
Abstract
Study Design
A prospective case-control study.
Objective
To analyze global coronal malalignment (GCM) in degenerative lumbar scoliosis (DLS) and to prospectively investigate the performance of priority-matching correction technique on preventing postoperative coronal imbalance.
Methods
A total of 444 DLS inpatients and outpatients were recruited. GCMs were classified into 2 types: Type 1, GCM with thoracolumbar (TL/L) curve as the main contribution on coronal imbalance; Type 2, GCM with lumbosacral (LS) curve as the main contribution on coronal imbalance. Patients receiving priority-matching correction were assigned to Group P-M and receiving traditional correction were assigned to Group T form August 2020. The fundamental principle of priority-matching technique was to first correct the key curve contributing to coronal imbalance rather than the curve with greater magnitude.
Results
Type 1 GCM accounted for 45% and Type 2 GCM accounted for 55% of patients. Type 2 GCM was detected to have greater LS Cobb angle and L4 tilt. At 1-year follow-up, 29.8% of patients with Type 2 GCM, whereas 11.7% of patients with Type 1 GCM were observed to have postoperative coronal decompensation. Patients with postoperative imbalance were revealed to have greater preoperative LS Cobb angle and L4 tilt and smaller correction extent of LS curve and L4 tilt. 6.25% of patients developed postoperative coronal imbalance in Group P-M, whereas 40.5% developed in Group T.
Conclusion
Highlighting priority and aggressive correction of the key curve to coronal imbalance, priority-matching technique was proved to be able to limit the development of postoperative coronal decompensation.
Keywords
Introduction
Degenerative lumbar scoliosis (DLS) is a de novo spinal deformity due to lumbar degeneration after bone mature, which involves not only the spinal curvature on the coronal plane, but also the global coronal imbalance that is defined as lateral deviation of C7 plumbline (C7PL) with substantial displacement from the midline of the sacrum for more than 20 mm.1-3 Coronal imbalance is often related to cosmetic concerns and back pain because of the limited compensatory mechanisms and increases the difficulty of surgical decision-making for DLS.4,5 Correction surgery is more likely to be appropriate for DLS with severe living disability or nervous lesion when compared with conservative treatment. 6 Nevertheless, outcomes might not always be satisfactory for each patient because of the high prevalence of postoperative coronal imbalance ranging from 20.7 to 35.6%.7-13
In order to address this problem, there is a growing body of studies focusing on identifying the risk factors for failed restoration of coronal balance in DLS. In a retrospective study, Bao et al 7 analyzed the radiographic characteristics of global coronal malalignment (GCM) in 284 DLS patients and classified this deformity into 3 types (A, B, C) based on coronal balance distance (CBD) and the direction of C7PL shifted. They found patients with preoperative C7PL shifted to the convex side of lumbar curve (Type C) were more likely to develop postoperative coronal imbalance. Similarly, Zhang et al10-12 classified GCMs into consistency and opposition patterns based on the orientation of L4 coronal tilt relative to C7PL in their DLS series and revealed the similar results that L4 coronally tilting toward C7PL (consistency patterns) was an independent risk factor for postoperative coronal decompensation. Regardless of classifications, significant preoperative coronal imbalance and great tilt of lumbar foundation were reported to be prone to postoperative coronal imbalance.8,9 With respect to surgical procedure, hypercorrection of the main thoracolumbar/lumbar (TL/L) curve and undercorrection of lumbosacral (LS) curve were believed to be related with new onset and deterioration of postoperative coronal imbalance.7,11,13 Accordingly, achieving coronal balance in long scoliosis correction for DLS presented a real challenge to spinal surgeons.
TL/L curve in DLS is usually considered as the major curve, whereas LS curve is the fractional curve. The majority of attention is often directed towards the main TL/L curve during the operation, which is gradually reported to be the critical factor of postoperative coronal decompensation.7,11,13 For DLS patients, in our opinions, restoring global coronal balance is more important than complete correction of the curvatures. However, there is a need for understanding that the main curvature may not always be the primary driver of coronal imbalance. Hence, it is necessary to figure out the key curve that contribute to the development of coronal imbalance. In the present study, we analyzed the characteristics of GCMs in DLS and designed a priority-matching correction technique that first and aggressively correct the curve with major contribution on coronal imbalance. We conducted this study to prospectively investigate the performance of this technique on preventing postoperative coronal decompensation.
Methods
Subjects
This radiographic study was approved by the Institutional Review Board of Capital Medical University Xuanwu Hospital. We were exempt from the requirement of patients’ informed consent. The consecutive DLS inpatients and outpatients at our single institution from January 2018 to August 2022 were retrospectively reviewed. Inclusion criteria were as follows: (1) age >50 years, (2) a diagnosis of DLS based on radiography and previous medical record. Subjects with leg length discrepancy and a history of spinal or pelvic surgery were excluded. DLS was defined as a TL/L or LS fractional curve with the Cobb angle >10° measured on long-cassette standing radiographs.
3
In August 2020, we designed the priority-matching correction technique. From then on, inpatients meeting surgical indications (lumbar spinal stenosis, neurological impairment and pre-operative Cobb angle >20°) were randomly performed the priority-matching correction technique that first correct the major curve contributing on coronal imbalance and the traditional correction technique that first correct the curve with major magnitude. Patients receiving priority-matching correction were assigned to Group P-M and those receiving traditional correction were assigned to Group T (Figure 1). Basic demographic and surgical information were recorded. Oswestry Disability Index (ODI) where 0% indicated no disability and 100% indicated extremely debilitating disability and Visual Analogue Score (VAS) where 0 score indicated no pain and 10 score indicated extremely pain were used to assess patients’ health-related quality of life (HRQOL). Flow chart of patients recruiting and evaluating.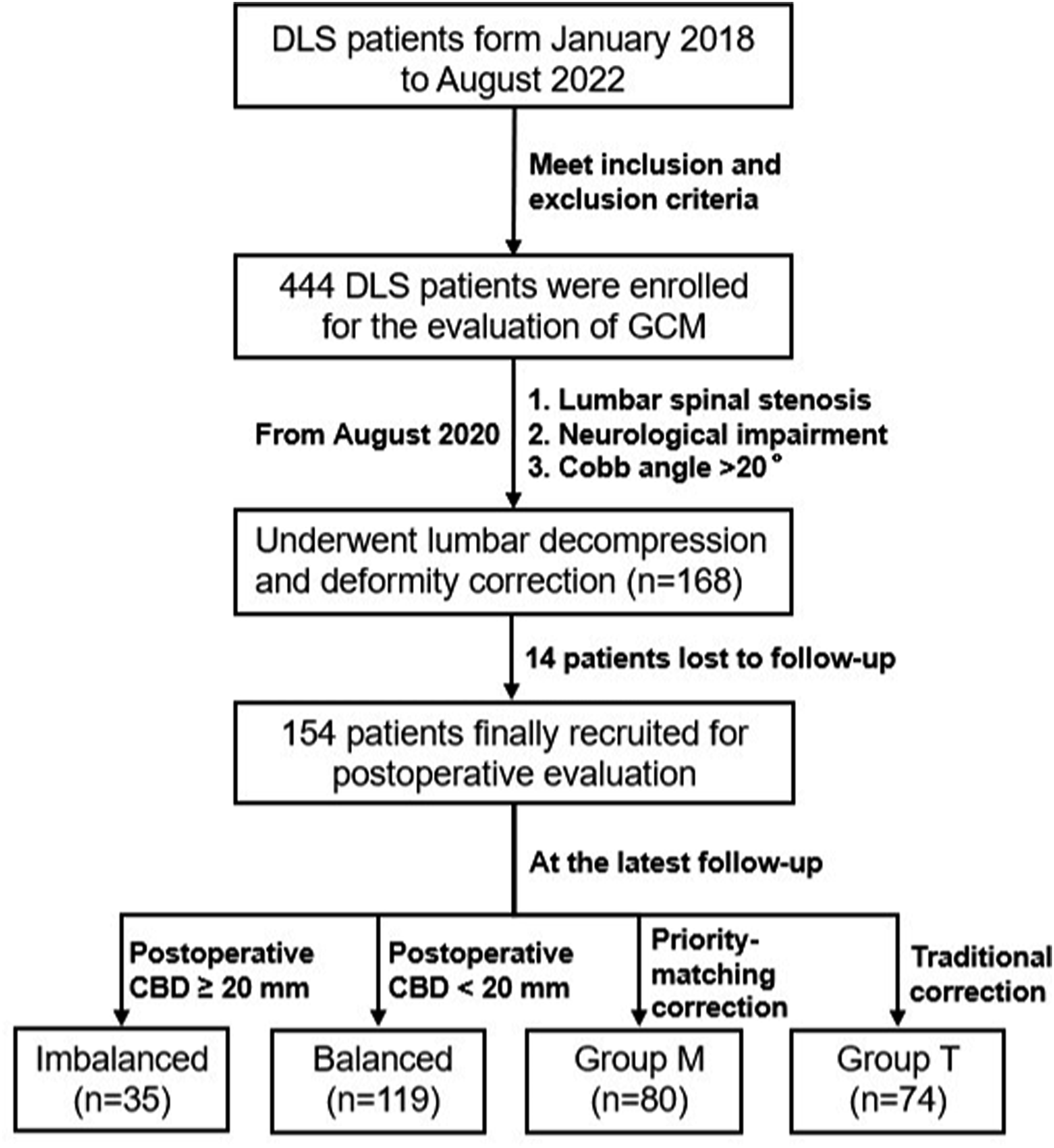
Radiographic Analysis
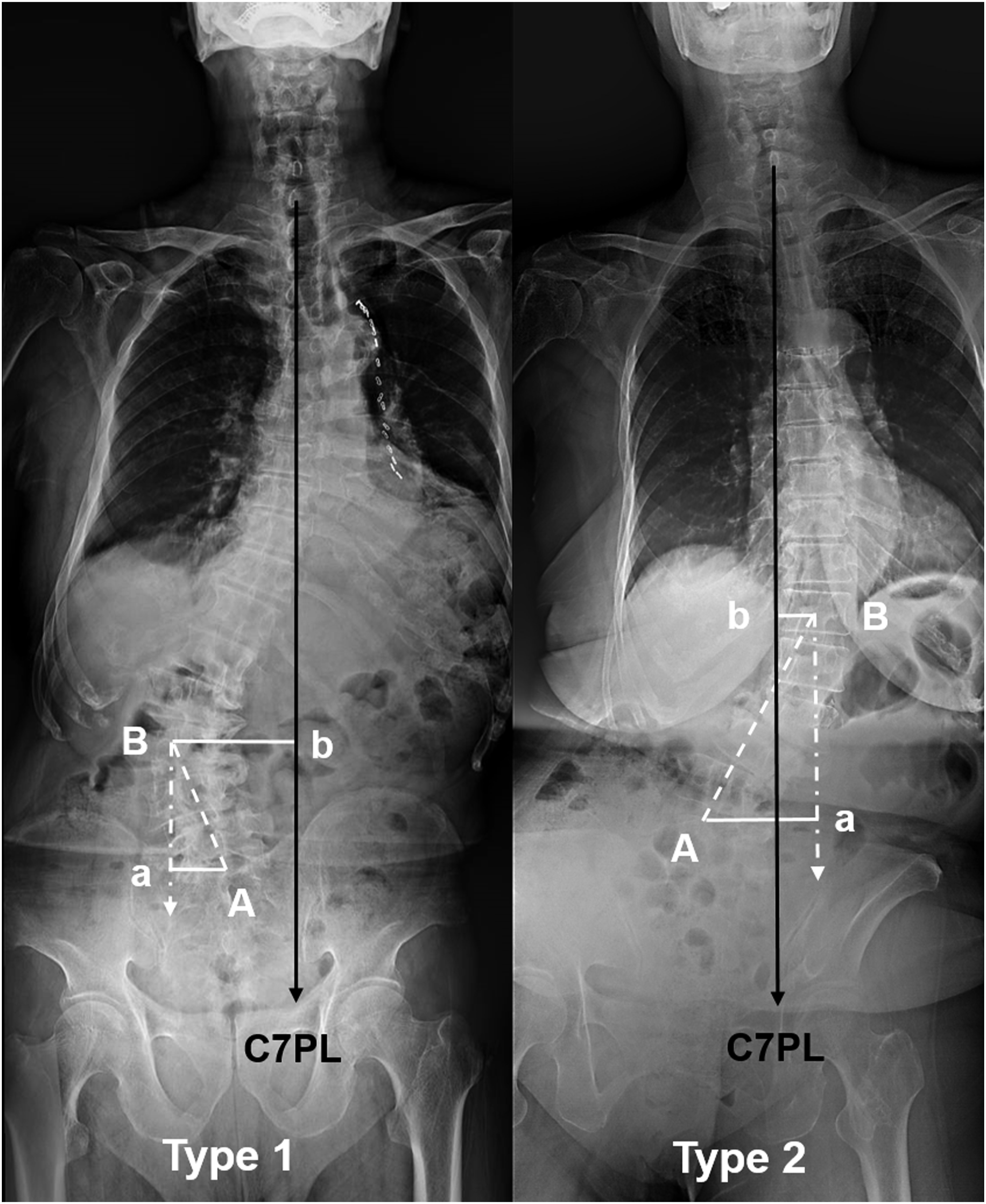
Long-cassette standing anteroposterior and lateral radiographs of the whole spine were obtained pre-operatively for all the DLS patients and at 1-year follow-up for those who underwent PSF including lumbar decompression and deformity correction. As shown in Figure 2, point A was the midpoint of the superior endplate of S1. Point B was the center of the apex vertebra or intervertebral space of lumbar curve. Point a was the vertical intersection of the line connecting point A and the plumb line connecting point B. Point b was the vertical intersection of the line connecting point B and C7PL. Biomechanically, the distance between points A and a (Aa) could represent the contribution of LS curve on moving C7PL to a direction, while the distance between points B and b (Bb) could represent the contribution of TL/L curve on moving C7PL to the opposite direction. In this classification, curve with the greater contribution on C7PL shifting was determined as key curve, whereas that with smaller contribution was determined as minor curve. Two main GCM patterns were identified. • Type 1 GCM is defined as GCM with TL/L curve as the key curve contributing to coronal imbalance (Aa < Bb, Figure 2 right). • Type 2 GCM is defined as GCM with LS curve as the key curve contributing to coronal imbalance (Aa ≥ Bb, Figure 2 left). Two types of GCMs in patients with degenerative lumber scoliosis. (A): the midpoint of the superior endplate of S1; (B): the center of the apex vertebra or intervertebral space of TL/L curve; a: the vertical intersection of the line connecting (A) and the plumb line connecting B; b: the vertical intersection of the line connecting (B) and C7PL. Aa represents the distance between points A and a. Bb represents the distance between points B and b. GCM with Aa < Bb was classified as Type 1 (left). GCM with Aa ≥ Bb is classified as Type 2 (right).
The following coronal and sagittal parameters were measure using Surgimap software (Nemaris, Inc, New York, NY, USA). Coronal parameters: (1) coronal balance distance (CBD), the horizontal distance between C7PL and central sacral vertical line; (2) Aa distance (Aa), the distance between point A and point a (Figure 2); (3) Bb distance (Bb), the distance between point B and point b (Figure 2); (4) TL/L curve Cobb angle, the angle between the superior endplate of the most tilted vertebra cranially and the inferior endplate of the most tilted vertebra caudally; (5) LS curve Cobb angle, the angle between the superior endplate of L4 and the superior endplate of S1; (6) L4 coronal tilt (L4 tilt), the angle between the superior endplate of L4 and the horizontal line. When measuring Aa and Bb, C7PL falling at the concavity was assigned a positive value, and C7PL falling at the convexity was assigned a negative value. The difference between Aa and Bb (Aa-Bb) was geometrically equal to CBD (a positive value represented C7PL fallen at the concavity of LS curve and a negative value represented C7PL fallen at the convexity). In this study, coronal imbalance was defined as GCM with CBD ≥20 mm. The directions of pre- and postoperative coronal imbalance were recorded. Specifically, the correction rate of coronal Cobb angle was calculated using the following formula: (preoperative angle – postoperative angle)/preoperative angle × 100%. Sagittal parameters: (1) thoracic kyphosis (TK), measured from the superior endplate of T5 to the inferior endplate of T12; (2) thoracolumbar kyphosis (TLK), measured from the superior endplate of T10 to the inferior endplate of L2; (3) lumbar lordosis (LL), measured from the upper endplate of L1 to the superior endplate of S1; (4) pelvic incidence (PI), measured from the perpendicular to the superior endplate of S1 at its midpoint to the line connecting the point to the middle axis of the femoral heads; (5) sacral slope (SS), measure from the sacral plate to the horizontal plane; (6) pelvic tilt (PT), measured from the line connecting the midpoint of the superior endplate of S1 to the axis of the femoral heads to the gravity line; (7) PI-LL mismatch (PI-LL), equaled to PI minus LL; (8) sagittal vertical axis (SVA), the horizontal distance between the C7 plumbline and the posterior-superior corner of the sacrum. At 1-year follow-up, patients with postoperative CBD ≥20 mm were assigned to Group imbalanced, while those with postoperative CBD <20 mm were assigned to Group balanced. Radiographic measurements were performed by 2 independent researchers (D. W. and P. C.) and the mean values were collected for statistical analysis.
Priority-Matching Correction Technique
The fundamental principle of priority-matching correction technique is to give priority to aggressively correct the key curve to coronal imbalance instead of the curve with greater magnitude, followed by matching correction of the minor curve to adjust global balance (Fig, 3). The correction extent of a curve is mainly up to its contribution on coronal imbalance. 14
For Type 1 GCM, TL/L curve makes the primary contribution on C7PL shifting. First, inserting pedicle screws bilaterally (Figure 3(a)). Second, aggressively decreasing the magnitude of TL/L curve (Figure 3(b)). Third, moderately leveling L4 endplate to pull the fusion segments to the middle line with hand pressure on the convexity of TL/L curve (Figure 3(c)). If the correctability of the key curve was limited, the correction of the minor curve would be convergent. For Type 2 GCM, LS curve makes the primary contribution on C7PL shifting. First, releasing LS curve from the concave side using facetectomy after screws inserted (Figure 3(d)). Second, performing L4-5 or L5-S1 transforaminal lumbar interbody fusion (TLIF) from the convexity of the fractional curve, with cages inserted at the concave side to assist deformity correction (Figure 3(e)). Third, compressing the convexity of LS to horizontalize L4 endplate, followed by moderate manipulative reduction of TL/L curve to adjust intraoperative coronal balance (Figure 3(f)). With respect to the sagittal plane, correcting the local thoracolumbar kyphosis or restoring the local lumbar/lumbosacral profile with PI-LL within 10° and PT within 20°.
15
Schematic diagram of priority-matching correction steps for GCM in degenerative lumbar scoliosis. (A) A Type 1 GCM with C7PL shifting to the concavity of key curve TL/L; First, inserting pedicle screws bilaterally. (B) Then, aggressively correcting TL/L curve with standard maneuver. (C) Finally, moderately leveling L4 endplate (triangle arrow) to pull the fusion segments to the middle line. (D) A Type 2 GCM with C7PL shifting to the concavity of key curve LS; First, releasing LS curve from the concavity using facetectomy after screws inserted (triangle arrow). (E) Second, performing L4-5 or L5-S1 TLIFs from the convexity (hollow arrow) with cages inserted at the concave side (triangle arrow) to assist L4 horizontalization. (F) Third, moderately decreasing the magnitude of TL/L curve to adjust intraoperative coronal balance.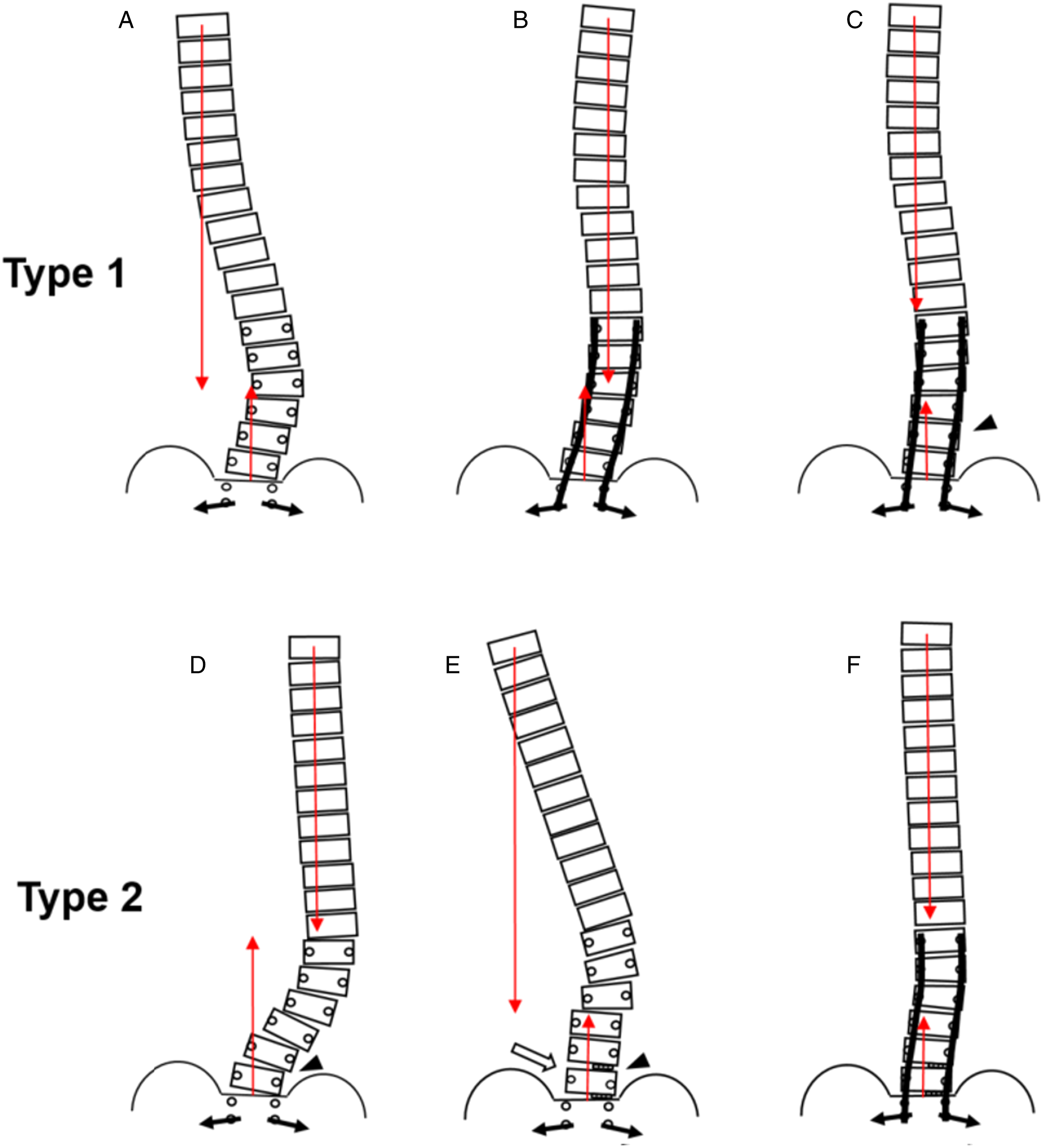
For traditional correction technique, the standard correction maneuver was first utilized in the main curve with a greater curvature. Priority-matching technique and traditional technique were randomly performed. All lumbar decompressions were completed with TLIF procedure. No high-grade osteotomy was applied. The proximal end vertebra in the measured scoliosis was selected as upper instrumented vertebra (UIV). Lower instrumented vertebra (LIV) was determined depended on the TLIF level. S2 iliac screws would be used if lumbosacral fixation and fusion was performed.
Statistical Analysis
All data were presented as the mean ± standard deviation with absolute value and were analyzed using SPSS version 26.0 statistical software (SPSS Inc). The correlations between coronal parameters and CBD were analyzed with the Pearson correlation coefficient. Comparisons of continuous variables between pre-operation and post-operation and between different groups were performed using the Mann–Whitney U test. Chi-square analysis was applied to assess the categorical variables. A P value <.05 was considered statistically significant.
Results
General Information
The Correlation Analysis Between Coronal Parameters and CBD.

CBD Coronal balance distance, TL/L Thoracolumbar/Lumbar Cobb angle, LS Lumbosacral Cobb angle, TL/L-LS the absolute value of the difference between TL/L and LS, L4 tilt L4 coronal tilt angle, L5 tilt L5 coronal tilt angle, Aa the distance between point A and point a, Bb the distance between point B and point b, Aa-Bb the absolute value of the difference between Ab and Bb.
Comparisons between Type 1 and Type 2
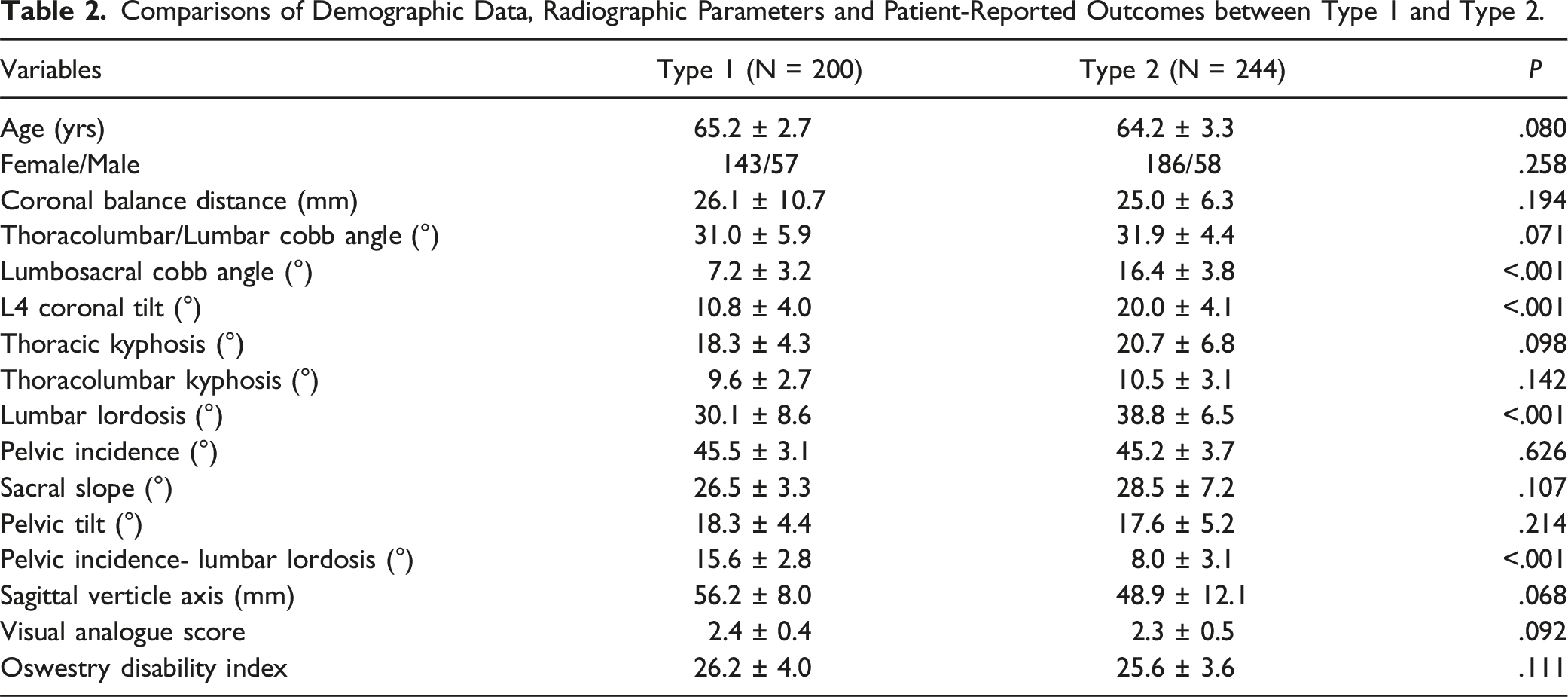
Comparisons of Demographic Data, Radiographic Parameters and Patient-Reported Outcomes between Type 1 and Type 2.
Distribution of Postoperative Coronal Imbalance
At 1-year follow-up, 35 patients (22.7%) were revealed to have postoperative coronal decompensation. The specific incidences were 29.8% in Type 2 GCM and 11.7% in Type 1 GCM based on our classification method. Regardless of the correction techniques, higher incidence of postoperative decompensation was discovered in Type 2 GCM. Thirty-four subjects had the same directions of postoperative imbalance with preoperative imbalance (including 28 in Type 2 GCMs and 6 in Type 1 GCMs), while 1 subject with Type 1 GCM had the opposite direction.
Comparisons between Patients with and without Postoperative Coronal Imbalance
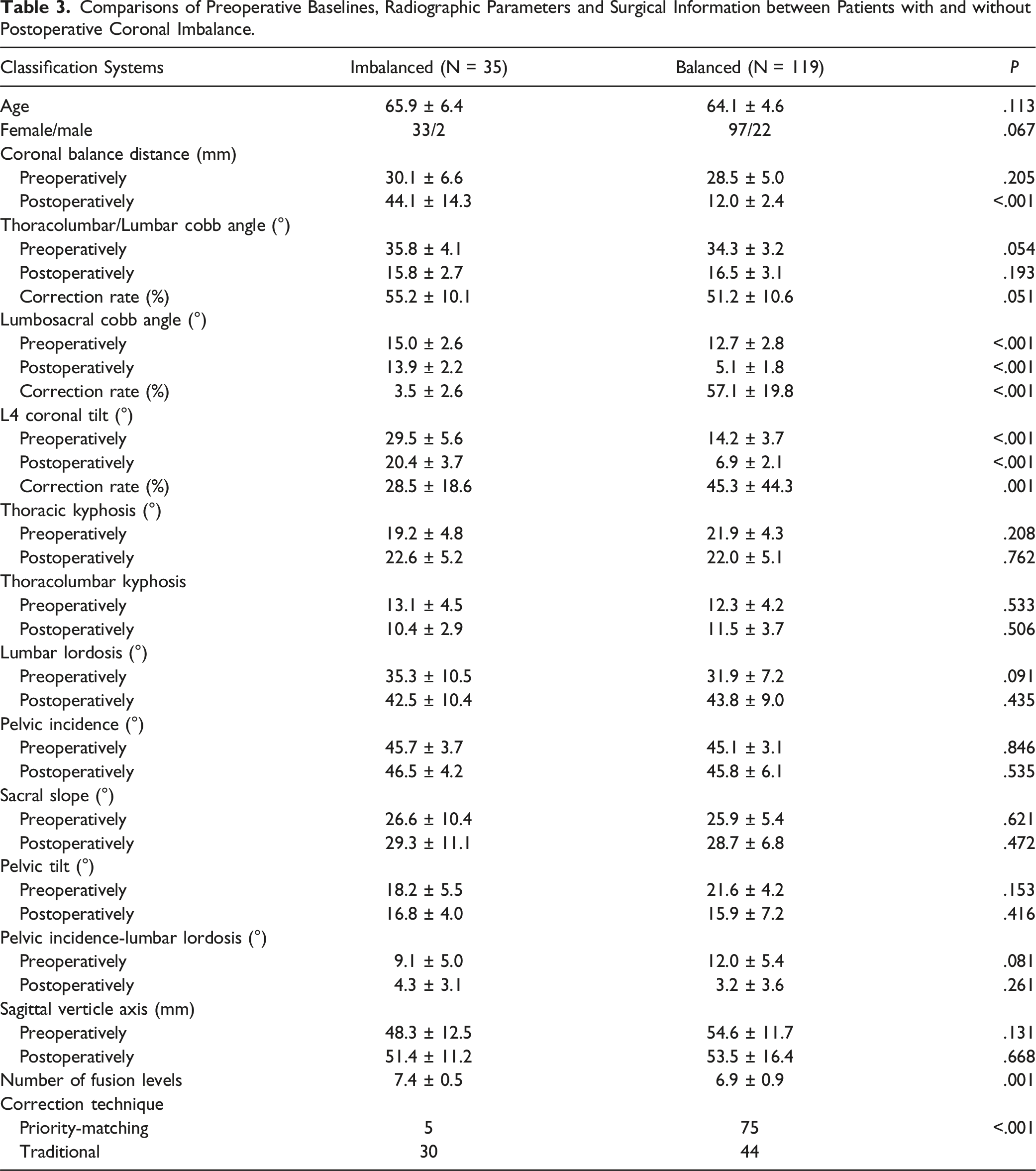
Comparisons of Preoperative Baselines, Radiographic Parameters and Surgical Information between Patients with and without Postoperative Coronal Imbalance.
Comparisons between Group P-M and Group T
Comparisons of Demographic Data, Surgical Information and Radiographic Parameters between Group P-M and Group T
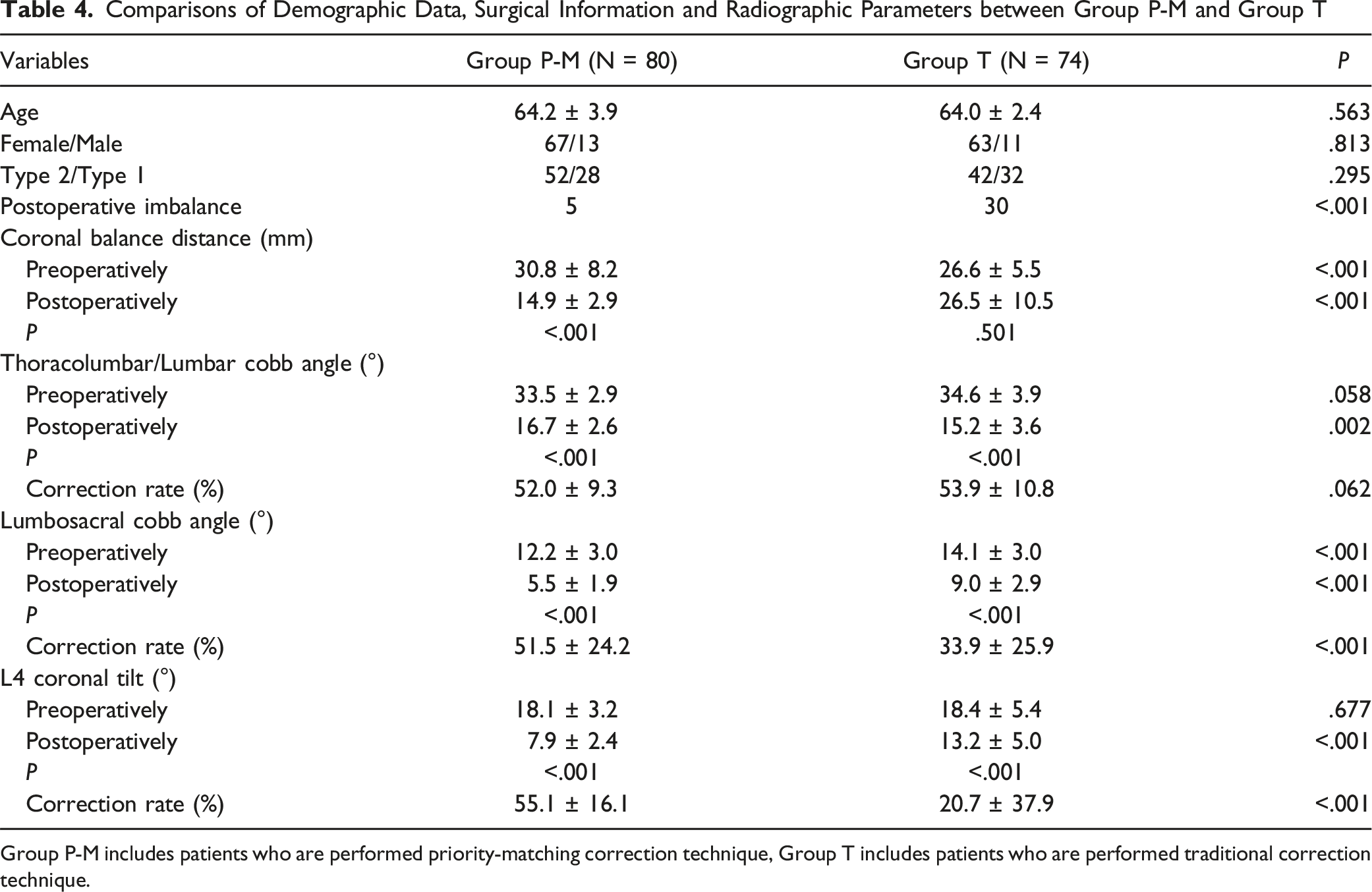
Group P-M includes patients who are performed priority-matching correction technique, Group T includes patients who are performed traditional correction technique.
Discussion
To date, the specific mechanism of coronal imbalance in DLS has not been clearly defined. Biomechanically, TL/L and LS curves in DLS move the gravity of trunk (represented by C7PL) to the opposite directions in coronal plane (Figure 2). Different shifted distances of C7PL to opposite directions will generate coronal imbalance. If LS curve contributes more on C7PL shifting, this gravity line will stand at its concavity. Otherwise, C7PL will stand at the concavity of TL/L curve. According to the directions of gravity line shifted relative to main curve or L4 orientation, previous authors have designed 3 classification systems for GCMs and identified certain patterns prone to coronal imbalance after correction surgery.7,10-12,14 Unfortunately, their classifications could not well govern how to correct and how much to correct to prevent postoperative decompensation.
There is a need for understanding that a curve with a greater Cobb angle may not make a greater contribution on C7PL displacement. Our results revealed a weak correlation between the magnitude of coronal curve and CBD (Table 1). Contrastively, CBD was strongly correlated with the distance parameters Aa-Bb (r = .980) and Aa (r = .636) that could be regarded as the contribution of coronal curve on trunk shift. Based on this finding, we classified GCMs according to the contributions of coronal curves on C7PL shifting. In this classification, the primary driver of C7PL shifting is determined as the key curve. GCM with LS as the key curve was classified as Type 2 and that with TL/L as the key curve was classified as Type 1 (Fig. 2). 55.0% of subjects in our whole cohort were identified with Type 2 GCM and 45.0% were identified with Type 1 GCM. Measurements showed Type 2 GCMs had a greater LS angle and a greater L4 coronal tilt angle than Type 1 GCMs (Table 2). LS curve in Type 2 GCM was the primary driver of coronal imbalance, thus it was easy to comprehend that it had a more tilted foundation. In addition, LL was smaller and PI-LL was greater in Type 1 GCM, which was speculated to be related with the significant lumbar degeneration in Type 1 GCM.
Previous studies have reported Type C GCMs and GCMs with consistency pattern were more likely to develop postoperative coronal imbalance.7,10-12 Their efforts were the first step to avoid this complication and could serve as a warning for surgical decision-making. Upon most occasions in correction operation for DLS, more attentions were paid to the correction of TL/L curve that usually had greater curve magnitude and more vertebrae participated. If C7PL stands at the convexity of TL/L (Type 2, Type C or consistency pattern) preoperatively, more correction of TL/L will further move C7PL to the same direction, which deteriorates the postoperative coronal imbalance (Fig. 4). Obeid et al
14
held the same view that correction of the TL/L curve in the convex GCM (T1 plumbline falling at the convexity of lumbar curve) would result in coronal imbalance. Hence, decreasing the correction of TL/L curve or increasing the correction of LS curve might be effective for decreasing postoperative imbalance. A 70 year-old female patient suffering from low back pain and major disability, presented with a Type 2 GCM (A). Despite with a greater magnitude, TL/L curve made the minor contribution on C7PL shifting. Traditional correction procedure with a long fusion from T10 to S2 and L4-S1 TLIFs was performed. Focusing on decreasing the magnitude of TL/L curve, 50.3% of TL/L Cobb angle was corrected, whereas 15.8% of LS Cobb angle was corrected. CBD was increased from 15.6 mm preoperatively to 50.2 mm at 1-year follow-up (B).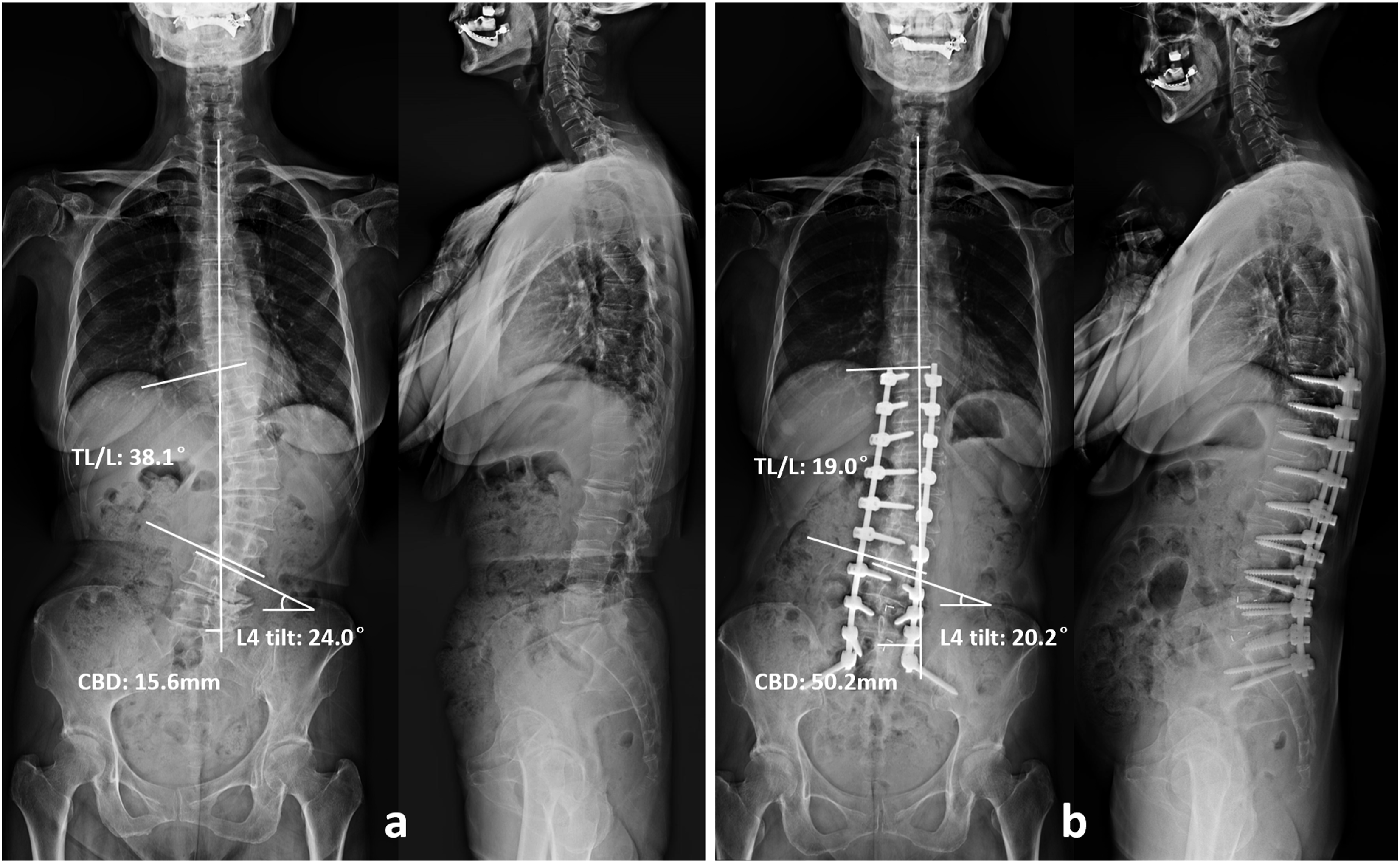
Previous authors have realized the importance of leveling the foundation curve (LS) on achieving postoperative coronal balance. Lewis et al 8 retrospectively reviewed the demographic, surgical and radiographic characteristics of 46 adult spinal deformity patients who underwent correction surgery with long fusions to the pelvis. Thirty-two patients were balanced after surgery and 14 were imbalanced. Comparisons revealed greater L4 and L5 coronal tilt angle in imbalanced group than balanced group at discharge and follow-up (Table 3). They concluded leveling L4 and L5 coronally had the greatest impact on the ability to achieve coronal balance. Zhang et al10-12 reported the similar findings in their researches that unsatisfactory horizontalization of L4 in patients with consistency pattern would induce postoperative coronal decompensation. Bao et al 7 and Shi et al 16 introduced the sequential correction technique to reduce postoperative coronal decompensation for Type C GCMs, in which leveling the foundation of whole spine was also emphasized.
Coronal horizontalization of L4 could be a critical factor for achieving coronal balance only when LS fractional curve is the primary driver of the coronal imbalance, while does not seem to be reasonable in those with TL/L as the major contributor of coronal imbalance. Nevertheless, considerable postoperative coronal decompensations were also revealed in GCM with preoperative C7PL shifted to the concavity of TL/L curve. Bao et al 7 reported 29.4% of patients with Type B GCM developed postoperative coronal imbalance at 2 weeks postoperatively. In Zhang et al’s 10 study, 27.5% of patients with opposition pattern were detected to have postoperative coronal decompensation at 2 weeks postoperatively or discharge. Our results also discovered an unacceptable incidence of postoperative coronal imbalance in Type 1 GCM at 1-year follow-up. Therefore, how to prevent the development of postoperative decompensation in these GCMs was also an important issue.
Obeid et al
14
suggested to perform corrections at the apex of lumbar curve in concave GCM and at the lumbosacral junction in convex GCM in adult spinal scoliosis to reduce postoperative imbalance. Nevertheless, they did not specifically describe how to correct and how much to correct. Our results revealed that all the postoperative coronal imbalance in Type 2 GCMs and 85.7% of postoperative coronal imbalance in Type 1 GCMs had the same direction with preoperative imbalance, indicating the overcorrection of TL/L curve or undercorrection of LS curve in Type 2 GCMs and undercorrection of TL/L curve or overcorrection of LS curve in Type 1 GCMs. Based on our new classification, we introduced the priority-matching correction technique, the fundamental principle of which was to first and aggressively correct the key curve to coronal imbalance rather than the curve with greater magnitude (Fig, 3). As for Type 2 GCM, coronal horizontalization of L4 by unilateral facetectomy and unilateral cage could provide a leveled foundation to facilitate the correction of the lumbar curve above L4. Moderate correction of TL/L curve was then performed with the goal of achieving the intraoperative coronal balance (Fig. 5). This correction order could avoid the situation that there was not enough potential to pull the whole spine back to the middle by LS curve, in case TL/L curve was overcorrected. As for Type 1 GCM, aggressive correction of TL/L curve was performed to decrease the curvature magnitude and push gravity line to the middle or to the opposite direction. L4 leveling was then conducted to keep the fusion segments centered over the pelvis (Fig. 6). Besides, ideal sagittal profile with PI-LL <10° and PT <20° was also strived.
15
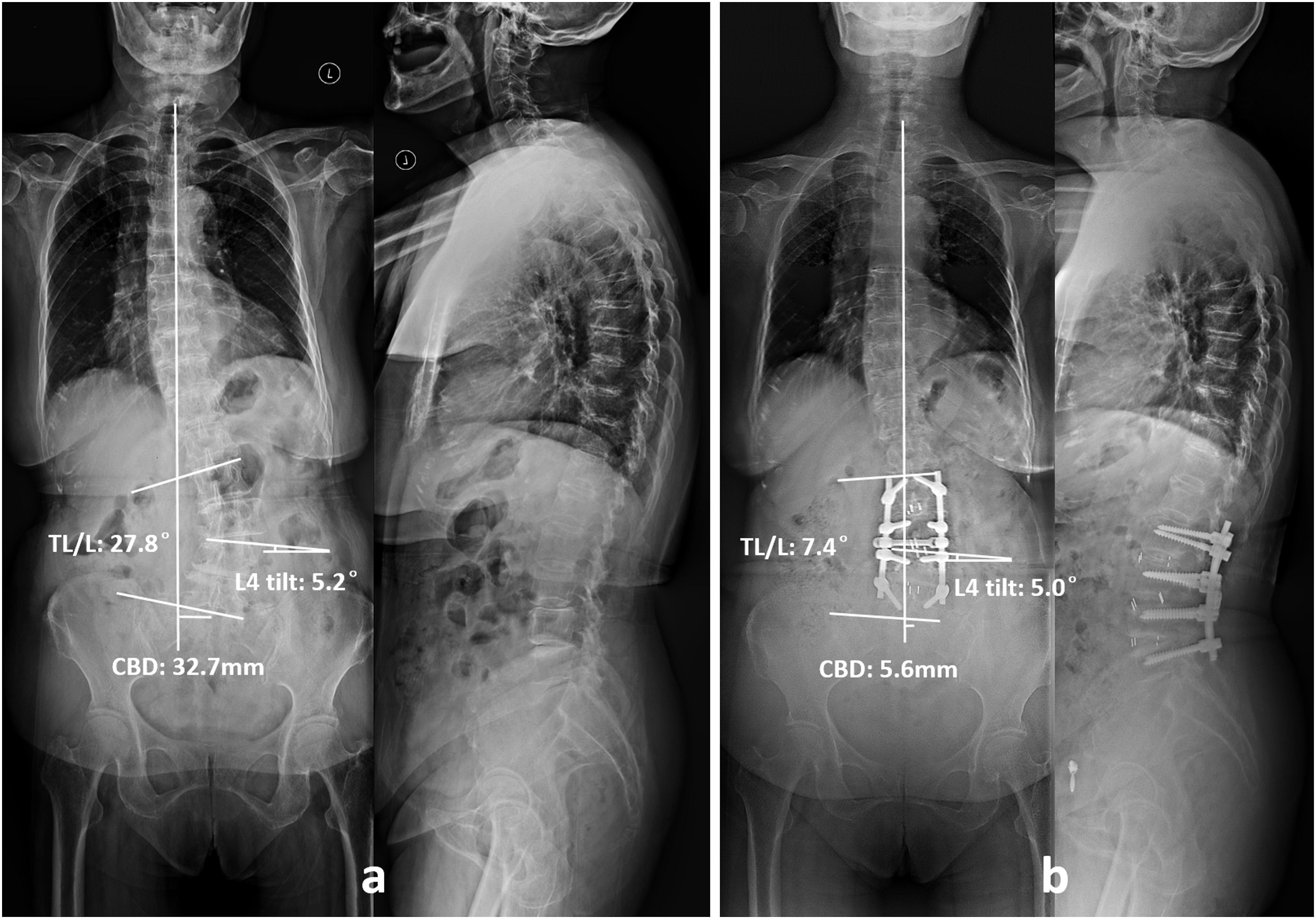
At 1-year follow-up, CBD was 14.9 ± 2.9 mm in Group P-M, whereas 26.5 ± 10.5 mm in Group T (P < .001). No matter which type of GCM, this technique was proved to be more effective on preventing the development of postoperative coronal decompensation than traditional procedure (6.3% vs 40.5%, Table 4). Complete correction of coronal curves was not pursued in priority-matching procedure, thus high-grade osteotomy was absolved, reflecting it friendly property for the elderly population. A 64 year-old female patient suffering from low back pain and major disability, presented with a Type 2 GCM (A). Priority-matching correction procedure with a long fusion from T11 to S2 and L3-S1 TLIFs was performed. As for Type 1 GCM, LS was the major curve contributing to trunk shifting. Adequate horizontalization of L4 cranial endplate was first obtained, followed by matching correction of TL/L curve to adjust the coronal balance. At 1-year follow-up, the correction rate of L4 tilt was 84.4%, whereas the correction rate of TL/L was 76.6%. CBD was decreased from 31.0 mm preoperatively to 7.5 mm at 1-year follow-up (B). A 63 year-old male patient suffering from low back pain and reduced walking distance, presented with a Type 1 GCM (A). Priority-matching correction procedure with a long fusion from L2 to L5 and L2-5 TLIFs was performed. As for Type 2 GCM, TL/L was the major curve contributing to coronal imbalance. More efforts were first put into decreasing the magnitude of TL/L curvature, followed by matching correction of L4 tilt to pull the fusion segments to the middle line. At 1 year follow-up, the correction rate of TL/L was 73.4%, while the correction rate of L4 tilt was 3.8%. CBD was decreased from 32.7 mm preoperatively to 5.6 mm at 1-year follow-up (B).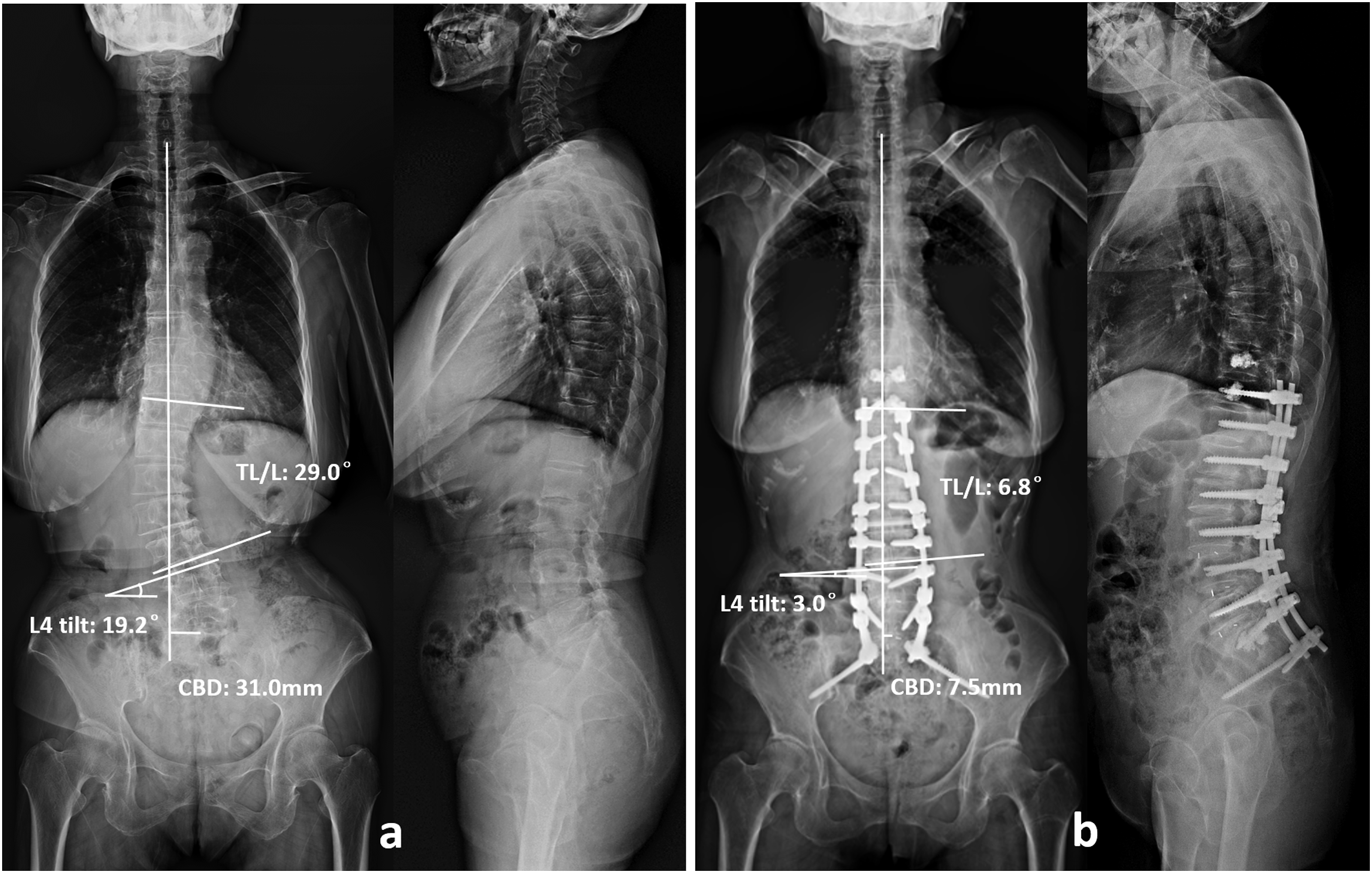
Our study figuring out the primary driver of coronal imbalance instead of the larger curvature, which is helpful for governing the correction order of curves. The priority-matching correction technique could serve as a reference for clinical practice when dealing with coronal imbalance in the surgical management of DLS. Despite, this study still has some limitations. First, this is a single-center and single-surgeon study, limiting the generalize ability of our findings. Second, the follow up period was relatively short with only 1 year. Third, this study did not involve sagittal profile evaluation, which might have influence on the postoperative outcome in terms of coronal alignment. Forth, the quantitative extent for correction of the minor curve was not defined. Further work with multi-center data and long-term follow-up is needed in the future.
Conclusion
GCMs with LS curve as the primary driver of C7PL shifting (Type 2) are demonstrated to be at greater risk for postoperative coronal decompensation after traditional correction surgery. Priority-matching correction technique, which highlight the importance of priority and aggressive correction of the key curve and second matching correction of the minor curve to adjust to intraoperative coronal balance, is proved to be able to limit the development of postoperative coronal imbalance in DLS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Key Research and Development Program of China (Grant No. 2020YFC2004900).
Disclosure
The authors have no personal, financial, or institutional interest in any of the drugs, materials, or devices described in this article. This study was performed under the approval from the Ethics Committee of Capital Medical University Xuanwu Hospital. We were exempt from the requirement of patients’ informed consent.
This study was performed under the approval from the Institutional Review Board of Capital Medical University Xuanwu Hospital (IRB approval number: 086[2018]).