
Abstract
Study design
Retrospective cohort study.
Objectives
This study aimed to investigate the failure of the caudal end of lumbar posterior fixation in terms of pre-operative and post-operative spinopelvic parameters, correction performed, demographic and clinical data.
Methods
The lumbar, thoraco-lumbar and lumbo-sacral posterior fixations performed with pedicle screws and rods in 2017-2019 were retrospectively analyzed. As 81% failures occurred within 4 years, an observational period of 4 years was chosen. The revision surgeries due to the failure in the caudal end were collected in the junctional group. Fixations which have not failed were gathered in the control group. The main spinopelvic parameters were measured for each patient on standing lateral radiographs with the software Surgimap. Demographic and clinical data were extracted for both groups.
Results
Among the 457 patients who met the inclusion criteria, the junctional group included 101 patients, who required a revision surgery. The control group collected 356 primary fixations. The two most common causes of revision surgeries were screws pullout (57 cases) and rod breakage (53 cases). SVA, PT, LL, PI-LL and TPA differed significantly between the two groups (P = .021 for LL, P < .0001 for all the others). The interaction between the two groups and the pre-operative and post-operative conditions was significant for PT, SS, LL, TK, PI-LL and TPA (P < .005). Sex and BMI did not affect the failure onset.
Conclusions
Mechanical failure is more likely to occur in patients older than 40 years with a thoraco-lumbar fixation where PT, PI-LL and TPA were not properly restored.
Keywords
Introduction
Posterior instrumented fixation is a well-established treatment for patients with adult or adolescent idiopathic scoliosis 1 and adult spine deformity. 2 This type of correction aims to achieve a balanced spine in the coronal and sagittal plane while preserving as much functional motion as possible,3,4 avoiding future complications. 1 Complications after spine surgery include adjacent segment pathology: although at the proximal end of instrumented fusions this complication has been well described, substantially less has been documented about distal adjacent segment pathology.
In 2006, Lowe et al, 5 first defined the progression of the kyphosis below the instrumented segment as distal junctional kyphosis (DJK). They described DJK radiographically, as a Cobb angle in the sagittal plane higher than 10° in the caudal end of the fusion. DJK is also described as implant failure at the caudal end of fixation (DJF).6,7 Distal junctional failure (DJF) has been reported as a complication of adult and adolescent idiopathic scoliosis, adult spine deformity and Scheuermann’ kyphosis. 7 DJF requiring revision surgery can be caused by component failure, such as breakage of the rods or screws, but also by screws loosening (eg pseudoarthrosis). Additional mechanisms leading to DJK are degenerations of the adjacent intervertebral disc and/or vertebra.6,8
Additionally, Zanirato et al, 9 reviewed the complications in adult spine deformity surgery. They found that instrumentation failure, adjacent segment degeneration, proximal junctional kyphosis and hardware related symptoms were the most frequent long-term complications. Although mechanical complications are often described as the most relevant, they have a lower incidence than expected, suggesting underreporting.
When adults with spinal deformity are treated, special attention should be placed on sagittal alignment, because this radiographic parameter is strongly associated with pain and disability. 10 Sagittal imbalance is commonly defined as the sagittal vertical axis (SVA). 11 However, the SVA alone is suspected to underestimate the sagittal alignment 12 because it could be modified in presence of compensatory mechanisms, such as pelvic retroversion or knee flexion.11,13-15
As reported by Lafage et al, 16 the pelvis plays a fundamental role in the chain of correlation between spine and lower limbs with respect to the sagittal balance. In particular, the SVA, the pelvic tilt (PT), and the mismatch (PI-LL) between the pelvic incidence (PI) and the lumbar lordosis (LL) are highly correlated with pain and disability 16 and were used to set thresholds of correction for realignment procedures. 12 Therefore, the above-mentioned spinopelvic parameters should be included in a classification system.
The fact that the pelvic alignment is related to sagittal spinal alignment, and postoperative pelvic parameters are tightly correlated both to pain and spine-related disability was the rationale behind the new SRS-Schwab classification. 10 This modified classification, in fact, is based on frontal curve types and sagittal curves modifiers, including pelvic parameters. 17
While the importance of several spinopelvic parameters has been hypothesized, to date their correlation to the incidence of DJF has been poorly assessed. Moreover, the correlation between the ranges of the different spinopelvic parameters and the different modes of failure leading do DJF has not been completely assessed.
The aim of this retrospective study was to investigate the failure of instrumented posterior stabilisation of the lumbar spine in the caudal region requiring revision surgery. In detail, this study aimed to assess: • If differences exist between successful and failed surgeries, in terms of pre-operative spinopelvic parameters; • If differences exist between successful and failed surgeries, in terms of correction performed (correction levels, number of instrumented levels, use of cages); • If differences exist between patient groups based on age, sex, indications for surgery, BMI; • The incidence of the individual and combined mechanisms leading to these failures; • If post-operative variations of the spinopelvic parameters are predictors of failure.
Materials and Methods
Ethics
This study was approved by the local Ethics Committee (Comitato Etico di Area Vasta Emilia Romagna- AVEC, prot. number 0014318, September 30th, 2021). Study-specific informed consent was not required for this retrospective study, due to the regulations relevant to health institutions dedicated to scientific research.
Study Design
All the spine surgeries performed at the Spine Surgery Unit of our Institution, between January 2017 and December 2019 were retrospectively analysed (Figure 1). Patients with short segment fusions at our Institution are followed up for at least 4 years (twice during the first year, at least once per year at least up to the fourth year post-op). Longer fixations are monitored more frequently and for a longer period. Workflow of the retrospective study.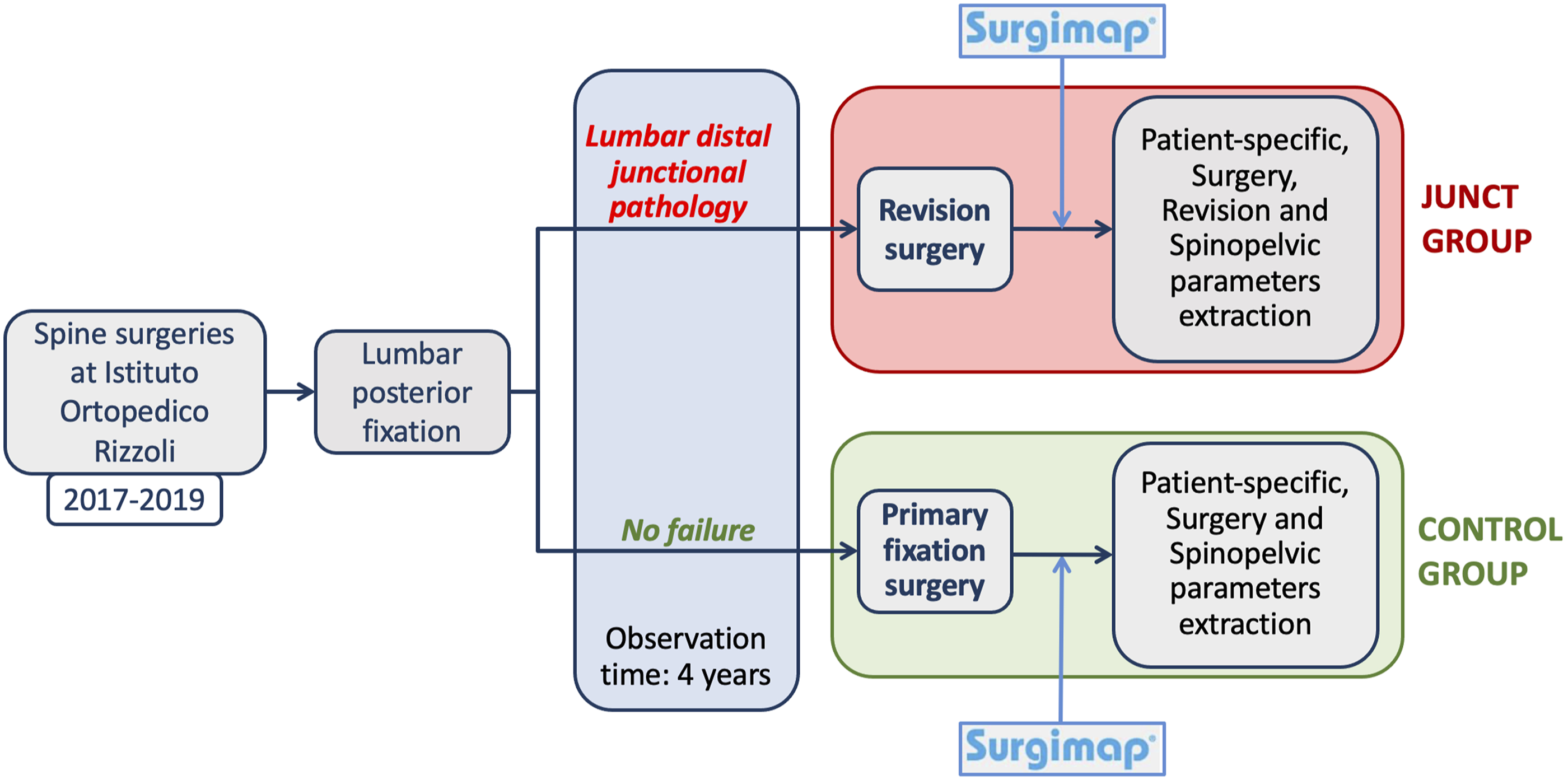
The medical histories, surgical reports, follow-up reports, and all the diagnostic images (radiographs, CT and MRI images) of all the patients that were uploaded into the digital archive of the hospital were evaluated. The evaluation identified all cases of failure caused by distal junctional pathology.
The inclusion criterion was: all posterior spinal stabilisation procedures which included the lumbar region. The study therefore included also thoraco-lumbar fixations, as well as fixations involving the pelvis. Only posterior fixations performed with pedicle screws and rods were considered: all cases which used anterior fixation, fixation with pedicle hooks, magnetic or growing rods were excluded from the study. Revision surgeries due to a proximal failure or a distal failure in the cervical or thoracic regions were excluded. Patients with junctional pathology without failure were excluded. No age or pathology restrictions were applied. Previous surgeries at the spine or at any other anatomical district were not considered as exclusion criteria.
The included cases were categorised into two groups: the junctional failure group (Junct) and the control group (Control). Specifically, a patient was assigned to the junctional group if a failure occurred in the last instrumented fused level or in the vertebra immediately caudal, with one or more of the following causes: i) Pullout of the pedicle screws and/or ii) Mechanical breakage of the rods in the caudal half of the fixation, or breakage of one or more of the caudal-most pedicle screws and/or iii) Vertebral fracture and/or iv) Degeneration of the intervertebral disc with a Pfirrmann’s score
18
of 4 or higher.
Demographic and clinical data, including sex, age at surgery, Body Mass Index (BMI), number of fused levels, presence and number of cage(s), were extracted both for the Junct and for the Control groups. Additionally, in the junctional group, causes of failure and timing of onset of junctional pathology were also analysed.
The frequency of failure was analysed by years post-operation. Revision surgery performed within 4 years after fixation surgery accounted for 81% of the patients of the junctional group (as detailed in Section Demographics and Causes of Failure of the Results). For this reason, an observational period of 4 years was considered. Therefore, in order for the two groups to be comparable, only patients with an observational period of at least 4 years were included. As the observation period was 4 years, the Junct group included all and only those cases who underwent revision within 4 years after surgery. The control group included all those patients with a posterior spine fixations, which did not present complications or failure, or required modifications or removal of instrumentation in the 4 years after primary surgery (ie also those case who possibly failed after the fourth year).
Radiological Measurements
The spinopelvic parameters were measured for both groups (Junct and Control) from available lateral standing radiographs including the whole spine, or at least the C2-femoral heads range. For each patient, the images before surgery (pre-op) were examined. Similarly, the images after the primary fixation surgery were examined (post-op, ie as soon as the patient could undergo standing radiographs and in all cases no later than 1 month post-op). In case of implant failure, the lateral standing radiographs just before the revision surgery (pre-rev) were also evaluated.
The spinopelvic parameters were extracted using the software Surgimap (Nemaris Inc, New York, NY, www.surgimap.com). Surgimap is a free software with tools for the surgical planning that integrates spine-related measurements in combination with data from the published literature, which has been extensively validated. 14
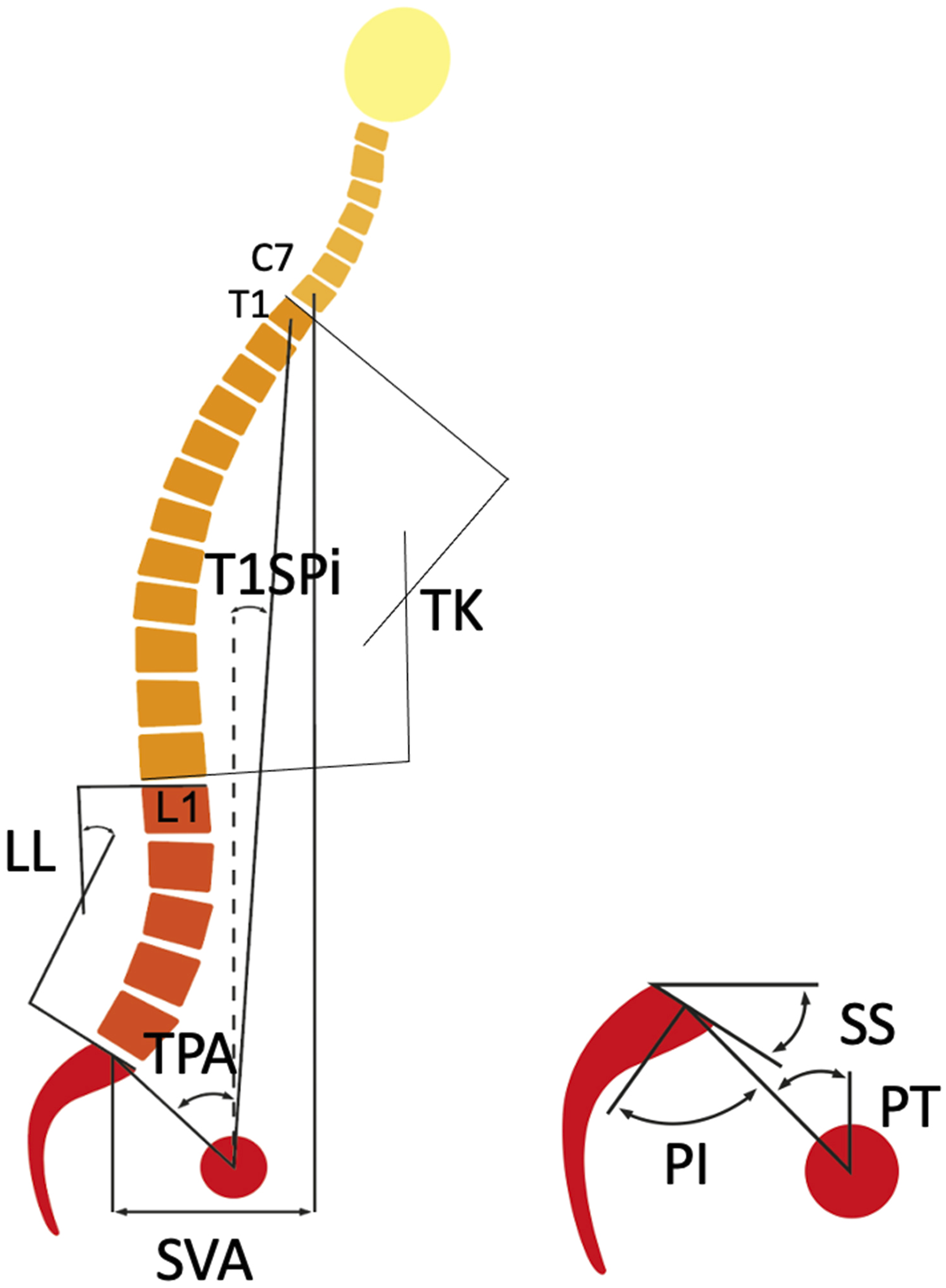
The following spinopelvic parameters, as defined in11,19-22, were measured for each patient (Figure 2): • SVA: this was considered negative if the plumb line from C7 was posterior to the posterior corner of the sacrum; • PI; • PT; • Sacral slope (SS), • Thoracic kyphosis (TK); • LL; • The mismatch between the pelvic incidence and the lumbar lordosis (PI-LL); • T1 pelvic angle (TPA), defined as the angle between the line from the femoral head axis to the centroid of T1 and the line from the femoral head axis to the middle of the S1 superior end plate
23
; • T1 spinopelvic inclination (T1SPi), defined as the angle between the vertical plumbline and the line from the femoral head axis to the centroid of T1.
16
Spinopelvic parameters measured on the standing lateral radiographs using Surgimap.
For certain patients, some of the radiographs were missing because they were not acquired or were not uploaded to the orthopaedic database, or did not include the entire spine. For these patients, the spinopelvic parameters were measured at all the time points where suitable images were available, and were missing at the other time points. For instance, the post-operative image might have been missing, whereas the pre-operative was available and analysed. This was not correlated to a specific patient group and therefore did not introduce any bias.
Statistical Analysis
The distribution of each data was tested for normality using the Shapiro-Wilk test. The quantitative parameters are reported as mean and standard deviation (SD). The qualitative parameters are described as frequencies (%).
A repeated-measures mixed-effect model for each spinopelvic parameter was created from the pre-op and post-op data of both groups. This was used to analyse the effect of the group, time, and interaction between the two factors on each spinopelvic parameter. Repeated-measures mixed-effects models with post-hoc Tukey’s multiple comparisons tests were also performed on Junct data to assess variations of each parameter before and after the fixation surgery and before the revision.
Univariate and multivariate logistic regression models were applied to investigate for baseline differences in sex, age, BMI, primary diagnosis, number of instrumented levels and number of cages between the two groups. Continuous variable, as age, BMI, instrumented levels, and number of cages were categorized into classes. According to clinicians, age at the fixation surgery was divided into the following classes: 0-20 years, 21-40 years, 41-65 years and >65 years. BMI classification followed the standard classification: <18.5, 18.5-24.9, 25-29.9 and >30. To grant sufficient statistical power, the different obesity levels were not separated (BMI >30), as this would result in some classes being underrepresented. The instrumented levels were categorized as only lumbar fixation, thoraco-lumbar fixation from a lumbar vertebra up to T10 at maximum, and long thoraco-lumbar fixation with the upper instrumented vertebra higher than T10. The number of cages was categorized according to the number of cages actually inserted in each patient: zero, one, two or three cages. For a more in-depth investigation of only lumbar fixation, a univariate logistic regression test was applied to identify the probability of failure of L4-Sacrum levels.
The relationship of lumbar spinopelvic parameters with PI were assessed. The linear regression of PT vs PI, SS vs PI and LL vs PI were calculated before and after the fixation surgery, for both groups (in total 4 linear regressions for each comparison). The difference in the linear regression between Junct and Control was assessed with the Z test.
A P-value smaller than .05 was considered significant. All statistical analyses were performed using GraphPad Prism (Windows version 9.3.1, GraphPad Software, La Jolla, CA, USA).
Results
Demographics and Causes of Failure
A total of 1690 spine surgeries were explored and included in the initial screening. Among these cases, 125 (7.4%) patients required a revision surgery due to lumbar distal junctional pathology on average within 36 months of the primary fixation surgery. 101 revisions (81%) were performed within 4 years after the primary fixation surgery (Figure 3). As the risk of failure is mainly concentrated within the first 4 years, and in order to have comparable observational period among all fixation surgeries, only patients with an observational period of 4 years were included in the analysis. Number of revision surgeries by years after the primary fixation surgery. Within the fourth year (dashed bars), 81% of the total revisions have been performed.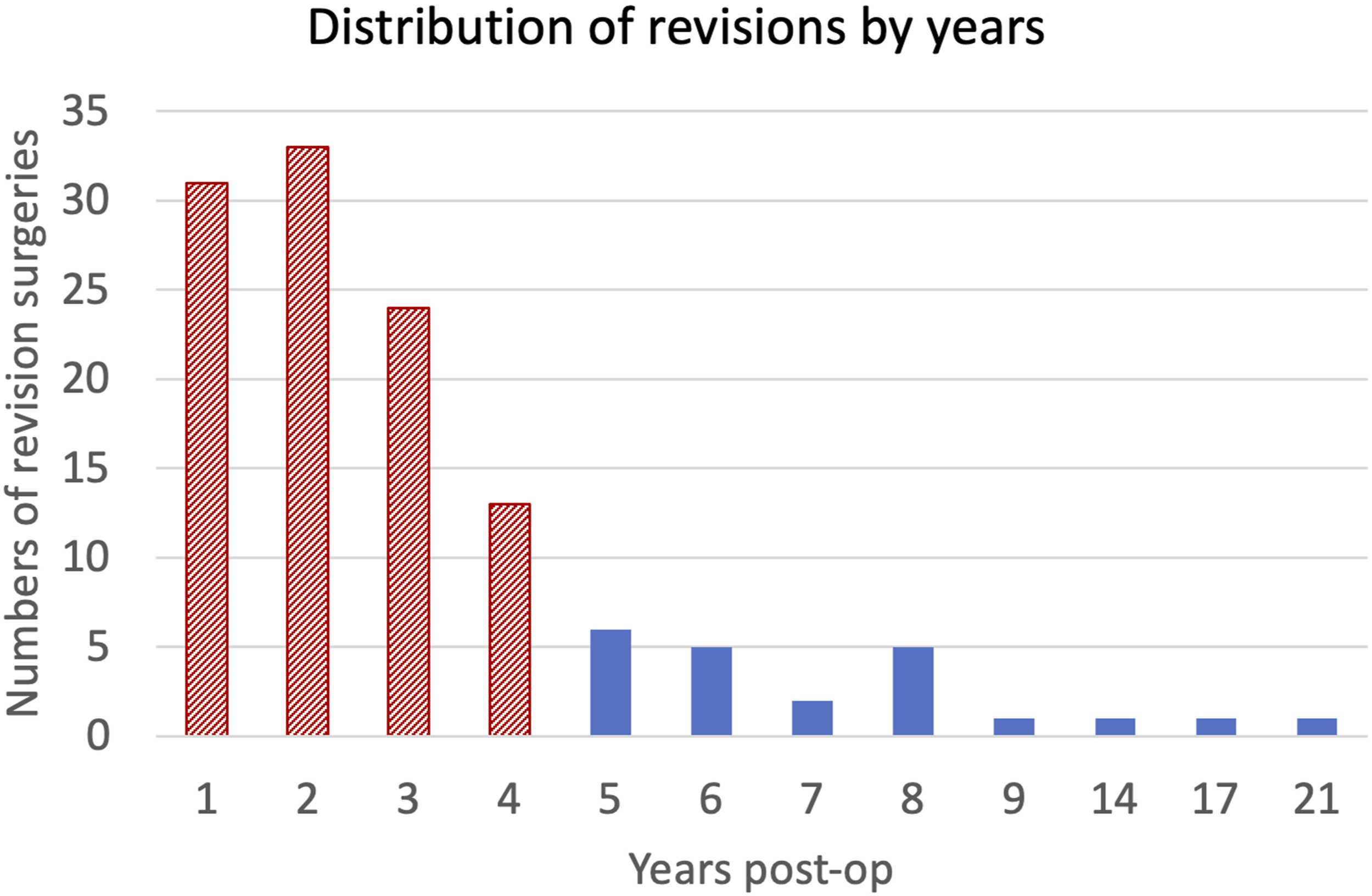
Summary of Patients’ Data for Junct and Control Group.

aAverage ± standard deviation.
The mean age was 61 ± 13 years for Junct and 45 ± 22 years for Control. The average BMI was 26.7 ± 5.0 kg/m2 for Junct and 23.8 ± 4.8 kg/m2 for Control. Demographic and clinical data, for the Junct patients, were those at the time of the primary fixation surgery.
The level of the lower instrumented vertebra (LIV, most caudal) was recorded both for the Junct and for the Control groups (Figure 4) Percentage of the lower instrumented vertebra (LIV) in fixations of both Junct and Control groups. Patients with LIV in sacrum and in ilium were considered together, because in both cases the pelvis is fixed to the spine. Note: *In the Junct group were included also the patients with LIV in T12 who required the revision surgery due to L1 vertebral fracture.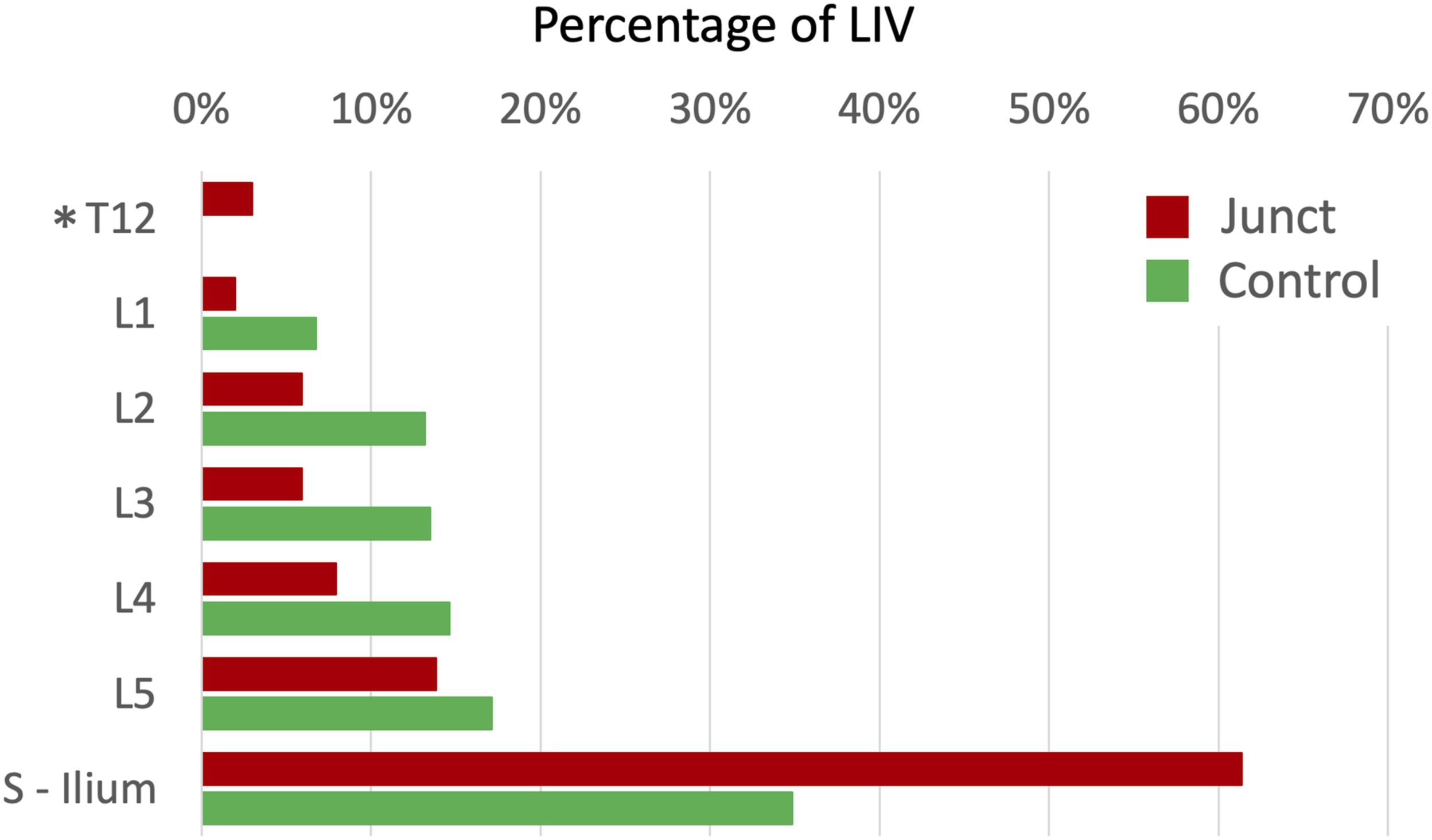
In 57 cases, the lumbar distal junctional pathology presented screws pullout and in 53 cases rod breakage. Vertebral fracture and disc degeneration occurred in 10 and 7 cases respectively. 26 cases presented more than one failure mechanism; in particular, 65% of cases presented both screws pullout and rod breakage (Figure 5). Left: mechanisms of failure which determined the revision surgery in the junctional group (Junct). Right: In 26 patients more than one mechanism of failure was present: the pie chart summarizes how the combinations of 2 or more mechanisms were distributed.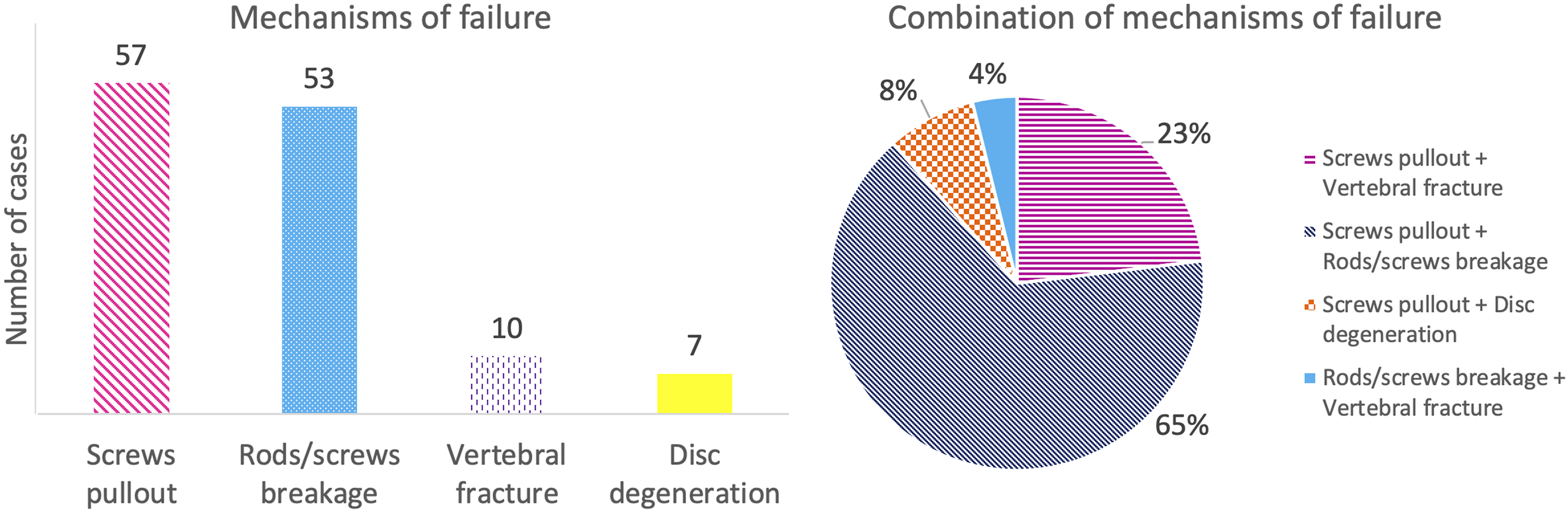
Variation of the Spinopelvic Parameters From Before to After Primary Surgery
• SVA showed statistically significant differences between Junct and Control groups (P < .0001) but not between the pre- and post-operative condition (P = .11) and between the two factors (P = .12). • PT showed statistically significant differences between the two groups (P < .0001) but not between the pre- and post-operative condition (P = .34); the interaction between the two factor was statistically significant (P < .0001). • SS did not show statistically significant differences neither between the pre- and post-operative condition (P = .61) nor between the two groups (P = .27); the interaction between the two factors was statistically significant (P = .0021). • LL showed statistically significant differences between the two groups (P = .021) but not between the pre- and post-operative condition (P = .56); the interaction between the two factor was statistically significant (P = .0044). • TK did not show statistically significant differences neither between the pre- and post-operative condition (P = .85) nor between the two groups (P = .33); the interaction between the two factors was statistically significant (P = .0048). • PI-LL showed statistically significant differences between the two groups (P < .0001) but not between the pre- and post-operative condition (P = .26); the interaction between the two factor was statistically significant (P = .0017). • T1SPi did not show statistically significant differences neither between the pre- and post-operative condition (P = .18) nor between the two groups (P = .085); also, the interaction between the two factors was no statistically significant (P = .85). • TPA showed statistically significant differences between the two groups (P < .0001) but not between the pre- and post-operative condition (P = .23); the interaction between the two factor was statistically significant (P = .0018).
Figure 6 shows the change for each spinopelvic parameter from the pre-to the post-operative condition, for the Junct and for the Control groups. Changes between pre-operative and post-operative values for each spinopelvic parameter. The dashed line represents the junctional group (Junct); the solid line represents the control group.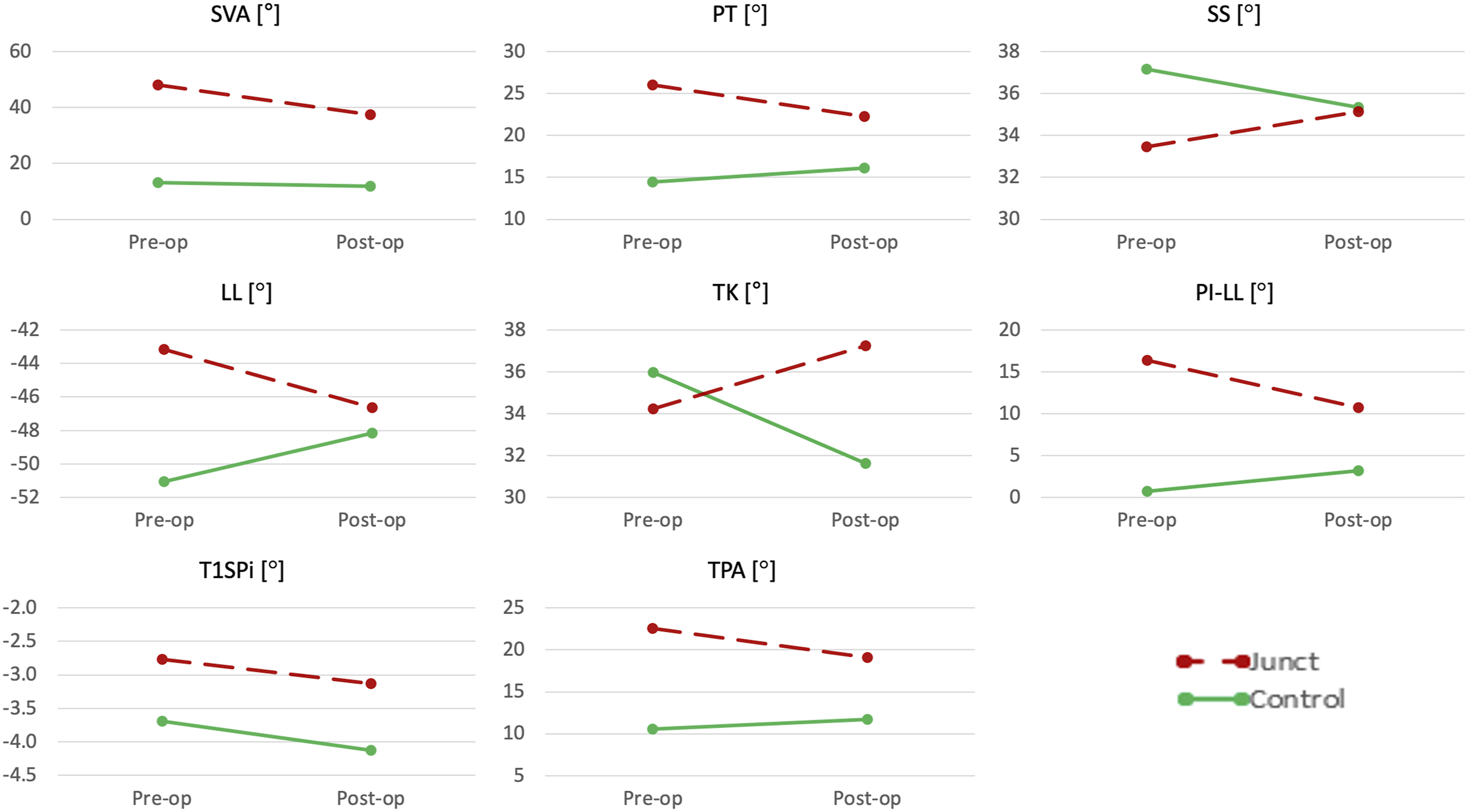
Evolution of the Spinopelvic Parameters in the Junctional Group
All the Junct spinopelvic parameters, apart from TK, statistically differed before the revision surgery compared to the post-operative fixation (SVA: P = .0009, PT: P = .0001, SS: P = .0006, LL: P < .0001, PI-LL: P < .0001, T1SPi: P = .016, and TPA: P < .0001). PT, TK, PI-LL and TPA were significantly modified (PT: P = .0024, TK: P = .028, PI-LL: P = .022 and TPA: P = .038) with the fixation surgery. PT, PI-LL and TPA decreased, while TK increased. SS and LL showed statistically significant differences before the revision surgery compared to pre-operative values.
Correlation Between Probability of Failure, and Demographics and Spinopelvic Parameters
Both the patient’s sex, and the primary diagnosis did not significantly influence the risk of junctional pathology onset (P = .48 and P = .52, respectively). Therefore, these two parameters were not included in the multivariate logistic regression model. The multivariate logistic regression model showed that patients younger than 40 years at the time of the first fixation surgery had a lower probability of developing a distal junctional pathology with respect to patients older than 65 years (age 0-20: OR = .13 and P = .0016; age: 21-40: OR = .021 and P < .0001). Patients aged between 40 and 65 did not significantly differ (P = .20). The lumbar-only fixation showed a 30% lower risk of failure than the long thoraco-lumbar fixation, while the short thoraco-lumbar showed a 90% higher risk of failure than the long thoraco-lumbar fixation. BMI and number of cages did not show a significant effect on the risk of lumbar junctional pathology onset.
L4-Sacrum fixation did not show a higher significant probability of failure than lumbar only (P = .26).
Before the fixation surgery, there was no statistically significant difference between the linear regression for the Junct and the Control (PI vs PT: P = .053, PI vs SS: P = .049). In Junct, the linear regression of LL related to PI was found to be not significant (P = .14), thus, the linear regression was not comparable with the Control one. After the fixation surgery, only the linear regression of SS vs PI differed between Junct and Control (P = .032, PI vs PT: P = .57, PI vs LL: P = .83) (Figure 7). Linear regression of PT (top), SS (middle), and LL (bottom) vs PI before fixation surgery (pre-op, on the left) and after fixation surgery (post-op, on the right).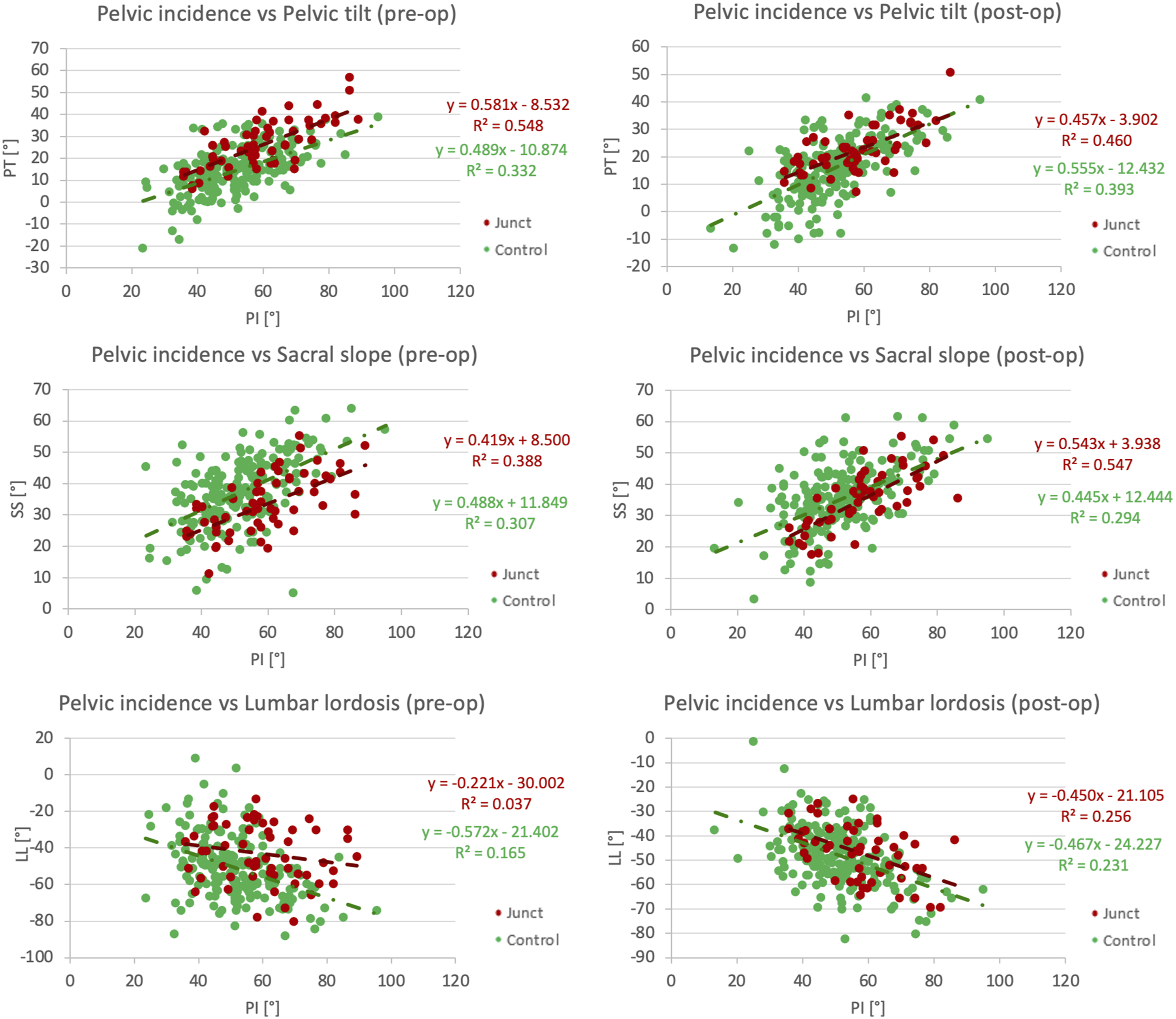
Discussion
This study aimed to explore the mechanical aspects of failures in the caudal region in lumbar, thoraco-lumbar and lumbo-sacral posterior fixation, and the mechanisms associated with these failures. Furthermore, this study investigated the correlation between the spinopelvic parameters and the incidence of distal junctional pathology.
This retrospective analysis of 1690 spine surgery showed that distal failure of fixation most frequently occurred within 4 years from the first fixation surgery. This is consistent with literature studies, in which a follow-up of at least 2 24 -5 years is generally analyzed. 25 In their revision Sciubba et al, 26 reported complications for adult spine deformity with a mean follow-up time of 3.49 years. Kwon et al, 27 found that the elapsed time between the index procedure and the patient’s presentation with symptomatic DJF was 8 months. In our study, we analyzed the time elapsed until the revision surgery, rather than until the appearance of symptoms.
In our cohort, screws pullout and rod breakage, individually or in combination, are the main factors which characterized lumbar distal junctional pathology. Similar to our study, Kwon et al, 27 found a prevalence of caudal pedicle screws pullout or migration in 11 over the 13 patients enrolled in their study, despite the fact that they did not include patients with trauma and tumours.
The spinopelvic parameters PT, SS, LL, TK, PI-LL and TPA had different trends in the junctional and control groups after the primary fixation surgery. SS showed similar values in the 2 groups, therefore suggesting it does not impact the probability of revision surgery.
PI in the junctional and control groups, were similar to the sagittal balanced and decompensated patients in Cho et al, 28 study. They found that a PI <55° had a higher probability to develop sagittal decompensation.
In our study, all the junctional spinopelvic parameters, apart from TK, significantly worsened before the revision surgery. The decline of the sagittal balance significantly impacted the likelihood of mechanical failure in the caudal end of the implant. Similarly, loss of lordosis seemed to accelerate degenerative changes at the adjacent segments, which could be associated with sagittal imbalance. 28 The fixation surgery significantly modified PT, TK, PI-LL and TPA. Surgical reduction of PT and PI-LL in the junctional group was not sufficient to fall within the recommended range, corresponding to good stability (PT <20° and PI-LL <10°), 17 and it correlates with the subsequent failure. Conversely, in the control group, PT and PI-LL were in the recommended ranges both before and after the fixation surgery.
TPA describes the sagittal alignment considering simultaneously both spinal inclination and pelvic retroversion. Protopsaltis et al, 23 demonstrated that a TPA lower than 14° correlates with a minimal disability (ODI = 20 points). Later, Banno et al, 29 and Li et al, 30 demonstrated that if postoperative TPA is lower than 19.3°, patients have better spinopelvic parameters and ODI scores. In our study, we found that post-operatively, the mean TPA was 11.7° for the control group, and 19.1° for the junctional group. The value of the control group correlated with a good alignment, as confirmed by. 23 In the junctional group, TPA decreased until the limit of an ODI score of 40 points, which indicated a moderate disability.29,30 This seems to indicate that, when the post-operative sagittal balance is marginally within the threshold, there are chances that it will get worse post-operatively, possibly leading to failure. In fact, before the revision surgery TPA worsened, increasing beyond 19.3° in 68% of patients. Pre-operatively, there was a difference of 12° between patients in the control group and those in the junctional group. TPA was lower than 14° only in the control group.
Therefore, our findings confirm that PT, PI-LL, and TPA are important parameters in the surgical planning of spine fixation surgeries as identifies if the sagittal balance has been restored or not. Failure to restore these parameters eventually led to failure.
The improvement of the mean post-operative SVA in the junctional group was associated with the mean PT, which remained higher than the Schwab 17 recommendation. PT quantifies the pelvic rotation around the femoral heads; it is also an indicator of pelvic retroversion, which is an established compensatory mechanism. An increase in PT correlates with increased pain and disability.16,31 For this reason, SVA alone did not permit accurate quantification of the sagittal balance, as it does not include information on how much this value is compensated for by increased retroversion. 14 In the sagittal alignment assessment, the information provided by SVA must be integrated with the other parameters. It is well-established that thoracic hypokyphosis, hip extension, pelvic retroversion, knee flexion and ankle dorsiflexion are compensatory mechanisms to compensate for sagittal malalignment.11,15 Only pelvic retroversion and TK could be assessed from the radiographs included in this study, while it was not possible to assess the effects of the other compensatory mechanisms.
T1SPi did not differ between the junctional and the control group; therefore, it did not seem to impact the sagittal balance or the probability of failure. Conversely, Lafage et al, 16 found a significant correlation between T1SPi and the clinical scores (HRQOL) in adult patients with spinal deformity. The study of Vialle et al, 20 reported similar values of T1SPi in healthy subjects compared to pre-operative values in the junctional group.
The spinopelvic parameters observed in both groups in this study were different from the normality ranges for healthy subjects.19,20 Generally, the subjects included in these past studies were mostly men, and much younger than the patients studied in this work.
LL in healthy volunteers in the work of Vialle et al, 20 was similar to pre-operative LL in the junctional group, while the value of pre-operative PT in the control group was comparable to the measured value in the above mentioned study.
The pre-operative sagittal imbalance was significantly associated with post-operative degeneration retrospectively.28,32 Brown et al 32 analyzed 16 adult scoliotic symptomatic patients who underwent a long thoraco-lumbar posterior fusion reaching down to L5, which required revision surgery due to the degeneration of the L5-S1 disc. The focus of their study and the limited number of patients could explain the differences to our study regarding the LL, TK and SVA values.
Similarly, Kumar et al 33 investigated the radiographic correlation between the sagittal plane modifications and the adjacent segment degeneration in lumbar fixation. They focused only on adjacent disc degeneration, without separating results with respect to the upper or lower levels of fixation. They also excluded patients with spondylolytic spondylolisthesis and degenerative scoliosis and used different target values to assess good spinal alignment. For these reasons, our results were not comparable.
The values of pre-operative, post-operative and pre-revision LL were reported by Kwon et al 27 differed from the ones in the present study. This difference could be due to the fact that they had a small patient cohort who required revision surgery with signs of distal junctional pathology, and they did not include patients with a primary diagnosis related to trauma and tumour.
The prevalence of female patients in both groups in our study indicated that women seemed to be more prone to spine deformity requiring fixation surgery, as was also found by.27,34 Merril et al 35 included patients with a minimum 5 levels fixations without distinguishing between fixation or revision surgery. As in this study, they found a prevalence of female patients. However, sex does not affect the result of treatment, as confirmed in, 34 and it is not a significant factor in the lumbar distal failure onset.
Fixation surgeries in our study were mainly performed due to non-oncologic pathologies rather than oncologic reasons. The probability of mechanical failure in the caudal end was similar between non-oncologic and oncologic patients.
According to the univariate analysis age, obesity, number of cages and length of fixation were found to be significant. Similarly, Soroceanu et al, 36 found that obesity was a significant factor in the development of complications in adult spine deformity surgery in the univariate analysis.
The multivariate logistic regression showed that age and length of fixation were the only 2 statistically significant parameters in both univariate and multivariate logistic regression models. A fixation including the thoraco-lumbar junction in patients older than 40 years old had a higher probability of developing junctional pathology in the caudal end compared to younger people with lumbar fixation. Similar to this work, Ayhan et al 34 found that the increase in age increases the probability of improvement of SF-36 PCS after posterior fixation due to adult spine deformity, until the breaking point of 37.5 age (1-year follow-up). Conversely, in Cho et al’s study 28 patient’s age did not affect the development of sagittal decompensation. In that study a cohort of less fifty patients with adult degenerative lumbar scoliosis were recruited in order to assess sagittal decompensation as the SVA higher than 8 cm.
In this study, patients with long thoraco-lumbar fixations had a higher probability to present junctional pathology and require revision surgery. In fact, the long level arm of the fused segment associated with an insufficient restoration of the sagittal alignment increased the flexion moment on the caudal junctional segment. The magnitude of this bending moment was able to exceed the mechanical resistance against flexion of the caudal junctional segment, and caused distal failure. 7
The equations obtained from the linear regression modelling of SS related to PI could help to assess postoperative SS, which could be used as a guideline for the risk of junctional failure. Le Huec and Hasegawa, 37 Legaye and Duval-Beaupere 38 and Schwab et al, 39 implemented a similar model of linear regression of PI vs PT, PI vs SS and PI vs LL using parameters obtained from healthy subjects. By comparing the three pre-operative linear regression models of this study with the past studies it was possible to observe that both the slope and the intercept of the linear regression for the control group are similar to the ones of the healthy subjects for PI vs PT. Conversely, for the PI vs LL only the control slope was similar. Conversely, the model which describes the relationship between the SS and PI was different between healthy subjects and patients scheduled for spinal fixation surgery. All three models fitted on the spinopelvic parameters of junctional people differed from the linear regression of healthy subjects.
As in all retrospective studies, one of the most critical factors was the availability of suitable radiological images: if the sagittal radiographs was not acquired or uploaded in the informatic database, or if it did not cover the whole spine, it was not possible to extract the spinopelvic parameters. The excluded/missing radiographs were less than 46% for both the junctional and control group. The missing data were quite equally distributed between the groups. For these reasons the spinopelvic parameters data were analyzed with mixed-effect models. Moreover, almost all the eligible radiographs of patients involved in this study were confined to the pelvis and proximal structures, so it was not possible to account for lower limb compensatory mechanisms.
Due to the large number of cases examined, only one trained observer measured all the spinopelvic parameters. However, Surgimap was previously validated with an accuracy of ±1.6 mm for distance and ±.4° for angle. 40 Therefore, the results provided can be assumed to have a similarly small uncertainty.
A further limitation relates to the fact that this is a radiographic study: outcomes do not account for the effect of neural element decompression, muscle quality, or other dynamic effects between balance and alignment.
It is possible that the different type of cages may correlate with implant failure. Because this is a retrospective study and several different cage models were implanted in the patients included in this study, it would not be possible to examine the cage as a statistical factor, so it was left as a confounding factor. The same applies to the type of screws and rods.
Finally, it is important to note that an exact incidence of lumbar distal junctional pathology will be difficult to determine as some patients requiring a revision surgery had their primary fixation surgery performed elsewhere and some of the patients had their fixation surgery at our institution could have developed lumbar distal junctional pathology and had a revision surgery elsewhere. 41
Conclusions
This retrospective study aimed to explore the mechanical failure of caudal instrumented posterior stabilisation of the lumbar spine, including the thoraco-lumbar junction and the pelvis. More than 80% of the mechanical failures occurred within 4 years of the primary fixation surgery.
The differences found between the control and the junctional groups confirmed that failure is more likely if the PT, the mismatch between the PI-LL and the TPA are not correctly restored.
To assess the sagittal balance the SVA alone should be carefully evaluated in relation to the PT and TPA, so as to take into account the pelvis compensatory mechanisms.
Fixations including the thoraco-lumbar junction were more prone to fixation failure with respect to the only lumbar fixation, while the number of cages did not significantly affect the risk of failure. Patients older than 40 years showed a higher probability of requiring a revision surgery due to the mechanical failure of the posterior fixation in the caudal end. Conversely, sex, primary diagnosis and BMI did not affect the likelihood of a mechanical failure onset. Screws pullout and rod breakage have been conformed as the primary causes of implant failure, alone or in combination. In the junctional group, a variation of all the spinopelvic parameters (except for TK) at follow up with respect to the post-operative values was observed.
Footnotes
Acknowledgments
The Authors wish to thank the entire team of the Spine Surgery division for the advice and stimulating discussions; Elisa Carretta for the statistics; Samuele Gould for revising the manuscript. The charity Re-Use with Love is gratefully acknowledged for the generous donation.
Author contributions
S.M. Conceptualization, Data collection, Data analysis, Statistical analysis, Data interpretation, Writing - original draft, Revising of the manuscript. C.G. Conceptualization, Data Collection, Revising of the manuscript. L.C. Conceptualization, Data analysis, Data revision, Founding acquisition, Revising of the manuscript, Supervision. M.G. and A.G. Conceptualization, Data interpretation, Revising of the manuscript. G.B. Conceptualization, Data interpretation, Revising of the manuscript, Supervision. All authors agreed and approved the submitted version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.