
Abstract
Study Design
Retrospective study.
Objective
This study aimed to evaluate the ability of the mortality and adverse events prediction following metastatic spinal surgery of MRI-based cross-sectional psoas muscle area (PMA).
Methods
A retrospective chart review, 120 patients who had undergone metastatic spinal surgery were included. The cross-sectional area identified the PMA under MR-imaging at the L3 or L4 pedicle level, which was classified into 3 tertiles. We used univariate and multivariate cox proportional hazard regression to assess whether PMA was associated with 30-day, 90-day, 1-year, and overall mortality.
Results
The small psoas tertile group populations had a higher mortality rate than the large psoas tertile group. PMA in T1 and T2 had a probability of a higher 90-d mortality rate than PMA in T3 (T1 VS T3: P = .29 and T2 VS T3: P = .12). The median survival time was 7 months, 9 months, and 10 months in PMA T1, T2, and T3, respectively. PMA in tertile 2 had a significantly higher mortality rate of 38% compared to PMA in tertile 3 (HR 1.38, 95% CI .83-2.32, P = .02). Considering PMA as a continuous variable, every 1 mm2 increment of PMA resulted in the increase survivorship of 1% (HR .99 with 95% CI .99-1)
Conclusion
The MRI-based cross-sectional PMA tends to predict the 90-d mortality rate and overall mortality rate in spinal metastasis patients who underwent spinal surgery. The PMA should be considered one of the prognostic factors in the treatment of metastatic spinal patients
Introduction
The spine is the most common site of bone metastases, accounting for approximately 50% of cases, and spinal metastasis occurs in about 5% to 10% of patients with primary cancer (Choi SH et al., 2020; Parkin DM et al., 2000; Ware JE Jr, 2000).1-3 The survival rates of metastatic spinal tumors are increasing with improved diagnostic modality and treatment. However, the mortality and adverse events in metastatic spinal surgery were still high, so the preoperative scoring systems may guide clinical decision-making and stratify therapies regarding surgery or palliative care. In 2015s, Dardic et al studied the prognostic scoring systems for spinal metastases and showed Bauer or modified Bauer has an impact on predicting the remaining survival in patients with spinal metastases. Also, the New England Spinal Metastasis Score (NESMS) and Skeleton Oncology Research Group machine learning algorithms (SORG-MLAs) had a good potential utility of predicting major mortality for decision-making in the clinical guide of treatment following metastatic surgery (Park S et al., 2015; Lee CH et al., 2015; Hibberd CS and Quan GMY, 2017; Balain B et al., 2013; Tokuhashi Y et al., 2014; Wibmer C et al., 2011; Dardic M et al., 2015; Schoenfeld AJ et al., 2016; Karhade AV et al., 2020).4-12
Sarcopenia is a progressive and generalized skeletal muscle disorder that is associated with an increased likelihood of adverse outcomes, including falls, fractures, physical disability, and mortality. Low muscle strength is the key parameter of sarcopenia (Cruz Jentoft et al., 2019). 13 The computed tomography-based cross-sectional psoas muscle area (PMA) has been proposed as a useful prognostic factor for predicting mortality and adverse events in spinal metastasis surgery. Dohzono et al showed low CT-based PMA (0–25%) is a poor prognostic factor of survival rate in cervical spinal metastatic surgery (Dohzono et al, 2019). 14 Zakaria et al classified the PMA into 3 tertiles. The tertile-1 (low muscle mass) can predict 90 days and overall mortality in metastatic spinal surgery. Hu MH. et al reported that CT-based PMA is a prognostic factor for 90-day survival and improves the discriminatory ability of the earlier-proposed preoperative scoring system in Asian population (Hu MH et al, 2022). 15
Most of published studies evaluated the CT-based cross-sectional PMA but there was no published study which evaluated the MRI-based cross-sectional PMA for prediction the mortality and adverse events in spinal metastatic surgery. Most of spinal metastatic patient commonly underwent the MRI of spine for preoperative evaluation. This study aimed to evaluate the ability in the mortality and adverse events prediction following spinal metastatic surgery of MRI-based cross-sectional PMA and the correlation between CT-based and MRI-based cross-sectional PMA for prediction the mortality.
Methods
The data were obtained from the medical database of the Department of Orthopedic Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University. We identified consecutive spinal metastasis patients who underwent palliative spinal surgery, between 2009 and 2020. The study was approved by the Siriraj Institutional Review Board (SIRB) (COA No. 569/2563(IRB1)) The informed consent have been deemed exempt from the SIRB.
The inclusion criteria are patient who aged more than 18 years old, patient who has histopathological confirmed spinal metastatic disease, patients who underwent MRI that could be used for morphometric analysis cross-sectional area of the psoas muscle. The exclusion criteria are patients who had more than one primary cancer origin; patients who had any congenital disorder; patients with psychosis or impaired cognitive function; patients who did not previously receive radiotherapy, chemotherapy, or surgery.
Data Source and Variables
We collected demographic data of patients (age, sex, number of spinal metastasis, primary of cancer type, internal organ metastasis, underlying disease), preoperative status (Frankel score, American Society of Anesthesiologists Classification (ASA), The Eastern Cooperative Oncology Group performance status (ECOG)), postoperative status (Level of surgery), and prognostic score (SORG, Nomogram, Modified-Bauer score, NESMS). Morphometric analysis of PMA at the L3 pedicle (or L4 pedicle if the tumor had involved each of the L3 pedicle) was performed by two spinal surgeons at Siriraj Hospital. The PMA measurement was performed twice and 3 weeks apart. The PMA was calculated by cross-sectional area in axial view of magnetic resonance imaging, which selected closely to the date of surgery. Figure 1 illustrates a patient with PMA under cross-sectional magnetic resonance imaging and the location of measurement. The primary outcomes were postoperative 30-d, 90-d, and overall mortality from the date of surgery. Secondary outcomes were adverse events 30-d, 90-d, and overall morbidity, defined as any of the following, surgical site infection (Badhiwala JH et al., 2021)
16
surgical site dehiscence (SSD), pulmonary embolism (PE), deep vein thrombosis (DVT), pneumonia, anemia, Methodology for psoas measurements.
Quantitative Variables and Statistical Methods
Demographic Data.

The bold use when P<0.05
The mean survival time at overall time was computed using Kaplan–Meier estimates for all patients in 3 tertiles. The log-rank test was used to assess differences among the 3 Kaplan–Meier curves. We utilized a Cox regression analysis to calculate an estimate of the HRs of overall mortality. The variables with the P-value of less than .2 in univariable analysis were included into the multivariable analysis. We also used the backward elimination in the variable selection. Candidate variables were removed step by step until its P-value below a stopping rule; P-value of .05.
We also assessed the measurement reproducibility by using intraclass correlation coefficient (ICC) and also compare the correlation between measuring PMA under MRI and CT. Reliability was also determine by calculating Cronbach’s alpha. The internal consistency estimates of a >.70 were considered acceptable for group comparisons (Koo TK et al., 2016). 17
All statistical analysis was performed by using StataCorp. Version 17. College Station, TX: StataCorp LLC; 2021 and PASW Statistics for Windows, Version 18.0. Chicago: SPSS Inc; 2009
Results
Participants and Descriptive Data
A total of 655 patients were included in the study, with 535 being excluded due to the lack of an MR image. This left a final sample of 120 patients. Demographic data was collected for these participants, including gender (66 males, 55%), age (mean age of 62.63 + 10.36 for T1, 56.93 + 11.74 for T2, and 58.23 + 13.24 for T3, P = .08), ASA score (ASA 2 was predominant in each tertile, with 26 [31.70%] in T1, 34 [41.50%] in T2, and 22 [26.80%] in T3), underlying diseases (the most common being hypertension, present in 19 [33.9%], 17 [30.4%], and 20 [35.7%] for T1, T2, and T3, respectively, P = .79, followed by diabetic mellitus, present in 11 [45.8%], 2 [12.5%], and 10 [41.7%] for T1, T2, and T3, respectively), primary cancer (the most common being lung cancer, present in 11 [44%], 6 [24%], and 8 [32%] for T1, T2, and T3, respectively, in both genders; male genitourinary tract cancers, including prostate and bladder, were the second most common, present in 11 [45.8%], 6 [25%], and 7 [29.2%] for T1, T2, and T3, respectively), preoperative neurological status (Frankel C was most prevalent in all tertiles, P = .81), and preoperative scoring systems (PSS) including SORG, Nomogram, Modified-Bauer score, and NESMS. The level of metastasis, surgical spinal level, and postoperative medical and surgical complications were also recorded. The demographic details are shown in Table 1.
90-d Mortality
90-d Mortality.

365-d Mortality
365-d Mortality.

Overall Mortality
The Kaplan–Meier survival analysis of patients in the 3 different tertiles was presented in Figure 2, showing that patients in T3 (Large PMA) had a better survival rate, while patients in T1 had worse survival compared to T2 and T3. The mean survival time was 7 months for T1, 9 months for T2, and 10 months for T3. However, there was no significant difference between tertiles (log-rank test P = .56). Kaplan–Meier curve for overall survival in different tertiles. The log-rank test was not significant with a P-value of .56 but the mean survival rate in each tertiles has a tendency of high mortality rate in low psoas tertile. Blue lines indicate T1 (low PMA), Red line indicate T2 (medium PMA), and green lines indicate T3 (large PMA).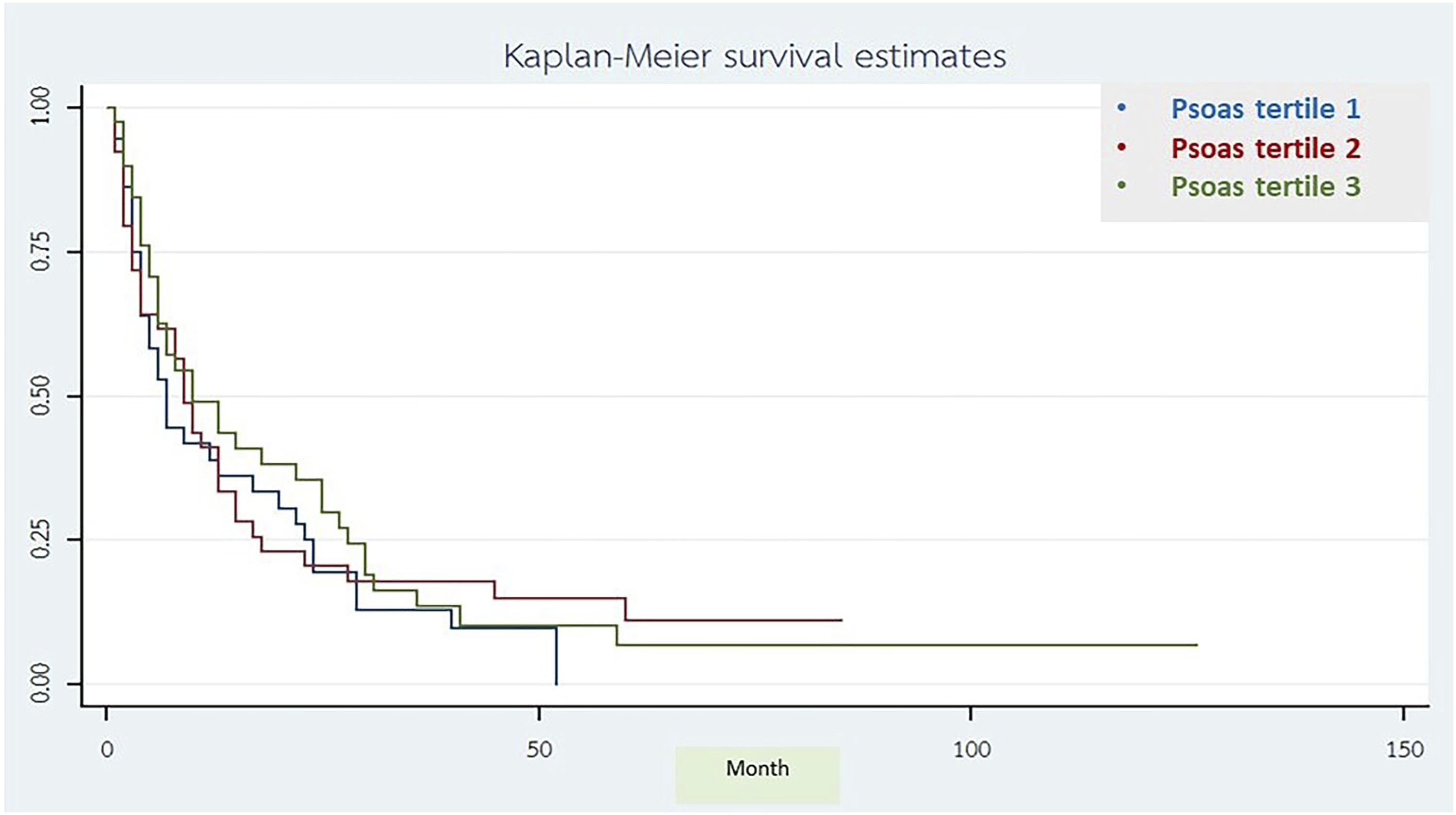
Measurement Reproducibility
The Cronbach’s alpha was acceptable for our study, the ICC for correlation between measurement under CT and MRI was .76 (95% CI, .66–.84), the ICC for intra-observer reliability was .986 (95% CI, .98–.99) and the ICC for inter-observer reliability was .95 (95% CI, .908–.973) (Supplementary table)
Univariable and Multivariable Cox Regression
Univariable and Multivariable Cox Regression.

aPsoas muscle area which classify as tertile was not include in the multivariable cox regression.

Forrest plot of adjust hazard ratio.
The PMA T1 and T2, PMA T3 as a reference, showed adjusted HR 1.21 (95% CI .74–2.08; P = .49) and 1.38 (95% CI .83–2.32; P = .02) respectively. The PMA T2 had a significantly high mortality rate when compared to PMA T3 by adjusted HR. Considering PMA as a continuous variable, every 1 mm2 increment of PMA resulted in the increase survivorship of 1% (HR .99 with 95% CI .99–1)
Secondary Outcome
Postoperative Complication.

Discussion
According to previous studies, sarcopenia is the one of the predictors of the mortality following spinal metastatic surgery, the PMA has become a surrogate of sarcopenia. Most of studies, the PMA was identified by cross-sectional view of computer tomography at L3 or L4 pedicle level. Bourassa-Moreau E. et al studied the sarcopenia for prediction the early mortality and adverse events in emergent spinal metastatic surgery, the result showed the sarcopenia predicted 3-month mortality, independent of primary tumor. 17 Dohzono S. et al studied showed the lowest percentage quartile (0-25%) of the psoas muscle mass was associated with poor overall survival rate in cervical spine metastatic surgery (HR 1.93, 95% confident interval 1.12-3.32; P = .0017). 18 Hu MH. et al. studied, PMA is the prognosticator for 90-day survival and improves the discriminatory ability of earlier-proposed PSS in Asian populations (c-index, .74; 95% CI .67-.82 vs c-index, .74; 95% CI .66-.81). 15 Pielkenrood B.J. et al studied a body fat distribution and sarcopenia on the overall survival in spinal metastatic patients who received radiotherapy, showed the muscle density was statistically significant associated with survival after 90 and 365 days, but body fat distribution was not significantly associated with overall survival. 19
MRI is generally considered to be a more sensitive and specific modality for evaluating soft tissue, such as the muscles in the abdominal and pelvic region. MRI can also provide detailed images of the spine and pelvis, which may be important in some cases where those information is being used to guide surgical planning. Additionally, MRI does not expose the patient to ionizing radiation, which may be a consideration in certain clinical situations. In some circumstances, patients require urgent spinal surgery, such as decompression of cord compression. The selected imaging modality should be MRI, as it provides more information for surgical planning.
This study investigated the relation between the PMA under magnetic resonance and overall mortality rate. From our knowledge, this is the first study that used magnetic resonance imaging to evaluate the PMA in spinal metastatic patients who underwent the palliative spinal surgery. The PMA in T1 and T2 had a tendency of high 90-d mortality rate when compared to PMA in T3, the multivariable regressions showed that patients with low PMA had 38% higher mortality rate than large PMA in overall time. Kaplan–Meier graph showed the relation between psoas tertiles and time of death; PMA in T3 (large PMA) had a better probability of mortality rate than PMA in T1 and 2 (low PMA). According to the ICC was .76 (95% CI, .66–.84), the correlation between PMA under magnetic resonance imaging and computer tomography has a good reliability, but our study has a very low rate of the populations with computer tomography of lumbar spine. The preoperative characteristic is one of the prognostic factors which has a probability to predict the mortality rate; multivariable regression for the comorbidity showed 59% higher mortality rate than non-comorbidity in populations. Although, our study has not statistically difference in psoas tertiles at 90-d, 1-year, and overall mortality but there was a tendency of high mortality in low psoas group (PMA in T1 and T2), especially in 90-d mortality. Most of spinal metastatic patients have been undergone the magnetic resonance of screening whole spine for diagnosis and treatment, so this the benefit to evaluate the PMA in this imaging.
Limitations
There are several limitations in this study. First, this study limited by the retrospective review, which can potentially create a hidden bias due to the possibility of incomplete or inaccurate data. The population is heterogeneous in term of clinical decision-making and postoperative therapy due to the improvement of modality and treatment between 2009 and 2020 with a relatively small number of patients. In demographic data, the comparison between the psoas tertiles turned out of be insignificant but most population have the thoracic and lumbar spinal metastatic surgery, there was low cervical spinal metastatic surgery which may have a higher mortality rate than other site of spine surgery.
Conclusion
The MRI-based PMA tend to predict the 90-d mortality rate and overall mortality rate in spinal metastasis patients who undergone the spinal surgery. The PMA could be one of prognostic factors which can be used in decision-making, cooperated with other prognostic factors, in treatment of spinal metastatic patients. However, the future large-sized, prospective, and preferably multicenter studies are required to confirm or deny our results.
Supplemental Material
Supplemental Material - The Magnetic Resonance Imaging of the Psoas Muscle Area as the Prognostic Factor for Survival and Adverse Events in Spinal Metastasis Surgery
Supplemental Material for The Magnetic Resonance Imaging of the Psoas Muscle Area as the Prognostic Factor for Survival and Adverse Events in Spinal Metastasis Surgery by Kitidate Boonchai, Borriwat Santipas, Sirichai Wilartratsami, Monchai Ruangchainikom, Ekkapoj Korwutthikulrangsri, Pawin Akkarawanit, and Panya Luksanapruksa in Global Spine Journal.
Footnotes
Acknowledgments
The authors gratefully acknowledge Miss Sara Rawdeng of the Division of Research, Department of Orthopaedic Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University for assistance with data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.