
Abstract
Study Design:
Retrospective review of prospective database.
Objective:
Complication rates for adult spinal deformity (ASD) surgery vary widely because there is no accepted system for categorization. Our objective was to identify the impact of complication occurrence, minor-major complication, and Clavien-Dindo complication classification (Cc) on clinical variables and patient-reported outcomes.
Methods:
Complications in surgical ASD patients with complete baseline and 2-year data were considered intraoperatively, perioperatively (<6 weeks), and postoperatively (>6 weeks). Primary outcome measures were complication timing and severity according to 3 scales: complication presence (yes/no), minor-major, and Cc score. Secondary outcomes were surgical outcomes (estimated blood loss [EBL], length of stay [LOS], reoperation) and health-related quality of life (HRQL) scores. Univariate analyses determined complication presence, type, and Cc grade impact on operative variables and on HRQL scores.
Results:
Of 167 patients, 30.5% (n = 51) had intraoperative, 48.5% (n = 81) had perioperative, and 58.7% (n = 98) had postoperative complications. Major intraoperative complications were associated with increased EBL (P < .001) and LOS (P = .0092). Postoperative complication presence and major postoperative complication were associated with reoperation (P < .001). At 2 years, major perioperative complications were associated with worse ODI, SF-36, and SRS activity and appearance scores (P < .02). Increasing perioperative Cc score and postoperative complication presence were the best predictors of worse HRQL outcomes (P < .05).
Conclusion:
The Cc Scale was most useful in predicting changes in patient outcomes; at 2 years, patients with raised perioperative Cc scores and postoperative complications saw reduced HRQL improvement. Intraoperative and perioperative complications were associated with worse short-term surgical and inpatient outcomes.
Keywords
Introduction
The rise in adult spinal deformity (ASD) diagnoses and procedures in the United States reflects the rising population and increased surgical intervention for the management of the condition. 1 -5 There are multiple ASD etiologies, including degenerative scoliosis, iatrogenic deformity, and multiplanar malalignment/imbalance. Surgical correction and decompression can improve outcomes and patient satisfaction, even in higher risk individuals, including elderly patients. 4 But ASD retains elevated overall complication rates, which have yet to be shown to predict outcome measures. 6,7 Improved complication grading may provide a more accurate reflection of the impact of adverse events on ASD patients, thereby optimizing treatment. 8
Complication rates for ASD reported in the literature vary. 9 -11 The recent ASD literature review by Nasser et al 12 identified a thoracolumbar complication incidence range of <1% to 70%. More typical estimates, though, usually range from 8% to 40%. 13 -17 This variability may be explained by the lack of standard outcome assessment in spine surgery and the diversity in methodology of classifying and reporting specific procedure-related complications. 12,18 With ASD’s complexity, and as complication reporting varies by practice, opportunities are missed to improve the quality of care. 18,19 Moreover, ASD procedure-related complications do not have a clear impact on patient-reported health-related quality of life (HRQL) scores. For example, Uribe et al 14 failed to elicit a significant link between sustaining a complication during ASD surgery and final Oswestry Disability Index (ODI) score, whereas Glassman et al 20 reported that ASD complications adversely affected postoperative Short Form-12 scores.
Complication grading in ASD surgery should accurately reflect the potential impact on patient outcomes. Multiple methods of reporting procedure-related complications have been attempted, with varying levels of success. Authors have distinguished, for example, between specific complication type (medical vs surgical) and severity (minor-major). 21,22 More comprehensive systems have also been implemented to standardize classifications: in 2004, Dindo et al 23 expanded on Clavien’s classification system and proposed a standardized scale from I (minor; not increasing hospital stay) to V (death), characterizing complications by their impact. 23,24 The Clavien-Dindo system has been successfully implemented in a variety of surgical settings, including spine, as reported by Huang et al. 25
This study aimed to determine the impact of multiple ASD procedure-related complication classification methods on surgical and patient-reported outcomes. Complications were grouped using the Clavien-Dindo Scale and the minor-major distinction to quantify the impact of complications on outcomes in an ASD surgical setting.
Materials and Methods
Study Design and Inclusion Criteria
This study is a retrospective review of a prospective multicenter database that was composed of consecutively enrolled ASD patients from 11 US-based sites. Prior to study initiation, institutional review board approval was obtained at all participating sites. Patients undergoing ASD corrective thoracolumbar surgery were enrolled according to the following criteria: radiographic determination of ASD (age >18 years, scoliosis ≥20°, sagittal vertical axis ≥5 cm, pelvic tilt ≥25°, and/or thoracic kyphosis >60°), with complete demographic, surgical, and radiographic data at baseline and 2 years postoperatively.
Complications Classification and Categorization
In this database, any complications experienced were organized according to the following groups: cardiopulmonary, gastrointestinal, implant, infection, musculoskeletal, neurological, operative, other, radiographic, renal, vascular, and wound. Complications as a result of the index surgery at enrollment were considered at 3 surgical stages: intraoperative, perioperative (<6 weeks of index), and postoperative (>6 weeks of index). At each stage, complications were classified into 3 different groups by the enrolling surgeon: complication presence (yes/no), minor or major, and by Clavien-Dindo score assigned to the complication. Minor-major complication designation was assigned according to criteria in previously published literature (Appendix A). 20 Patients with an estimated blood loss (EBL) ≥4 L were excluded from analysis of intraoperative EBL in order to analyze the impact of other complications on this factor. The Clavien-Dindo complication classification (Cc) is a 1 to 5 complication scale: 1, any deviation from normal postoperative course; 2, complication requiring modest pharmacological treatment; 3, requiring surgical, endoscopic, or radiological intervention (dependent on actually receiving the intervention); 4, life-threatening requiring intensive care unit management; 5, death as a result (Appendix B).
Data Collection
Patient data was recorded by surgeons on standardized data collection sheets and collected in a multisurgeon database. Surgical variables, including EBL, length of hospital stay (LOS), reoperation requirement, operative time, and number of levels fused were collected and analyzed. HRQL scores were collected at baseline visit and at each follow-up time point (6 weeks, 1 year, and 2 years postoperatively). The following HRQL scores were collected: ODI, Short Form Health Survey with associated Mental Component Summary and Physical Component Summary (PCS), and Scoliosis Research Society (SRS-22r) Questionnaire Activity (AC), Pain (P), Appearance (AP), Satisfaction (S), Mental (M), and Total (T) scores.
Statistical Analyses
For comparisons between groups for demographic and operative variables, Student t-tests and χ2 analyses were used. Using baseline to 2-year data, 2-way or univariate ANOVA analyses were used to determine the impact of complication presence, complication type (minor-major), and Cc grade on operative variables and postoperative HRQL scores. All statistical analyses were done using “no complication” as a reference group. Adjusting for possible confounding factors and loss to follow-up, the complication schemes that were compared all used the same cohort of patients. Statistical analyses were performed using SPSS 20.0 (IBM Corp, Armont, NY) and R Statistical Package (R Core Team, Vienna, Austria). 26
Results
Patient and Complications Overview
Of 558 eligible surgical ASD patients in the database, this study included 167 with required complete data (147 female, 20 male). Of those lost, 297 patients did not reach the 2-year follow-up, and 104 did not receive Clavien-Dindo scores by the enrolling surgeons. Complications are summarized in Table 1: 51 (30.5%) patients sustained an intraoperative complication, 81 (48.5%) a perioperative complication, and 98 (58.7%) a postoperative complication.
List of Most Commonly Experienced Complication Categories and Specific Complication Subtype Frequencies Per Operative Period (Intraoperative, Perioperative, Postoperative) Broken Down by Severity (Minor-Major).
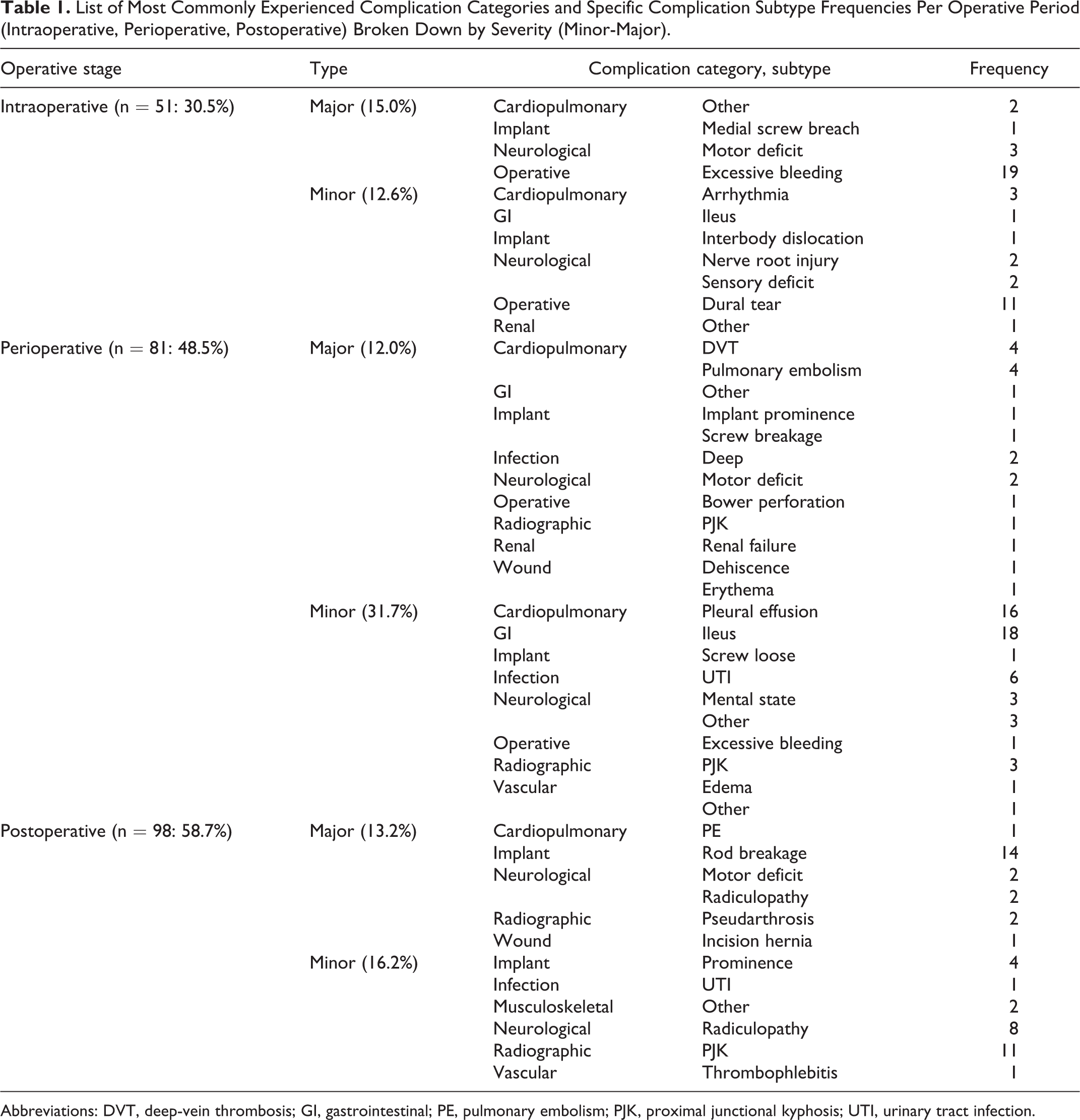
Abbreviations: DVT, deep-vein thrombosis; GI, gastrointestinal; PE, pulmonary embolism; PJK, proximal junctional kyphosis; UTI, urinary tract infection.
Table 1 presents a summary of the most prevalent complications encountered in the patient sample, organized by operative period, complication category, and subtype. The most frequent types of intraoperative complications were operative (n = 43, 84.3%), specifically excessive bleedings (n = 19, 41.2%) and dural tears (n = 11, 21.6%). Perioperatively, cardiopulmonary pleural effusions (n = 16, 19.8) and gastrointestinal ileus (n = 18, 22.2%) were the most frequently recorded complications. Among all postoperative complications reported, implant-related rod breakages (n = 14, 14.3%) and radiographic proximal junctional kyphosis (n = 11, 11.2%) were the most prevalent.
Surgical Summary
A summary of operative characteristics of the cohort based on complication subtype is available in Table 2. Across all surgical periods, there were 91 major (54.5%) and 87 minor (52.1%) complications recorded. Reoperations were observed in 40 (24.0%) cases of the total study cohort. A total of 19 patients (11.3%) had an intraoperative blood loss ≥4 L, a major complication, and were therefore excluded from analyses relating to intraoperative EBL. The mean patient age was 57.96 ± 13.82 years (range: 19-86 years), and the average body mass index was 27.74 ± 5.92 kg/m2 (range: 17.49-54.15 kg/m2). At baseline presentation, there were 71 (42.5%) patients with osteoarthritis, 66 (39.5%) with hypertension, and 22 (13.2%) with osteoporosis. The index procedure involved an average of 11.52 levels operated on, with the median uppermost vertebra at T10 (20.2%).
Description of Operative Variables by Complication Severity (Minor-Major) and Clavien-Dindo Scale (1-5).
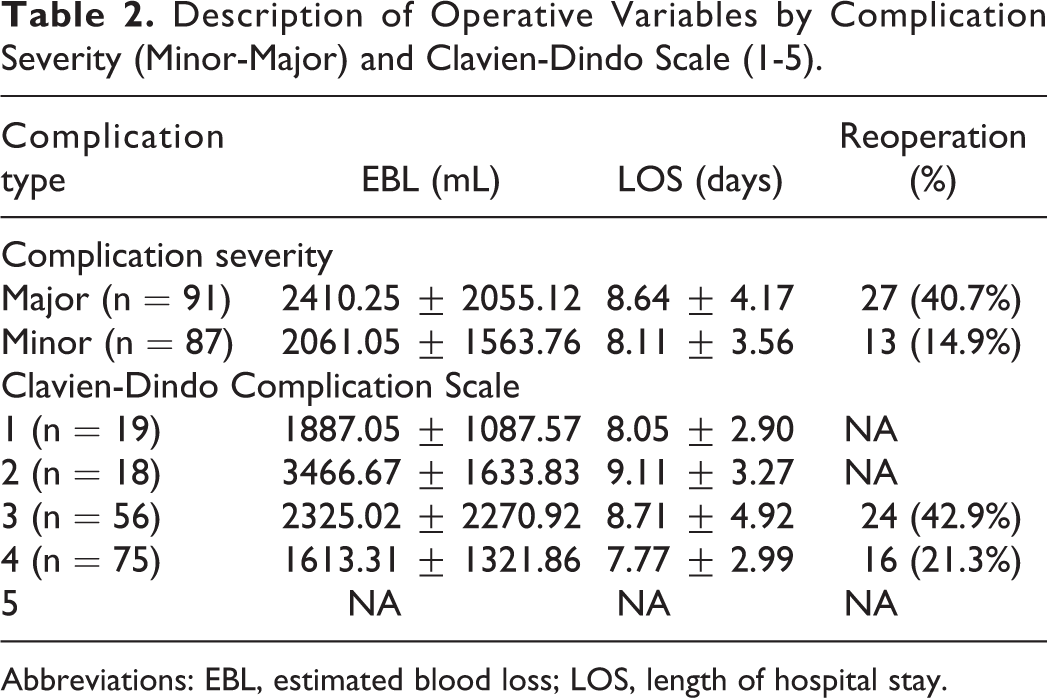
Abbreviations: EBL, estimated blood loss; LOS, length of hospital stay.
Complication Presence
Table 3 displays the results of the analysis for associations between complication presence and surgical variables. The presence of an intraoperative complication was determined to be associated with an increase in EBL (P < .001) relative to the no complications reference group. The presence of both intraoperative and perioperative complications were associated with a decrease in reoperative risk (P = .012 and P = .036, respectively); postoperative complication presence, however, was associated with an increased reoperation risk (P < .001).
Univariate Analyses for Association of Complication Presence (Y/N) at 3 Considered Surgical Stages (Intraoperative, Perioperative, Postoperative) with EBL, LOS, and Reoperation.a
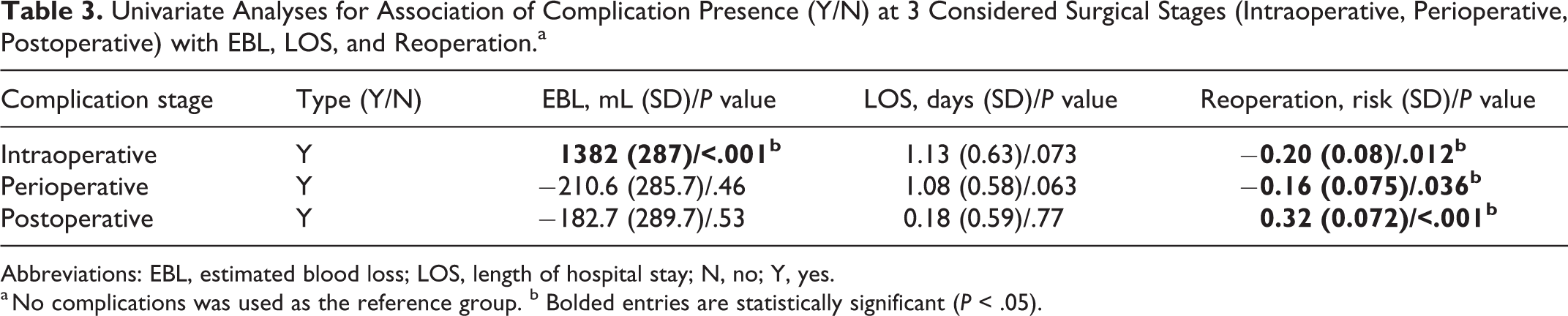
Abbreviations: EBL, estimated blood loss; LOS, length of hospital stay; N, no; Y, yes.
a No complications was used as the reference group. b Bolded entries are statistically significant (P < .05).
Surgical Invasiveness
Analysis of measures of surgical invasiveness found that patients who experienced major complications had a greater number of Smith-Petersen osteotomies (P = .034) and 3-column osteotomies (P = .007). However, there was no similar correlation between major complications and levels fused or operative time: patients who did and did not have a major complication had 11.61 versus 11.34 average levels fused (P = .738) and averaged 429.9 versus 398.5 minutes in the operating room (P = .255).
Minor-Major Complications
Table 4 presents the results of univariate analyses for impact of major and minor complications against a “no complications” reference group. Minor intraoperative complications were associated with decreased reoperation risk (P = .019), whereas major intraoperative complications were linked to increased EBL (P < .001) and LOS (P = .009). Intuitively, a major postoperative complication was associated with an increased reoperation risk (P < .001).
Univariate Analyses for Association of Major Versus Minor Complication Presence at 3 Considered Surgical Stages (Intraoperative, Perioperative, Postoperative) With EBL, LOS, and Reoperation.a
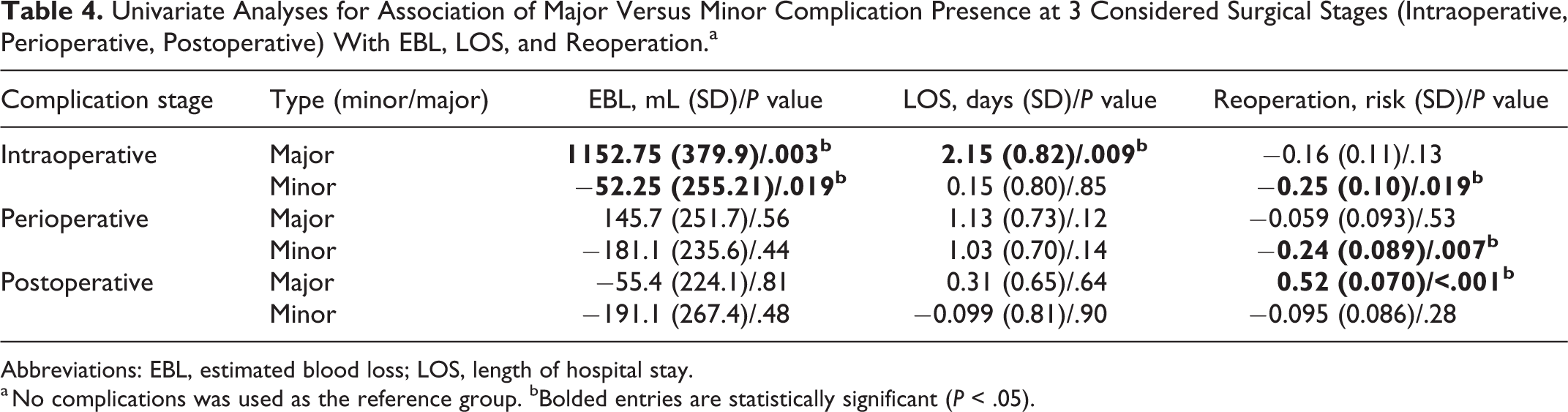
Abbreviations: EBL, estimated blood loss; LOS, length of hospital stay.
a No complications was used as the reference group. bBolded entries are statistically significant (P < .05).
Clavien-Dindo Classification Complications
Figure 1 displays the distribution of Cc grade scores across the 3 considered surgical stages. There was a statistically significant difference in the number of perioperative and intraoperative complications (P = .001) as well as between perioperative and postoperative complications (P < .001), and between intraoperative and postoperative complications (P < .001). Specifically, the 3 most prevalent Cc scores observed in this cohort were as follows: postoperative Cc 4 (n = 58, 59.2% of all postoperative complications), postoperative Cc 3 (n = 34, 34.7% of all postoperative complications), and perioperative Cc 4 (n = 32, 39.5% of all perioperative complications). Table 5 displays the results for the analyses of Cc score and considered surgical variables. Patients with intraoperative Cc 2 were associated with increased LOS (P = .03). However, intraoperative Cc 4 was associated with decreased reoperation (P = .041). Perioperative complications assigned a Cc score 1 were associated with decreased reoperation risk (P = .026), and those with a Cc 3 score demonstrated increased LOS (P = .017).
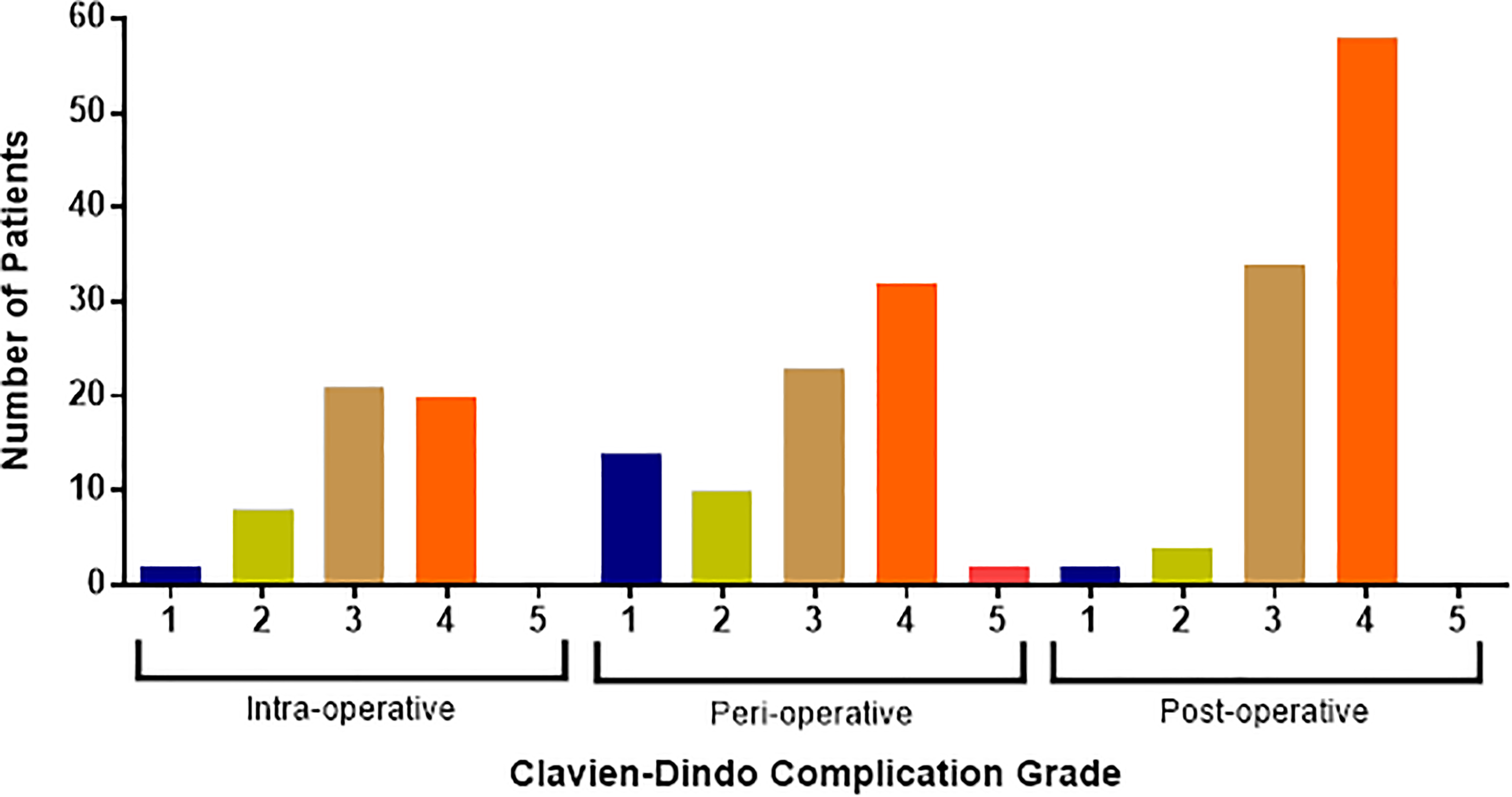
Distribution of intraoperative, perioperative, and postoperative complications experienced based on Clavien-Dindo Classification (Cc) score: (1) minor, (2) potentially life-threatening, (3) potentially life-threatening needing reoperation, (4) associated with residual disability, (5) death as a result.
Univariate Analyses for Association of Clavien-Dindo Classification (Cc) Score for Complications Based on Considered Surgical Stages (Intraoperative, Perioperative, Postoperative) With EBL, LOS, and Reoperation.a
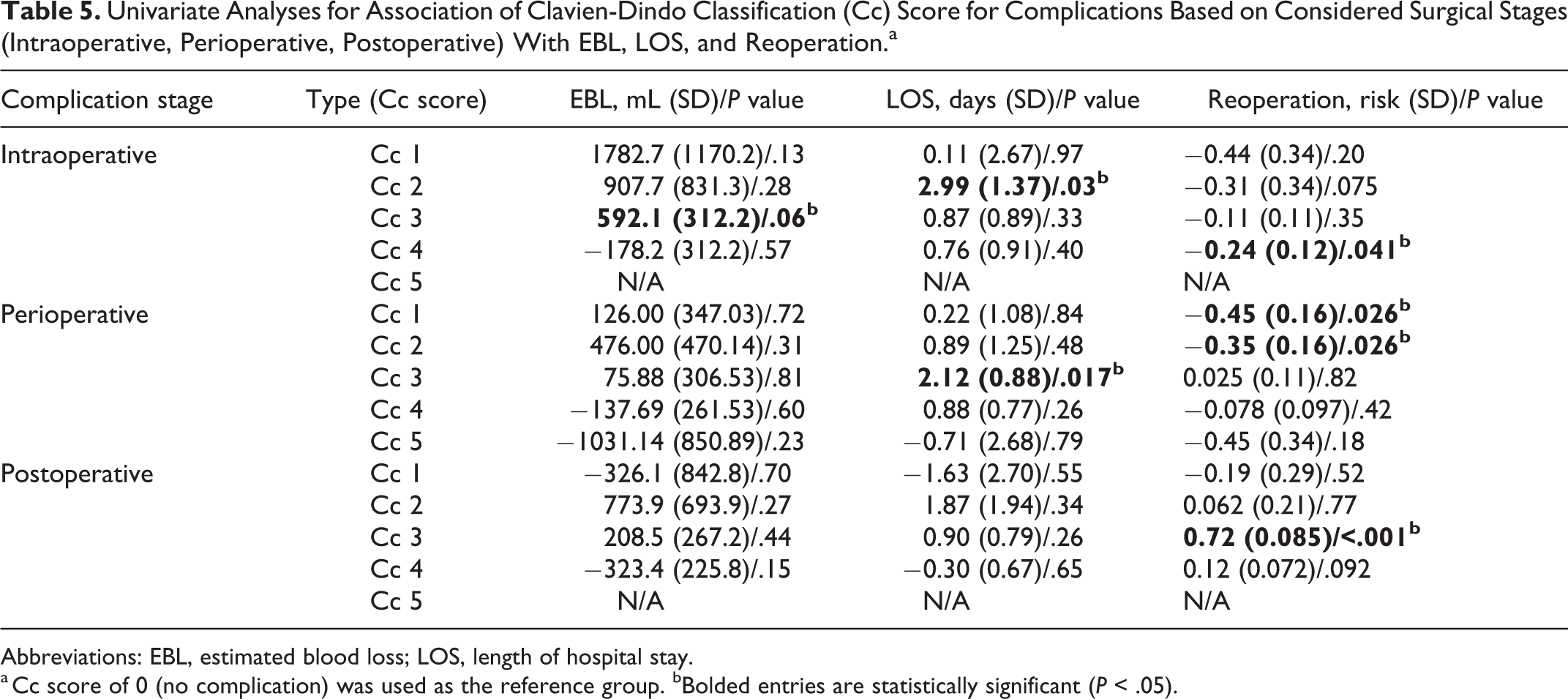
Abbreviations: EBL, estimated blood loss; LOS, length of hospital stay.
a Cc score of 0 (no complication) was used as the reference group. bBolded entries are statistically significant (P < .05).
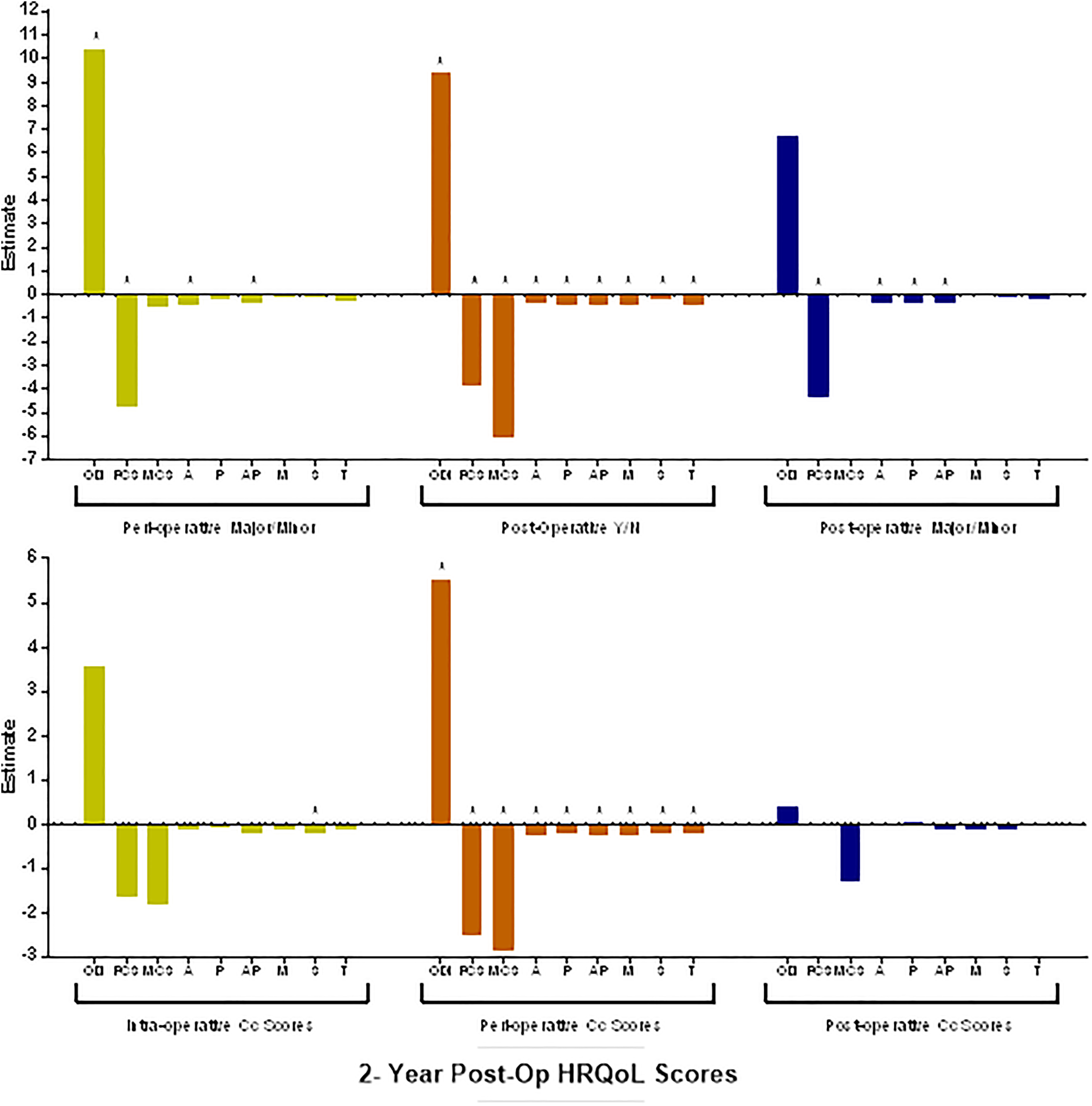
Mixed model results for the impact of complication type on 2-year HRQL scores: Oswestry Disability Index (ODI), Short Form (SF-36) Mental Component Summary (MCS), SF-36 Physical Component Summary (PCS), Scoliosis Research Society Patient Questionnaire Activity (AC), Pain (P), Appearance (AP), Satisfaction (S), Mental (M), and Total (T). Top: Complication presence (Yes/No) and complication type (Minor-Major) at 3 surgical stages. Bottom: Increasing Clavien-Dindo Classification score for complication presence at 3 surgical stages. *Denotes statistical significance at P <.05.
Patient-Reported Outcomes
When considering HRQL score changes 2 years postoperatively, major perioperative complications were associated with worse ODI, PCS, SRS AC, and SRS AP scores (P < .02) when compared with no complications. Postoperative complication presence worsened all HRQLs considered (P < .05) compared with the no complication group. Major postoperative complications were also linked to decreases in the following HRQLs: PCS, SRS AC, SRS P, and SRS AP (P < .05). Higher intraoperative Cc scores were associated with decreased SRS S (P = .01) overall, and higher perioperative Cc scores were associated with a worsening in all considered HRQLs (P < .05) compared with the no complication group. All groups considered, however, significantly improved in HRQL when compared with their own baseline. These results, based on complication category, are compiled and displayed in Figure 2.
Discussion
The continuous assessment of care for ASD is crucial for optimizing patient outcomes. Effective quality control is difficult, though, without an accepted and utilized methodology for reporting complications associated with ASD surgical correction. Specific preoperative patient and operative characteristics have been associated with increasing complication rates, including advanced age, number of instrumented vertebrae, and combined anterior-posterior approaches. 8,17,27 However, few reports focus on differing methods of classifying ASD procedure-related complications and how differing classification systems are correlated with operative and patient-reported outcomes.
In this study, intraoperative complications were associated with increased EBL (independent of “excessive bleeding” complications) and greater LOS. Although literature documenting the impact of complications on immediate patient outcomes exists, intraoperative complications largely did not affect postoperative HRQL measures in this study. 28 Intraoperative complications were also not associated with increased risk for later reoperation. The most common intraoperative complications were excessive bleeding (11.4%) and dural tears (6.0%). Dural tear incidences range from 3.1% to 15% in ASD surgery. Primary closure with close monitoring usually leads to excellent results, with no postoperative symptoms, but persistent symptoms can extend hospital stays. 29 -31 Excessive bleeding, similarly, usually only necessitates transfusion but can sometimes lead to myocardial infarction and other life-threatening consequences. 32,33 However, our recording of intraoperative complications found that in the long-term, they only affected 1 HRQL score (SRS S). Rampersaud et al, 18 in 2006, found similar results in an exhaustive analysis of intraoperative “adverse events” in spine surgery, where 76.5% were not connected to any clinical sequelae.
Patients with perioperative complications showed elevated Clavien-Dindo scores and significantly extended length of stay. Perioperative complications were most frequently gastrointestinal ileus (22.2%), pleural effusion (19.7%), or urinary tract infection (7.4%), all of which were minor. The most frequent major complications were deep-vein thrombosis (4.9%) and pulmonary embolism (4.9%). Perioperative complications are particularly important for their reported impact on LOS and impact on overall cost 6,34 -36 ; McCarthy et al 34 observed an increase of $2887 on average per extra day spent in the hospital for ASD procedures. Similar to intraoperative complications, there was no observed increase in reoperation risk associated with perioperative complications. Although the perioperative time is often studied as an important period to closely monitor patients, complications occurring perioperatively are not reflected in long-term outcomes. 17,20,37
The complication rate at each operative stage was as follows: 30.5% intraoperatively, 48.5% perioperatively, and 58.7% postoperatively. This finding is consistent with that of Nasser et al, 12 which showed increasing complication incidence over time. Postoperative complications were observed in greater numbers and higher severity on the Clavien-Dindo and minor-major scales. These postoperative complications were usually radiological or implant related: proximal junctional kyphosis (11.2%), rod breakage (14.3%), and implant prominence (4.1%), most frequently. This is consistent with the findings by Schwab et al 17 that implant failures were the most common major postoperative complications. Expectedly, these complications increased reoperation risk by 32% to 72%, depending on the scale used.
In our study, we found that perioperative and postoperative complications had a far more consistent impact on HRQLs. Intraoperative Cc scores only significantly affected SRS S scores. As less-invasive surgical procedures are analyzed for their reduction in intraoperative complications, research should also include how important that effect is at 2 years. 14,38,39 The best predictors for decreased HRQL scores were higher perioperative Cc scores and postoperative yes-no grouping. Interestingly, perioperative Cc scores were a better predictor for decreased HRQL metrics than postoperative Cc scores. This is likely statistically confounded by the few number of low Cc score complications in the postoperative period. Glassman et al 20 found decreased HRQLs for major perioperative complications, but not minor ones, supporting increasing Cc and minor-major scores as a good risk predictor.
We used the yes-no, minor-major, Clavien-Dindo, and temporal classification systems to accurately describe the impact of complications on surgical outcomes—higher EBL, longer LOS, and increasing odds of reoperation—and their impact on patient outcomes—HRQL metrics. Each classification system reports the same overall complication rate for the cohort studied (because of our procedure). However, each can be represented differently—many studies only report major complications, for example. Classification systems should balance their level of detail and ease of use against how they reflect a complication’s outcomes. 23 Of note is that all 3 systems, to varying degrees, were of use in reflecting consequences of complications. The Clavien-Dindo Scale found a significant decrease in patient satisfaction for intraoperative and perioperative complications but not for postoperative complications because its specificity was lost on the high-risk ASD population. Interestingly, the scales did not reflect surgical complexity, which has been correlated previously with increased rates of major complications. 40 Further study is needed to clarify the relationship between invasiveness and complications.
Spine research has long needed a complication classification system for uniform reporting, which allows quality control and comparisons between different facilities, surgeons, and times. The minor-major scale is commonly used, but differences arise, as demonstrated by the works of Glassman et al, 20 Schwab et al, 17 and Bess et al. 41 All 3 articles use minor-major categorization on perioperative complications in ASD, and all 3 would define >4000 mL of EBL in 3 different ways Currently, studies analyzing risk have to define terms—major, minor, surgical, medical—differently depending on their procedure or focus. 21,22 The Clavien-Dindo Scale may represent a more effective alternative, demonstrated in its rapid usage increase (Appendix C), though its adoption in spine surgery remains hesitant. 23,24 It was designed for in-hospital complication reporting but is now being used for postoperative complications in spine surgery. 42 This article elucidates how any categorization system for complications, even yes-no if consistently applied, can be more useful than contrived reporting. So long as variability persists between reports on surgical risk and adverse events, assessment and comparison of risk remains difficult.
Limitations
We appreciate several study limitations. This was a retrospective review of a multicenter database, which carries inherent problems of site and surgeon bias, particularly in complication reporting protocol. The considered patients are those with complete 2-year follow-up data; excluded patients may have been those with relevant complications who were lost to follow-up. The follow-up requirement also resulted in a particularly morbid patient population, which may confound complication rates.
Conclusion
There is a correlation between both the Clavien-Dindo and minor-major classification systems with established markers for patient improvement. However, only the Cc system accurately reflected changes in patient satisfaction at 2 years. A complication classification system must, both accurately reflect the impact of complications and predict the influence on outcome and satisfaction. This may allow us to objectively evaluate the complications associated with surgery. Regardless of system grade or complication, all ASD surgical patients improved their HRQL metrics at 2 years, but only the Cc system was able to predict satisfaction. Further research to allow the classification system to predict cost and outcome are needed.
Footnotes
Appendix A: Updated 2004 Clavien-Dindo scale
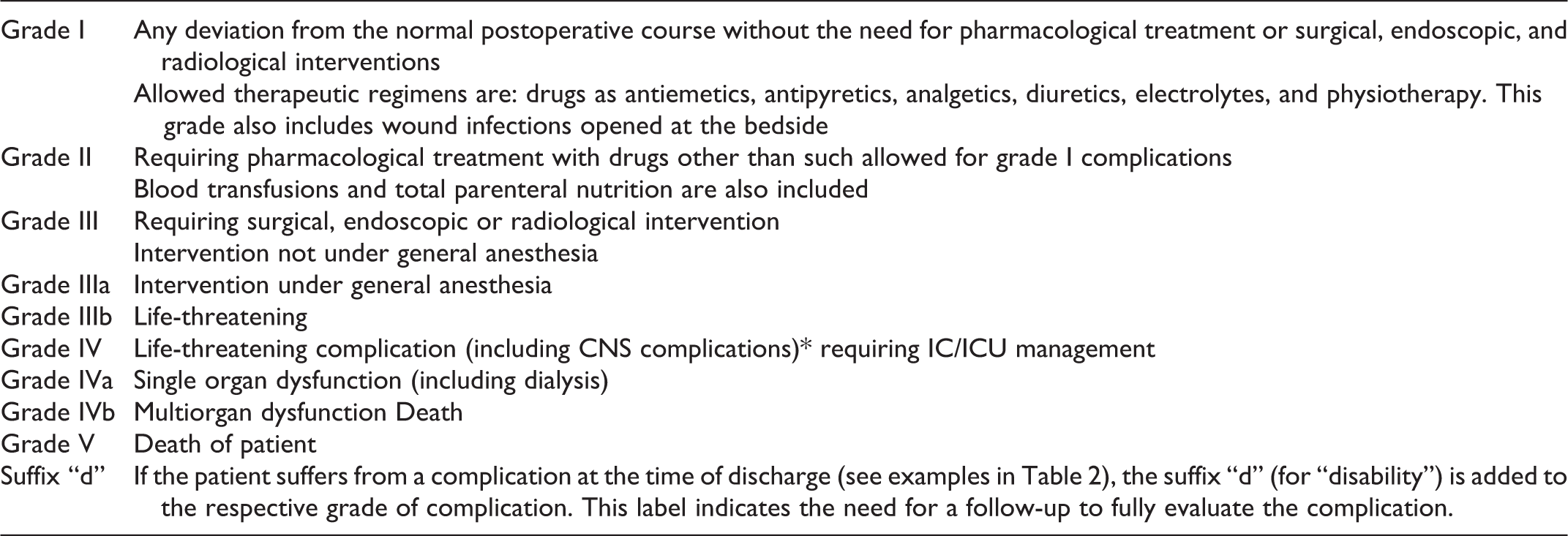
| Grade I | Any deviation from the normal postoperative course without the need for pharmacological treatment or surgical, endoscopic, and radiological interventions Allowed therapeutic regimens are: drugs as antiemetics, antipyretics, analgetics, diuretics, electrolytes, and physiotherapy. This grade also includes wound infections opened at the bedside |
| Grade II | Requiring pharmacological treatment with drugs other than such allowed for grade I complications Blood transfusions and total parenteral nutrition are also included |
| Grade III | Requiring surgical, endoscopic or radiological intervention Intervention not under general anesthesia |
| Grade IIIa | Intervention under general anesthesia |
| Grade IIIb | Life-threatening |
| Grade IV | Life-threatening complication (including CNS complications)* requiring IC/ICU management |
| Grade IVa | Single organ dysfunction (including dialysis) |
| Grade IVb | Multiorgan dysfunction Death |
| Grade V | Death of patient |
| Suffix “d” | If the patient suffers from a complication at the time of discharge (see examples in Table 2), the suffix “d” (for “disability”) is added to the respective grade of complication. This label indicates the need for a follow-up to fully evaluate the complication. |
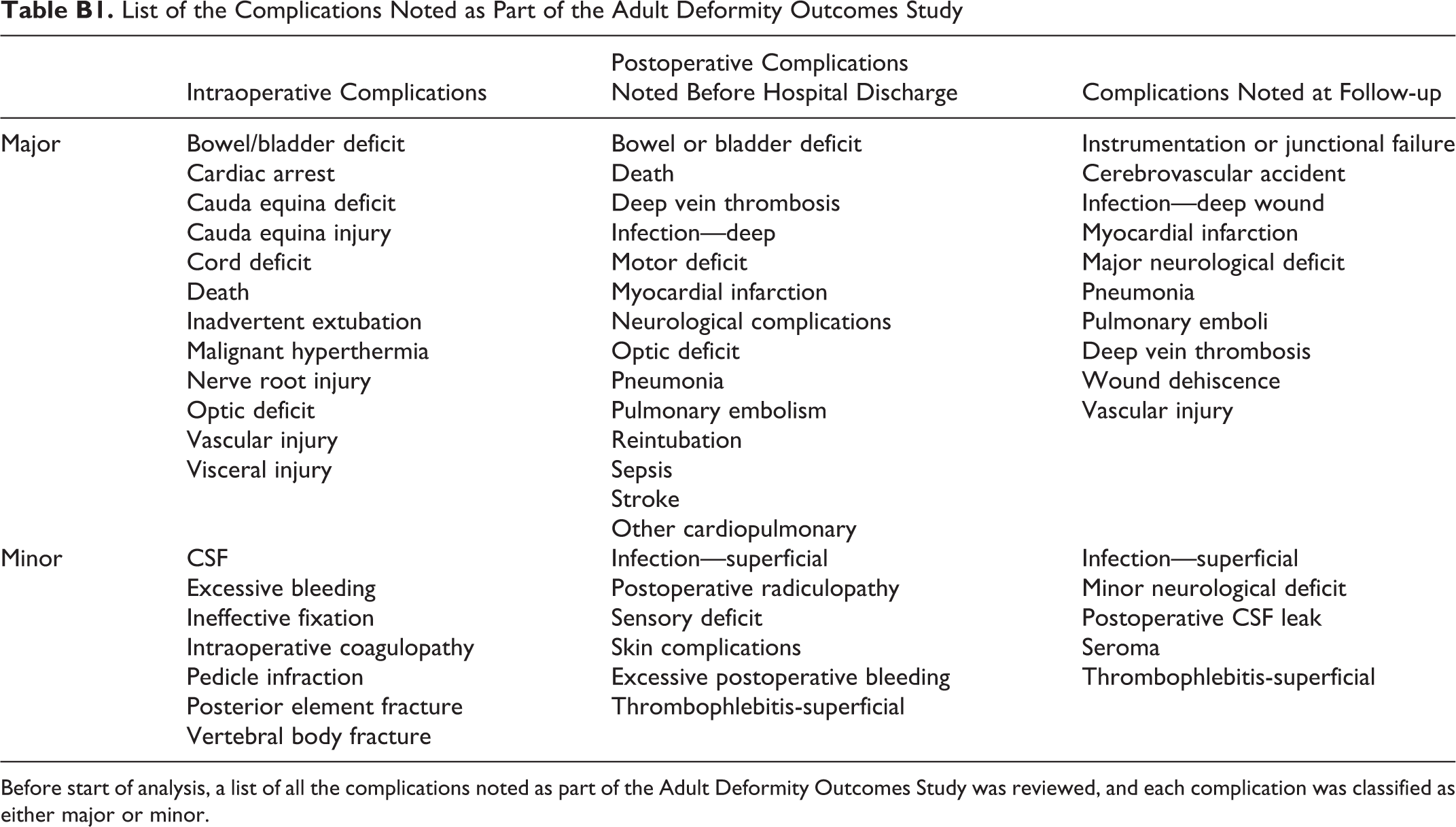
Appendix B: Minor-major scale as defined by Glassman et al in “The impact of peri-operative complications on clinical outcome in adult deformity surgery” 20
List of the Complications Noted as Part of the Adult Deformity Outcomes Study
| Intraoperative Complications | Postoperative Complications Noted Before Hospital Discharge | Complications Noted at Follow-up | |
|---|---|---|---|
| Major | Bowel/bladder deficit | Bowel or bladder deficit | Instrumentation or junctional failure |
| Cardiac arrest | Death | Cerebrovascular accident | |
| Cauda equina deficit | Deep vein thrombosis | Infection—deep wound | |
| Cauda equina injury | Infection—deep | Myocardial infarction | |
| Cord deficit | Motor deficit | Major neurological deficit | |
| Death | Myocardial infarction | Pneumonia | |
| Inadvertent extubation | Neurological complications | Pulmonary emboli | |
| Malignant hyperthermia | Optic deficit | Deep vein thrombosis | |
| Nerve root injury | Pneumonia | Wound dehiscence | |
| Optic deficit | Pulmonary embolism | Vascular injury | |
| Vascular injury | Reintubation | ||
| Visceral injury | Sepsis | ||
| Stroke | |||
| Other cardiopulmonary | |||
| Minor | CSF | Infection—superficial | Infection—superficial |
| Excessive bleeding | Postoperative radiculopathy | Minor neurological deficit | |
| Ineffective fixation | Sensory deficit | Postoperative CSF leak | |
| Intraoperative coagulopathy | Skin complications | Seroma | |
| Pedicle infraction | Excessive postoperative bleeding | Thrombophlebitis-superficial | |
| Posterior element fracture | Thrombophlebitis-superficial | ||
| Vertebral body fracture |
Before start of analysis, a list of all the complications noted as part of the Adult Deformity Outcomes Study was reviewed, and each complication was classified as either major or minor.
Appendix C: Top: number of articles citing Clavien-Dindo scale by year;Bottom: Number of orthopaedic articles citing Clavien-Dindo scale by year
Authors’ Note
The authors report the following updated disclosures:
AO Spine: Paid presenter or speaker; Research support
DePuy, A Johnson & Johnson Company: Paid consultant
Medicrea: Paid consultant
Stryker: Paid consultant
Allosource: Other financial or material support
Cervical Scoliosis Research Society: Research support
Globus Medical: Paid presenter or speaker
Medicrea: Paid consultant
SpineWave: Paid consultant
Terumo: Paid consultant
Zimmer: Paid presenter or speaker
Baxter: Paid consultant
DePuy, A Johnson & Johnson Company: Paid consultant
K2M: Paid consultant
Medtronic: Paid consultant
Nuvasive: Paid consultant
Stryker: Paid consultant
European Spine Journal: Editorial or governing board
Nuvasive: Research support
Bioventus: Research support
DePuy, A Johnson & Johnson Company: IP royalties; Paid consultant; Research support
Pfizer: Research support
Progenerative Medical: Stock or stock Options
Scoliosis Research Society: Board or committee member
Spine Deformity: Editorial or governing board
DePuy, A Johnson & Johnson Company: IP royalties; Paid consultant; Paid presenter or speaker
European Spine Journal-Advisory Board: Editorial or governing board
Global Spine Journal-Reviewer: Editorial or governing board
Innomed: IP royalties
Johnson & Johnson: Stock or stock Options
Medtronic: Paid consultant
Spine Deformity, Associate Editor: Editorial or governing board
SRS-IMAST & Education committee: Board or committee member
travel: Board or committee member
Wolters Kluwer Health - Lippincott Williams & Wilkins: Publishing royalties, financial or material support
Alphatec Spine: Stock or stock Options
Carlsmed: Paid consultant
Cerapedics: Paid consultant
DePuy: Research support
DePuy, A Johnson & Johnson Company: Paid consultant
Journal of Neurosurgery Spine: Editorial or governing board
Neurosurgery: Editorial or governing board
Nuvasive: IP royalties; Paid consultant; Research support
Operative Neurosurgery: Editorial or governing board
Scoliosis Research Society: Board or committee member
Spine Deformity: Editorial or governing board
Stryker: Paid consultant
Thieme: Publishing royalties, financial or material support
Zimmer: IP royalties; Paid consultant
American Orthopaedic Association: Board or committee member
Cervical Spine Research Society: Board or committee member
DePuy, A Johnson & Johnson Company: IP royalties; Paid consultant; Paid presenter or speaker
Globus Medical: IP royalties; Paid consultant; Paid presenter or speaker
International Spine Study Group: Board or committee member
ISSLS Textbook of the Lumbar Spine: Editorial or governing board
Medtronic: Paid consultant; Paid presenter or speaker
North American Spine Society: Board or committee member
Orthofix, Inc.: Paid consultant; Paid presenter or speaker
Scoliosis Research Society: Board or committee member
SeaSpine: IP royalties
Spine Connect: Stock or stock Options
Western Ortho Assn: Board or committee member
DePuy, A Johnson & Johnson Company: Research support
Medtronic: Paid presenter or speaker
Biomet Spine: IP royalties
DePuy, A Johnson & Johnson Company: IP royalties; Paid consultant; Research support
Global Spine Analytics - Director: Other financial or material support
International Spine Study Group (ISSG): Research support
International Spine Study Group (ISSG) - Executive Committee: Other financial or material support
K2M: IP royalties; Paid consultant
Medicrea: IP royalties; Paid consultant
Medtronic: Paid consultant
Next Orthosurgical: IP royalties
Nuvasive: IP royalties
Operative Neurosurgery - Editorial Board: Other financial or material support
Scoliosis Research Society (SRS) - Grant Funding: Other financial or material support
Stryker: IP royalties
Titan Spine: Research support
DePuy, A Johnson & Johnson Company: Research support
Globus Medical: Paid consultant; Paid presenter or speaker
K2M: IP royalties; Paid consultant; Paid presenter or speaker
Medicrea: Paid consultant
Medtronic: Paid consultant
Medtronic Sofamor Danek: IP royalties; Paid presenter or speaker
Nuvasive: Research support
Scoliosis Research Society: Board or committee member
spine deformity: Editorial or governing board
Stryker: Research support
VP of International Spine Society Group (ISSG): Board or committee member
Zimmer: IP royalties; Paid consultant; Paid presenter or speaker
DePuy, A Johnson & Johnson Company: Paid presenter or speaker
European Spine Journal: Editorial or governing board
Globus Medical: Paid consultant
International Spine Study Group: Board or committee member
Nuvasive: IP royalties
Scoliosis Research Society: Board or committee member
The Permanente Medical Group: Paid presenter or speaker.
The following authors have no conflicts of interest to disclose:
Gregory W Poorman, BA, Cyrus Jalai, BA, Abiola Atanda, MD, Nancy Worley, MS, Samantha Horn, BA, Alexandra Soroceanu, MD.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: International Spine Study Group (ISSG) has received financial support from DePuy, which helped fund the data found in this work.