
Abstract
Study Design
Prospective cohort study.
Objectives
To show population variance in the Inflection Point (IP) and its role in defining maximum Thoracic Kyphosis (TK) and Lumbar Lordosis (LL).
Methods
468 asymptomatic adult volunteers were included in the Multi-Ethnic Normative Alignment Study (MEANS). To find parameters correlating with IP, the vertebrae and discs were numbered such that C7 was 0, T1 was 1, with T1-T2 disc being 1.5, etc. Statistical analysis was performed by a correlation matrix for IP and the 9 other selected parameters along with linear regressions.
Results
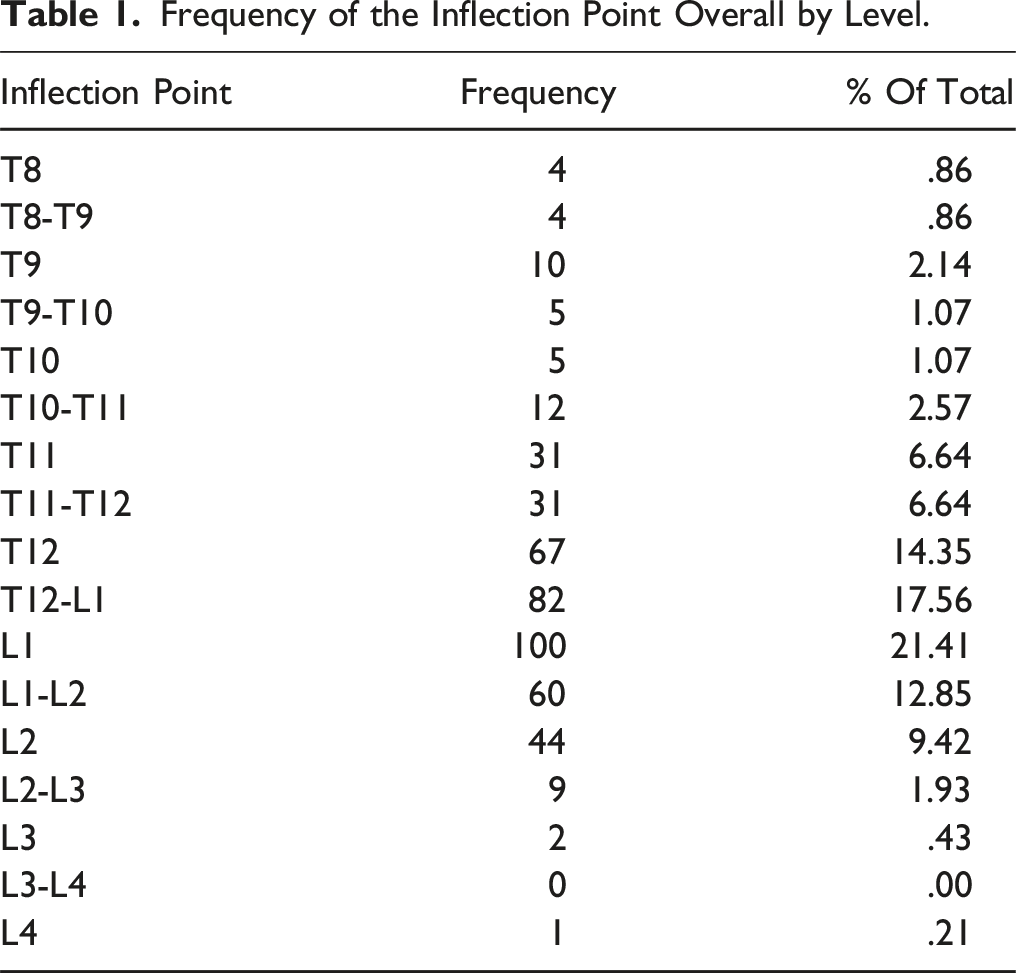
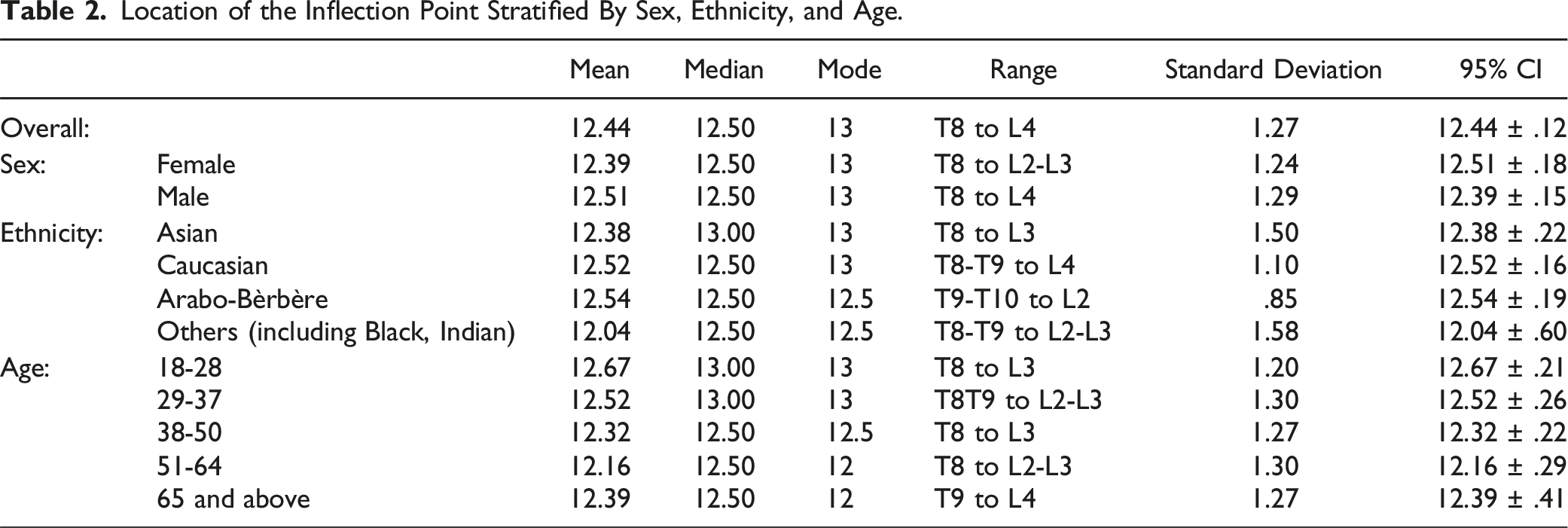
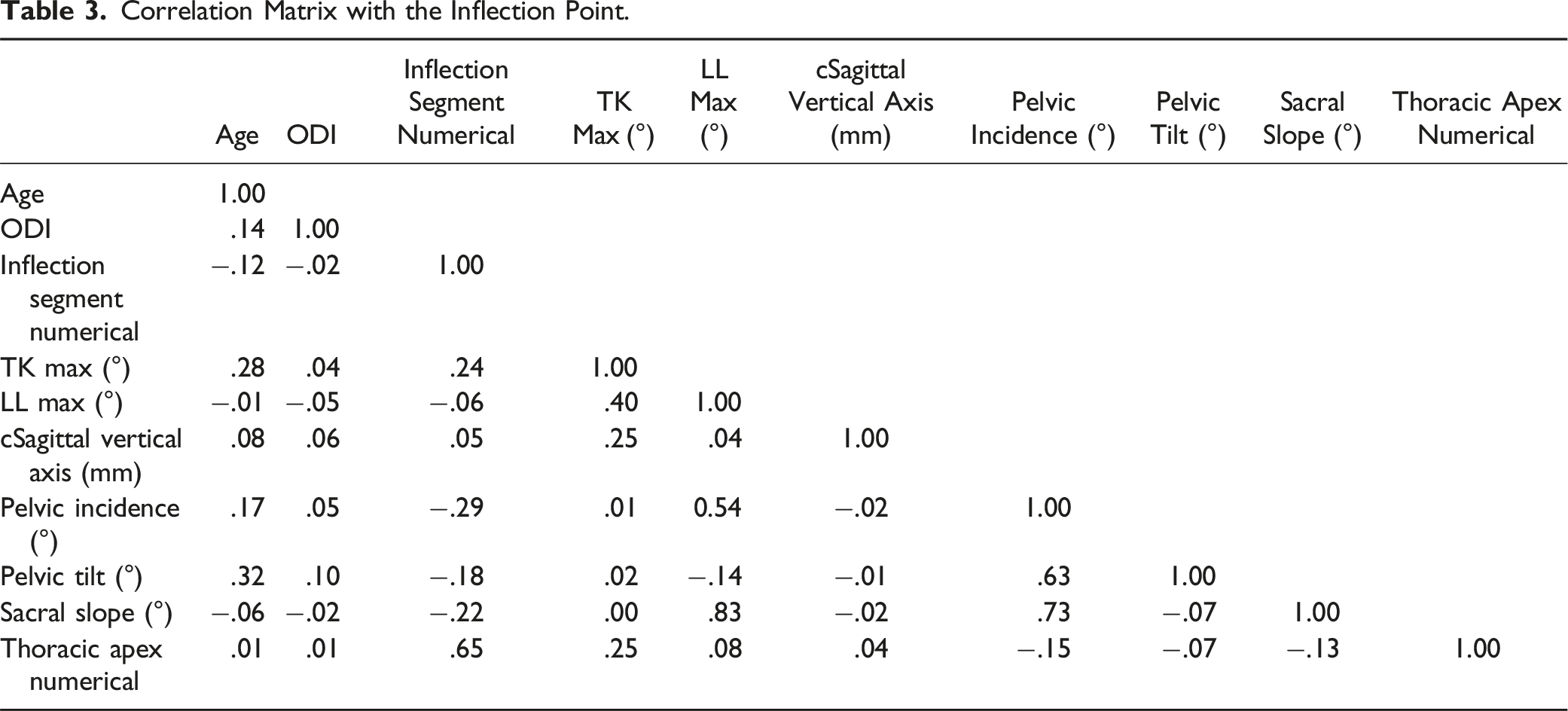
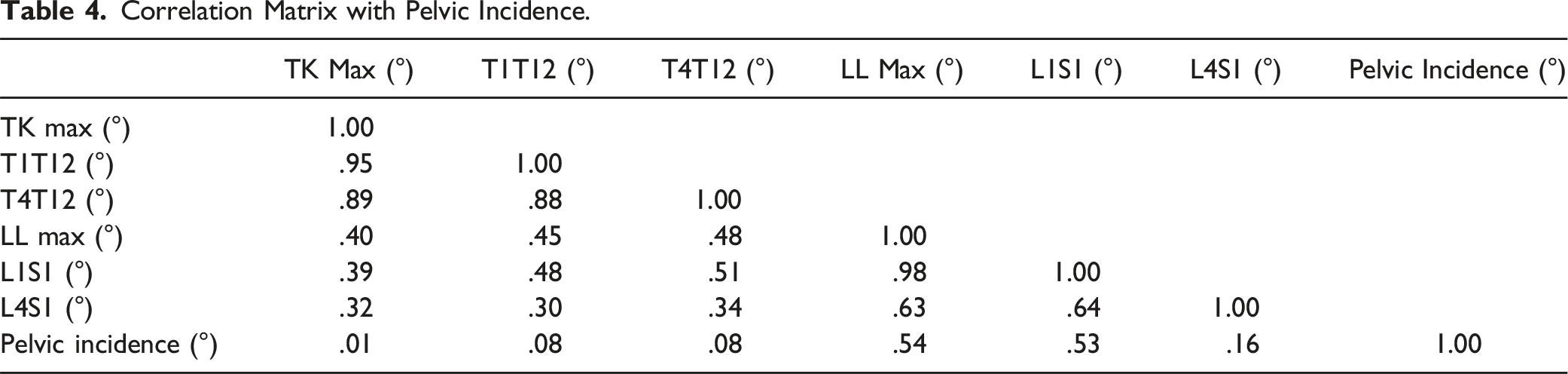
The overall mean IP was 12.44 approximately corresponding to T12-L1 disc with the median being 12.50, range was T8-L4. The cohort was then stratified by sex and ethnicity, but there was no significant difference in IP between groups. IP in younger subjects was 13 (L1), compared to 12.5 (T12-L1 disc) in older subjects (P < .05). IP was moderately correlated with the TK apex (r = .66). No strong correlation was found between IP and LL magnitude or apex, TK magnitude, sacral slope, or Pelvic Incidence (PI). In terms of other sagittal parameters, PI and LL demonstrated a significant positive correlation. PI and TK did not have a strong association.
Conclusions
The mean IP was at the T12-L1 disc, however IP ranged from T8 to L4. Older subjects tended to have a relatively more cephalad IP. No radiographic variable was found to be a strong predictor of the IP. TK apex was found to have a moderate correlation.
Introduction
Adult spinal deformity (ASD) can affect the coronal, sagittal, and axial planes. 1 ASD is a significant contributor to the global burden of disease 2 ; specifically, sagittal imbalance has been shown to have a significant association with poor health-related quality of life compared to coronal imbalance.3-5
The inflection point (IP) is known as the vertebra or disc in the spine that is a transition point from kyphosis to lordosis or vice versa. 6 Two inflection points exist in the spine-a cervicothoracic IP, the transition point from cervical lordosis and thoracic kyphosis (TK) and a thoracolumbar IP which transitions TK to lumbar lordosis (LL). The level of the IP along the spine governs the magnitude of a patient’s kyphosis or lordosis as it alters the length of the kyphotic and lordotic segments. 7 The IP has been established as a significant parameter to systematically describe normal sagittal shapes and variations of the spine when the Roussouly classification was presented. 8
The location of thoracolumbar IP is imperative to surgical deformity correction spanning the thoracolumbar junction in ASD. Altering a patient’s inflection point by either over or under correction may lead to complications postoperatively. Several studies have shown a correlation of negative outcome scores and positive imbalance of sagittal alignment.9-11 Pizones et al demonstrated that improper sagittal alignment after deformity correction significantly increased the risk of mechanical complications such as proximal junctional kyphosis (PJK), pseudoarthrosis, rod or screw breakage, and screw pullout. 12 Sebaaly et al showed that neglecting to restore sagittal alignment according to the Roussouly classification could increase the risk of mechanical complications by 3 times. 13 Bari et al found that successful restoration according to the Roussouly classification was correlated with a lower risk of revision surgery compared to patients who were not restored. 14 Oe et al validated this finding while also comparing outcomes based on the Hamamatsu formula and Global Alignment and Proportion (GAP) score. While there was a significant reduction in complication rate in patients who were Roussouly restored, there were no significant differences in complications among patients who were corrected according to GAP score or the Hamamatsu formula. 15 Baum et al also found no statistical significance in the rate of postoperative mechanical complications between the proportioned, moderately disproportioned (MD), or severely disproportioned (SD) groups according to GAP scores. 16 Hart and the International Spine Study Group (ISSG) proposed the PJK severity scale (PJKSS) which is calculated based on: neurological deficit, focal pain, instrumentation problem, change in kyphosis/PLC integrity, fracture location, and level of uppermost instrumented vertebrae (UIV). 17 The PJKSS was shown to be highly correlated with functional outcomes, and higher scores were strongly correlated with higher rates of revision surgeries with scores greater than 8 yielding rates of 96%-100%. 18 Despite these findings, no standard consensus exists as to the optimal way to align an instrumented spine in the sagittal plane. A multitude of suggested radiographic parameters have been established, such as pelvic incidence – lumbar lordosis (PI-LL) mismatch, T1 pelvic angle (TPA), cervical-thoracic pelvic angle (CTPA), minimizing sagittal vertical axis (SVA), and others. 19
The TK-LL IP is an important parameter to consider when planning a surgical correction for ASD. Previous literature has shown that the classically accepted IP of L1 is not constant among the population. The purpose of this study is to determine the location of from the IP from TK to LL in asymptomatic volunteers stratified by sex, ethnicity, and age.
Methods
The Multi-Ethnic Alignment Normative Study (MEANS) is a large multi-center, multi-ethnic cross-sectional study conducted across 5 countries (France, Japan, Singapore, Tunisia, and the United States). It was established with the aim to improve understanding of alignment parameters in asymptomatic adult volunteers. MEANS investigates skeletal alignment of the spine and lower extremities and is the largest adult multi-ethnic cohort of asymptomatic volunteers. This study was approved by the institutional ethics and review boards of all participating centers. The institutional review board number from Washington University in St. Louis was IRB 201812144. Healthy, asymptomatic adult volunteers between the ages of 18-80 years were enrolled prospectively across the 5 sites forming the MEANS cohort. Informed consent was obtained from all volunteers in MEANS. Volunteers included in the study reported no significant neck or back pain (Visual Analog Scale ≤ 2), nor any known spinal disorder(s), and had no history of prior surgical or non-surgical treatment for a spine related disorder. Oswestry Disability Index (ODI) scores were also obtained from volunteers. Exclusion criteria consisted of the following: volunteers with a proximal thoracic (PT), main thoracic (MT), or thoracolumbar/lumbar (TL/L) Cobb angle greater than 20°; volunteers with an abnormal vertebral count or transitional anatomy; and volunteers with an ODI score above 20. Following exclusion, a total of 468 volunteers were included in the MEANS cohort.
Basic demographic data such as age, sex, body mass index (BMI), and ethnicity were collected. Since 122 out of the 468 volunteers were Japanese, the non-Japanese Asian volunteers were characterized as a separate group. Due to the low number of Black and Indian volunteers, these cohorts were consolidated under the ethnicity group designated as “Other”.
All volunteers underwent a standing full body or full spine low dose stereoradiograph (EOS imaging, Paris, France) for enrollment in the study. All radiographic measurements were performed using a 2D/3D sterEOS® modeling software (EOS imaging, Paris, France), specifically EOS 3D Service. The EOS 3D Service software was used to measure the orientation of each vertebral segment from C2 to L5 in the sagittal, frontal, and axial planes. Additionally, intervertebral rotations were measured for each intervertebral segment from C2 to L5; these were computed as the angle between the local frame of the vertebra above projected into the local frame of the vertebra below.
Data Analysis
The population data of 468 was originally included in the MEANS study Figures 1 and 2. However, 1 additional patient was removed from the data analysis because the location of the IP was missing. The data from 467 volunteers was then evaluated. In order to find parameters that correlate with the location of the IP as well as a possible linear regression model predicting the IP, a new numbering system of the vertebrae and discs was created in the following manner: C7 was given the numerical value of 0, T1 was 1, with T1-T2 disc being 1.5, and so on. Mean and standard deviation (SD) were reported for continuous variables along with a 95% confidence interval. A correlation matrix was formed for the IP and 12 other selected parameters. Linear regression tested for linear relationships between the IP and various variables such as maximum TK and maximum LL. A multivariate linear regression was used to create an equation for the maximum LL as a function of maximum TK and the IP. Strength of correlation was classified accordingly: 0-.3 negligible, .3-.5 low, .5-.7 moderate, .7-.9 high, .9-1.0 very high. Statistical significance was set at α < .05. ANOVA was also used to compare variables for significant differences. Volunteer with the inflection point at T12-L1 disc. Volunteer with the inflection point at L3 vertebra.

Results
Of the total number of volunteers, 284 (60.8%) were female and 183 (39.2%) were male. The mean age of the volunteers was 40.4 +/− 14.8, with a range of 18 to 79 years. The stratification of the individuals on the basis of age were as follows: 127 (27.2%) aged 18-28, 100 (21.4%) aged 29-37, 126 (27.0%) aged 38-50, 76 (16.3%) aged 51-64, and 38 (8.1%) aged 65 and above.
Frequency of the Inflection Point Overall by Level.
Location of the Inflection Point Stratified By Sex, Ethnicity, and Age.
Possible Correlations
Correlation Matrix with the Inflection Point.
Correlation Matrix with Pelvic Incidence.
Regression Analysis
Regression analyses were used in order to find a possible equation linking the IP, Max LL, and the Max TK. A linear regression was performed between the IP and the Max LL yielding no correlation between the 2 variables (P = .20). A linear regression between the IP and Max TK found a weak correlation between them (P = 8.29E-08). Another linear regression was performed between the IP and the L4S1 which found a low correlation of .37 (P = 9.68E-17). A multivariate regression analysis of Max LL vs IP and Max TK was done which found a moderate correlation of r = .423 (P = 2.738E-21). The equation derived from this regression analysis is Max LL = −1.442*(IP) + .4143*(TK Max) + 57.598. To test the accuracy of the equation, the predicted Max LL was calculated using each of the 467 pairs of IP and TK Max. The average deviation from the measured Max LL was 7.67° with a range of .01° to 27.65°.
Discussion
This study reports on the average IP of the largest cross-sectional cohort of asymptomatic multiethnic volunteers to date. The average IP among all healthy volunteers was the T12-L1 disc. The average IP at the T12-L1 disc is consistent with the existing literature.4,8,20 In this study, IP did not vary significantly with sex or ethnicity. The IP did however become more cephalad with age, volunteers ages 18 to 28 had an average IP of L1, while over age 65 was on average the T12-L1 disc (P < .05) whereas Park et al found that the most common thoracolumbar IP was L2 which did not vary among the study’s age groups. 21
The correlation of age with IP is an inconsistent finding in previous studies. Pan et al found that in a cohort of 205 asymptomatic Chinese volunteers, IP was statistically correlated with age. 4 Conversely, Wang et al demonstrated no correlation between IP and age in an asymptomatic cohort of 385 Chinese volunteers. 22 Overall it seems older volunteers might have a slightly cephalad IP, the T12-L1 disc, as compared to L1 in younger volunteers; this is a helpful parameter for surgeons to keep in mind while planning surgical correction.
Multivariate regression analysis between LL, IP, and TK demonstrated a moderate positive correlation between these variables. Linearly, no correlation was found between IP and LL, and only a weak correlation was demonstrated between IP and TK. In addition, the IP was found to be moderately correlated with the apex of TK (r = .66), meaning the more superior the apex of TK, the more superior the IP point. The existing literature is inconsistent with respect to these findings. Pan et al also found in their cohort of 205 asymptomatic Chinese volunteers that IP was statistically correlated with apex of TK, and apex of LL. However, similarly, no correlation was found between IP and magnitude of the LL. 4 On the other hand, Wang et al demonstrated that in a cohort of 385 asymptomatic Chinese volunteers with an average age of 38, IP had a weak negative correlation to LL (r = −.28, P < .01). 22 Roussouly et al found that the apex of lumbar lordosis was statistically significantly correlated with IP (r = .52, P < .01 in 160 asymptomatic Caucasian volunteers. 8 The correlation between magnitude of TK and LL with the IP seems to be an unreliable measure. The TK apex appears to be a slightly more reliable predictor of IP; that if a patient has a more proximal TK apex, their IP will be more proximal.
There are some limitations to our study. This study was a cross sectional study, involving a small total sample size of asymptomatic volunteers; thus, the study design may allow for the inadvertent introduction of selection bias. However, all volunteers underwent standing full body or full spine low dose stereoradiographs, and all radiographic measurements were performed using a 2D/3D sterEOS® modeling software (EOS imaging, Paris, France), specifically EOS 3D Service. Though this may limit the generalizability of our findings to all other imaging systems, this also could be considered a study strength. By limiting all asymptomatic volunteers to a single consistent imaging format, we were able to limit any confounding variables that would have been introduced if multiple systems were assessed. Further, the number of volunteers in the older age groups, no volunteers above the age of 79, and a limited number of ethnicities represented are also limitations of the MEANS cohort.
Conclusion
The inflection point between thoracic kyphosis and lumbar lordosis is a useful sagittal parameter for spine surgeons planning surgical deformity correction and fusion. In this study, the average IP was the T12-L1 disc, with younger subjects tending to be closer to L1 and older subjects closer to T12. The magnitude of TK, LL, and PI were not significantly correlated with IP. The only sagittal parameter with a fairly significant correlation was the TK apex, a proximal apex was correlated with a proximal IP. Asymptomatic patient’s sagittal parameters can be useful to deformity surgeons restoring a patient’s native anatomy to mitigate postoperative clinical and mechanical complications.
Footnotes
Acknowledgments
Though EOS imaging software was used to analyze radiographs, EOS company did not fund this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The research conducted in this study received institutional review/ethics board approval at all sites.
Device Status/Drug Statement
The manuscript submitted does not contain information about medical device(s)/drug(s).