
Abstract
Study Design:
Retrospective database analysis.
Objective:
Spine surgeries in elderly patients have increased in recent years due to aging of society and recent advances in surgical techniques, and postoperative complications have become more of a concern. Postoperative delirium is a common complication in elderly patients that impairs recovery and increases morbidity and mortality. The objective of the study was to analyze postoperative delirium associated with spine surgery in patients aged 80 years or older with cervical, thoracic, and lumbar lesions.
Methods:
A retrospective multicenter study was performed in 262 patients 80 years of age or older who underwent spine surgeries at 35 facilities. Postoperative complications, incidence of postoperative delirium, and hazard ratios of patient-specific and surgical risk factors were examined.
Results:
Postoperative complications occurred in 59 of the 262 spine surgeries (23%). Postoperative delirium was the most frequent complication, occurring in 15 of 262 patients (5.7%), and was significantly associated with hypertension, cerebrovascular disease, cervical lesion surgery, and greater estimated blood loss (P < .05). In multivariate logistic regression using perioperative factors, cervical lesion surgery (odds ratio = 4.27, P < .05) and estimated blood loss ≥300 mL (odds ratio = 4.52, P < .05) were significantly associated with postoperative delirium.
Conclusions:
Cervical lesion surgery and greater blood loss were perioperative risk factors for delirium in extremely elderly patients after spine surgery. Hypertension and cerebrovascular disease were significant risk factors for postoperative delirium, and careful management is required for patients with such risk factors.
Introduction
Postoperative delirium is a common complication of surgical procedures in the elderly and causes difficulty in postoperative care. 1,2 The incidence of postoperative delirium ranges from 3.3% to 77%, with variation between studies depending on the patient population and surgeries. 3 -9 Delirium involves an acute generalized impairment of cognitive function that affects orientation, attention, memory, planning and organizational skills, and disturbs the sleep-awake cycle, thought process, perception, and activity level. 10 -12 Acute delirium as a postoperative complication also increases morbidity and mortality and prolongs hospitalization. 13 -15 Prevention of delirium is important to reduce these problems and the associated costs, and thus there is a need for improved understanding of the risk factors to permit early diagnosis and effective management strategies.
The term elderly is generally accepted to indicate a chronological age of 65 years or older. 16 -22 The demand for spinal surgery in elderly persons has grown with aging of society and recent advances in surgical techniques and general anesthesia. Studies of postoperative complications after spine surgery have included extremely elderly patients aged over 80 years, 23 -26 and there are several reports on the incidence and risk factors for postoperative delirium associated with spine surgery. 4,15,27 -29 However, a study of delirium after spine surgery in extremely elderly patients aged 80 years or older and including surgeries for all spinal lesions has not been performed. Therefore, in this study, the frequency of delirium after spine surgery in patients aged 80 years or older and patient-specific and surgical risk factors were examined in a retrospective analysis of a multicenter database.
Materials and Methods
A retrospective multicenter survey was performed by JASA (Japan Association of Spine Surgeons with Ambition) in 262 patients aged 80 years or older who underwent spinal surgery at 35 centers. Institutional review board approved was obtained, and all data was obtained from medical records or nursing records. Of the patients, 122 were male and 140 were female. Age ranged from 80 to 91 years, with a mean of 82.7 years. None of the patients were receiving treatment for any specific form of dementia. The causative diseases were lumbar spinal canal stenosis due to spondylosis (n = 132), cervical spondylotic myelopathy (n = 56), lumbar spinal canal stenosis due to spondylolisthesis (n = 21), thoracic-lumbar compression fracture (n = 19), cervical ossification of the posterior longitudinal ligament (n = 6), pyogenic spondylitis (n = 5), and others (n = 23). The lesions were cervical (n = 74, 28%), thoracic (n = 13, 5%), and lumbar (n = 175, 67%). The mean operative time was 171 minutes, and the mean estimated blood loss (EBL) was 289 mL. There were 87 fusion surgeries with instrumentation.
Total intravenous anesthesia was administered during intraoperative spinal cord monitoring. The drugs administered were propofol (3-4 mg/mL), fentanyl (2 mg/kg), and vecuronium (0.12-0.16 mg/kg). Anesthesia was maintained using propofol (3-4 mg/mL), fentanyl (0.75-1 mg/kg/h), and vecuronium (0-0.04 mg/kg/h).
Delirium has 4 features—(1) acute onset and a fluctuating course, (2) inattention, (3) disorganization of thinking, and (4) an altered level of consciousness—and diagnosis requires the presence of features 1 and 2 and either 3 or 4. 30 Age, gender, previous spinal surgery, body mass index, disease duration, smoking status, drug use (nonsteroidal anti-inflammatory drugs, opioids, osteoporosis agents, and anticoagulants), comorbidities (hypertension, preexisting neoplasm, diabetes, and cerebrovascular disease), and operative factors (operative time, EBL, and fusion with instrumentation) were examined as potential risk factors for postoperative delirium.
For statistical analysis, differences between 2 groups were analyzed by Mann-Whitney U test, Student’s t test, and those between 3 groups were analyzed by Kruskal-Wallis test. A multivariate logistic regression model was constructed using variables with P < .05 in univariate analysis. Multivariate hazard ratios are reported with 95% confidence intervals. Statistical analysis was performed using SPSS version 22 for Windows (IBM, Chicago, IL). P < .05 was considered to be significant in all analyses.
Results
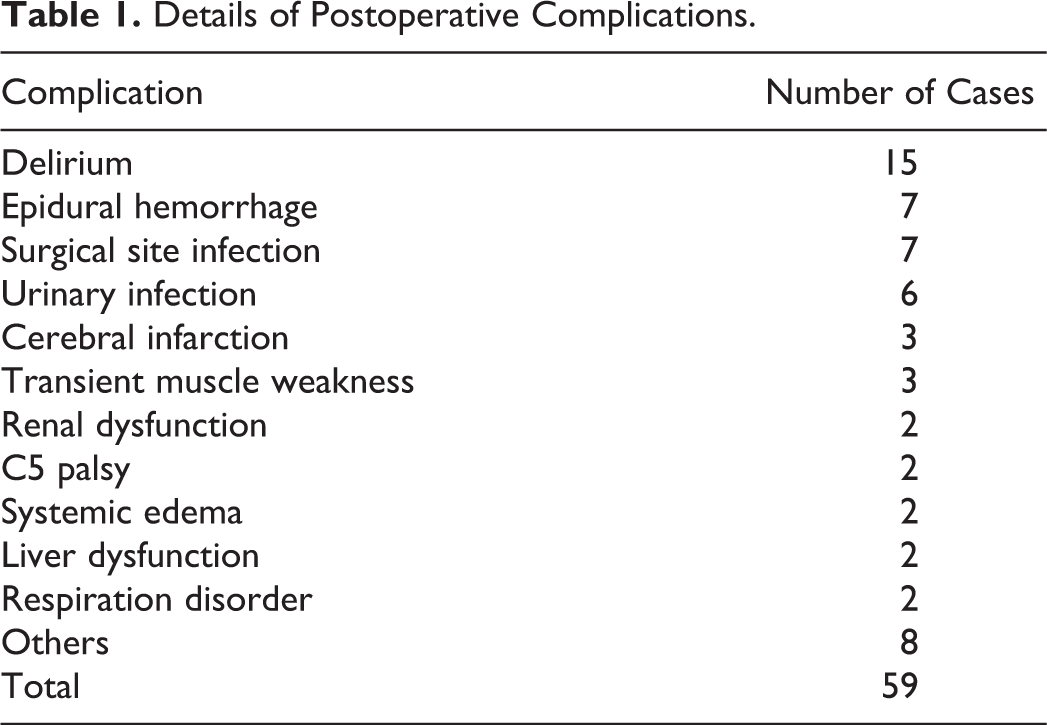
Postoperative complications occurred in 59 of the 262 operations (23%) in 50 patients. The details are shown in Table 1. Delirium was most frequent, occurring in 15 patients (5.7%), including 7 men and 8 women. Delirium lasted from a few hours to 3 days, and medication for treatment was not used in all cases. Of the 15 delirium cases, 4 (27%) occurred in the intensive care unit (ICU) on the day of surgery and improved on the next day after leaving the ICU. Delirium was more frequent in patients with hypertension (P < .01) and cerebrovascular disease (P < .05), and in those with a cervical lesion (P < .01) and greater EBL (P < .05; Table 2). Delirium occurred after 8, 1, and 6 surgeries on the cervical, thoracic, and lumbar spine, respectively, and was significantly more frequent after cervical spine surgery (P < .05; Figure 1). In multivariate logistic regression using perioperative factors, cervical lesion surgery (odds ratio = 4.27, 95% confidence interval = 1.41-12.8; P < .05) and EBL ≥300 mL (odds ratio = 4.52, 95% confidence interval = 1.50-13.7; P < .05) were significantly associated with postoperative delirium (Table 3).
Details of Postoperative Complications.
Associations Between Categorical Variables and Postoperative Delirium.
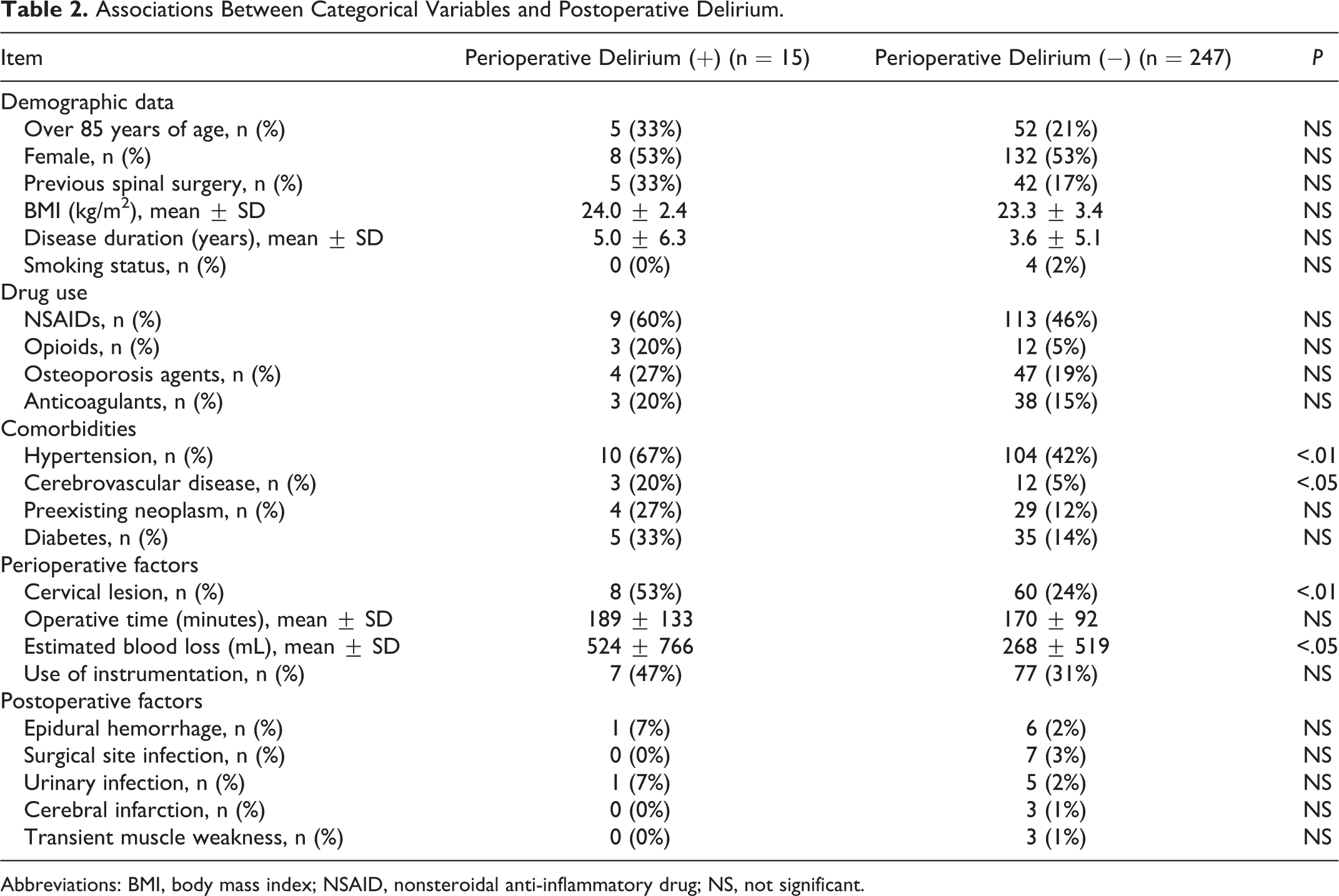
Abbreviations: BMI, body mass index; NSAID, nonsteroidal anti-inflammatory drug; NS, not significant.
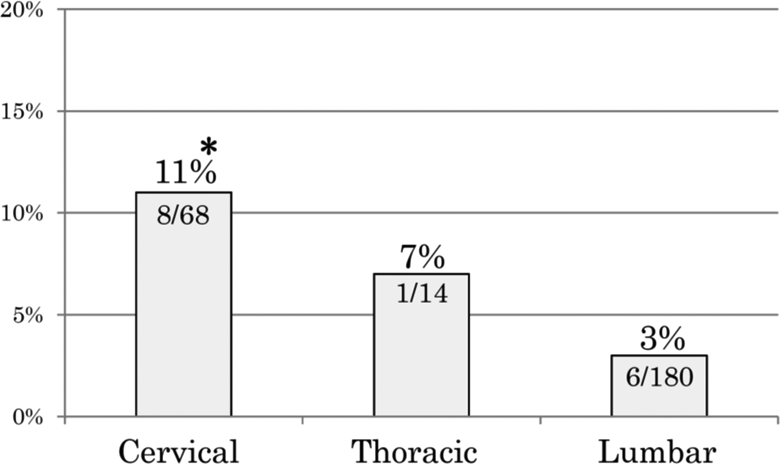
Relationship between surgical lesion and postoperative delirium. Delirium was significantly more frequent after cervical spine surgery. *P < .05.
Perioperative Risk Factors for Postoperative Delirium in a Multivariate Logistic Modela.
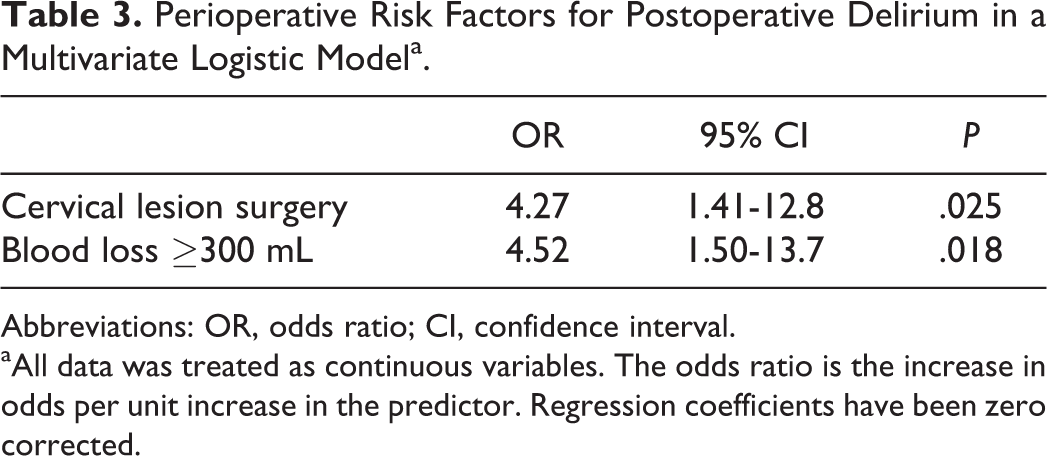
Abbreviations: OR, odds ratio; CI, confidence interval.
aAll data was treated as continuous variables. The odds ratio is the increase in odds per unit increase in the predictor. Regression coefficients have been zero corrected.
Discussion
Delirium is an acute confused state with alterations in attention and consciousness 31 that develops in 5% to 52% of older patients hospitalized for medical reasons or surgery. 32 The incidences of delirium are 7% to 14% after general surgery, 6,33 21% to 61% after hip surgery, 34 13% to 41% after joint replacement surgery, 9,35 and 7% to 77% after open-heart surgery. 36,37 The different rates in each surgery cause a major problem in clinical management.
The incidence of delirium after spine surgery has ranged from 0.49% to 21% in 6 previous reports (Table 4). Imagama et al 1 reported an incidence of delirium of 0.49% in 1012 lumbar spine surgeries in a single-center study and concluded that postoperative psychotic symptoms occurred significantly more often in older patients. Fineberg et al 29 found an incidence of delirium of 8.4 per 1000 lumbar spine procedures in an analysis of the Nationwide Inpatient Sample database, with an increased incidence in older females with more comorbidities. Kawaguchi et al 4 reported an incidence of delirium of 12.5% in patients over 70 years of age who underwent spine surgery, and 2 patients who developed postoperative delirium died during the follow-up period. Previous studies of postoperative delirium in spine surgery have included patients of all ages 1,4,27 -29 or have focused on particular surgical procedures, 28,29,38 but none have examined all spinal lesions in extremely elderly patients.
Summary of Studies on Postoperative Delirium.
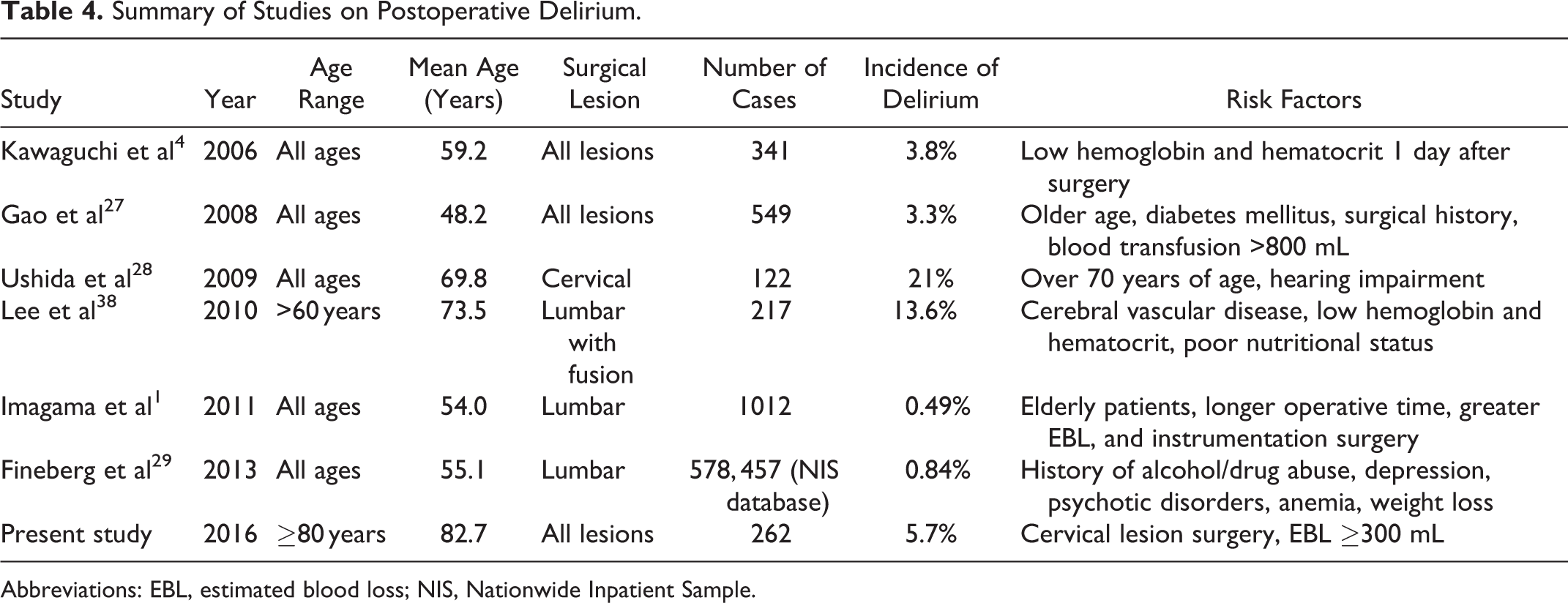
Abbreviations: EBL, estimated blood loss; NIS, Nationwide Inpatient Sample.
In the current study, we focused on spine surgery in patients aged 80 years or older. In the ultra-aging society, the demand for spinal surgery in extremely elderly patients has grown and surgeries have increased in recent years. 23,24 Thus, a study focused on extremely elderly patients is significant. In our series, delirium was the most common complication after spine surgery, and the comorbidity rates of hypertension and cerebrovascular disease were significantly higher in patients with delirium. Postoperative delirium in extremely elderly patients is relatively common and has been associated with significant increases in mortality, complications, length of hospital stay, and admission to a long care facility. 30 There is also strong evidence for an association of cerebrovascular disease with postoperative delirium. 39 Our findings are consistent with these previous results.
Delirium is an acute confused state with fluctuations in consciousness, memory, attention, perceptions, and behavior. 29,33 In extremely elderly patients, postoperative delirium also includes hallucinations, illusions, anxiety, psychomotor agitation, and disorientation, but the condition might be silent and unnoticed, or misdiagnosed as depression. 40 The adverse effects of delirium include a prolonged hospital stay and a decline in walking ability and functional restoration, which lead to further postoperative complications and higher mortality within 1 year. 41 Delirium following surgery affects readmission and discharge rates, and ultimately leads to high resource use. 42 Symptoms are usually seen on the first or second postoperative day and are often worse at night. Recovery is common, but delirium may result in death at as high a rate as 20% to 30%. 31
There are several reports on risk factors for postoperative delirium, and the risk is multifocal. Predisposing factors include advanced age, history of alcohol/drug abuse, depression, psychotic disorders, neurological disorders, anemia, fluid/electrolyte disorders, and weight loss. 29 In addition, use of a stretcher or wheelchair at admission was found to be significantly higher in patients with delirium compared to those without delirium. 4 This may indicate a poorer preoperative physical condition in patients who develop delirium, and postoperative delirium is common in older patients.
Cerebral vascular disease is significantly associated with the incidence of delirium, 39 and hypoxic brain injury might cause postoperative delirium in those with cerebral vascular disease. 43 Preoperative exposure to stress, such as pain, immobilization, and psychological stress before surgery, may also cause delirium 4 and such patients may have a poor postoperative prognosis. 44 Low serum albumin is a risk for postoperative complications and mortality, 45 and lower levels of hemoglobin and hematocrit may reduce oxygen supply to the brain, causing delirium. 46 Low oxygen saturation has also been associated with postoperative delirium. 47 Delirium in an ICU is frequently observed, with a prevalence of 46% to 70%. 48 -50 Delirium in the ICU is significantly increased by age and severity of illness, 49 and it may be associated with iatrogenic factors such as sedatives and analgesics causing brain dysfunction, in addition to sepsis, postoperative cognitive dysfunction, and changes in biomarkers and neurotransmitters. 48
In our series, cervical spine surgery and EBL >300 mL were significant risk factors for delirium. In head and neck surgery, the rate of postoperative delirium is 17% to 36%. 51 -55 Similarly, in cervical spine surgery, postoperative restriction is often necessary due to the risk of drain removal and prevention of excessive hematoma, and external fixation with a collar might also increase postoperative stress. Increased EBL might reduce albumin and cause anemia. 4,27,38 Imagama et al also reported that greater EBL and longer operative time were significantly associated with postoperative complications. 1 The systemic excess capacity is poor in extremely elderly patients, and thus it is important to suppress intraoperative bleeding as much as possible.
Prevention of delirium is important for postoperative management since this condition can produce unexpected trauma and accidental drain removal. Early postoperative free movement wearing an orthosis may be effective for preventing delirium, along with drugs such as melatonin, haloperidol, donepezil, risperidone, and benzodiazepines 56 -59 and reduced use of methylprednisolone. 28 In our series, none of the 15 cases with delirium received methylprednisolone, and this drug was not routinely used in postoperative care. Delirium may also be prevented by normalization of circadian rhythm from a disordered state caused by multiple surgery-related factors. Such prevention in the extremely elderly may be important to avoid interference with postoperative rest and nursing. A prospective study is needed to evaluate preventive methods for postoperative delirium.
This study has several limitations. First, it was a retrospective study based on a data review that did not allow evaluation of preoperative severity. Second, the details of delirium were not available. Despite these limitations, postoperative delirium is of great concern in extremely elderly patients, and the results presented here provide important estimates of inpatient morbidity and mortality after spinal surgery. This is the first study that revealed the risk factors for postoperative delirium after spine surgery in patients aged 80 years or older.
In conclusion, cervical lesion surgery and greater blood loss were found to be perioperative risk factors for postoperative delirium in extremely elderly patients, which suggests a need for careful surgical planning. Hypertension and cerebrovascular disease were significant factors for postoperative delirium. Early recognition and management of delirium based on identifiable risk factors may be useful for prevention, which may improve morbidity and delayed functional recovery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.