
Abstract
Study Design
Prospective multicenter study.
Objective
To investigate the validity of transcranial motor-evoked potentials (Tc-MEP) in thoracic spine surgery and evaluate the impact of specific factors associated with positive predictive value (PPV).
Methods
One thousand hundred and fifty-six cases of thoracic spine surgeries were examined by comparing patient backgrounds, disease type, preoperative motor status, and Tc-MEP alert timing. Tc-MEP alerts were defined as an amplitude decrease of more than 70% from the baseline waveform. Factors were compared according to preoperative motor status and the result of Tc-MEP alerts. Factors that showed significant differences were identified by univariate and multivariate analysis.
Results
Overall sensitivity was 91.9% and specificity was 88.4%. The PPV was significantly higher in the preoperative motor deficits group than in the preoperative no-motor deficits group for both high-risk (60.3% vs 38.3%) and non-high-risk surgery groups (35.1% vs 12.8%). In multivariate logistic analysis, the significant factors associated with true positive were surgical maneuvers related to ossification of the posterior longitudinal ligament (odds ratio = 11.88; 95% CI: 3.17–44.55), resection of intradural intramedullary spinal cord tumor (odds ratio = 8.83; 95% CI: 2.89–27), preoperative motor deficit (odds ratio = 3.46; 95% CI: 1.64–7.3) and resection of intradural extramedullary spinal cord tumor (odds ratio = 3.0; 95% CI: 1.16–7.8). The significant factor associated with false positive was non-attributable alerts (odds ratio = .28; 95% CI: .09–.85).
Conclusion
Surgeons are strongly encouraged to use Tc-MEP in patients with preoperative motor deficits, regardless of whether they are undergoing high-risk spine surgery or not. Knowledge of PPV characteristics will greatly assist in effective Tc-MEP enforcement and minimize neurological complications with appropriate interventions.
Keywords
Introduction
Thoracic spine surgeries are relatively infrequent compared with lumber or cervical spine surgeries, but with an aging society, surgery frequencies are increasing. Thoracic spine surgery generally has favorable outcomes, but postoperative neurological complications sometimes occur. 1 Intraoperative neuromonitoring (IONM) is a useful standard care technique to assist in performing safe spine surgery.2-4 Especially in high-risk spinal surgeries, such as ossification of the posterior longitudinal ligament (OPLL) 5 and intramedullary spinal cord tumors (IMSCT), 6 IONM is reportedly highly effective. In our previous studies, transcranial motor-evoked potentials (Tc-MEP) are reported to have high sensitivity and specificity in detecting motor paralysis, thus, appropriate interventions indicated by Tc-MEP alerts may mitigate postoperative motor status degeneration.7,8
However, the positive predictive values (PPV) of Tc-MEP alerts are influenced by various factors, including spinal disease type, surgical procedure, Tc-MEP alert timing, vital signs, preoperative motor status, and surgical site location. Therefore, a better understanding of these factors will greatly assist in the appropriate use of Tc-MEP. Previously, we reported that the PPV increased in patients with poor preoperative motor status, even in non-high-risk cervical spine surgeries. 9 This study aimed to evaluate the efficacy of Tc-MEP and factors influencing PPV for thoracic spine surgery based on large, prospective, multicentered observational data.
Materials and Methods
This study was approved by the institutional review board of Yamaguchi University hospital’s Institutional Review Board (IRB no. H2020-024), and all patients provided written informed consent before enrollment. A total of 2308 prospectively enrolled thoracic spine surgery cases from 16 institutions in the monitoring committee of the Japanese Society for Spine Surgery between April 2017 and March 2022 were evaluated for inclusion. Of these, 1156 were selected for this study. Of the 1152 patients excluded, 1111 were excluded due to combined surgeries requiring extensive fusion or decompression across the lumbar or cervical spine, and as a result, all scoliosis and adult spine deformity surgeries were excluded. An additional 41 cases were excluded due to poor derivation of Tc-MEP waveform in all lower limb muscles (Figure 1). Preoperative motor deficits were observed in 26 patients (61.9%) and postoperative paralysis worsened in 2 patients (4.8%). The inclusion criteria in the present study. Tc-MEP indicates transcranial motor-evoked potential.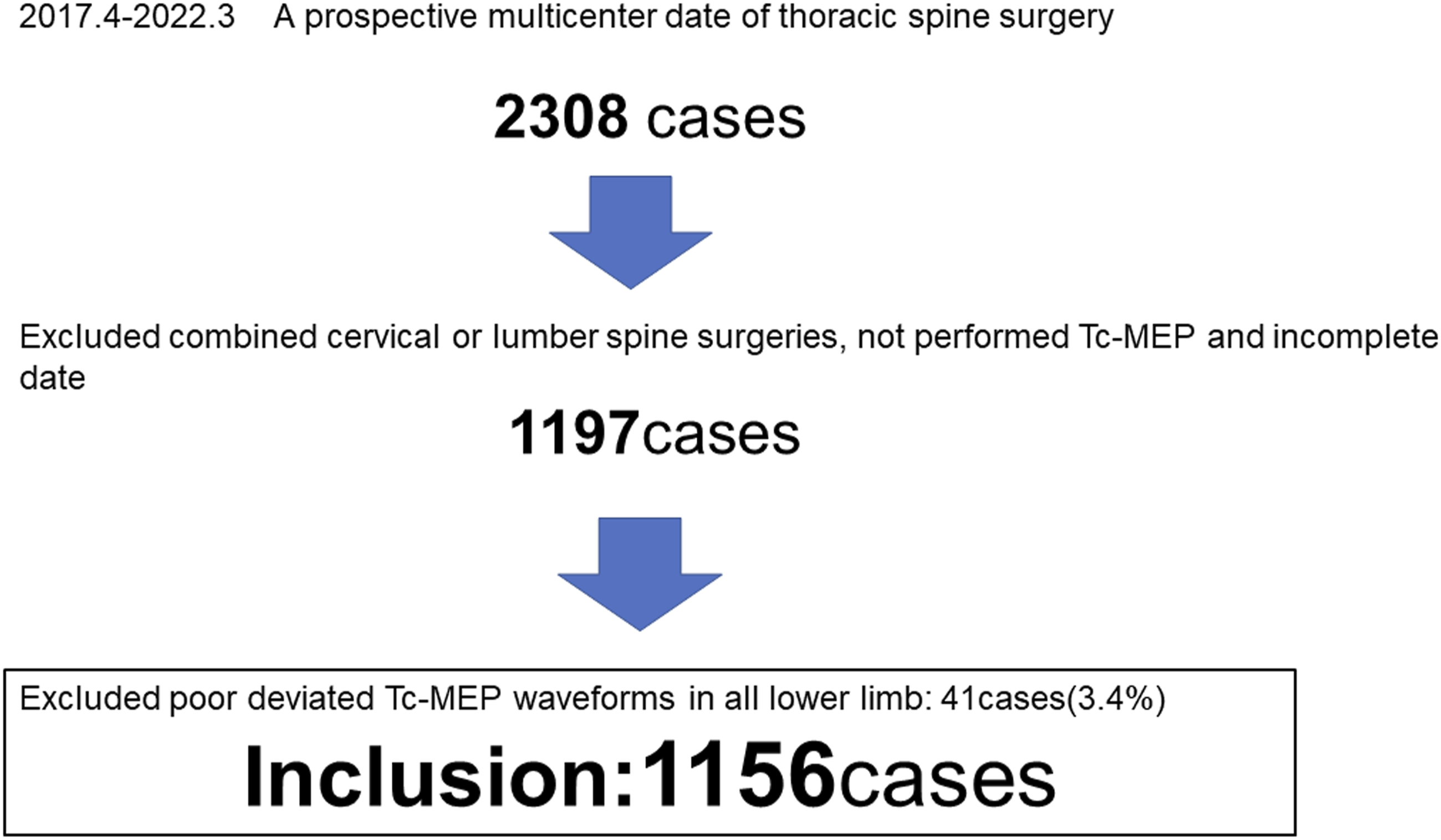
The Institutional Review Board at each center approved the protocol of the present study, and all patients provided their informed consent.
As control waveforms, the abductor digit minim (ADM) or abductor pollicis brevis muscles in the upper limb were measured. At least one or more proximal and distal muscles were selected as derivation muscles including the quadriceps (Qc), tibialis anterior (TA), gastrocnemius, flexor hallucis brevis, and abductor hallucis (AH) muscles in the lower limb. A corkscrew electrode (Nihon Kohden Corporation, Tokyo, Japan) was inserted symmetrically 5–7 cm lateral and 2 cm anterior to the Cz point. Radial cranial electrical stimulation was performed at a stimulation intensity of 100–200 mA (duration .5 ms), filter 50–1000 Hz, and recording time 100 ms, with a stimulation interval of 2 ms, 5–10 times, with a stimulation frequency not exceeding 20 times.
Anesthesia was induced by intravenous propofol (3–4 mg/mL), fentanyl (2 mg/kg), and vecuronium (.12–.16 mg/kg), and during IONM, propofol (100–150 mg/kg/min, targeted control injection), remifentanil (1 mg/kg/h), and vecuronium (0–.04 mg/kg/h) maintained by intravenous anesthesia. Systolic blood pressure was maintained above 90 mmHg. Tc-MEP amplitude was measured from the baseline to the peak of the negative wave. Tc-MEP was detected promptly, and the baseline waveform recorded at the beginning of the surgical procedure. If waveforms were not derived from all muscles examined, they were defined as partial waveforms, and defined as full if they were derived from all muscles. As in previous studies, a 70% decrease in amplitude from the baseline waveform was defined as a Tc-MEP alert.7-9 The occurrence of a worsened postoperative motor function was defined as an immediate postoperative MMT decrease of at least one level from the preoperative MMT. Delayed onset paralysis was not included in the worsened postoperative motor function group.
Outcomes were defined as follows: (1) True positive was defined as new or worsened postoperative motor function with the Tc-MEP alert persisting until the end of the surgery, (2) true negative was defined as no new or worsened postoperative motor function and no alert, (3) false positive was defined as no worsened postoperative motor function with the alert persisting until the end of surgery, (4) false negative was defined as no alert during surgery and new or worsened postoperative motor function, and (5) rescue was defined as no worsened postoperative motor function after surgery and intervention that restored the Tc-MEP waveforms after Tc-MEP alerts. 8 Rescue was confirmed by the Monitoring Committee of the Japanese Society for Spine Surgery after case review. The rescue rate was defined as the number of rescue cases divided by the number of rescued cases and the number of true positive cases. Rescue cases were not included in the accuracy analysis as, in the absence of a wake-up test, it is not possible to confirm whether the temporal decrease in Tc-MEPs reflected true motor impairment.
High-risk spine surgery and the non-high-risk spine surgery were classified as follows.
High-risk group: intradural IMSCT, intradural extramedullary spinal cord tumors (EMSCT), and OPLL.
Non-high-risk group: ossification of ligament flavum (OLF), degenerative spondylotic myelopathy including disc herniation (DSM), trauma, extradural spinal tumor including metastatic spinal tumors, and “others” including pyogenic spondylitis, adhesive arachnoiditis, hemosiderosis, spinal dural arteriovenous fissure, arachnoid cyst or web, and epidural hematomas.
The following items were collected for analysis: (1) age, (2) gender, (3) body mass index (BMI), (4) type of spinal disease, (5) incidence of Tc-MEP alert, (6) surgical procedures immediately before Tc-MEP alert (7) motor status with motor deficit defined as preoperative MMT grade 4 or less, (8) surgery time (minutes), (9) estimated blood loss (g), (10) postoperative motor paralysis, (11) the surgical manipulation immediately preceding Tc-MEP alerts. Factors causing Tc-MEP alerts that cannot be identified by surgical manipulation Tc-MEP alerts were defined as non-attributed alerts.
The above items were categorized and compared according to (1) a preoperative motor status: preoperative MMT ≤4 (group D) as the case group or normal motor status: preoperative MMT = 5 (group N) as the control group and (2) true-positives as the case group and false-positives as the control group.
Statistical Analysis
Univariate analysis using the Mann-Whitney U test, or the chi-square test was performed to compare parameters between groups. To search for factors associated with true positives, multivariate logistic analysis was performed using a stepwise parameter selection method with repeated forward and backward selection of explanatory variables with a threshold of P < .1. In the analysis, all available explanatory variables were included, except for surgery time and estimated blood loss, so as to not exclude variables unevaluated in the univariate analysis. Statistical analysis was performed using StatFlex for Windows V7.0, (Artech Co, Osaka), with P < .05 indicating a significant difference.
Result
Demographic Data and Univariate Analysis Comparison With the Preoperative Motor Status.
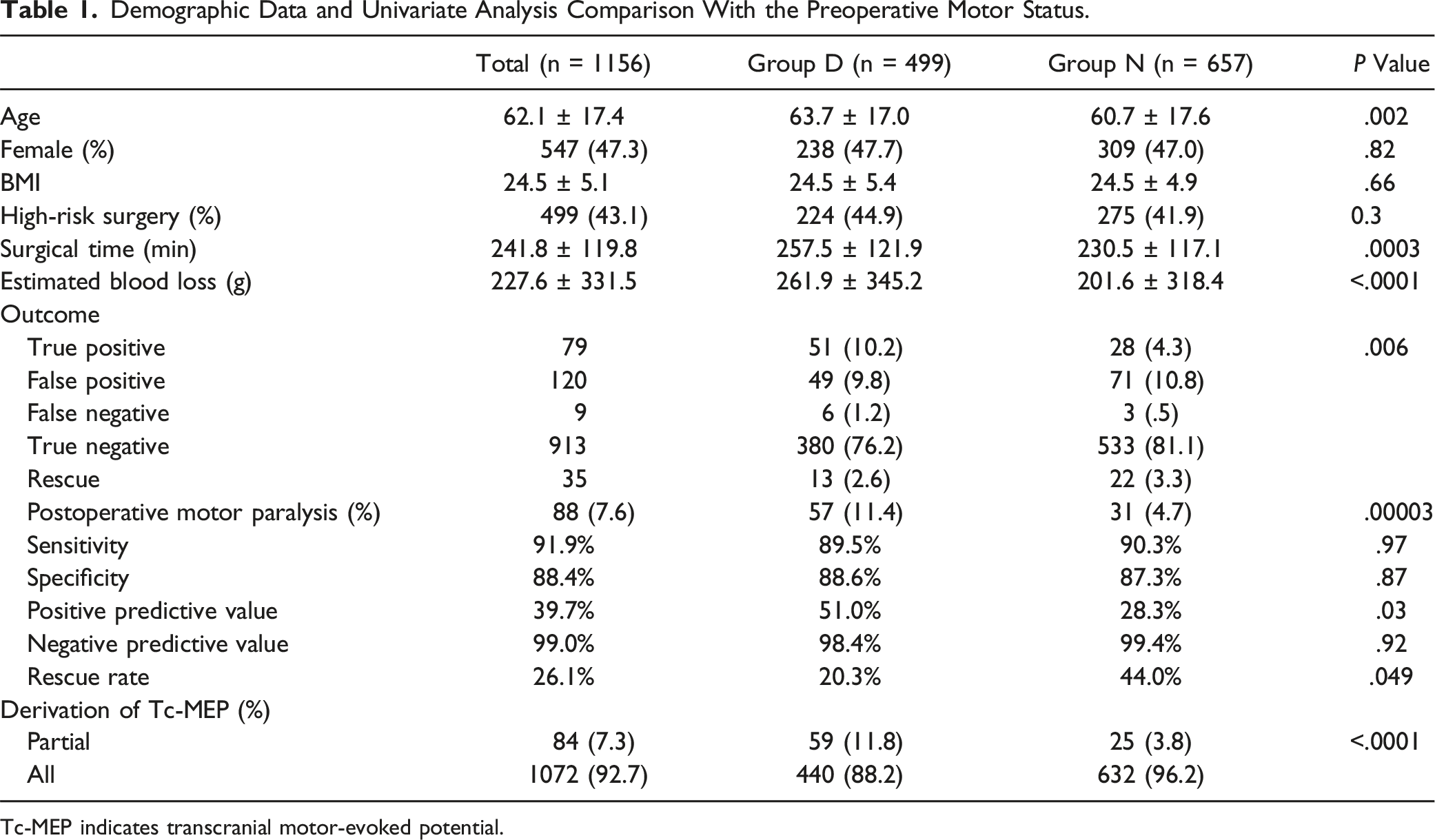
Tc-MEP indicates transcranial motor-evoked potential.
The Incidence of Postoperative Motor Paralysis
The incidence of postoperative motor paralysis was significantly higher in Group D than in Group N (11.4% vs 4.7%) for both the high-risk (17.4% vs 9.1%) and non-high-risk surgery groups (6.5% vs 1.6%), and especially higher in Group D than Group N for OPLL (23.8% vs 7.1%) and EMSCT (13% vs 3.9%) (Figure 2). The highest rate of postoperative motor paralysis was observed in IMSCT (28.6%), followed by OPLL (16%) and EMSCT (7.6%). The incidence rate of postoperative motor paralysis. Tc-MEP indicates transcranial motor-evoked potential; OPLL, ossification of the posterior longitudinal ligament; IMSCT, intradural intramedullary spinal cord tumors; EMCST, Intradural extramedullary spinal cord tumors; OLF, ossification of ligament flavum; and n.s, not significant.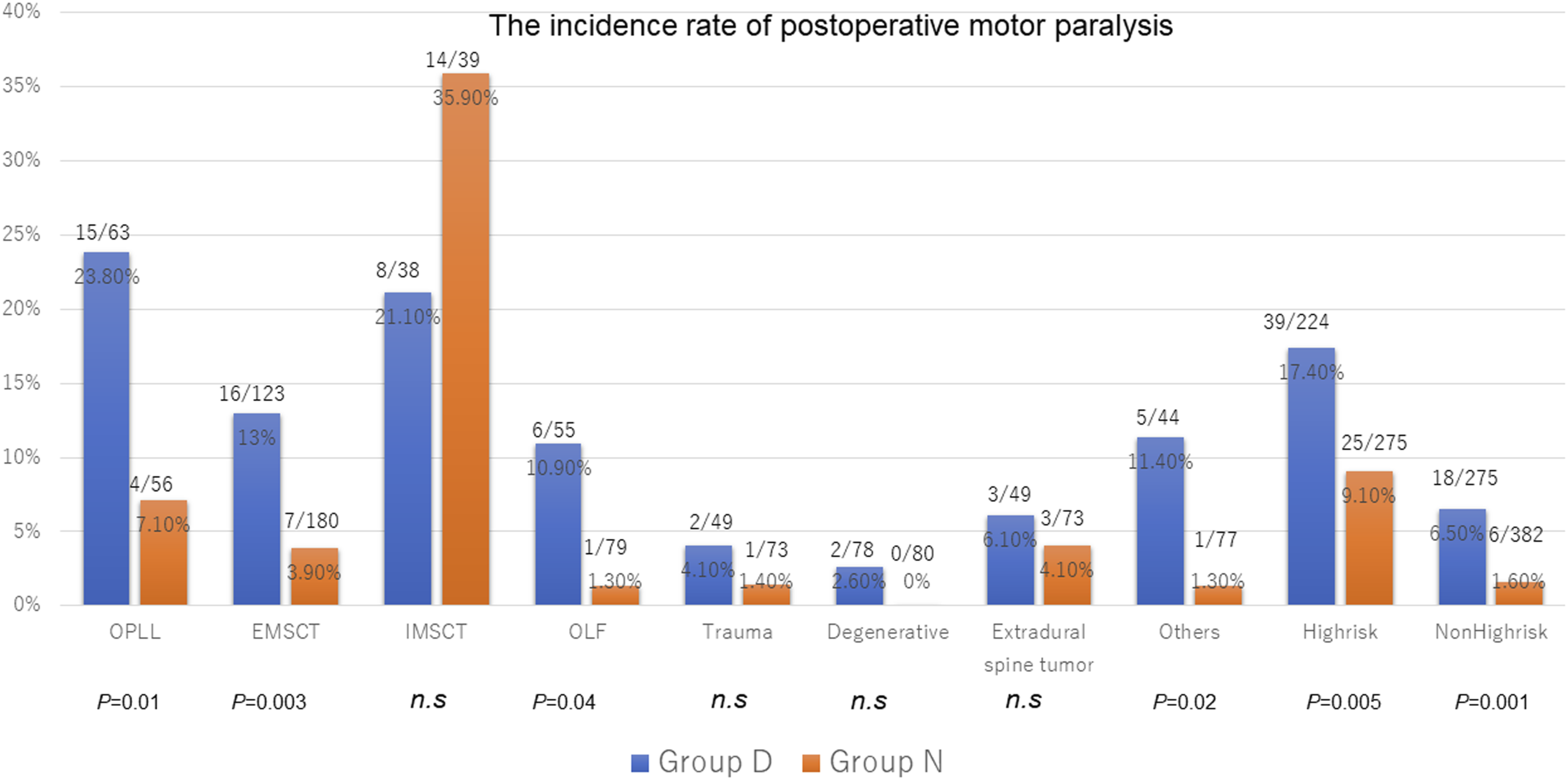
The Incidence of Tc-MEP Alerts and PPV
The highest rate of Tc-MEP alerts was observed in IMSCT (45.4%), followed by OPLL (27.7%). There was no significant difference between Group N and D in any type of spinal disease. The highest PPV was observed in IMSCT (60%), followed by OPLL (57.5%) and EMSCT (38.2%). The PPV was significantly higher in Group D than Group N for both the high-risk (60.3% vs 38.3%) and non-high-risk surgery groups (35.1% vs 12.8%) (Figure 3). Positive predictive value of Tc-MEP alerts. Tc-MEP indicates transcranial motor-evoked potential, OPLL, ossification of the posterior longitudinal ligament; IMSCT, intradural intramedullary spinal cord tumors; EMSCT, Intradural extramedullary spinal cord tumors; and OLF, ossification of ligament flavum.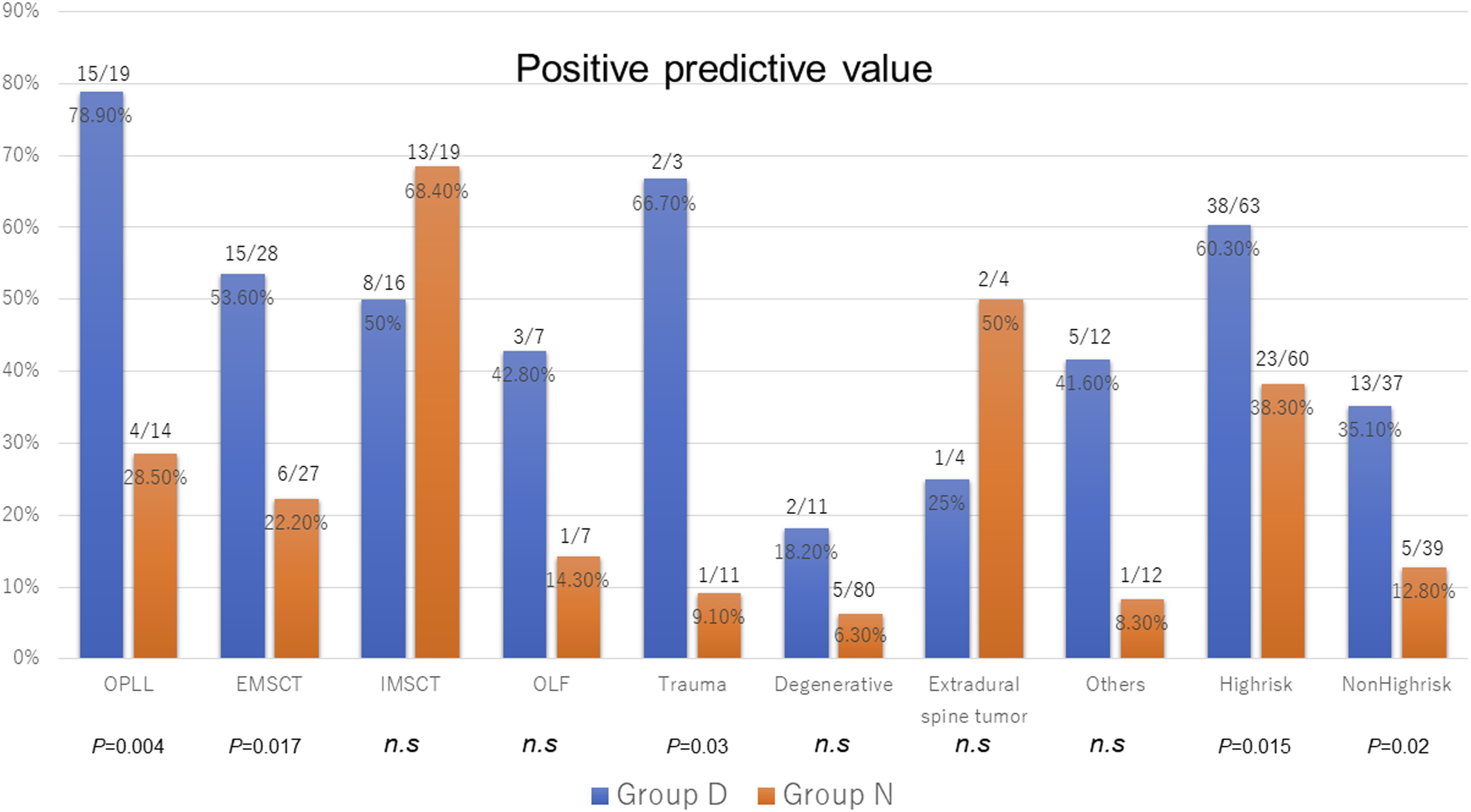
Characteristics of Factors Contributing to the Occurrence of Tc-MEP Alerts
Univariate Analysis Comparing False Positive to True Positive.
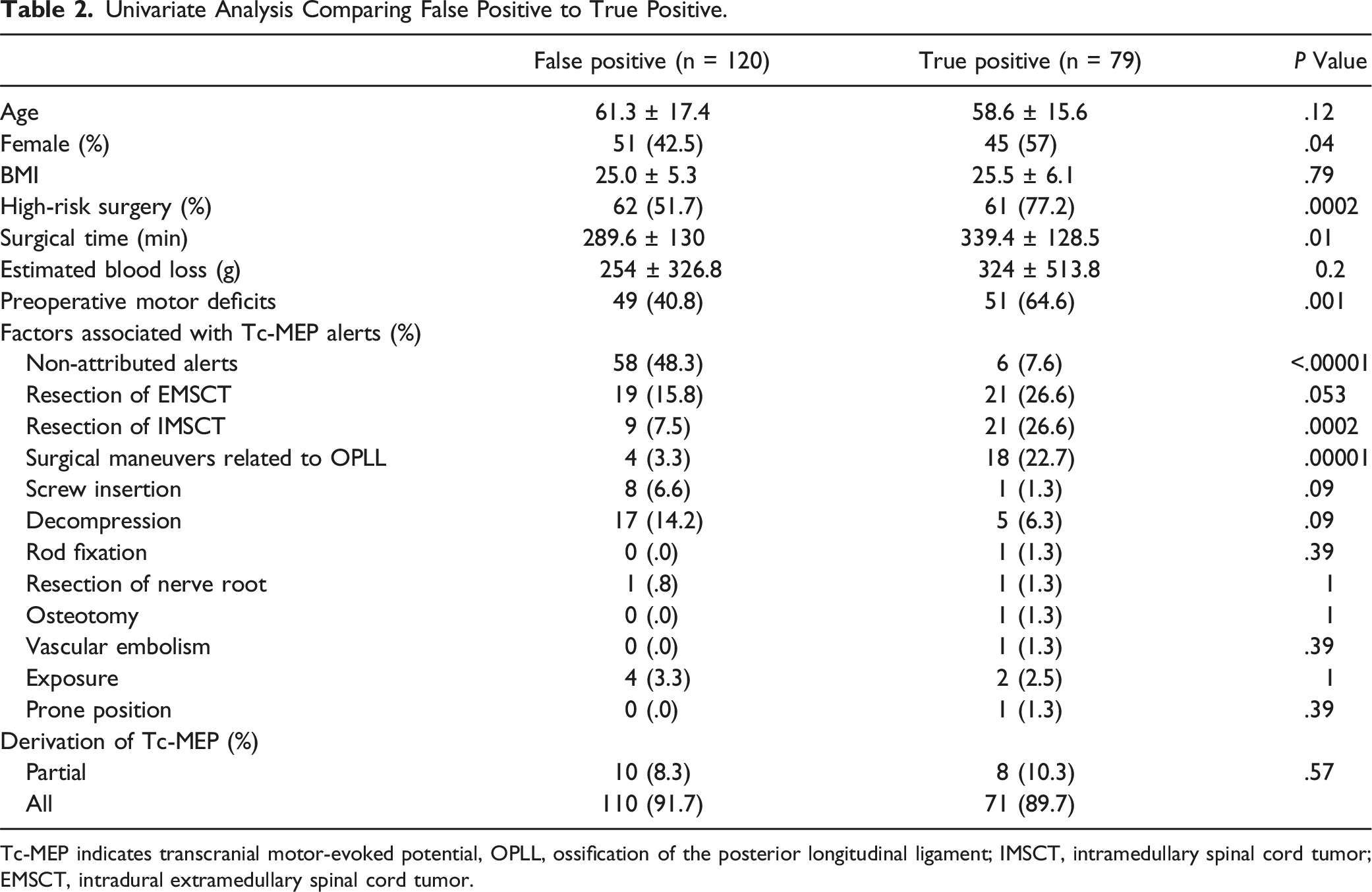
Tc-MEP indicates transcranial motor-evoked potential, OPLL, ossification of the posterior longitudinal ligament; IMSCT, intramedullary spinal cord tumor; EMSCT, intradural extramedullary spinal cord tumor.
False-Negative
Nine false negative cases were observed in this study. Seven of nine underwent thoracic surgeries including conus level (T12-L1). Two patients with spinal cord tumors (upper thoracic metastatic spinal tumor and T9 vertebral hemangioma) showed preoperative motor deficits and somewhat deteriorated Tc-MEP waveforms but did not reach the waveform threshold.
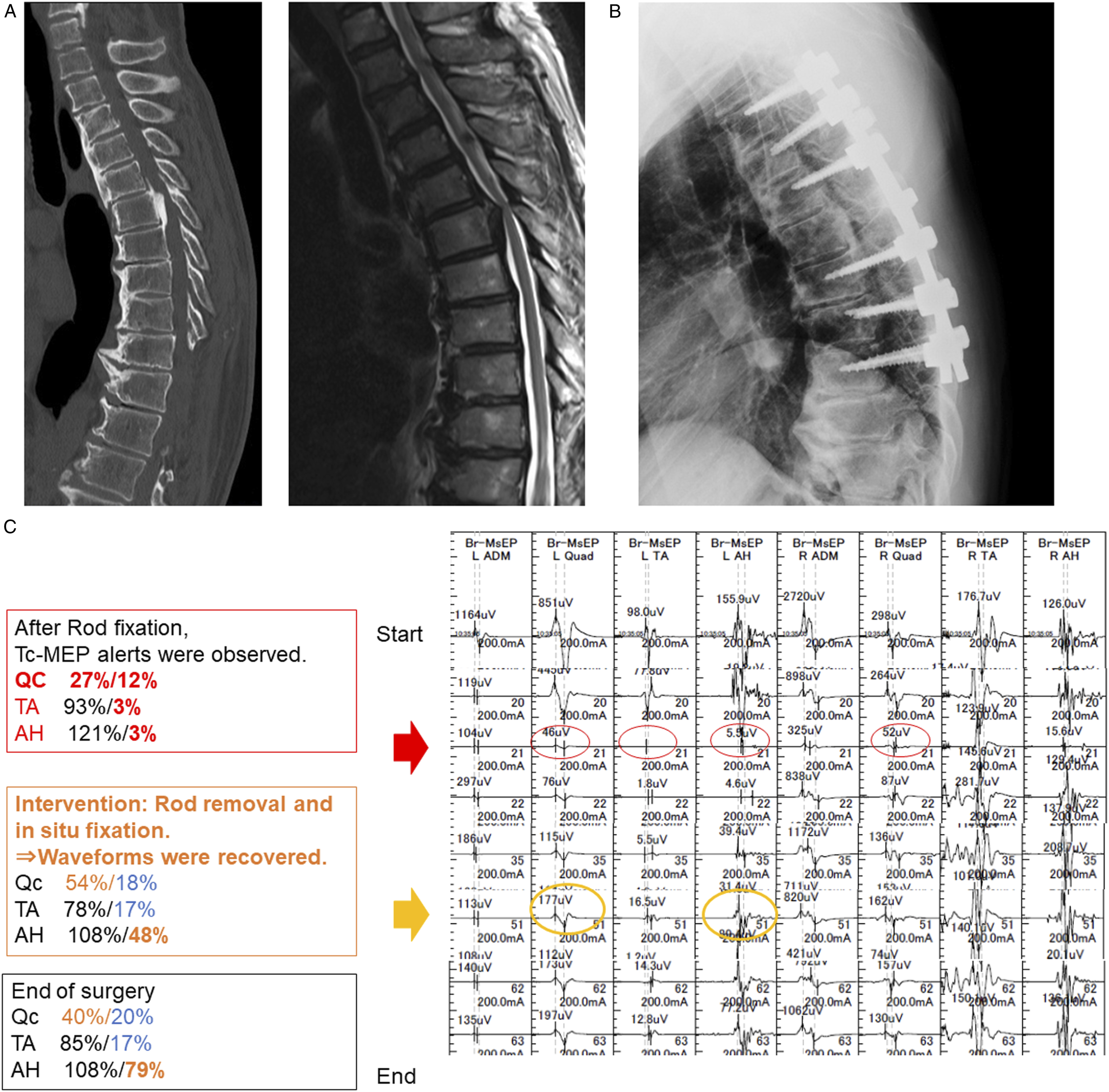
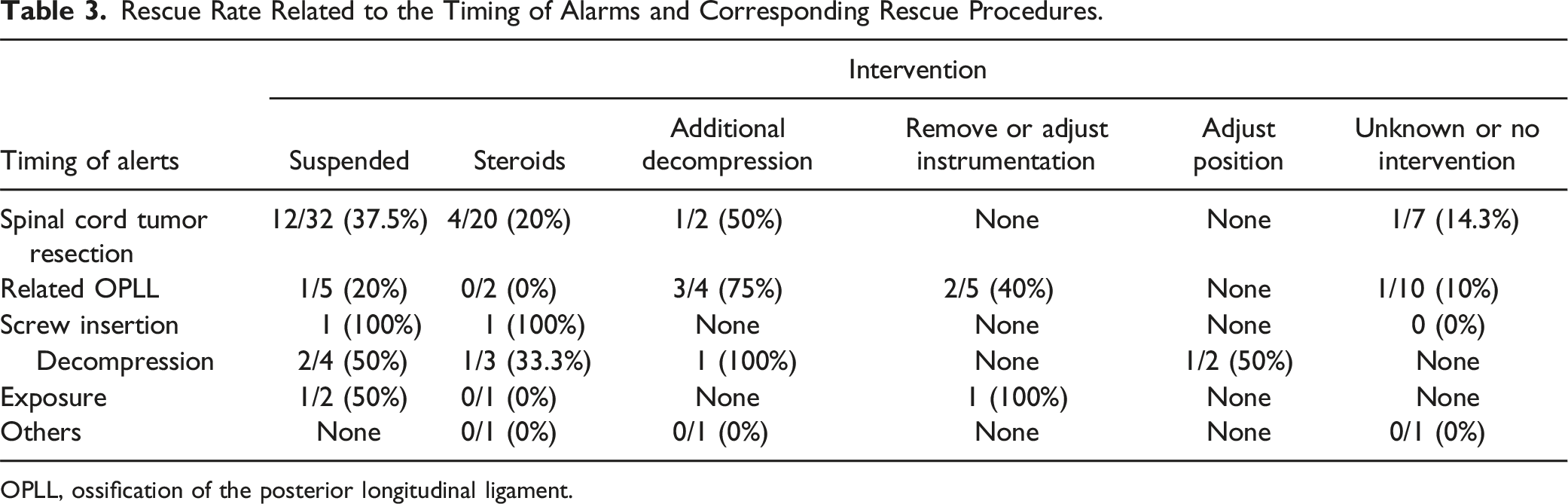
Rescue Rate
The overall rescue rate was 26.1%, with the rescue rate of Group N higher than that of Group D (44% vs 20.3%) (Table 1). In OPLL and EMSCT surgery, the rescue rates of Group N were higher than that of Group D, but for IMSCT surgery, rescue rates were equal for both Group N and D. (Figure 4) An illustrative rescue case is shown Figure 5. Detailed information on the timing of alerts and corresponding rescue procedures is shown in Table 3. Rescue rate. OPLL indicates ossification of the posterior longitudinal ligament; IMSCT, intradural intramedullary spinal cord tumors; EMCST, Intradural extramedullary spinal cord tumors; OLF, ossification of ligament flavum; U.T, unable to test due to small numbers, and n.s, not significant. A 65-year-old male patient with thoracic ossification of the posterior longitudinal ligaments (T5-6) had preoperative lower limb motor deficits, with Tc-MEP waveforms collected. The Tc-MEP waveforms in the left lower limb muscles deteriorated remarkably after rod fixation but the Tc-MEP waveforms of the AH muscles recovered when the rod was removed, adjusted, and fixed again. Postoperative motor status did not worsen, and gait disturbance recovered. Tc-MEP indicates transcranial motor-evoked potential, Qc, quadriceps; TA, tibialis anterior; AH, abductor hallucis. Rescue Rate Related to the Timing of Alarms and Corresponding Rescue Procedures. OPLL, ossification of the posterior longitudinal ligament.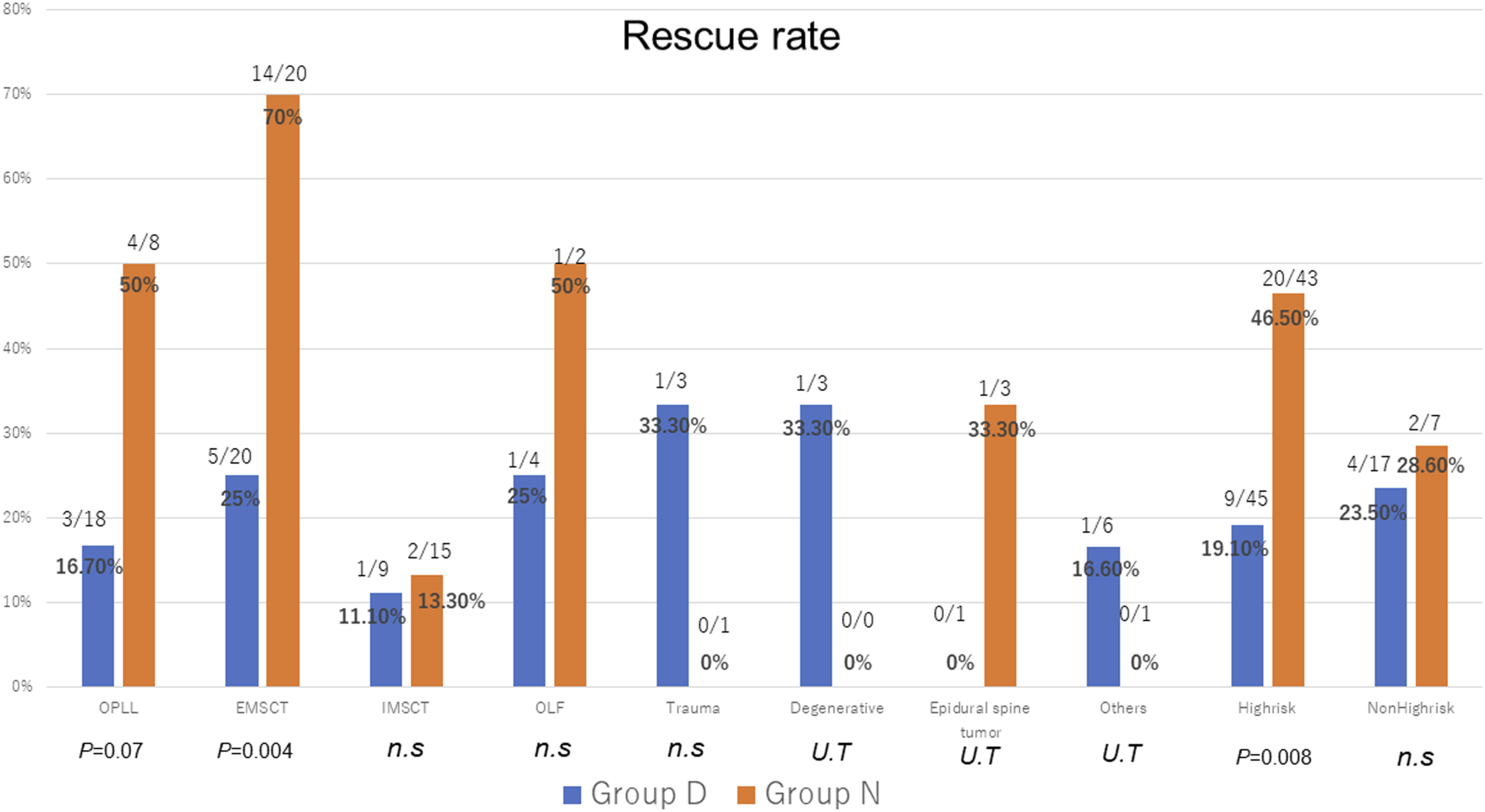
Multivariate Logistic Analysis
Multivariate Logistic Analysis for the Factors Related to True Positive.
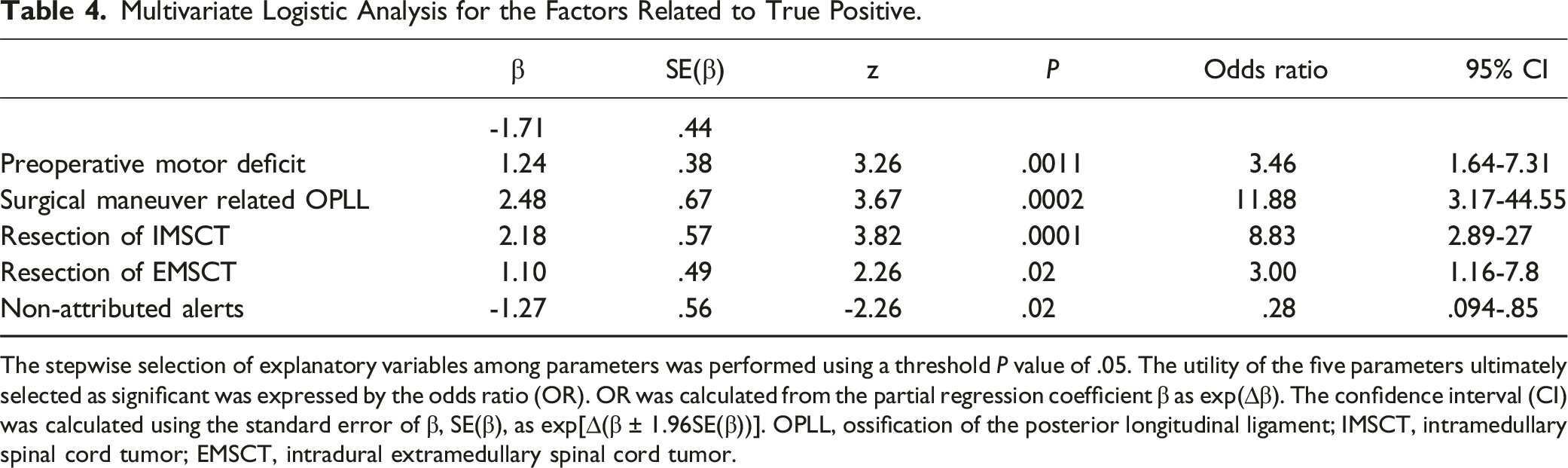
The stepwise selection of explanatory variables among parameters was performed using a threshold P value of .05. The utility of the five parameters ultimately selected as significant was expressed by the odds ratio (OR). OR was calculated from the partial regression coefficient β as exp(∆β). The confidence interval (CI) was calculated using the standard error of β, SE(β), as exp[∆(β ± 1.96SE(β))]. OPLL, ossification of the posterior longitudinal ligament; IMSCT, intramedullary spinal cord tumor; EMSCT, intradural extramedullary spinal cord tumor.
Discussion
This study constituted the largest prospective evaluation of Tc-MEP for 1156 thoracic spine surgeries. The major finding in this study is that Tc-MEP is highly useful in thoracic spine surgery and that PPV is higher in patients with preoperative motor deficits, even in non-high-risk spine surgery.
About half of the patients in this study had preoperative motor deficits. The thoracic spine lesion is a site of poor blood flow, especially in the upper thoracic level, so the perioperative neurological complication rate tends to be higher than that for lumber or cervical spinal surgery. 1 Typically, thoracic OPLL surgery is reported to have a generally higher perioperative complication rate, 5 with significantly more postoperative neurological complications. The use of Tc-MEP alert mediated interventions for thoracic OPLL is reported to improve postoperative motor paralysis.10,11 Tc-MEP is particularly effective in the evaluation of motor function for thoracic spine surgeries. However, the more poor the preoperative motor status, the more difficult it is to derive Tc-MEP waveforms. Distal muscles, such as the AH, are recommended as appropriate muscles from which to derive Tc-MEP waveforms.12,13 Distal muscles are more innervated by the lateral corticospinal tracts with higher derivation rates than the proximal muscles. 14 Thus, multichannel Tc-MEP derivation may achieve improved sensitivity and specificity with the increased coverage of potential postoperative paralysis muscles. 15 In recent years, multi-train stimulation and constant voltage stimulation methods are also shown to improve waveform derivation and may be considered when waveforms are difficult to obtain.16-18 Multimodal IONM, like the combination of D-wave and Tc-MEP monitoring, may also reduce false positives and false negatives.19-21 D-wave also evaluates motor function and may indicate permanent motor paralysis in spinal cord tumor surgery.3,22 It may also be important, for high-risk spine surgery, to consider the use of multimodal neuromonitoring in cases of preoperative motor deficits.
In Japan, a 70% or more decrease in Tc-MEP from the baseline waveform is defined as the alert threshold, with excellent sensitivity and specificity for thoracic spine surgery. Like previous studies,23,24 false-negative results were more common in conus medullaris surgery, suggesting that the AH muscles are mainly S2 segment-dominated, making S1 segment-dominated corticospinal tract defects easier to detect, but increasing detection difficulty below S2.25,26 Using Tc-MEP from the external anal sphincter or somatosensory evoked potentials (SSEP) may reduce these false negative results.27,28
Tc-MEP accuracy was excellent, regardless of preoperative motor status in this study, but only the PPV varied significantly on preoperative motor status. The results showed that preoperative motor status affected the PPV in addition to alert timing, and spinal disease type. In this study, the risk of neurological complications during surgical manipulation related to OPLL and intradural spinal cord tumor was in line with previous studies.5,6,24,29 The frequency of neurologic complications in a previous Nationwide study related to thoracic OPLL in Japan was more than 30%, 5 whereas, in this study, it was less frequent at 16%. In addition to the refinement of surgical techniques and knowledge, IONM may minimize neurological complications. However, for high-risk spine surgeries such as OPLL and EMSCT, while the rescue rate tended to exceed 50% for group N, it was low for intramedullary tumors. Thus, further studies to prevent postoperative motor paralysis are necessary. In this study, the PPV of IMSCT and the postoperative motor paralysis rate were almost equal in comparison with preoperative motor status. Resection of IMSCT may be more likely to directly damage the spinal cord, causing spinal cord ischemia, than resection of EMSCT or surgical maneuvers related to OPLL, which may lead to postoperative motor deficits, regardless of the preoperative motor status. The 70% threshold yielded high sensitivity, but multimodal IONM may be more effective in communicating Tc-MEP changes during IMSCT surgery to surgeons.
On the other hand, non-attributed alerts were associated with false positives. These results reflect previous studies, suggesting that alerts were influenced by hypotension, hypoxia, body temperature, anesthesia, and prolonged surgery.30-33 Therefore, it is important to share information and use a checklist with the anesthesiologist and surgical team when a non-attributed alert occurs.
34
However, position-related neurological complications are not to be forgotten.
35
Yoshida et al.
36
reported that in thoracic OPLL, Tc-MEP deteriorated upon shifting the patient to the prone position, and recovered upon return to the supine position. It is important to carefully prepare by performing supine and prone position tests before surgery,
5
especially in patients with high BMI, women, and upper thoracic OPLL. Rescue procedures such as suspended surgery including steroid administration, adding decompression, and adjusting instruments were effective for Tc-MEP alerts caused by surgical procedures. If the MEP alert occurs during surgery, an important process for safe spine surgery would be for the surgical team to quickly take appropriate intervention to restore the Tc-MEP waveform. The flow chart for the occurrence of Tc-MEP alerts is shown in Figure 6. Flowchart of an alert generated by Tc(E)-MEP. Tc(E)-MEP indicates transcranial motor-evoked potentials.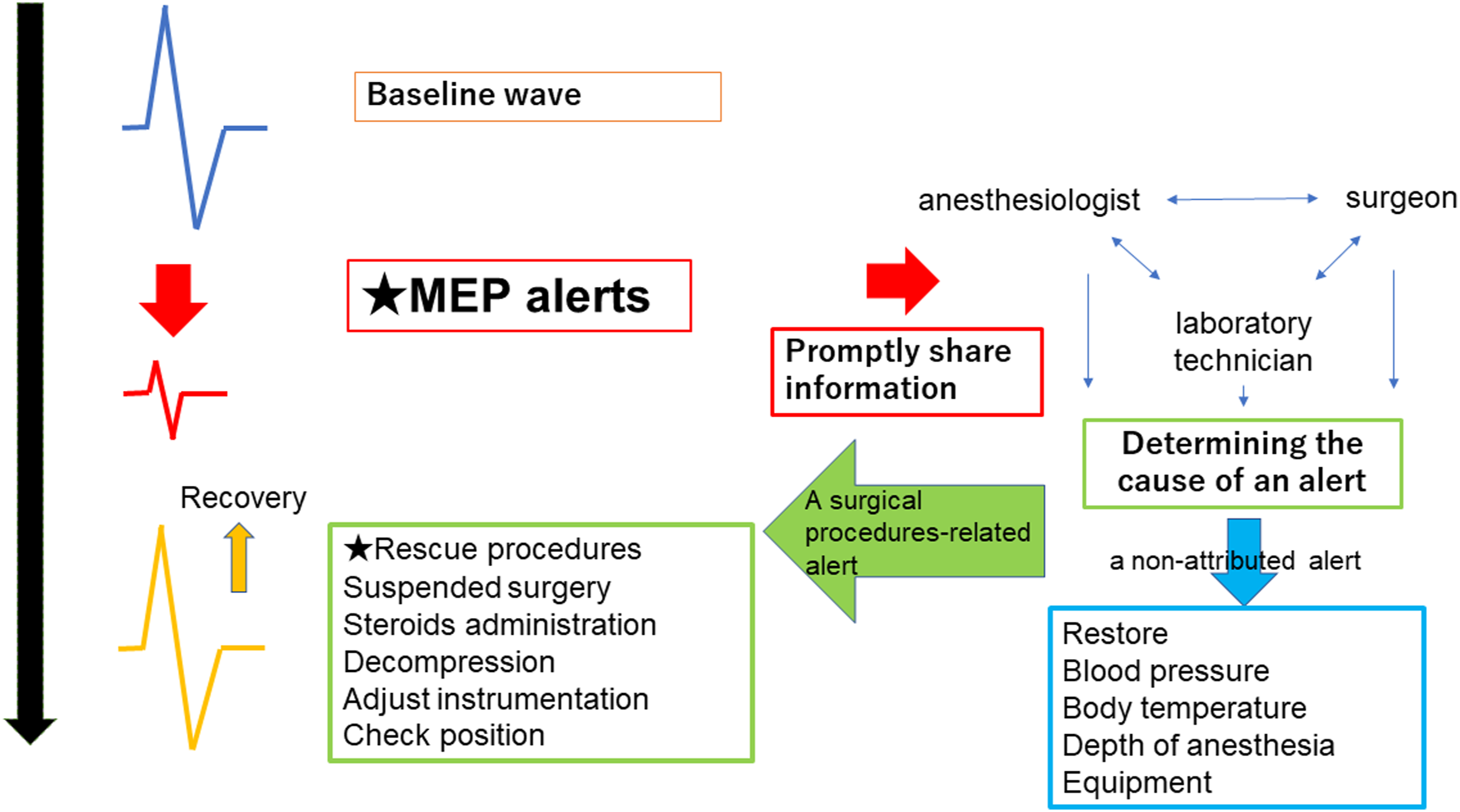
There are several limitations to this study. First, Tc-MEP was the only modality analyzed. As this is a multicenter study, modality choice was delegated to each institution, thus unification across all patients was not possible and SSEP was not evaluated. Second, imaging parameters were not collected and could not be evaluated. Third, details of non-attributed alerts were not collected. The fourth is the heterogeneity of collected cases. The incidence of postoperative paralysis and PPV may be higher than in the general case because of the composition of facilities that are more likely to perform high-risk spine surgeries. This is still a preliminary study, and evaluation of a larger number of cases is required to analyze factors in more detail.
In conclusion, factors affecting PPV at the 70% threshold were analyzed. Surgeons are strongly encouraged to use Tc-MEP in patients with preoperative motor deficits, regardless of whether they are undergoing high-risk spine surgery or not. Recording the characteristics of PPV will greatly assist in performing effective Tc-MEP and may minimize neurological complications upon appropriate intervention.
Footnotes
Author Contributions
Conceptualization: MF, TK and GY. Methodology: MF and TK. Data curation: MF Formal analysis: MF. Investigation: MF, TK, GY, MM, HU, SK, MA, KY, HI, HS, YF, NT, MT, ST, KW, NY, AY, SM. JH, TT, KK, KA, KKu, NS and HN. Resources: MF, TK, GY, MM, HU, SK, MA, KY, HI, HS, YF, NT, MT, ST, KW, NY, AY, SM. JH, TT, KK, KA, KKu, NS and HN. Writing—original draft preparation: MF. Writing—review and editing: TK, GY, MM, HU, SK, MA, KY, HI, HS, YF, NT, MT, ST, KW, NY, AY, SM. JH, TT, KK, KA, KKu, NS, HN, KN, KT, YM and SI. Visualization: MF. Supervision: NK, KT, YM and SI. All authors contributed to the article and approved the submitted version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.