
Abstract
Study design
Retrospective study.
Objective
Spinal cord stimulation has been mainly used for the management of postsurgical persistent neuropathic. The purpose of the study was to evaluate the rate and causes for reoperation following spinal cord stimulation, and to identify risk factors for reoperation.
Methods
A retrospective study was conducted including patients who underwent surgical implantation of spinal cord stimulators within a 10-year period. The medical records of the included patients were reviewed for reoperations, demographics and certain clinical parameters. Demographics and clinical parameters were compared between patients with and without reoperations, and between patients with and without surgical site infections.
Results
Overall, 1014 index procedures and 175 reoperations were performed within the study period. At least 1 reoperation was performed in 97 (9.5%) cases. The most common cause for revision was lead migration or lead misplacement (n = 31, 3.0%). In 31 (3.1%) cases the stimulator was removed due to no pain relief. Surgical site infection that required reoperation developed in 30 cases (2.9%). Younger age was associated with a need for reoperation (Odds Ratio [OR]: .97,95% Confidence Interval [CI]:0.95-.99, P = .005), while higher Body Mass index and diabetes were associated with development of infection (OR: 1.05, 95% CI: 1.00-1.11, P = .036 and OR: 2.42, 95% CI: 1.05-5.47, P = .033 respectively).
Conclusions
The results of this study indicate that certain measures could improve the overall reoperation rate after spinal cord stimulation, such as accurate positioning of the spinal cord stimulators and design of smaller generators. Moreover, preoperative optimization of patients could result in lower complication rate, lower reoperations rate, and subsequently better clinical outcomes.
Introduction
Spinal cord stimulation is most commonly used for the management of neuropathic radicular and axial low back pain following lumbar spinal surgeries, while other indications include complex regional pain syndrome and degenerative disc disease. Although the exact mechanism of action for the spinal cord stimulation is not fully elucidated, these implants target the altered sensory signal which is the core pathophysiology involved in neuropathic pain. Spinal cord stimulators deliver electrical impulses to the dorsal columns of the spinal cord in a controlled fashion, resulting in orthodromic and antidromic activation of the large and myelinated A-beta nerve fibers and augmentation of inhibitory signals through activation of supraspinal nuclei.1-6 However, the results of spinal cord stimulation regarding pain reduction widely vary, with a reported rate of clinically significant pain relief ranging from 16% to 85%.7-12 It is still unknown which patients will demonstrate the greatest benefit from spinal cord stimulation and since these procedures are also associated with a high rate of complications, the risk-benefit equilibrium should be individually evaluated for each patient taking into consideration predisposing factors to success or failure.13,14 In this direction, more research is needed to accurately identify those predisposing factors for pain relief or development of complications.
Although there is a growing body of literature supporting the value and cost effectiveness of spinal cord stimulation in the management of persistent postoperative neuropathic pain in appropriately selected patients, the complications rate and risk factors associated with these complications have not been widely studied.15-17 Only small studies with short follow up have reported on the complication rate of spinal cord stimulation, while the evidence is even more scarce regarding the reoperation rate following these procedures. The lack of such information is a significant limitation for a reliable evaluation of the overall risk-benefit ratio of spinal cord stimulation in spine surgery. Infections have been reported to occur in approximately 1.5%–5% of patients following these procedures, and although this rate is similar to the infection rate of other instrumented spinal procedures, data regarding the infection rate in spinal cord stimulation again derive from small studies. 18 Moreover, even though there are well-established risk factors such as diabetes and smoking for development of infections in other common surgical procedures, the association of these risk factors with development of infection after implantation of spinal cord stimulators has not been validated in any study.
The primary purpose of the study was to evaluate the reoperation rate following surgical implantation of spinal cord stimulator, and to investigate the causes for reoperation following these procedures. The secondary purposes of the study were to identify any baseline clinical parameters or demographics associated with reoperations, and to identify any risk factors for surgical site infections that required reoperations following these procedures.
Methods
A single-center retrospective study was conducted including patients >18 years that they underwent surgical implantation of spinal cord stimulator over a 10-year period between January 2010 and November 2020. The study was approved by the Institutional Review Board of the hospital (Ref. No:20012022), while an informed consent from the included patients was not required due to the retrospective nature of the study. An electronic search in the hospital’s medical database was performed using relevant Common Procedures Terminology code (CPT) in order to identify the patients who underwent implantation of spinal cord stimulators. The retrieved medical records of the patients who underwent implantation of spinal cord stimulator in the cervical and thoracic spine were manually screened and assessed for any reoperation that was related to the spinal cord stimulators until March 2022. Moreover, the retrieved medical records were reviewed for certain baseline demographics and clinical parameters of the patients including age, gender, Body Mass Index, smoking status, diabetes and use of anticoagulants.
The number of reoperations for each index procedure was recorded, except from those that required to replace depleted generators. The operative reports of the reoperations from all cases were thoroughly read and examined. The reason for each reoperation was recorded along with other relevant information such as the time interval between the index procedure and the reoperation.
Statistical analysis
Statistical analysis included descriptive statistics of the study population regarding demographics, clinical parameters, and reoperations. Continuous variables are presented as means ± standard deviations (SD), medians and interquartile ranges [IQR], while categorical variables are presented as frequencies with percentages. Patients with and without postoperative infections, while also patient with and without reoperations were compared for age, gender, Body Mass Index, diabetes and smoking status using the non-parametric Wilcoxon rank sum test for non-categorical variables and the chi square test for categorical variable. In order to evaluate the independent association of these parameters with the need for reoperation for any cause, we performed a multivariable logistic regression analysis including age, gender, Body Mass Index (BMI), diabetes, and smoking status as independent variables and the need for reoperation as a dependent variable. Similarly, in order to evaluate the independent impact of these parameters on the development of an infection that requires a reoperation, we performed a multivariable logistic regression analysis including age, gender, BMI, diabetes, smoking status as independent variables and development of infection as a dependent variable. The STATA, version 15.0 (Stata Corp.) software was used for the statistical analysis, while statistical significance was set at a P value lower than .05 for all tests.
Results
Characteristics of the Study Population.
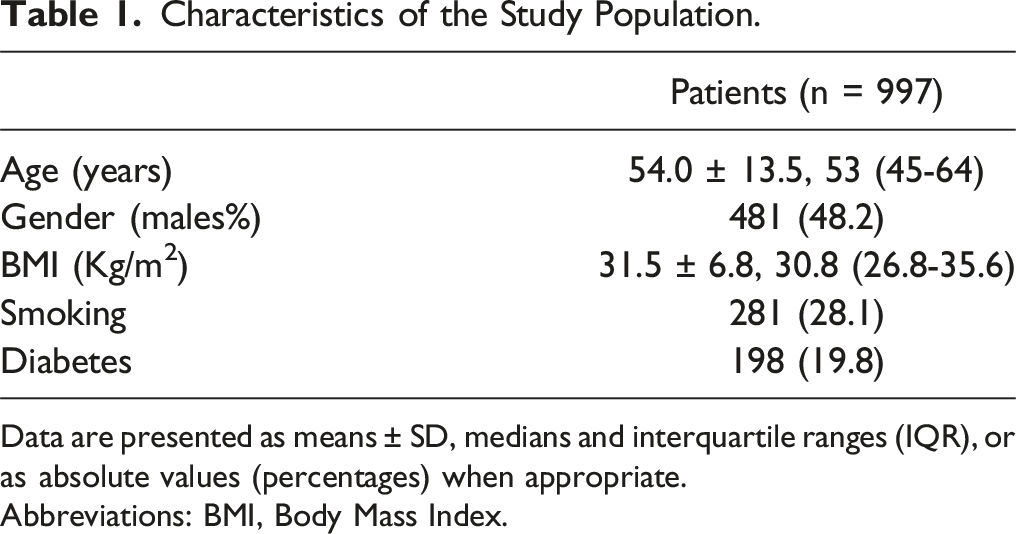
Data are presented as means ± SD, medians and interquartile ranges (IQR), or as absolute values (percentages) when appropriate.
Abbreviations: BMI, Body Mass Index.
Complications that Required Reoperation in the Study Population.
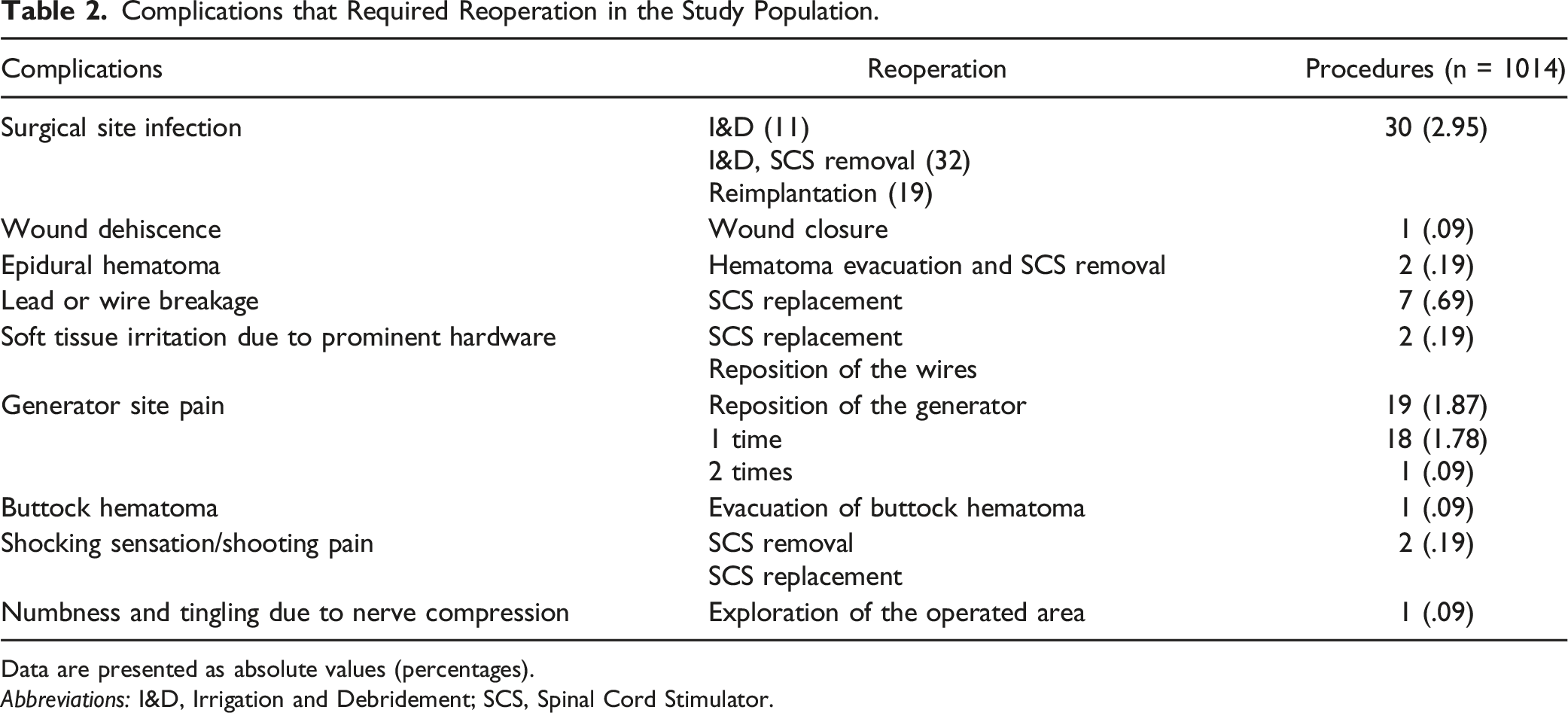
Data are presented as absolute values (percentages).
Abbreviations: I&D, Irrigation and Debridement; SCS, Spinal Cord Stimulator.
Reoperations related to Spinal Cord Stimulators in the Study Population.
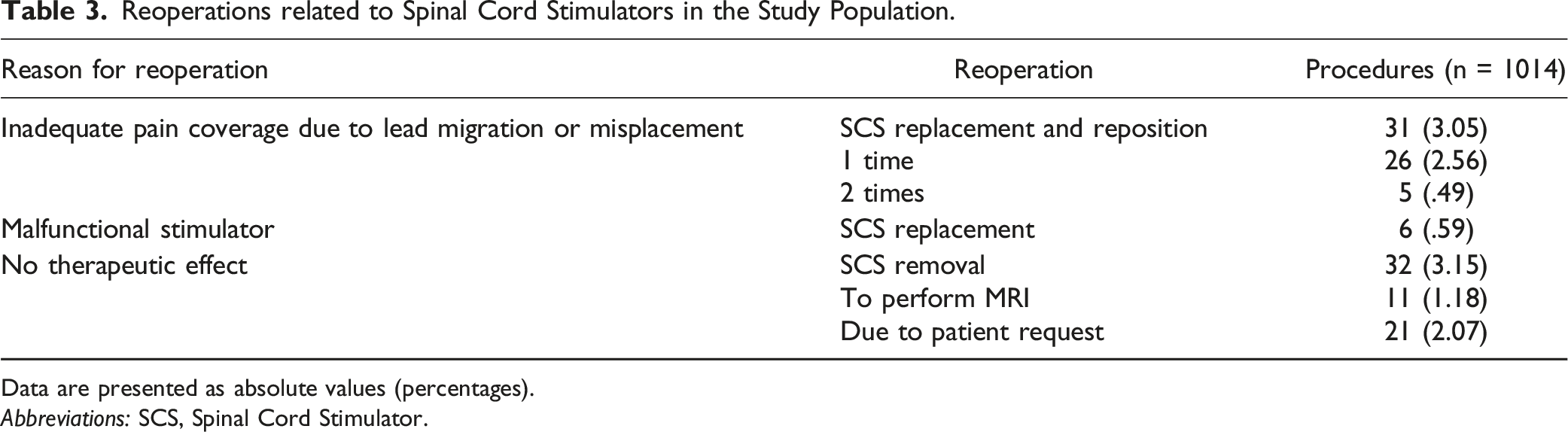
Data are presented as absolute values (percentages).
Abbreviations: SCS, Spinal Cord Stimulator.
Demographics and Clinical Parameters Between Patients With and Without Reoperations Following Implantation of Spinal Cord Stimulation.
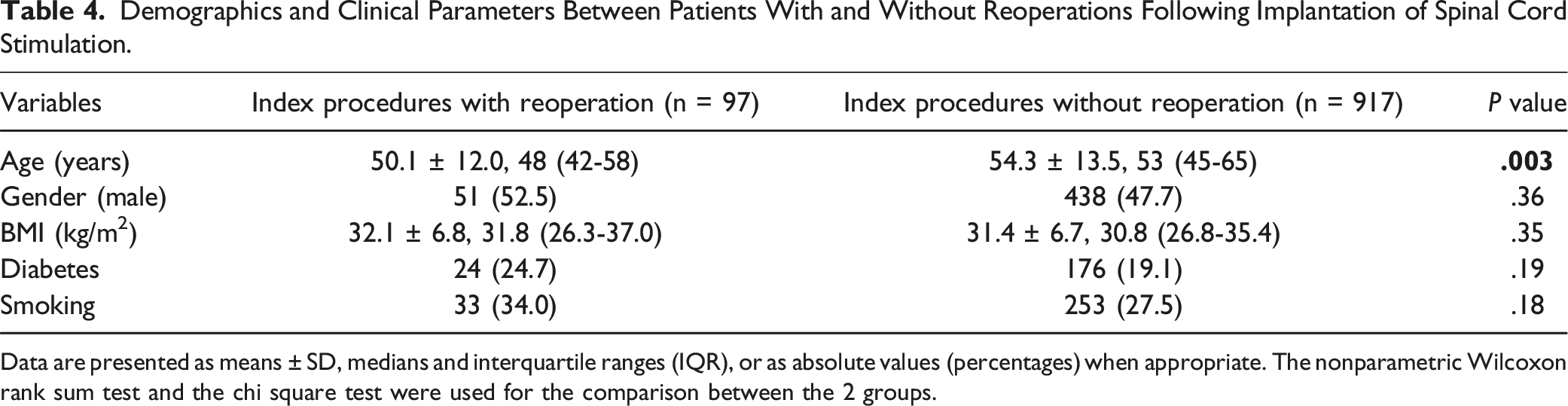
Data are presented as means ± SD, medians and interquartile ranges (IQR), or as absolute values (percentages) when appropriate. The nonparametric Wilcoxon rank sum test and the chi square test were used for the comparison between the 2 groups.
Demographics and Clinical Parameters Between Patients With and Without Surgical site Infections that Required Reoperation Following Implantation of Spinal Cord Stimulation.
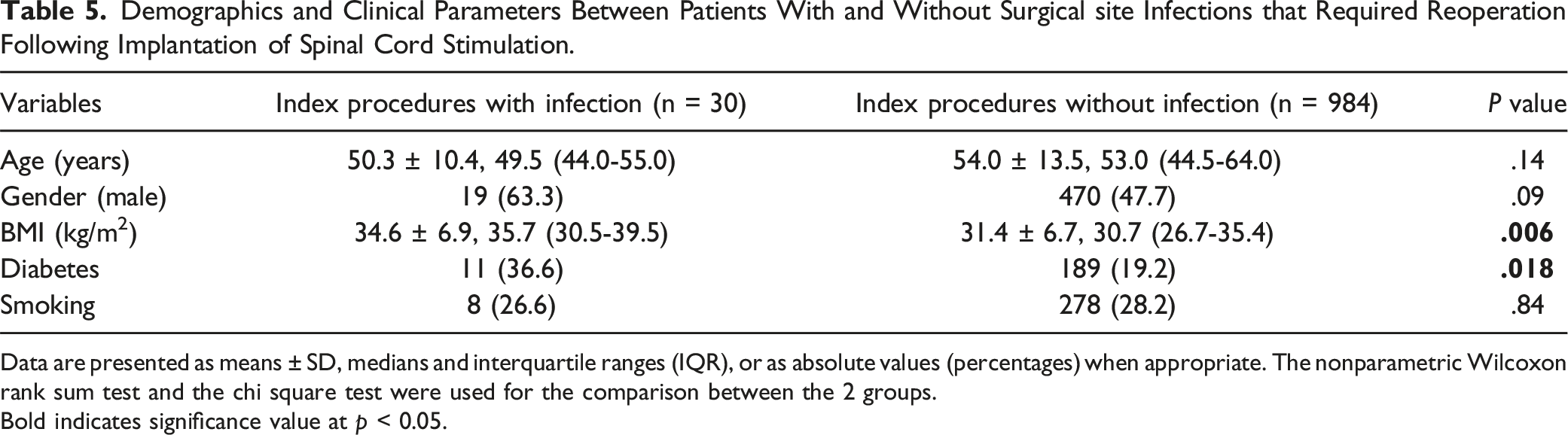
Data are presented as means ± SD, medians and interquartile ranges (IQR), or as absolute values (percentages) when appropriate. The nonparametric Wilcoxon rank sum test and the chi square test were used for the comparison between the 2 groups.
Bold indicates significance value at p < 0.05.
Results of the Multivariable Logistic Regression Analysis for Reoperation for Any Cause and Development of Infection as the Dependent Variables, with Age, Sex, BMI, Diabetes and Smoking as Independent Variables.
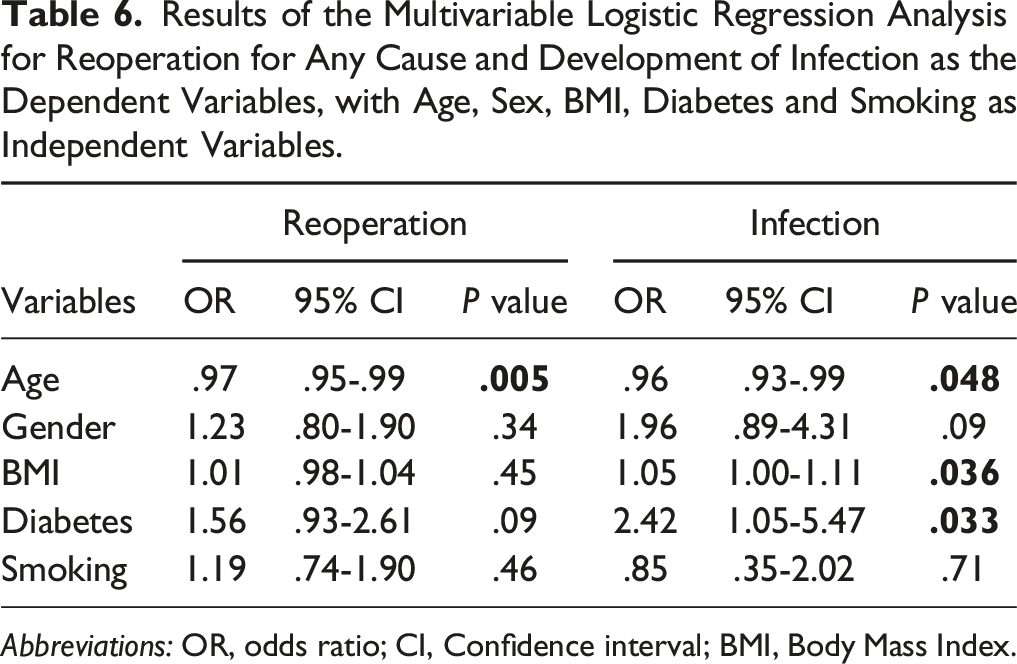
Abbreviations: OR, odds ratio; CI, Confidence interval; BMI, Body Mass Index.
Discusssion
Spinal cord stimulation has gained substantial clinical interest over the past decades for the management of persistent neuropathic as a cost-effective treatment modality.16,17 However, the evidence regarding the efficacy of spinal cord stimulation in pain reduction derived from only small studies with short-to-medium term follow up, while the complication and reoperation rates have not been widely evaluated. This is the largest study reporting on the reoperation rate following surgical implantation of spinal cord stimulators, providing also indirect information about the complication and success rate of these procedures. Although clinical outcomes regarding the efficacy of spinal cord stimulators in this study were not evaluated, 3.1% of the included patients in our study required removal of the stimulator due to lack of therapeutic effect. This indicates that the failure rate in terms of pain relief is higher than 3.1%, even though these patients had pain relief during the stimulation trial. Moreover, based on our findings, a reoperation was required in 9.5% of the cases, while in 2.9% of the cases the reoperation was related to surgical site infections. The most common cause for revision was lead migration or misplacement (3.0%) requiring a reoperation for repositioning or replacement of the stimulator for better pain coverage, while pain at the generator site was another frequent cause for reoperation occurring in 1.8% of the cases.
There are only few studies evaluating adverse events and complications following spinal cord stimulation, and even less reporting reoperation rates and causes for reoperation following these procedures.18-21 Among hardware-related adverse events, lead migration has been reported to be 1 of the most common causes for reoperation. In 1 of the largest serries in the literature regarding spinal cord simulation, Meckail et al retrospectively reviewed 707 patients who underwent implantation of spinal cord stimulators for various indications including failed back surgery and complex regional pain syndrome. 20 The authors reported that lead migration presented in 22.6% of their patients, much higher than in our study. Similarly, Shamji et al conducted a systematic review of prospective cohorts of patients who underwent implantation of spinal cord stimulators and they reported that lead migration or misplacement was 1 of the most common adverse events, occurring in 14.5% of the patients, also higher than in our study. 22 The higher frequency of lead migration in these studies compared to our study, may be due to the older design of implants that were used in these studies, while also we only reported complications that required reoperation, whereas this was not determined in these studies. More recent studies reported lower rates of lead migration, closer to the 1 revealed in our study. Gazelka et al conducted a retrospective study including 143 patients who underwent spinal cord stimulation and reported that lead migration requiring reoperation occurred in 2.1% of the cases, while Mekhail et al conducted a randomized trial including 134 patients who underwent implementation of spinal cord stimulators and reported that the most frequently reported adverse event was lead migration, presenting in 4% of the cases.21,23 The high frequency of lead migration or misplacement highlight the need to improve preoperative planning for an accurate positioning of the lead on the spinal cord, and to optimize the intraoperative technique of implementation. Moreover, preventive strategies for lead migration such as improved hardware and robust anchoring of the lead and the wires would further decrease the rate of this adverse event.
Pain at the site of the pulse generator is another complication that is commonly reported in the literature. Similar to our study, pain at the generator site was the second most common complication in the systematic review by Shamji et al. The authors of this systematic review reported that pain at the generator site waw evident in 9% of the included cases, while this occurred in 1.8% of our patients. In a recent randomized trial by Kapural et al, 159 patients were randomized to receive conventional medical management or surgical spinal cord stimulation for the management of nonsurgical refractory back pain. 24 Pain at the generator site was the most common adverse event in this study, occurring in 7 patients (4.8%), while in 3 of them (2.0%) a reoperation was required to reposition the implantable pulse generator. This is close to our reported rate of pain at the generator site that required reoperation (1.8%). The rate of pain at the generator site was 4% in another randomized trial by Mekhail et al, also similar to our study. 23 The high frequency of implantable pulse generator pocket pain indicates that industry research should focus on designing smaller generators in order to decrease the frequency of this complication and the overall reoperation rate.
Due to the small population size and the highly varying follow up of the available studies, the evidence regarding the infection rate in the literature is highly heterogenic, while risk factors for infections have not been evaluated in any previous study.20-24 The infection and wound dehiscence rate in the systematic review by Shamji et al was reported to be 5%, higher than the 1 observed in our study (2.9%). 22 Again, the higher infection rate in this systematic review could be attributed to the fact that the authors of the review reported the overall infection rate, while we recorded only those infections that required a reoperation. A similar high rate was reported in the large retrospective study by Mekhail et al, in which infections occurred in 4.5% of the patients following surgical implantation of spinal cord stimulators. 20 Moreover, the authors of this study aimed to investigate whether any baseline clinical parameters were associated with the development of infection. Specifically, the authors compared the infection rates between diabetic and non-diabetic patients and found that there was no difference in the infection rate between these 2 groups. A 1.4%- 2% infection rate was reported in recent randomized trials which enrolled 130-160 patients, lower than the previous studies and closer to the infection rate that was found in our study.23,24 Interestingly, Kapural et al in their randomized trial reported that all of their patients with infection underwent explanation of the device and reimplantation of the spinal cord stimulator following resolution of the infection, while in our study reimplantation of the spinal cord stimulator following resolution of the infection performed in 19 out of the 30 infection cases.
There are certain limitations of the study that must be addressed. First, we reviewed only complications that required a reoperation for their management, therefore we cannot accurately estimate the exact complication rate following spinal cord stimulation in our study population. Another limitation of the study is that we did not compare the reoperation and complication rates among different types of spinal cord stimulation in terms of waveform frequency, which could be potentially linked to certain causes for reoperation such as removal because of loss of therapeutic efficacy. Last, the rate of stimulators’ removals due to loss of therapeutic effect may have been underestimated since some patients may have been lost and treated in other institutions, therefore some removals of stimulators may have been performed elsewhere.
Conclusions
Conclusively, we found that surgical implantation of spinal cord stimulators was related to an overall reoperation rate of 9.5%, and the need for reoperation was associated with younger age. The most common reason for revision was lead migration or misplacement of the spinal cord stimulator which was evident in 3.0% of the patients, while also 3.1% of the patients did not experience any therapeutic effect and underwent removal of the spinal cord stimulator. Moreover, spinal cord stimulation was related to a 2.0% reoperation rate due to surgical site infections, while body mass index and diabetes were associated with the development of infection after implantation of spinal cord stimulators. Our results indicate that certain measures or strategies such as design of smaller generators, better preoperative and intraoperative planning for accurate positioning of the stimulator on the spinal cord, preventive measures for lead migration, and preoperative optimization of patients with risk factors for infection could result in lower complication and reoperation rates, and subsequently better clinical outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.