,20,24,25,31-33,35,37,42,49,51,54,56,57,60,62,71,72 and muscle mass in 28% (n = 17). Among the 13 surrogate markers, these were subdivided into six categories (Figure 3). There were two biochemical markers (albumin and serum protein), two anthropometric measurements (body weight/BMI and weight loss), two measures of body composition assessed by imaging (muscle mass and fat), five nutrition indices (Patient-Generated Subjective Global Assessment, Malnutrition Universal Screening Tool Score, Nutritional Risk Index, albumin-globulin ratio, and Prognostic Nutritional Index), one study examining preoperative nutrition consults, and one study examining “malnutrition” (including nutritional marasmus and severe protein-calorie malnutrition) (Figure 3). Markers of nutrition and frequency. Markers of malnutrition and common methods of assessment.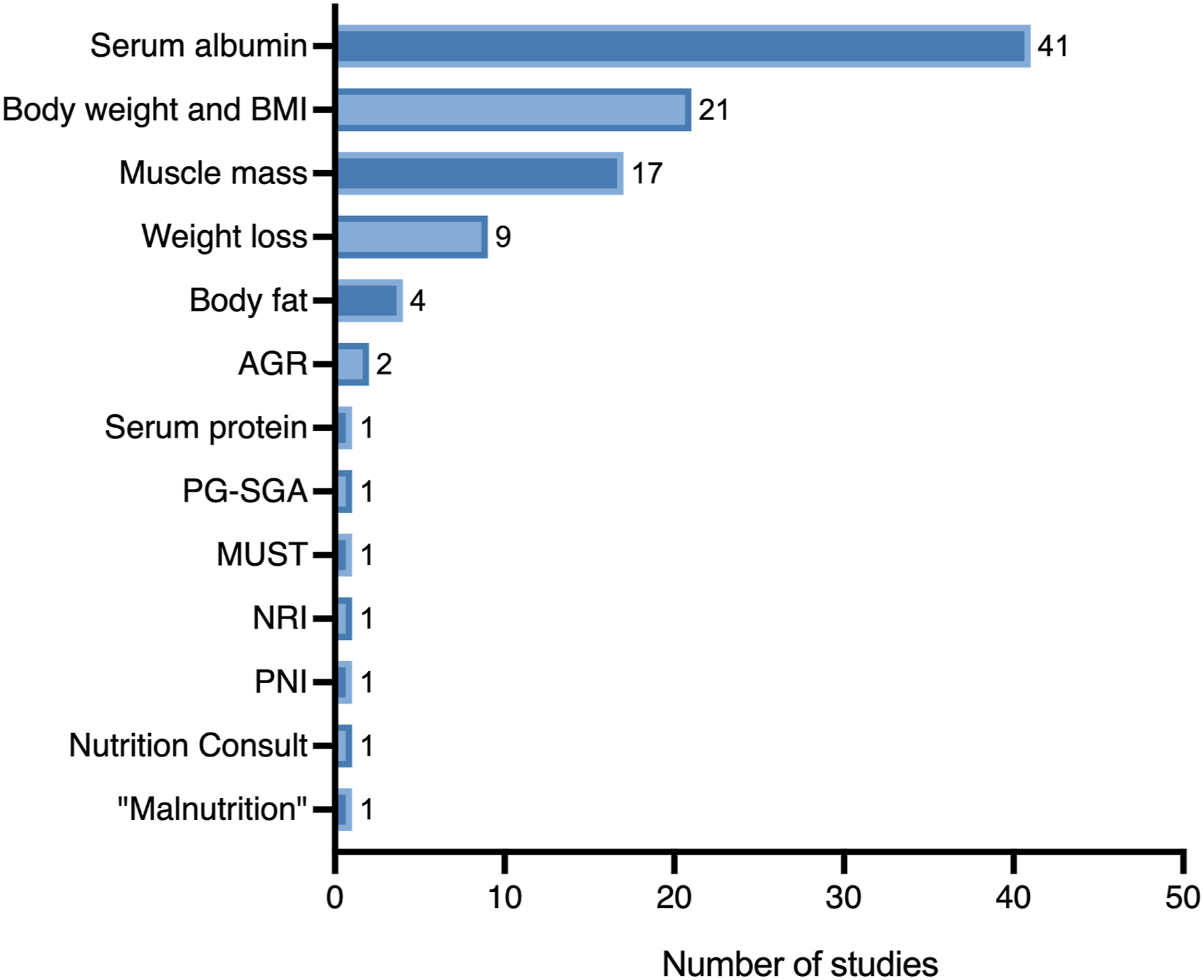
Outcomes
The examined outcomes were survival in 82% of studies (n = 50), complications (including wound complications) in 28% (n = 17), length of stay in 10% (n = 6), revision surgery in 5% (n = 3), functional outcome (one study examining postoperative Frankel grade and one study examining postoperative Eastern Cooperative Oncology Group performance status) in 3% (n = 2),40,60 discharge disposition in 3% (n = 2),25,33 postoperative ambulation in 2% (n = 1), 55 health-related quality of life outcome measures in 2% (n = 1), 11 and vertebral fracture progression in 2% (n = 1). 15 Out of 61 studies, 18% (n = 11) found no association between the examined markers and outcome on definitive (e.g. multivariate) analyses.14,29,30,37-40,43,57,61,68
Biochemical Markers
Serum albumin was the most studied biochemical marker.12,14,18-22,24,25,27-30,33-41,43-49,53-57,59,62,68,70-73 However, there was wide variability in how this was assessed, with studies examining albumin as a continuous variable and others defining hypoalbuminemia as a level <3.0 g/dL, ≤3.5 g/dL, or ≤3.7 g/dL. Most studies examined the association between albumin and survival, but few also examined the association between albumin and wound complications,39,44 and albumin and ambulatory outcome, 55 for example. Out of 47 studies examining albumin, 79% (37 of 47) found a significant association between albumin and the studied outcome (predominantly survival); the remaining 21% of studies found no association. Serum protein levels were assessed in one study that found that patients who had a wound infection after oncologic surgery had lower serum protein levels compared to controls. 44
Anthropometric Measures
Body weight and BMI were the second most studied markers in our review.15,16,19,20,24,25,31-33,35,37,42,49,51,54,56,57,60,62,71,72 Like albumin, there was variability on assessment methods, with studies examining BMI as a continuous variable and others at specific thresholds such as BMI >30 kg/m2. Weight loss was also assessed in 15% of studies (n = 9).14,19,31,33,37,58,62,71,72 Definitions of “weight loss” included loss of ≥10% body weight within 6 months preceding surgery, weight loss of >10% within 3 months preceding surgery, 19 and weight loss >6%. 62 Out of 21 studies examining BMI, only 10% (2 of 21) found an association between BMI and pathologic fracture progression 15 or survival. 51 Out of 9 studies examining weight loss, 33% (3 of 9) found an association between weight loss and outcome.31,58,62
Body Composition Measures
Body composition measures included muscle mass and body fat assessed on perioperative computed tomography scans or MRI. Many different methods were used to assess muscle mass, including total psoas area (TPA) at the L3 or L4 level by itself or as a ratio in relationship to the vertebral body (TPA/VB),17,21,22,26,32,60,63-67 total muscle area (TMA) including psoas, erector spinae, quadratus lumborum, transversus abdominus, external and internal oblique, and rectus abdominus muscles,42,43,51,52 and paraspinal/psoas muscle area.16,23 All studies examining muscle mass studied the association with survival; one also studied the association with complications 17 and another with length of stay. 42 Out of 17 studies examining muscle mass, 88% (15 of 17) found an association with outcome, mainly postoperative survival. Four studies looked at body fat composition.16,42,51,52 Body fat was assessed via measurement of visceral and subcutaneous fat areas, and 50% of these studies (2 of 4) found an association with outcome.
Nutrition Indices
Nutrition Indices.
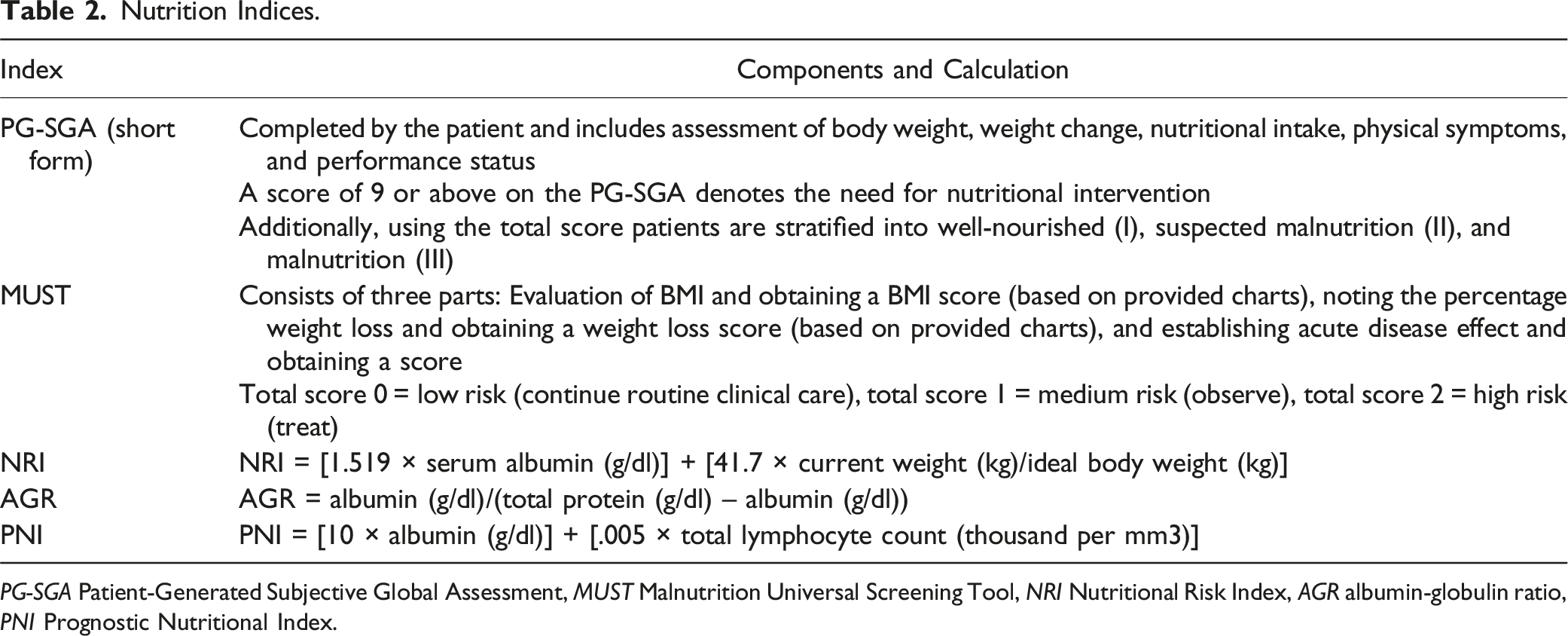
PG-SGA Patient-Generated Subjective Global Assessment, MUST Malnutrition Universal Screening Tool, NRI Nutritional Risk Index, AGR albumin-globulin ratio, PNI Prognostic Nutritional Index.
Preoperative Nutrition Consult
The utility of obtaining a preoperative nutrition consult in metastatic spine disease was evaluated in one study. 24 Authors compared outcomes of 17 patients who received a preoperative nutrition consult to 78 who did not, finding that patients in the nutrition consult group had had lower rates of 30-day morbidity and shorter hospital stays. However, no information regarding the indication for the nutrition consult or the intervention/optimization performed after patients received the consult was disclosed.
Malnutrition
One study of a national inpatient database in the United States examined “malnutrition” as a broad term and its association with complications, in-hospital mortality, and length of stay. 12 Malnutrition was defined based on ICD-9 codes and included a composite measure of patients with diagnoses of protein malnutrition and marasmus. Malnutrition was significantly and independently associated with the examined outcomes and was then incorporated into a “frailty index”. 12
Sub-Analysis Based on Cancer Type
As mentioned earlier, 10 studies focused on a single cancer type (Table 1). Among these, three studies examined outcomes in lung cancer,46,63,68 one on lymphoma, 30 two on renal cell carcinoma,38,43 two on breast cancer,65,69 and one on hepatocellular carcinoma. 59 For patients with lung cancer undergoing surgery, Ogihara et al. found an association between hypoalbuminemia and survival, 46 while Zang et al. found none. 68 On the other hand, Zakaria et al. found an association between low muscle mass and survival after radiation therapy. 63 For patients with renal cell carcinoma, one study found no association between albumin <4.0 g/dL with survival after surgery, 38 and another study found no association between the PNI or low muscle mass with outcome after multivariate analysis. 43 Lastly, for patients with breast cancer one study found an association between the albumin-globulin ratio and survival after multimodal treatment 69 and another between low muscle mass and survival after radiation therapy. 65
Discussion
Malnutrition is highly prevalent in cancer patients. For patients with metastatic spine disease, a malnourished or undernourished state can result in decreased tolerability to surgery, a higher risk of perioperative complications, and limited survival, among others. In this scoping review, we identified 61 manuscripts examining 13 different surrogate markers for malnutrition, finding that most studies found a significant association between malnutrition and the examined outcomes, which in most cases was survival.
The first step in evaluating the prevalence and risk of malnutrition in patients with metastatic spine disease is to critically appraise the tools and criteria for assessment. In general terms, malnutrition in cancer is considered a form of disease-related malnutrition with inflammation, 75 defined as “a state resulting from lack of intake or uptake of nutrition that leads to altered body composition (decreased fat free mass) and body cell mass leading to diminished physical and mental function and impaired clinical outcome from disease.” 76 The European Society for Clinical Nutrition and Metabolism (ESPEN) requires that prior to a diagnosis of malnutrition, patients need to be considered at risk according to any validated nutritional risk screening tools. Patients need to have a BMI <18.5 kg/m2 or unintentional weight loss (>10% over an indefinite amount of time or >5% over last 3 months) in addition to reduced BMI (using age-dependent cut-offs) or reduced gender-dependent fat free mass index. 75 On the other hand, the American Society of Parenteral and Enteral Nutrition (ASPEN) and the Academy of Nutrition and Dietetics (Academy) classify patients as “malnourished” when two of the following criteria are met: low energy intake, weight loss, loss of muscle mass, loss of subcutaneous fat, fluid accumulation, and/or hand grip strength. 75 In our review, however, none of the examined studies used any of these aforementioned criteria.
Malnutrition in Spine Oncology
In patients with metastatic spine disease, there has been limited research on the impact of malnutrition (as defined by ESPEN, ASPEN, or Academy) on outcomes. Rather, multiple different surrogate markers have been studied, some as single prognostic factors and others as part of nutrition indices. Our scoping review found that 67% of studies used albumin as a biomarker of nutritional status, followed by body weight/BMI in 34%, and muscle mass in 28%.
Albumin is the most abundant serum protein in humans and has been used for decades as an indicator of malnutrition. 77 In cancer patients, it is also widely accepted that pretreatment hypoalbuminemia (i.e. albumin levels before chemotherapy, radiotherapy, or surgery are undertaken) is associated with decreased survival. 7 Our review showed that out of 47 studies examining albumin, 79% (37 of 47) found a significant association between albumin levels and survival, complications, postoperative ambulation, readmissions, and others. The remaining 21% of studies found no association between albumin levels and the studied outcomes. Nonetheless, one of the main criticisms of using albumin as a proxy marker for malnutrition is that its concentration is also affected by age, inflammation, kidney disease, and GI disease, among others. 78 While hypoalbuminemia can be seen in patients who are malnourished, low albumin levels can also be seen in the context of physiologic stress as a result of disease or inflammation. 79 As such, albumin should be considered a nutritional-inflammatory marker and using it alone as a surrogate marker for nutritional status may not always be appropriate.
Body weight/BMI and a history of weight loss (i.e., anthropometric measures) were the second most common markers found in our review. These are both components of the ESPEN/ASPEN/Academy criteria, but there was wide variability on how studies assessed Body weight/BMI and weight loss. Furthermore, only 10% of studies examining BMI and 33% of studies examining weight loss found a significant association with the studied outcome, suggesting that using these parameters as single prognostic tools may not be appropriate. Measures of body composition such as muscle mass and body fat were described in 17 and 4 studies, respectively. Assessment was typically performed on perioperative imaging studies and many different methods were used. Muscle mass was most consistently associated with survival, with 88% (15 of 17) of studies reporting a significant association between low muscle mass and outcome. While muscle mass seems promising, its use in a clinical setting remains challenging. No clear threshold for low muscle mass has been defined. Additionally, while some of these measures can be performed easily (for example TPA/VB) others requires advanced software analysis.
Nutrition indices and questionnaires were among the least examined markers of malnutrition, despite them being considered more “objective” measures. Indices are calculated based on common laboratory markers such as albumin level or lymphocyte count. On the other hand, the PG-SGA short form and the MUST score are more traditional questionnaires/forms that can be time-consuming. Interestingly, malnutrition as defined by the PG-SGA score was only associated with worse quality of life but not survival in one study. 11 Similarly, malnutrition defined by the MUST score was not associated with wound complications. 39 Incorporation of indices and questionnaires can be understandably hard to obtain given the emergent nature of spinal cord compression. However, surgeons and mid-level providers can consider obtaining these measures as an inpatient, with serial follow-up in clinic postoperatively.
Implications for Clinical Practice
Other than malnutrition, cancer patients are often afflicted or at risk for frailty and sarcopenia. These three conditions frequently overlap and as seen in this review, many markers such as weight loss and decreased muscle mass are common to more than one of these conditions. Frailty corresponds to a state of abnormal homeostasis leading to increased vulnerability to stressors that can occur independent of advanced age. It is characterized by an accumulation of health deficits as seen in indices such as the Metastatic Spinal Tumor Frailty Index. 12 Sarcopenia refers to a syndrome characterized by both loss of muscle mass and loss of strength/function. While many studies refer to low muscle mass as “sarcopenia”, many fail to objectively assess muscle strength and function. It is a manifestation of frailty and is also referred to as cancer cachexia.
It is evident that malnutrition is also seen in frail and sarcopenic patients and further work into achieving a consensus definition in spine oncology is needed. Our review showed that albumin, body weight, and BMI were the most employed proxies for malnutrition. These variables are generally collected in most institutional databases, which explains their popularity. However, we believe that these are not reflecting the true nutritional status and therefore, should not be used in isolation to define malnutrition. Further research into the utilization of ESPEN/ASPEN/Academy criteria is needed, as well on the possible correlation between these and other markers of malnutrition. A study performed at an urban underserved cancer center found correlations between the Prognostic Nutritional Index and Nutritional Risk Index, Nutritional Risk Index and BMI, and Nutritional Risk Index and body weight, among others. 80 Given that some of the objective measures such as the PG-SGA may be time-consuming and difficult to implement in an emergency setting, research into the correlation of these measures and common laboratory markers/indices may reveal that they are perhaps correlated with one another and thus easier to utilize for prediction. Furthermore, the appropriateness of using some of these parameters such as albumin as markers of malnutrition needs to be reassessed, given they can also overlap with inflammation, older age, and illness.
One of the most interesting findings in our review is the very limited data on the impact of these markers/malnutrition on other important outcomes such as quality of life or ambulatory status. While most studies focused on overall survival, the impact of malnutrition on wound complications, tolerability of physical therapy, on the likelihood of postoperative ambulation, on the levels of postoperative pain, and on quality of life, among others, is something that remains unanswered.
Lastly, perioperative optimization, when feasible, may also have a role in improving outcome of patients undergoing treatment for spinal metastases that are considered as being at risk of or already suffering from malnutrition. A nutritional surveillance program could identify and treat symptoms such as nausea, vomiting, anorexia, and dysphagia in a timely manner. Depending on the degree of malnutrition, a stepwise approach could include optimizing regular food intake, food fortification with micro- and macronutrients, protein powder, oral nutritional supplements, parenteral nutrition, enteral nutrition, and others. 81 Nonetheless, patients presenting with symptomatic cord compression may not have the time for optimization, and thus malnutrition may not be a modifiable risk factor. In these urgent instances, identification of preoperative malnutrition may aid in counseling, expectations, risk stratification, and perhaps clinical decision making. On the other hand, nutritional counseling with inpatient dietitians for the immediate postoperative period can be considered and may also have the potential to improve outcomes, though this is an area that certainly requires more research.
Limitations
There are several limitations to this study. Given the heterogeneity of markers, thresholds, cancer diagnoses, and treatments, a meta-analysis was not possible. Even when attempting to focus on a single tumor type on our sub-analyses, there was variability in the surrogate markers used to identify nutritional status, as well as the type of intervention and outcomes evaluated. The quality of studies was also a limiting factor, given that the vast majority (89%) were retrospective cohort studies. The studied outcomes were also varied, but most focused on survival and complications; very few studies examined other outcomes including functional status or quality of life. Few studies have assessed the impact of malnutrition in spine oncology in a prospective fashion and it is certainly an area of opportunity for future research.
Conclusion
While the association between malnutrition and poor outcomes in the spine metastatic population is intuitive, our review of the literature has demonstrated the lack of a comprehensive and consistent way of assessing malnutrition and therefore the inconsistency in its relationship with outcomes. The most employed proxies for malnutrition were albumin and body weight/BMI. We believe these measures in isolation should not be used to define malnutrition as they do not capture the complexity of nutritional status. Given the absence of strong evidence towards the utilization of any single biomarker as a surrogate for malnutrition, our recommendation based on the current available evidence would be to employ and research objective evaluations such as those outlined by the ESPEN/ASPEN/Academy when feasible, followed by nutrition indices such as the PG-SGA or PNI. However, a consensus agreement on the assessment and definition of malnutrition in spine tumor patients has not been reached and warrants further investigation.
Supplemental Material
Supplemental Material - Malnutrition in Spine Oncology: Where Are We and What Are We Measuring?
Supplemental Material for Malnutrition in Spine Oncology: Where Are We and What Are We Measuring? by Rafael De la Garza Ramos, Raphaële Charest-Morin, C Rory Goodwin, Scott L Zuckerman, Ilya Laufer, Nicolas Dea, Arjun Sahgal, Laurence D Rhines, Ziya L Gokaslan, Chetan Bettegowda, Anne L. Versteeg, Hanbo Chen, Cordula Netzer, Daniel M Sciubba, John E O’Toole, Michael G Fehlings, Naresh Kumar, Alexander C Disch, Byron Stephens, Tony Goldschlager, Michael H Weber, John H. Shin in Global Spine Journal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Tumor, a focused group of international Tumor experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.