
Abstract
Study Design
Retrospective study.
Objectives
To demonstrate that repeat Percutaneous vertebroplasty (PVP) performed for the same cemented vertebrae in Kümmell’s disease can offer therapeutic benefit for patients with recurrent symptoms after initial percutaneous kyphoplasty (PKP) treatment.
Methods
From January 2019 to December 2021, we investigated 2932 patients with PKP. Among them, 191 patients were diagnosed Kümmell’s disease. 33 patients upon presentation of recurrent symptoms underwent repeat PVP procedure. Radiologic outcomes and clinic indices were investigated.
Results
Bone cement reperfusion surgery was successfully completed in 33 patients. The average age was 73.5 ± 8.2 years old. The kyphosis angle showed significant correction from pre-operation to the final follow-up, descending from pre-operation (20.6 ± 11.1°) to final follow-up (15.4 ± 7.9°). The vertebral heights at different follow-up appointments were significantly higher than the pre-operative appointments. The VAS and ODI scores at final follow-up were respectively 1.2 ± .8 and 27.3 ± 5.4%, which were both significantly lower than those before operation. No complications such as cement leakage into the spinal canal or cement displacement occurred during follow-up.
Conclusions
Bone cement reperfusion surgery can ameliorate kyphosis and restore vertebral height to some extent. Repeat PVP is a minimally invasive surgery that provides superior long-term results in clinical and radiological outcomes but is technically more difficult to perform.
Keywords
Introduction
Kummell’s disease (KD) is characterized by delayed vertebral collapse, dynamic instability, and progressive kyphosis with prolonged back pain or neurological deficits that occur after an asymptomatic or mild phase. 1 Many studies have discussed its pathogenic mechanism, special imaging features, and difficult treatment strategy. Percutaneous kyphoplasty has been proven to be a safe procedure for the treatment of KD. 2 Although it has many advantages such as minimal invasiveness, rapid pain relief, and vertebral height restoration, failures caused by different complications are not uncommon. Delayed cement displacement has been reported in cases of KD after cement augmentation which has serious consequences.3,4 Cement displacement is 1 of the complications of KD. It usually causes nonunion between the bone cement and the bone interface. Patients suffer from persistent or recurrent back pain due to the initial treated vertebrae. A similar imaging finding is a residual vacuum cleft showing a radiolucent line around the bone cement. 5 In this circumstance, surgical intervention is indicated.
Surgical interventions after the failure of the initial vertebral augmentation are varied. Yang et al thought that combined anterior and posterior surgery was the best salvage strategy. 6 The combination of posterior stabilization and anterior reconstruction could theoretically reduce overall morbidity and mortality. Li et al 7 reported on several open revision surgeries with pedicle screw fixation for the treatment of cemented vertebral nonunion. However, these open revision procedures are associated with large blood loss and long operation times, which may be difficult to tolerate, especially in the elderly. Only a few studies have reported repeat PVP for the treatment of recurrent pain resulting from refracture of the same segment in patients with OVCFs.5,8,9 Due to the characteristics of KD, repeat PVP may be the best treatment approach for the symptomatic recurrence of KD with no or only mild neurological symptoms. We assume that bone cement reperfusion revision surgery is an effective approach to restore the integrity and stability of the affected vertebra in the early stage and prevent delayed nerve injury. In this retrospective study, we reviewed the radiographic findings and clinical outcomes in patients who underwent bone cement reperfusion revision surgery at our institution. We also summarized the experience of the revision surgery.
Methods and Materials
Between January 2019 and December 2021, we investigated 2932 patients with OVCFs who underwent initial PKP. Based on preoperative imaging data, 191 patients were further diagnosed with Kummell’s disease. Of them, 50 patients showed symptomatic recurrence. Thirty-three patients underwent a repeat PVP procedure and provided written informed consent. Ten patients wanted conservative treatment. Seven patients underwent posterior decompression due to lower extremity neurological symptoms. Our study was approved by the ethics committee of the First Affiliated Hospital of Soochow University, China (Approval No. SUDA20221220A01). Informed consent was obtained for all patients.
Inclusion Criteria
(1) Patients diagnosed with KD by initial image data (2) Patients who previously underwent percutaneous kyphoplasty (3) Physical examination revealed percussion pain without neurological deficit symptoms (4) Magnetic resonance imaging (MRI) showed refracture at the same cemented vertebra
Exclusion Criteria
(1) Patients diagnosed with common OVCFs by initial image data (2) Physical examination revealed neurological deficit symptoms (3) Magnetic resonance imaging (MRI) showed fracture at the different segments (4) Patients with evidence of spinal infection or tumor
Detailed Indication
After the first PKP treatment, Kummell’s disease patients developed recurrent back pain symptoms without related lower extremity neurological symptoms. Physical examination revealed percussion pain at the same site as the first treatment. There is no significant relief after conservative treatment. When imaging examinations show that the vertebra is unstable due to the presence of bone cement and there are revealed fissures around the bone cement, we believe that the conditions for re-puncture are available. In this case, we would consider bone cement reperfusion surgery. The decision-making flow chart is shown in Figure 1. A decision-making flow chart.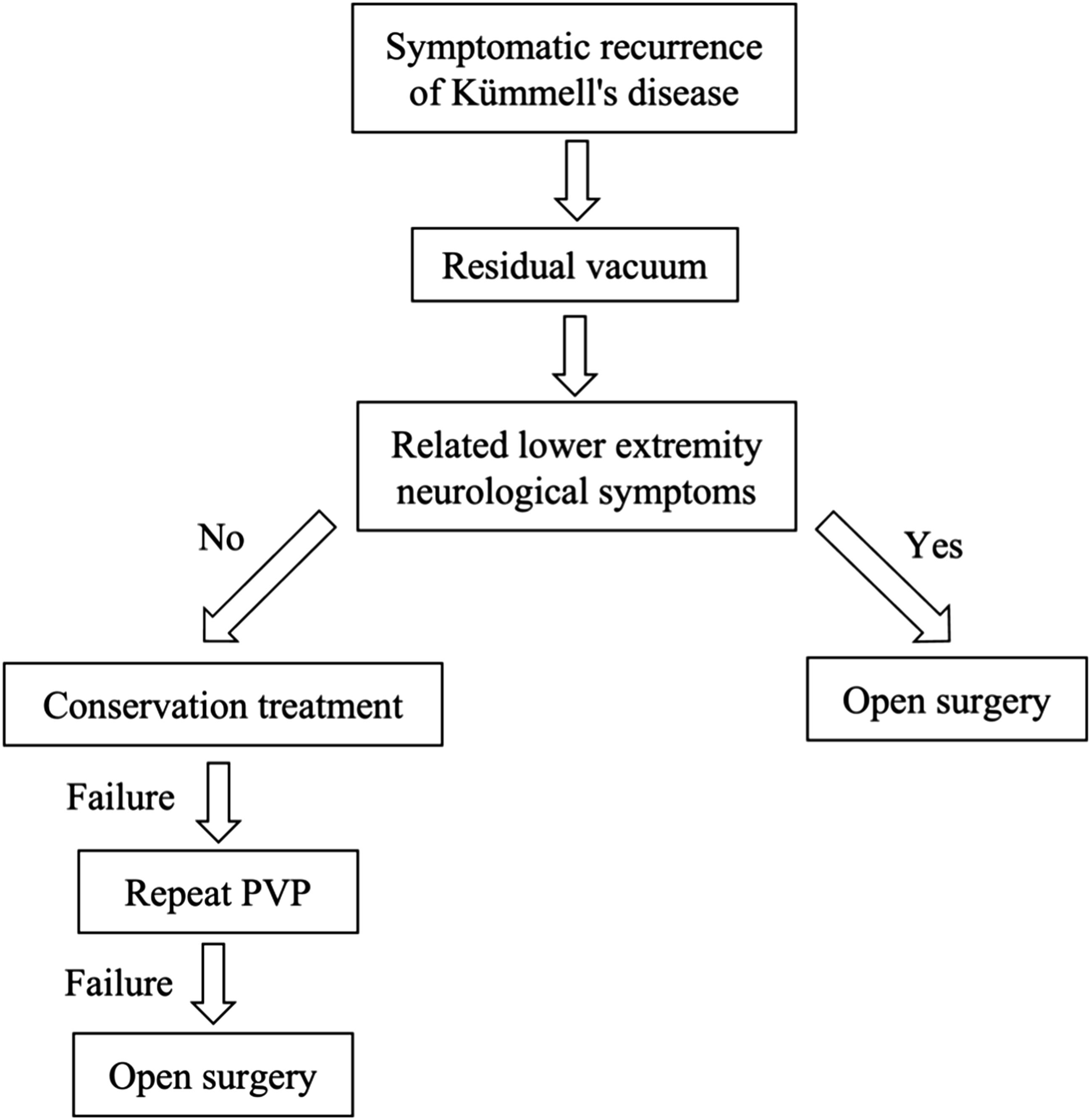
Repeat PVP Procedure
Patients were placed in the prone position, and the pedicle surface of the refractured vertebra was projected and marked under C-arm fluoroscopy. The surgeon punctured the needle through the skin and into the vertebral body via the bilateral transpedicular approach. One puncture needle was placed into the fissure above the cement, and another was placed into the fissure below the cement. To reach the residual fissure areas around the cement, the needle insertion angle was adjusted under multiple fluoroscopies. After the working channel was established, the needle core was pulled out. Then we injected the prepared bone cement (polymethyl methacrylate).
Imaging Measurement and Clinic Outcome
All patients were examined at 3 days and 3 months postoperatively. They were asked to undergo reexamination every year thereafter. Radiologic measurements and clinical questionnaires were obtained by the same surgeon on our team. The anterior and middle vertebral heights were measured on a lateral radiograph. The ratio of vertebral height = (the height of fractured vertebra)/(the mean height of adjacent vertebrae)∗100%. The kyphotic angle was measured by Cobb’s method, which is formed by the lines between the upper endplate of the vertebra above the injured vertebra and the lower endplate of the vertebra below the injured vertebra in the standard lateral radiograph. The concrete method of measurements is shown in Figure 2. Measurement of spine parameters. Red lines show the measurement of kyphosis angles. Black lines show the measurement of anterior vertebral height. White lines show the measurement of middle vertebral height.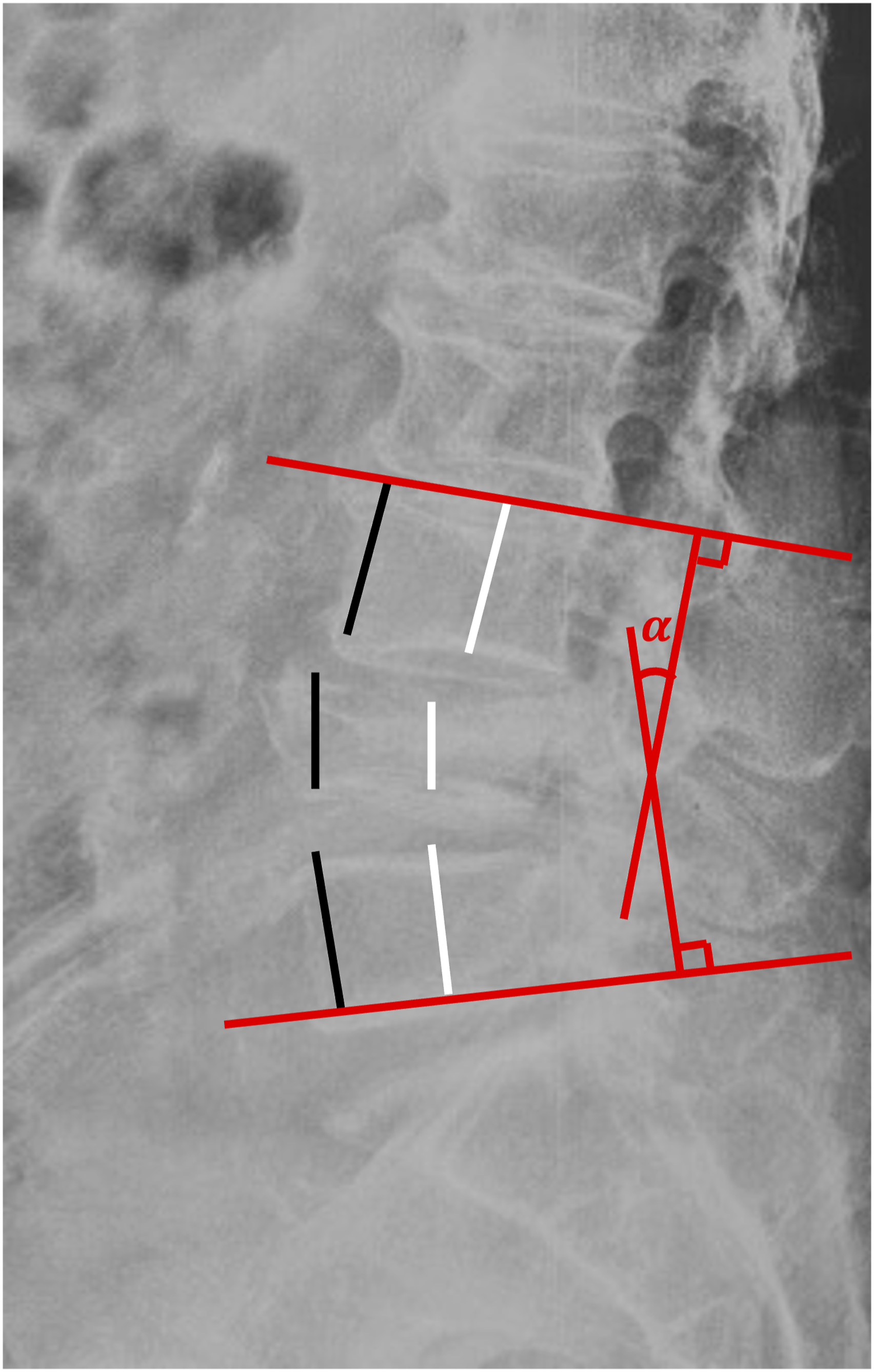
The visual analog scale (VAS) scores of the patients were calculated and compared (0-10 points). The higher the score, the more severe the pain. 10 Complete pain relief was defined as a score of 1 to 3, partial pain relief was defined as a score of 4 to 6, and unrelieved pain was defined as a score of 7 or above. The Oswestry Dysfunction Index (ODI) scores of the patients were calculated and compared. The higher the score was, the more serious the dysfunction was. 11 The ODI recovery rate (RR) was also calculated. RR = (preoperative ODI − postoperative ODI)/(preoperative ODI)∗100%. 12 At every follow-up visit, the patients were also asked whether they were satisfied with the procedure.
Statistical Analysis
SPSS (Version 26.0) was used to analyze the data. The normality was examined by the Kolmogorov-Smirnov test. Normally distributed measurement data were represented by the mean ± std. Preoperative and postoperative data, including ODI and VAS scores, the height of fractured vertebrae, and the kyphotic Cobb angle, were assessed using one-way ANOVA. The LSD test were used for multiple comparisons. P value less than .05 was statistically significant.
Results
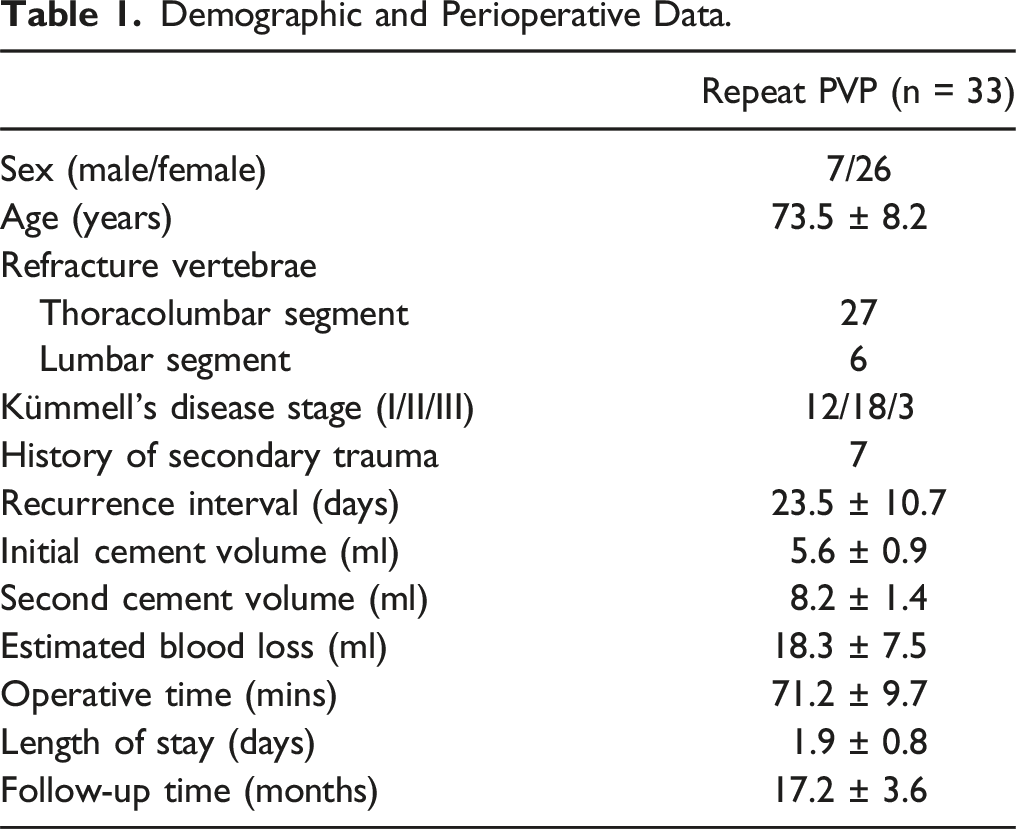
Demographic and Perioperative Data.
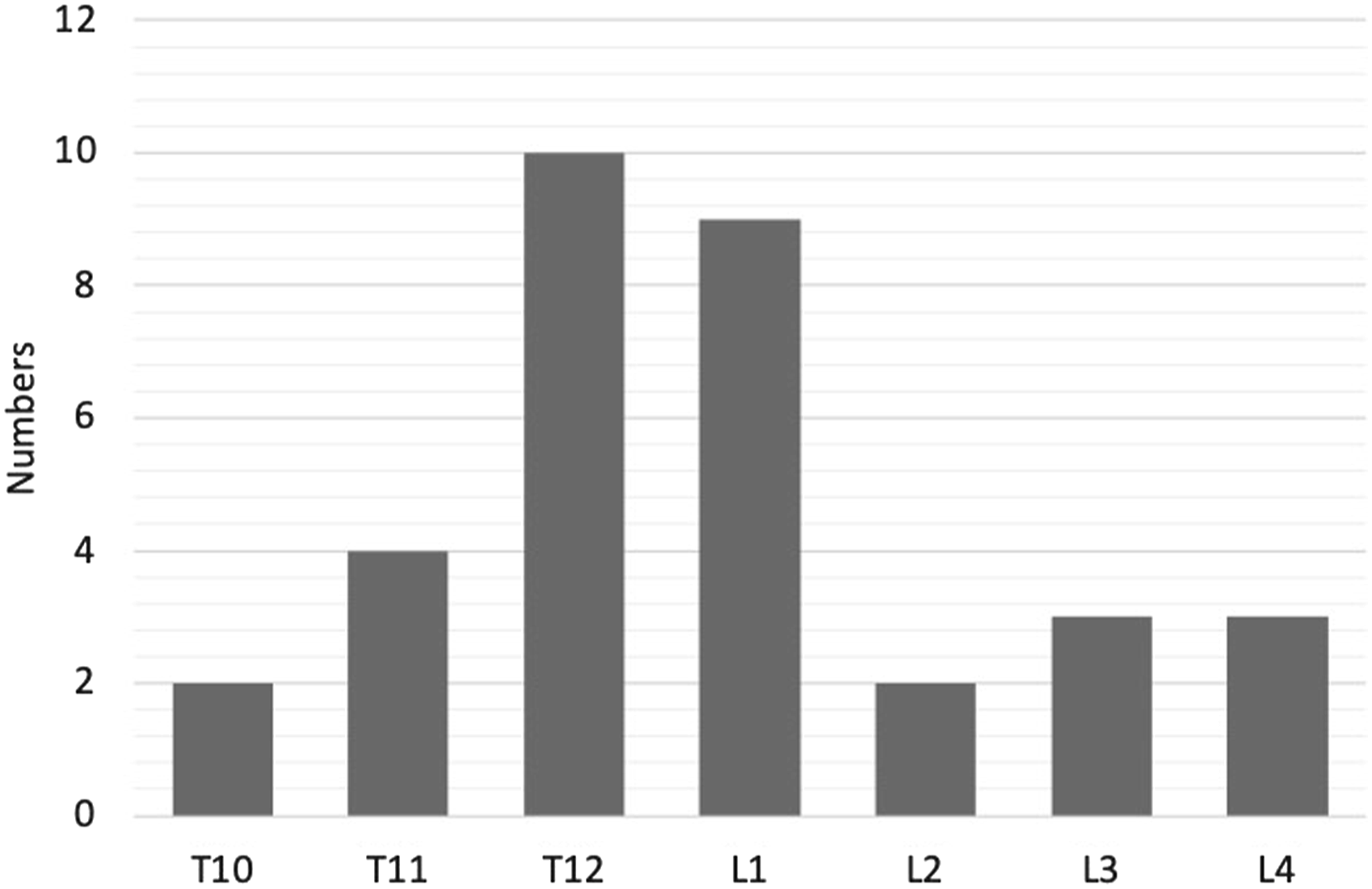
Distribution of the injured vertebrae.

A 66-year-old female patient who presented with intractable back pain 1 weeks received revision surgery. (A) MRI manifested L2 Kümmell’s disease. (B, C) Anteroposterior and lateral radiographs 2 weeks after primary PKP surgery. (D) MR showed a rim of fluid around cement with residual bone marrow edema. (E, F) Anteroposterior and lateral radiographs 3 days after repeat PVP. It is observed that the second inject of cement in L2 combined tightly with the previous cement mass and almost filled the entire vertebral body. (G, H) CT showed intact cement in L2 vertebra without displacement at 3 months follow-up.
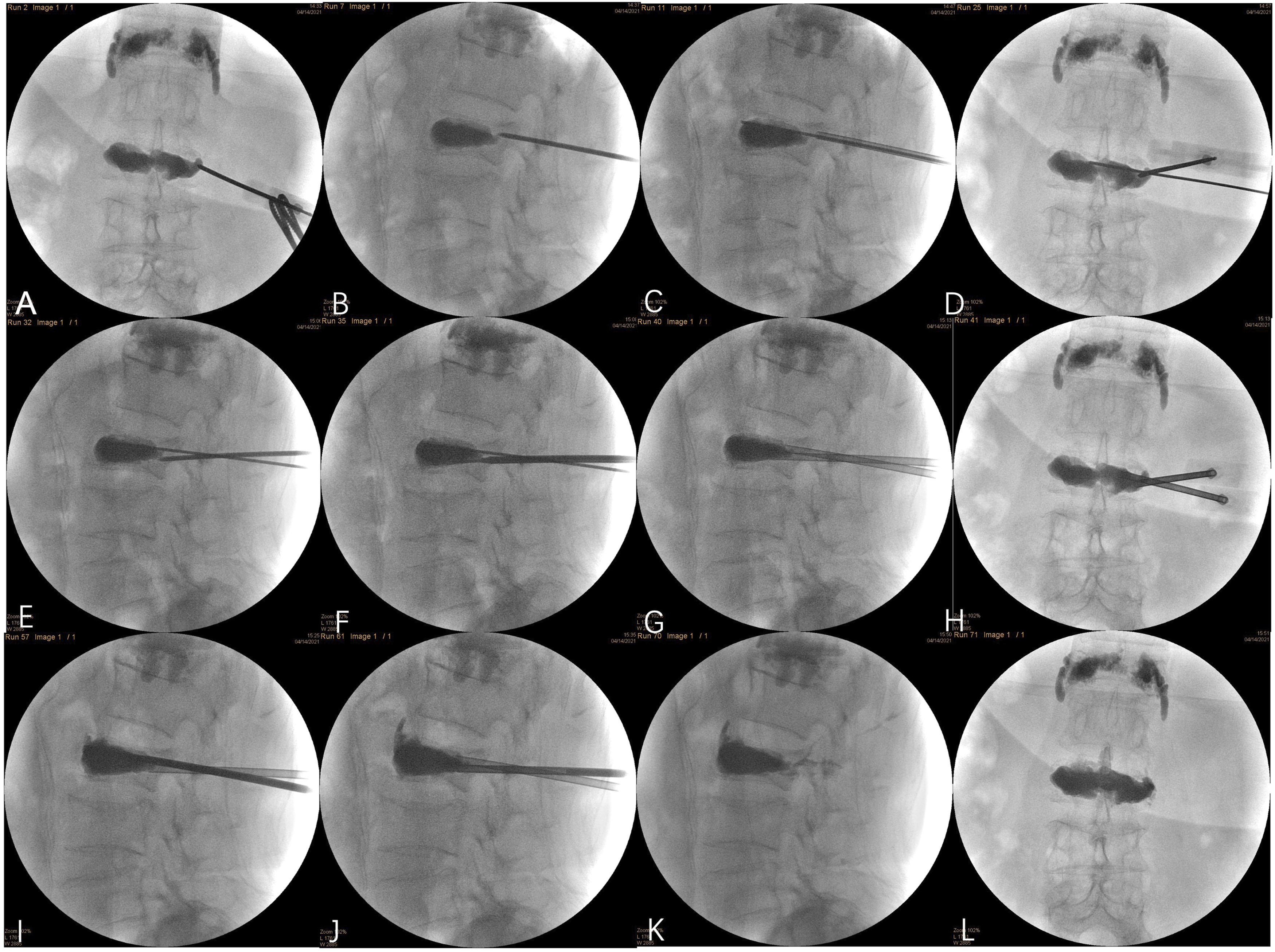
Intraoperative information of second revision operation. (A-F) Puncture through the left pedicle of L2 to the fissure above and below the bone cement. (G, H) Establish the bone cement channels. (I, J) Inject the bone cement. (K, L) Anteroposterior and lateral radiograph from C-arm fluoroscopy.
Clinical Outcomes.
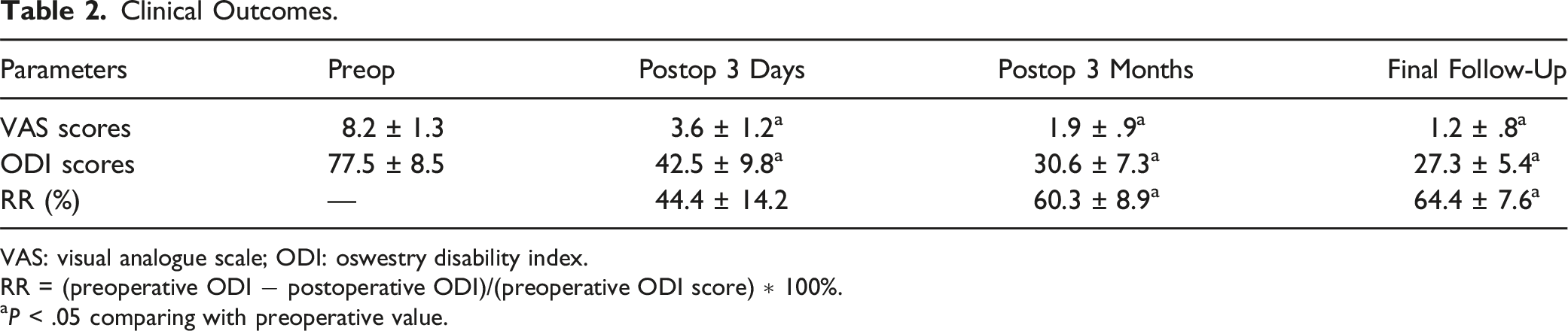
VAS: visual analogue scale; ODI: oswestry disability index.
RR = (preoperative ODI − postoperative ODI)/(preoperative ODI score) ∗ 100%.
aP < .05 comparing with preoperative value.
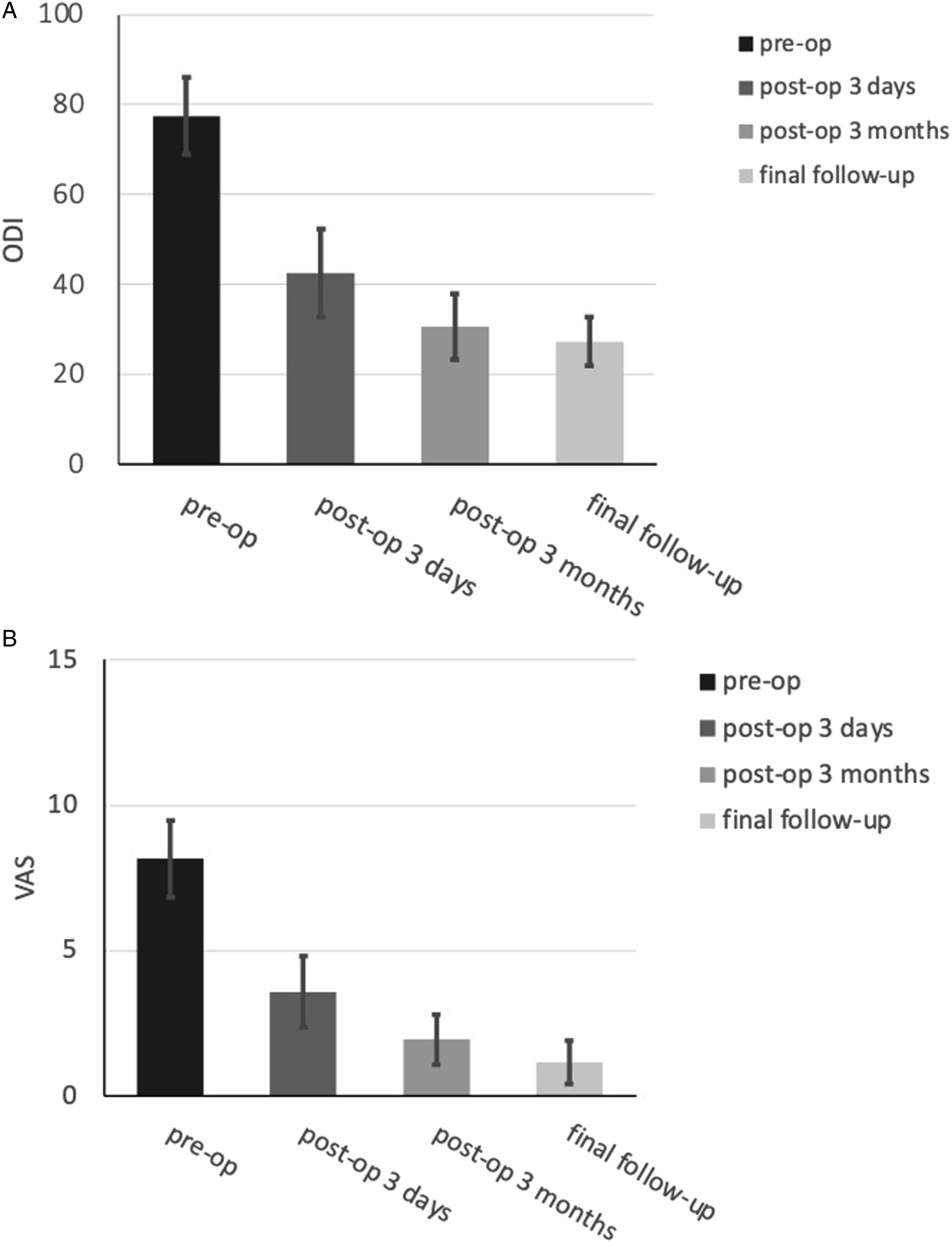
ODI scores (A) and VAS scores (B).
Radiological evaluation results.

The ratio of vertebral height = (height of fractured vertebrae)/(mean height of adjacent vertebrae) ∗ 100%.
aP < .05 comparing with the previous follow-up value.
bP < .05 comparing with preoperative value.
Discussion
In our study, the pain scores in all the patients were significantly improved. Because repeated PVP did not require balloon dilation, the correction of vertebral heights and the kyphotic angle was not as significant as in the initial PKP but was still statistically significant after surgery compared to that before surgery. Furthermore, the ODI and VAS scores showed significant differences within 3 days post-operation, but not at the 3-month follow-up or thereafter. Bone cement reperfusion surgery is an effective and less invasive method with a mean blood loss of 18.3 mL. Significant pain relief enabled patients to walk on the first day. Elderly patients stay in the hospital for 1.9 ± .8 days and do not need to experience the complications caused by open surgery, such as lung infection and deep vein thrombosis.
Recent studies have demonstrated that the refracture rate of OVCF in the same cemented vertebrae is .56% to 2.6%.13,14 However, due to the characteristics of KD, patients with KD are more prone to refracture than those with OVCFs. Lin et al 15 proposed that the fluid sign around the bone cement might indicate poor anchoring between the cement and the residual bone in the treated vertebrae. The lack of anchoring in the vertebra which causes cavity or pseudo joint may indicate the presence of a new fracture around the cement or poor fracture healing. Almost all patients have symptomatic recurrence because of this situation. Due to the cavity or pseudo joint, the cement appeared to be wrapped in “water” in the T2 image. The balance between the relative stability of the cement and the trabeculae may be broken over time. These patients will gradually develop intractable back pain and even neurological deficits. In our present study, almost all patients have symptomatic recurrence after the cavity or pseudo joint occur in MRI. Therefore, we assume that the larger and deeper fissures associated with KD are good indications for a secondary injection of bone cement.
Firstly, the recurrent pain of patients mainly caused by the insufficient amount of the bone cement. There is not yet a consensus on the optimal volume of bone cement to inject. Although a small volume of injected cement can control pain, 16 it is generally believed a sufficient amount of bone cement should be filled in patients with KD due to the easily occurrence of residual fissures. However, even if the initial vacuum cleft is not fully filled, patients still experience some degree of pain relief. Once misdiagnosed KD as common OVCF, the injection amount of bone cement will occur errors. Patients in our study developed excruciating back pain after 23.5 ± 10.7 days of pain relief, and only 7 patients had a history of secondary trauma. The exact mechanisms are uncertain. On the 1 hand, this is partly due to an insufficient amount of bone cement remaining after primary balloon dilation. On the other hand, some reports explained that the space could have been created by necrosis, which may have been caused by thermal effects and poor revascularization at the bone-cement interface. 17 Li et al 9 proposed several factors contributing to the phenomenon, such as no-osteoconductive PMMA, osteoporosis, and biomechanical effect changes between the insufficient bone cement and the residual bone. In our study, the volume of cement injected in the second procedures was larger than that injected in the initial procedures (8.2 ± 1.4 mL vs 5.6 ± 0.9 mL), and no cement leakage occurred. This means that a residual vacuum cleft may have created a real space where bone trabeculae are scarce.
Moreover, many studies have suggested that the main factor contributing to delayed neurological deficits is instability at the fracture site. 18 We attributed the patient’s recurrent pain to the unstable condition of the bone cement. Through a complete preoperative examination, we found no attributive findings except for the continued abnormalities at the initial treated vertebra. MRI showed fluid signs around the cement. Pseudarthrosis and movable cement mass within the vertebra were shown in hyperextension and hyperflexion radiographs. Also, we discovered that the initial cement had loosened and could be moved by the puncture needle intraoperatively. Traditionally, anterior surgery allows the removal of bone cement to allow thorough decompression, and artificial vertebral bodies or titanium mesh can be employed to reconstruct the stabilization of the anterior column. However, the trauma is massive. The implant may ultimately appear as if it is sinking or loosening, thus affecting the curative effect. 19 Li et al 7 reported several open revision surgeries with pedicle screw fixation for the treatment of cemented vertebral nonunion. Screw loosening causing fixation failure tends to occur in the posterior surgery. 20 In addition, these surgical interventions can be challenging in patients of advanced age with various basic diseases. Patients are also more likely to undergo minimally invasive surgery. In our present study, the purpose of revision surgery in patients experiencing refracture is to anchor the cement to restore vertebra stability. This was also demonstrated by improvements of vertebral heights and kyphotic angles during follow-up.
We also summarized our experience in performing bone cement reperfusion surgery (repeat PVP) for the treatment of KD with symptomatic recurrence. First, an intravertebral residual vacuum cleft is the basis for repeat PVP. MR images show the large transparent region around the cemented vertebrae. Hence, a thorough imaging examination before surgery is necessary to decide whether bone cement reperfusion surgery can be performed. Based on the analysis of the refractured vertebrae, it was believed that the initial amount of bone cement was insufficient and the unequal distribution of bone cement resulted in the bone cement nonunion. The residual cleft between the cement and bone interface provides the possibility of repeat PVP, especially in patients with KD.
Second, accurate needle puncture into the residual cleft is important. The ideal position of the puncture route was dependent on the degree to which the initial procedure left the vertebrae unfilled. It is sometimes difficult to identify the pedicle because of previous cement blocking field of view perspective. The pedicle of the vertebra can be positioned through the pedicle of the upper and lower vertebrae, while multiple anteroposterior and lateral fluoroscopy is required to confirm that the puncture needle can enter the vertebra through the pedicle. To reach the upper and lower areas within the vertebra, we adjusted the puncture needle in an upward or downward through the pedicle. Upon entry, if the punctured needle is blocked by previous cement, a Kirschner wires can be used to break through the blocking cement. Both unilateral and bilateral pedicle punctures can be performed in repeat PVP. Based on our experience, we concluded that determining the puncture site and path under C-arm fluoroscopy is essential at the beginning of surgery.
Third, restoring the stability of the vertebra and achieving good therapeutic results are the final goals. The anterior 1/3 of the vertebra is the area that bears the highest pressure according to Denis’s three-column theory. 21 On the 1 hand, the potentially ruptured anterior edge should be blocked. On the other hand, the anterior column of the vertebra needs adequate support. We used special bone cement perfusion techniques proposed by Yang et al 22 For patients with ruptured anterior edges, we injected late-period cement to block the anterior cleft. Then, medium-period cement was used to fill the residual cleft. This method can promote the distribution of cement and strengthen the riveting force with surrounding bone. Our aim was to tightly combine the second shot of cement mass with the previous cement mass to fill the entire vertebra.
Fourth, the proper amount of bone cement is crucial. Excessive bone cement increases the incidence of leakage, and an insufficient amount of bone cement cannot fill the cleft to provide adequate support. How can the proper amount of bone cement be determined? According to our experience, a possible reference is the apparent rebound of the push rod during injection. We also recommend jointing the initial bone cement that is unevenly distributed in the vertebrae. Because of the unpredictable fracture patterns, the injected amount of bone cement and the speed of injection require individual judgment. Although more cement could be injected intraoperatively than in the initial operation, it is still emphasized that cement must be injected carefully under fluoroscopic guidance to prevent cement leakage.
Our previous study found that the KD patient post-surgery developed pain at 23.5 ± 10.7 days. So, patients should pay more attention to wearing thoracolumbar braces within 1 month after surgery. In addition, the incidence of refracture in the thoracolumbar segment was 81.8%. The thoracolumbar region involves the physiological curvature of the spine, which is prone to fracture in the event of trauma or vertical gravity injury. For cemented vertebrae, cement fretting is more likely to be amplified and lead to refracture. We believe that thoracolumbar braces can reduce vertebral bone tissue pressure, trabecular friction, and facet joint movement. Therefore, integrated anti-osteoporosis therapy and thoracolumbar braces are necessary for perioperative rehabilitation. In the present study, 7 patients with neurological symptoms who were not included in the study underwent PVP or intraoperative VP procedures, followed by laminectomy and short segmental fixation. The patient’s postoperative symptoms were also relieved. Therefore, if repeat PVP fails to relieve pain, other open surgeries can still be performed as a remedial measure.
Limitations
This study is limited by its retrospective nature. Because this complication of KD is peculiar, the study population was relatively small, and most patients were transferred after receiving their first treatment at local hospitals. When patients have neurological symptoms, we will immediately consider posterior surgery. Due to different indications, no comparison can be made. Therefore, another limitation is that this study is an uncontrolled case series that only emphasizes the feasibility, safety, and effectiveness of bone cement reperfusion revision surgery. A further prospective study comparing minimally invasive surgery with open surgery should be carried out.
Conclusion
Symptomatic recurrence caused by cemented vertebral nonunion is the primary cause of revision surgery in patients with Kümmell’s disease. Bone cement reperfusion surgery can ameliorate kyphosis and restore vertebral height to some extent. Repeat PVP is a minimally invasive surgery that provides superior long-term results in clinical and radiological outcomes but is technically more difficult to perform. Additionally, for the major symptoms that can be resolved by surgery, standardized anti-osteoporosis treatment is also essential.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is supported by the Youth Fund for Medical and Health Basic Research of Suzhou (SYS2020096), Clinical application-oriented Innovation Foundation of China National Orthopaedic and Sports Rehabilitation Clinical Medical Research Center (2021-NCRC-CXJJ-PY-16), National Science Foundation of Jiangsu Province (BK20200199).