
Abstract
Study design
Systematic review and meta-analysis
Objectives
Postoperative ileus (POI) can negatively impact patient recovery and surgical outcomes after spine surgery. Emerging studies have focused on the risk factors for POI after spine surgery. This study aimed to review the available literature on risk factors associated with POI following elective spine surgery.
Methods
Electronic databases were searched to identify relevant studies. Meta-analysis was performed using random-effect model. Risk factors for POI were summarized using pooled odds ratio (OR) with 95% confidence intervals (CI).
Results
Twelve studies were included in the present review. Meta-analysis demonstrated males exhibited a higher risk of POI than females odds ratio (OR, 1.76; 95% CI, 1.54-2.01). Patients with anemia had a higher risk of POI than those without anemia (OR, 1.48; 95% CI, 1.04-2.11). Patients with liver disease (OR, 3.3; 95% CI, 1.2-9.08) had a higher risk of POI. The presence of perioperative fluid and electrolyte imbalances was a predictor of POI (OR, 3.24; 95% CI, 2.62-4.02). Spine surgery involving more than 3 levels had a higher risk of POI compared to that with 1-2 levels (OR, 1.82; 95% CI, 1.03-3.23).
Conclusions
Male sex and the presence of anemia and liver disease were significant patient factors associated with POI. Perioperative fluid and electrolyte imbalance and multilevel spine surgery significantly increased the risk of POI. In addition, through this comprehensive review, we identified several perioperative risk factors associated with the development of POI after spine surgery.
Introduction
Postoperative ileus (POI) is characterized by the impairment of gastrointestinal (GI) motility after surgery under anesthesia.1-3 The common symptoms of POI are postoperative nausea and vomiting, inability to tolerate diet, failure to pass gas or stool, and abdominal distension for more than 3 days. 2 Although abdominal surgery is known to be the most common cause of POI, POI is also observed as an adverse event after other types of surgery, including cardiovascular, 4 urological, 5 gynecology, 6 and orthopedic surgeries. 7 In addition, perioperative anesthetics and postoperative analgesics can compound the development of POI.8,9 Development of POI causes discomfort to the patient and increases patient recovery time, length of hospital stay, and financial burden.1,3 Patients with POI are at an increased risk of developing deep venous thrombosis, myocardial infarction, sepsis, and aspiration pneumonia. 10 GI motility is well controlled by homeostasis between the nervous and hormonal systems.11,12 Spinal problems are known to elicit some digestive problems preoperatively, 13 and spine surgeries inevitably manipulate the spinal cord or spinal nerves, which can result in bowel movement disorder postoperatively. 14
With aging, GI function and bowel motility decreases 15 and an increasing number of elderly patients with degenerative spinal diseases require spine surgery. 16 Accordingly, the spine surgeries have increased by a large number in the past 20 years.17,18 Although POI is not considered a direct surgical complication, POI does negatively affect patient recovery and surgical outcome.10,19,20 The pathogenesis of POI following spine surgery is multifactorial, encompassing surgical stress, secretion of inflammatory mediators, imbalance of electrolyte or fluid status, perioperative anesthesia and analgesia,1,21 and direct intraoperative manipulation of the neural structures.19,20,22,23 Emerging studies have focused on investigating the risk factors for POI in patients undergoing spine surgery.24-26 A recent published meta-analysis showed several risk factors associated with POI following spinal fusion surgery. 27 However, the results were based on univariate analysis, which would be greatly impacted by confounders and there are potential patient and perioperative factors associated with POI not clarified in the literature, such as gastroesophageal reflux disease (GERD) or fluid and electrolyte imbalances. Hence, we sought to perform a comprehensive review to integrate the available literature and update the risk factor profile associated with POI after spine surgery with a more robust statistical method.
Methods
We conducted a systematic review and meta-analysis in accordance with the Cochrane Handbook for Systematic Reviews of Interventions 28 and reported the results according to the Meta-analysis Of Observational Studies in Epidemiology reporting guideline (eMethod 1). The study was registered with PROSPERO (CRD42022358218).
Search Strategy and Study Selection
MEDLINE, Embase, and Cochrane Library databases were searched from inception until November 2022 for relevant articles without language restriction. The search strategy is summarized in eMethod 2.
Inclusion Criteria
Articles meeting the following criteria were included: prospective and/or retrospective cohort and case-control studies that reported POI following spine surgery; and articles reporting at least 1 risk factor for POI. Review articles and conference abstracts were excluded from our review.
Data Extraction
Two investigators (Y.C. and C.E.W.) independently extracted the following baseline and outcome data: first author’s name, study period, inclusion and exclusion criteria, sample size, POI definition, and significant risk factors for POI.
Statistical Analysis
Risk factors for POI with multivariate analysis reported in more than 2 studies were included in the meta-analysis. Statistical analyses were performed using functions available in the metafor package in the R software environment 29 (eMethod 3). Effect sizes were presented with corresponding 95% confidence interval (CI). 30 Heterogeneity was assessed using I2 statistics proposed by Higgins and Thompson, with I2 < 25%, 25% < I2 < 50%, and I2 > 50% indicating low, moderate, and high heterogeneity, respectively. 31
Appraisal of the Included Studies
Two investigators (Y.C. and H.H.H.) independently completed a critical appraisal of the included literature using the National Heart, Lung, and Blood Institute tool for case-control studies. 32
Results
Study Selection
Our search strategy identified 3343 references from the Cochrane Library, Embase, and MEDLINE electronic databases. After screening titles and abstracts, we excluded duplicates (n = 550) and irrelevant references (n = 2768). The remaining 25 studies were retrieved for a full-text review, 12 of which were included in this review19,20,22-26,33-37 (Figure 1). PRISMA diagram. We initially extracted 3343 potential references. Eventually, 12 studies fulfilled the eligibility criteria, and were included for meta-analysis. (PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses).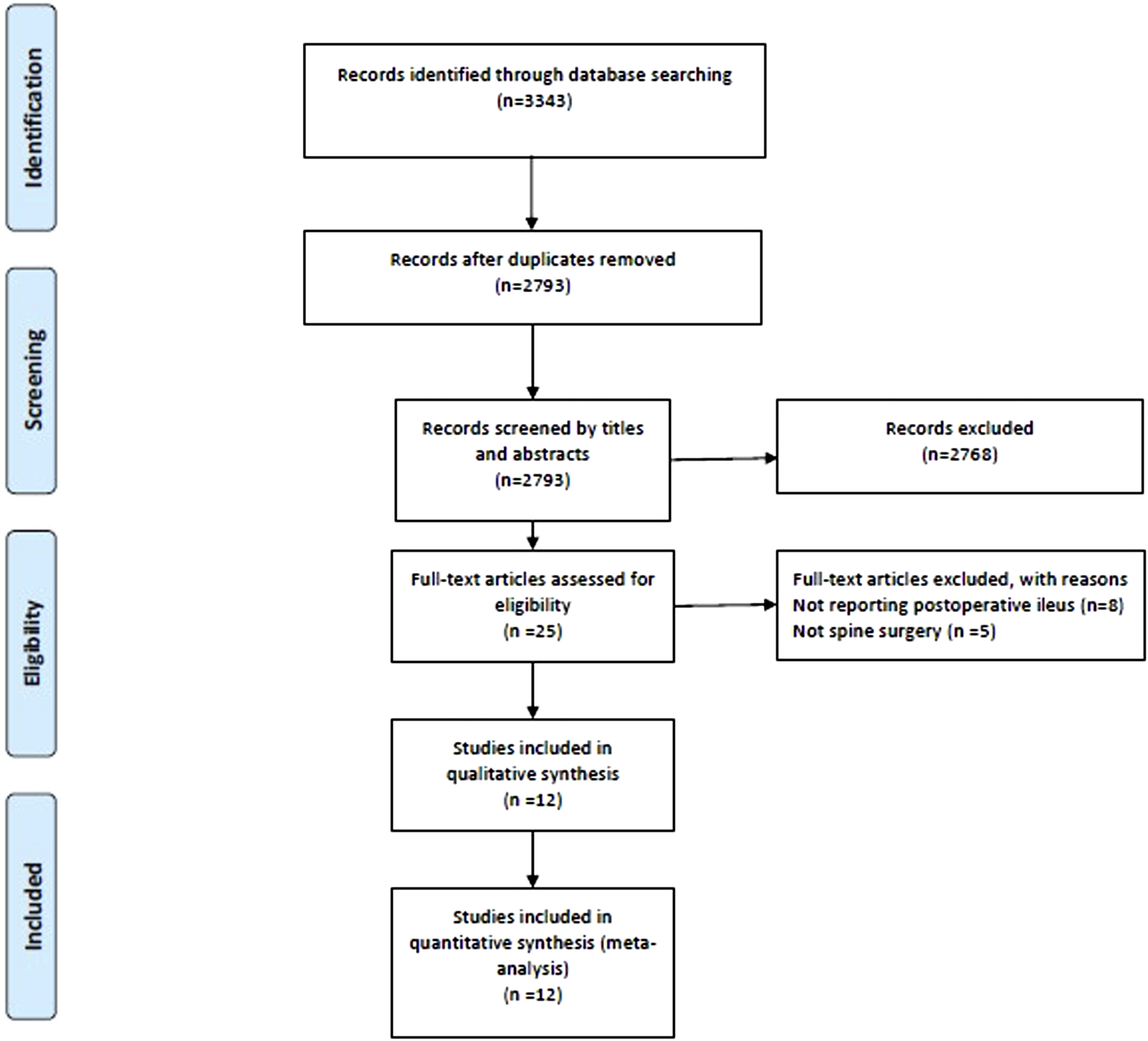
Characteristics of the Included Studies
Characteristics of Included Studies.
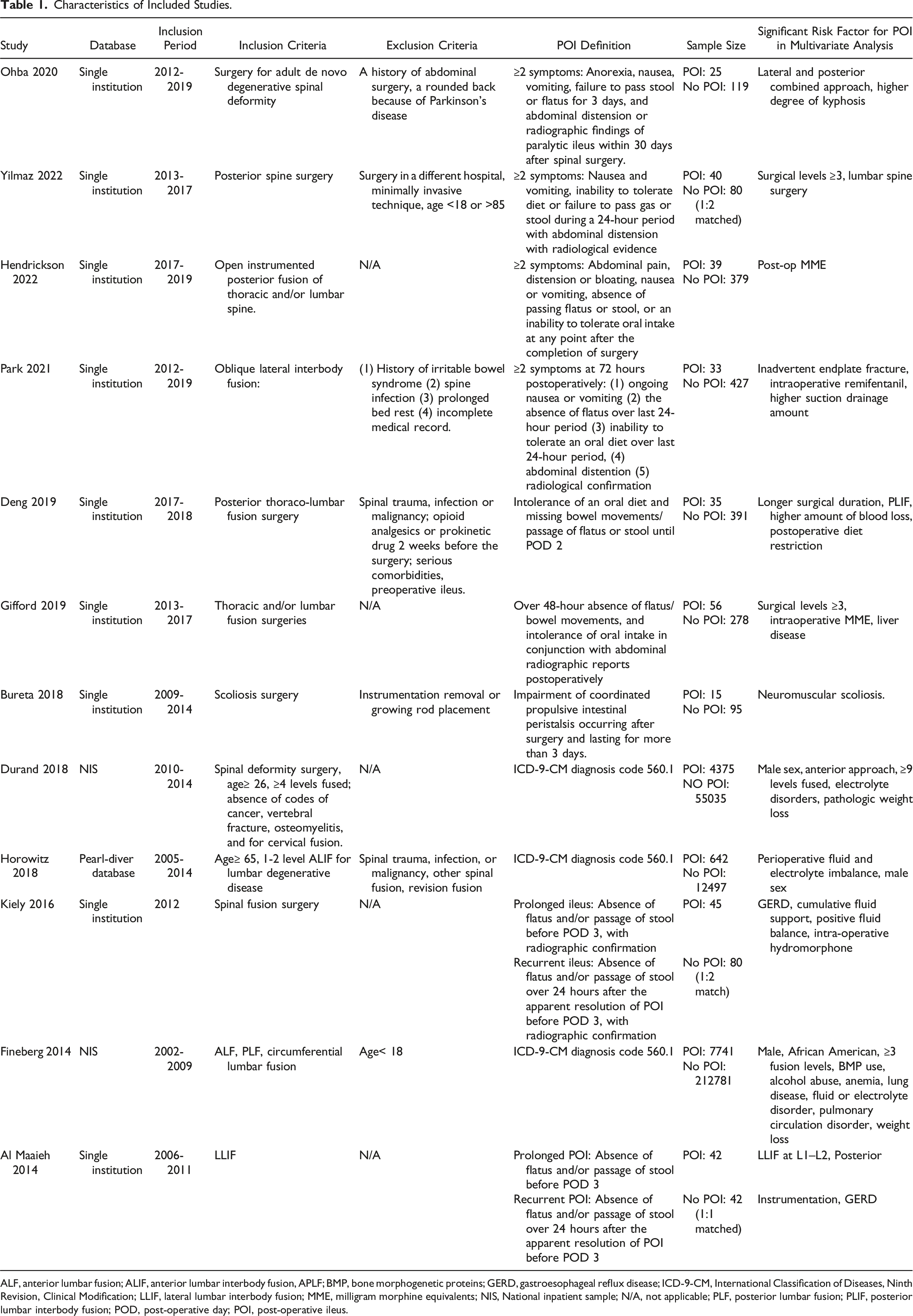
ALF, anterior lumbar fusion; ALIF, anterior lumbar interbody fusion, APLF; BMP, bone morphogenetic proteins; GERD, gastroesophageal reflux disease; ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; LLIF, lateral lumbar interbody fusion; MME, milligram morphine equivalents; NIS, National inpatient sample; N/A, not applicable; PLF, posterior lumbar fusion; PLIF, posterior lumbar interbody fusion; POD, post-operative day; POI, post-operative ileus.
Patient Risk Factors
By pooling the multivariate analysis results from the 2 studies, we found that age was not a significant predictor for the development of POI (OR, 1.03; 95% CI, 1.00-1.06, I2 = 0%, (e)Figure 1). Males exhibited a higher risk of POI than females (OR, 1.76; 95% CI, 1.54-2.01, I2 = 55%, (e)Figure 2). Patients with anemia had a higher risk of POI than those without anemia (OR, 1.48; 95% CI, 1.04-2.11, I2 = 35%, (e)Figure 3). Patients with liver disease (OR, 3.3; 95% CI, 1.2-9.08, I2 = 0%, (e)Figure 4) had a higher risk of POI. Neither GERD (OR, 2.79.45; 95% CI, .76-10.3; I2 = 80%, (e)Figure 5) nor chronic lung disease history (OR, 1.03; 95% CI, .65-1.61; I2 = 61%, (e)Figure 6) were associated with POI. There was no difference in the risk of POI between patients with and without preoperative weight loss (OR, 1.76; 95% CI, .79-3.9, I2 = 85%, (e)Figure 7). Smoking was not a risk factor for POI (OR, 1.57; 95% CI, .4-6.19, I2 = 60%, (e)Figure 8).
Perioperative Risk Factors
The presence of perioperative fluid and electrolyte imbalances was a predictor of POI (OR, 3.24; 95% CI, 2.62-4.02, I2 = 78%, (e)Figure 9). Spine surgery involving more than 3 levels was associated with a higher risk of POI compared to that with 1-2 levels (OR, 1.82; 95% CI, 1.03-3.23, I2 = 61%, (e)Figure 10).
Appraisal of the Included Studies
The quality assessment of the included studies using the National Heart, Lung, and Blood Institute tool for case-control studies is summarized in eResult1. All of the included studies were defined as having a fair study quality due to certain risk of bias without a fatal flaw detected.
Discussion
Summary of Findings of Meta-Analysis.
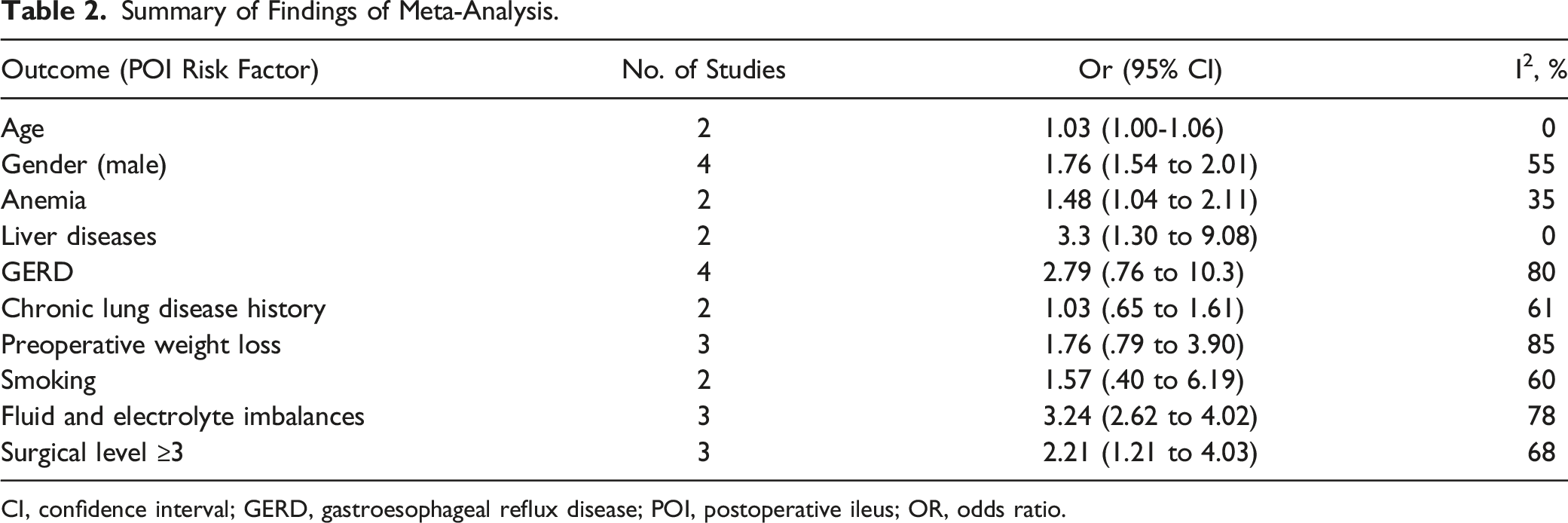
CI, confidence interval; GERD, gastroesophageal reflux disease; POI, postoperative ileus; OR, odds ratio.
In addition, through literature review, some patient characteristics were identified as potential risk factors for POI, including African American ethnicity, history of alcohol abuse, and pulmonary circulation disorder, but could not be meta-analyzed, because these factors were reported in only 1 study respectively. Similarly, perioperative factors not included in the meta-analysis but associated with a higher risk of POI were lumbar procedure (compared with cervical and thoracic), longer operative time, increased blood loss, use of bone morphogenetic proteins (BMP), perioperative morphine use, lateral lumbar interbody fusion (LLIF) at L1-L2, endplate fracture, increased suction drainage amount during oblique lumbar interbody fusion (OLIF), surgery for neuromuscular scoliosis, surgical level ≥9 level, and anterior approach in deformity surgery.
The occurrence of POI Is multifactorial.4,8,9 One of the most discussed patient characteristics related to risk of developing POI in the literature is age. 38 Although GI function and bowel motility decline with age, 15 our analysis showed that age did not contribute to the development of POI. As spinal procedures are more commonly performed in the elderly because of the higher prevalence of degenerative diseases, 39 it is reasonable that the age distribution of patients in the POI and non-POI groups would be similar, leading to no statistical difference. Although, without a clear explanation proposed, our meta-analysis is in line with studies focusing on POI following abdominal surgery40,41 that males tend to have a higher incidence of POI than in women. Liver disease was another significant risk factor identified in our study; however, it should be noted that only 2 studies22,35 reported this outcome, with a wide 95% CI. The overall significant results may be false positives due to the lack of statistical power. In addition, Gifford et al 22 defined liver disease as a history of hepatitis, fatty liver disease, or cirrhosis, while Horowitz et al used International Classification of Diseases (ICD) codes to identify patients with liver disease. This inconsistency in the definition of liver disease may have compromised the accuracy of our results. We investigated whether GERD was a significant risk factor for POI because GERD is associated with lower ghrelin levels, and ghrelin plays a role in stimulating intestinal activity through cholinergic pathways. 19 Therefore, it is possible that patients with GERD may have a higher risk of POI; however, our meta-analysis demonstrated no significant findings.
Given that manipulation of the bowel as well as its innervating nerves is relevant to POI, the surgical trajectory that demands bowel manipulation affects the occurrence of POI. At the vertebral level of interest, anterior or anterolateral lumbar spine surgeries, such as ALIF 42 and OLIF, 43 go through the retroperitoneal space and dissect and retract the visceral contents from the vertebra. Therefore, both ALIF and OLIF result in less postoperative pain than with standard posterior spine surgery by preventing paravertebral muscle dissection42,43; however, they exhibit a higher incidence of POI than with posterior surgery due to a higher degree of bowel manipulation.26,35 Conversely, LLIF and extreme lateral interbody fusion go through the lateral side of the vertebra using a transpsoas approach without bowel manipulation,44,45 which results in a lower incidence of bowel-associated complications compared to those with ALIF and OLIF. 37 In the study by Deng et al the incidence of POI was lower in the LLIF group compared to posterior approach. 33 It is noteworthy that a caveat postulated by Al Maaieh et al is that LLIF at the L1‒L2 level inherits the highest risk of POI compared to that with other levels, since the celiac plexus is located at L1 and carries parasympathetic innervation to the intestine, which is involved in intestinal motility. 37
For patients undergoing spine surgery for deformity correction, the stretching of nerve roots caused by maneuvers for severe curves can activate inhibitory spinal reflexes and cause bowel dysfunction. 46 In particular, procedures with vertebral fusion over 9 levels and using the anterior approach were both independent risk factors for POI 23 and Ohba et al found lateral and posterior combined approach, and higher degree of kyphosis correction increased the risk of POI. 24 Moreover, patients with neuromuscular scoliosis tend to have a kyphotic posture. A flexed posture in a lumbar kyphotic model inhibits GI myoelectric activity and is subsequently associated with a higher incidence of POI. 36
Several intraoperative factors have been thought to induce abnormal GI motility owing to inflammation. For example, Fineberg et al found BMP use during fusion surgery was associated with a higher risk of POI due to increased local inflammation. 20 Inadvertent endplate fracture during OLIF is also an independent risk factor for POI. 26 Endplate fractures might induce the release of cytokines and other inflammatory mediators and affect the nerve plexus in the vicinity of the vertebral column, leading to impaired GI motility. 47 Moreover, endplate fractures can cause increased postoperative pain, thereby promoting POI development.
Prolonged surgical duration in spine surgery leads to longer anesthesia time, increased blood loss, need for blood transfusion and fluid support, and several complications.48,49 Using cut-off values of surgical duration, Deng et al found that posterior thoracolumbar spinal fusion surgery over 4.375 h increased the risk of POI, 33 which aligns with the fact that patients undergoing spine surgery over 3 levels had a higher risk of POI due to longer operative time and increased intraoperative opioid use.20,22,33 Al Maaieh et al also reported that patients receiving additional posterior pedicle screw instrumentation after LLIF had a higher risk of POI than those who received a standalone LLIF approach due to longer surgical duration. 37 In addition, multilevel spine surgery, a known risk factor of postoperative urinary retention, 48 is indicative of prolonged operative duration, increased blood loss, and intravenous fluid support. Higher risk of nerve damage during these procedures would account for the higher risk of POI as well.
Regarding perioperative hemodynamics, intraoperative blood loss >750 mL was associated with a higher incidence of POI. 34 A decrease in hemoglobin concentration increases sympathetic and endocrinological stress responses, thereby leading to bowel edema and motility inhibition. 50 This finding was in accordance with our meta-analysis, which showed that patients with anemia had a significantly higher risk of POI. Increased postoperative drainage amount, signifying bleeding around the surgical field, was also an independent risk factor for POI in patients receiving OLIF. 26 Park et al postulated that increased retroperitoneal bleeding and hematoma may elicit derangement of the nerve plexuses and the release of cytokines and inflammatory mediators, leading to impaired GI motility. 26
Perioperative fluid and electrolyte imbalance is a potentially modifiable risk factor that is as high as 4-times the risk in patients without perioperative fluid and electrolyte imbalance.20,23,35 Moreover, excessive fluid support also puts patient at increased risk of developing POI. 19 Fluid and electrolyte imbalances may impair bowel movement and inhibit the GI nervous system. 50 Fluid support during spine surgery is based on the surgical procedures, duration, blood loss, and the patient’s condition. 51 Careful monitoring and management of perioperative fluid status and electrolyte levels are crucial, not only for intraoperative hemodynamics, but also for postoperative patient care.
Opioids are widely used clinically, including in spine surgery, to achieve optimal anesthesia and postoperative analgesia. 52 A higher amount of opioid use perioperatively increases the risk of POI.19,22,25,26 Several opioid receptor types, such as kappa, mu, and delta, have been identified in the intestinal tract. 53 Studies have demonstrated the dose-dependent effects of opioids on inhibiting intestinal motility.1,54,55 Park et al reported that remifentanil, a short-acting opioid with a rapid recovery time, was associated with the development of POI even when used on postoperative day 3. 26 In addition, a higher dose of opioid consumption is suggestive of more severe postoperative pain, which may impede early ambulation and further slow the recovery of bowel movement.
Postoperative care strategies to promote recovery also affect the likelihood of POI development. For instance, Deng et al reported that postoperative diet restriction may increase the risk of POI. 34 Alternatively, early enteral feeding promotes better functional recovery and patient-reported outcomes following surgery. 56 In line with postoperative care in patients undergoing abdominal surgery, early enteral nutrition in patients undergoing spine surgery lowers the incidence of POI, shortens the length of hospital stays and decreases the risk of postoperative complications.57,58
Limitations
The results of this systematic review and meta-analysis should be interpreted in the light of several limitations. First, all the included studies were retrospective in design, which was a potential source of bias due to confounding factors. Second, there was variation in the surgical procedure used across the included studies, which may have varying factors affecting the development of POI. Third, in our review, most of the single institutional studies defined POI using the diagnostic criteria from the review article by Vather et al. 2 However, for studies utilizing nationwide databases, the diagnosis of POI was based on the ICD codes. In addition, there were no reports of the severity of POI and subsequent management; for example, whether nasogastric tube decompression was needed or if prokinetic medications were prescribed.
Fourth, although liver disease and anemia were identified as significant predictors for the development of postoperative ileus, the inconsistency in the definition of these diseases may have hindered the accuracy of the analysis. Moreover, in nationwide databases, using the ICD codes may limit the data available on the disease severity.
Finally, through literature review, although several factors were reported with a higher risk of POI, we could not perform meta-analysis for these factors as they were reported only once among the included studies.
Conclusions
POI following spine surgery is detrimental to postoperative recovery and increases the risk for developing other complications. Our meta-analysis demonstrated that male sex, anemia, and liver disease were significantly associated with POI. Perioperative fluid and electrolyte imbalance and multilevel spine surgery significantly increased the risk of POI. In addition, through a comprehensive review, we identified several perioperative risk factors associated with the development of POI. The knowledge gained from this study could improve perioperative management and patient recovery after spine surgery.
Supplemental Material
Supplemental Material - Risk Factors for Postoperative Ileus Following Spine Surgery: A Systematic Review With Meta-Analysis
Supplemental Material for Risk Factors for Postoperative Ileus Following Spine Surgery: A Systematic Review With Meta-Analysis by Yu Chang, MD, Chia-En Wong, MD, Wei-Cheng Chen, MD, Hao-Hsiang Hsu, MD, Po-Hsuan Lee, MD, Chi-Chen Huang, MD, and Jung-Shun Lee, MD, MSc in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.