
Abstract
Study Design:
Retrospective cohort study.
Objectives:
To evaluate age as an independent predictive factor for perioperative morbidity and mortality in patients undergoing surgical decompression for metastatic cervical and thoracic spinal tumors using the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database from 2011 to 2014.
Methods:
We identified 1673 adult patients undergoing excisional laminectomy of cervical and thoracic extradural tumors. Patients were stratified into quartiles based on age, with Q1 including patients aged 18 to 49 years, Q2 including patients aged 50 to 60 years, Q3 including patients aged 61 to 69 years, and Q4 including patients ≥70 years. Univariate and multivariate regression analyses were performed to examine the association between age and 30-day perioperative morbidity and mortality.
Results:
Age was an independent risk factor for 30-day venous thromboembolism (VTE) and reoperation. Patients in Q3 for age had nearly a 4 times increased risk of VTE than patients in Q1 (odds ratio [OR] 3.97; 95% CI 1.91-8.25; P < .001). However, there was no significant difference in VTE between patients in Q4 and Q1 (P = .069). Patients in Q2 (OR 1.99; 95% CI 1.06-3.74; P = .032) and Q4 (OR 2.18; 95% CI 1.06-4.52; P = .036) for age had a 2 times increased risk of reoperation compared with patients in Q1.
Conclusions:
Age was an independent predictive factor for perioperative VTE and reoperation, but there was no clear age-dependent relationship between increasing age and the risk of these perioperative complications.
Keywords
Introduction
Spinal tumors are an important cause of morbidity and mortality in the Western world, with an incidence of 0.62 cases per 100 000 individuals in the United States. 1,2 Spinal tumors can be of primary type or metastatic in nature, the latter making up the majority of spinal tumors and found in up to 70% of cancer patients. 3,4 The tumors can be classified based on histology or anatomical location with respect to the dura, including extradural, intradural extramedullary, or intramedullary. Extradural tumors are predominantly metastatic in origin, and can cause neurological symptoms via extradural epidural cord compression. 5 Lesions of the cervical and thoracic spine are mostly due to the result of lung or breast cancer, while lumbosacral involvement is usually due to prostate, colon, or pelvic involvement. 6
In patients with neurological symptoms resulting from compression, surgery can be performed to help improve ambulatory function, decrease pain, and in some cases, improve survival. 7 –11 Surgery for spinal tumors are often extensive procedures and have higher rates of perioperative complications compared with elective spinal operations; such complications can worsen morbidity and mortality and can increase associated costs. 3,12 –16 Therefore, it is important to understand the incidence and risk factors that contribute to perioperative complications in this population. Postoperative complications have been suggested to vary according to multiple factors, including patient comorbidities, tumor location, tumor size and extent, as well as hospital- and surgeon-related factors. 7 –11,17 –21
Elderly patients are becoming an increasingly prevalent demographic in the Western world. 22 However, the influence of elderly age on outcomes following surgery for spinal tumors is currently not well established. 23,24 In general, there has been lack of literature assessing the incidence and predictors of outcomes and complications following extradural spinal tumor surgery. Prior studies have been predominantly limited to single institution, retrospective studies, which are limited in the generalizability of their conclusions given their selection bias. 17 –21
The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database has been queried extensively in the past for outcomes following elective spinal surgery, including fusions for degenerative spinal diseases and spinal deformity. 25 –34 Using the ACS-NSQIP database, this study aims to determine the role of age as an independent risk factor for perioperative complications following excisional laminectomy for extradural cervical and thoracic spinal tumors. By identifying perioperative complications that elderly patients are at risk, strategies can be developed and implemented to improve appropriate patient selection for surgery as well as direct postoperative management efforts to reduce complication rates.
Methods
This study received an exemption from the institutional review board at our institution.
Data Source
This was a retrospective study of prospectively collected data in the 2010-2014 ACS-NSQIP database. ACS-NSQIP is a large national database with risk-adjusted 30-day postoperative morbidity and mortality outcomes. More than 500 hospitals that vary in size, socioeconomic location and academic affiliation contributed data to the 2010-2014 ACS-NSQIP database. 35 ACS-NSQIP data is collected prospectively by dedicated clinical abstractors at each institution on more than 150 demographic, preoperative, intraoperative, and 30-day postoperative variables. 35
Inclusion and Exclusion Criteria
Adult patients (≥18 years) undergoing laminectomy and excision of cervical (Current Procedural Terminology [CPT]: 63 275) and thoracic extradural tumors (CPT: 63 276) were identified. Cases with missing preoperative data, emergency cases, patients with a wound class of 2, 3, or 4, an open wound on their body, current sepsis, current pneumonia, prior surgeries within 30 days, cases requiring cardiopulmonary resuscitation (CPR) prior to surgery, were excluded in order to reduce the risk of confounding variables. Patients were stratified into quartiles based on age. Quartile 1 (Q1) included patients aged 18 to 49 years, quartile 2 (Q2) included patients aged 50 to 60 years, quartile 3 (Q3) included patients aged 61 to 69 years, and quartile 4 (Q4) included patients aged ≥70 years.
Variable Definitions
Patient demographic variables included sex and race (white, black, Hispanic and other). Other race included American Indian, Alaska Native, Asian, Native Hawaiian, Pacific Islander, or Unknown/Not Reported. Preoperative variables included obesity (≥30 kg/m2), diabetes (non–insulin-dependent diabetes mellitus or insulin-dependent diabetes mellitus), current smoking (within 1 year of surgery), dyspnea (≤30 days prior to surgery), functional status prior to surgery (independent or partially/totally dependent ≤30 days prior to surgery), pulmonary comorbidity (ventilator dependent ≤48 hours prior to surgery or history of chronic obstructive pulmonary disease ≤30 days prior to surgery), cardiac comorbidity (use of hypertensive medication or history of chronic heart failure ≤30 days prior to surgery), renal comorbidity (acute renal failure ≤24 hours prior to surgery or dialysis treatment ≤2 weeks prior to surgery), steroid use for chronic condition (≤30 days prior to surgery), ≥10% loss of body weight (in the past 6 months), bleeding disorder (chronic, active condition), preoperative transfusion of ≥1 unit of whole/packed red blood cells (RBCs) (≤72 hours prior to surgery), concurrent posterior fusion, and preoperative oncologic treatment (chemotherapy, radiotherapy, or combined chemotherapy and radiotherapy ≤30 days prior to surgery).
Thirty-day perioperative outcome variables included mortality, wound complication (superficial or deep surgical site infection, organ space infection or wound dehiscence), pulmonary complication (pneumonia, unplanned reintubation, or duration of ventilator-assisted respiration ≥48 hours), venous thromboembolism (VTE; pulmonary embolism or deep vein thrombosis), renal complication (progressive renal insufficiency or acute renal failure), urinary tract infection (UTI), cardiac complication (cardiac arrest requiring CPR or myocardial infarction), intra/postoperative RBC transfusion, prolonged operative time ≥95th percentile (ie, ≥477 minutes), prolonged length of stay (LOS) ≥75th percentile (ie, ≥8 days), reoperation (related to initial procedure), and unplanned readmission (related to initial procedure). Nonelective surgery unrelated to the procedure includes those where the patient was transferred from another acute care hospital to the hospital for surgery, transferred from an emergency, clinic, undergoing emergent/urgent surgical case, or admitted to the hospital on the day(s) prior to a scheduled procedure for any reason. ACS-NSQIP provides further information on variable characteristics.
Statistical Analysis
Univariate analysis was performed on patient demographic, preoperative, intraoperative, and postoperative variables using Pearson’s chi-square test. Fischer’s exact test was used where appropriate. Multivariable logistic regression models were then employed to identify the effect of age on 30-day perioperative outcomes, while adjusting for patient demographics, comorbidities, and preoperative characteristics. The C-statistic, which is the area under the receiver operating characteristic (ROC) curve, was also retrieved from the multivariate logistic regression analysis to evaluate the accuracy of this model. The ROC curve is a graph of the fall-out rate (1 − specificity) against the sensitivity (true-positive rate). The area under this curve measures the ability of the model to correctly classify patients who experienced a complication and those who did not. Statistical significance was set at the P = .05 level. SAS Studio Version 3.4 (SAS Institute Inc, Cary, NC, USA) was used for all statistical analysis.
Results
Study Population
A total of 1673 patients met the inclusion criteria for the study. Age stratification of this cohort based on quartiles resulted in 430 patients in Q1 (25.7%), 438 patients in Q2 (26.1%), 416 patients in Q3 (24.9%), and 388 patients in Q4 (23.2%). Baseline patient demographics and characteristics among the 4 quartiles are outlined in Table 1. There were significant differences among the age quartiles in terms of sex, race, obesity, diabetes, dyspnea, functional status, pulmonary comorbidity, cardiac comorbidity, renal comorbidity, American Society of Anesthesiologists (ASA) classification, smoking, recent weight loss, bleeding disorder, nonelective surgery, and concurrent posterior fusion. There were no significant differences among the age quartiles in terms of preoperative steroid use (P = .207), blood transfusion (P = .835), chemotherapy (P = .167), radiotherapy (P = .329), and chemoradiotherapy (P = .083).
Baseline Patient Demographics, Preoperative Characteristics, and Intraoperative Variables.
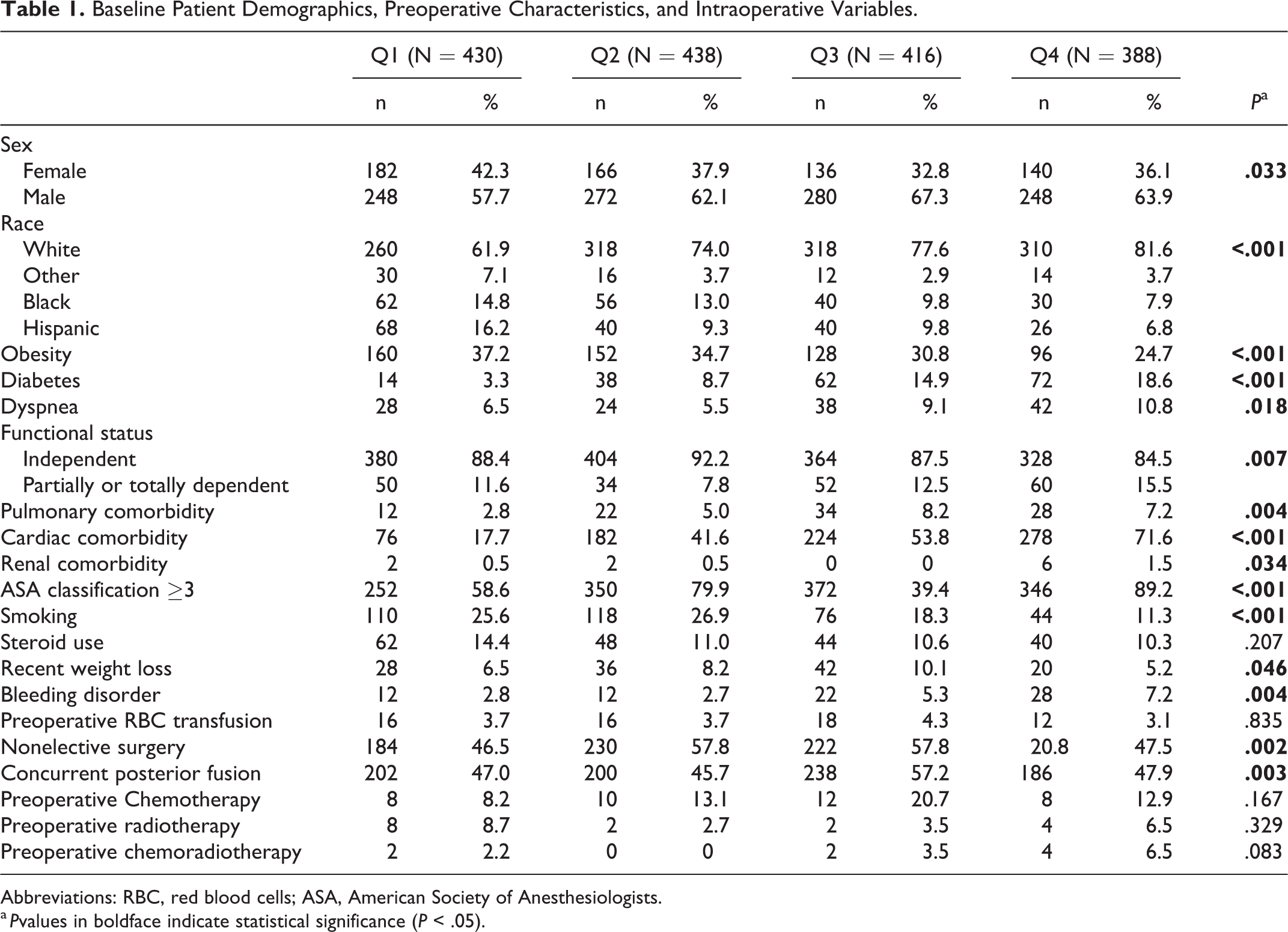
Abbreviations: RBC, red blood cells; ASA, American Society of Anesthesiologists.
a Pvalues in boldface indicate statistical significance (P < .05).
Unadjusted Analysis
The results of the unadjusted univariate analysis are summarized in Table 2. There was no significant difference in 30-day mortality rate among age quartiles (P = .19). There were significant differences among age quartiles in terms of VTE, renal complication, and reoperation. The highest rate of VTE was seen in patients aged 60 to 69 years, followed closely by patients aged 50 to 60 years and patients ≥70 years (Q1 = 2.3%, Q2 = 5.0%, Q3 = 8.2%, Q4 = 4.6%; P < .001). Patients aged ≥70 years had the highest rate of perioperative renal complications, followed closed by patients aged 50 to 60 years (Q1 = 0%, Q2 = 1.4%, Q3 = 0%, Q4 = 1.5%; P = .006). Patients aged 50 to 60 years had the highest incidence of reoperation, whereas patients aged 61 to 69 years had the lowest rate of reoperation (Q1 = 4.6%, Q2 = 7.0%, Q3 = 2.6%, Q4 = 5.5%, P = .035). There were no significant differences among the age quartiles in terms of wound complications (P = .417), pulmonary complications (P = .267), urinary tract infections (P = .090), cardiac complications (P = .129), intra- or postoperative RBC transfusions (P = .073), prolonged length of stay ≥8 days (P = .309), and unplanned readmission (P = .217).
Univariate Analysis of 30-Day Perioperative Outcomes.
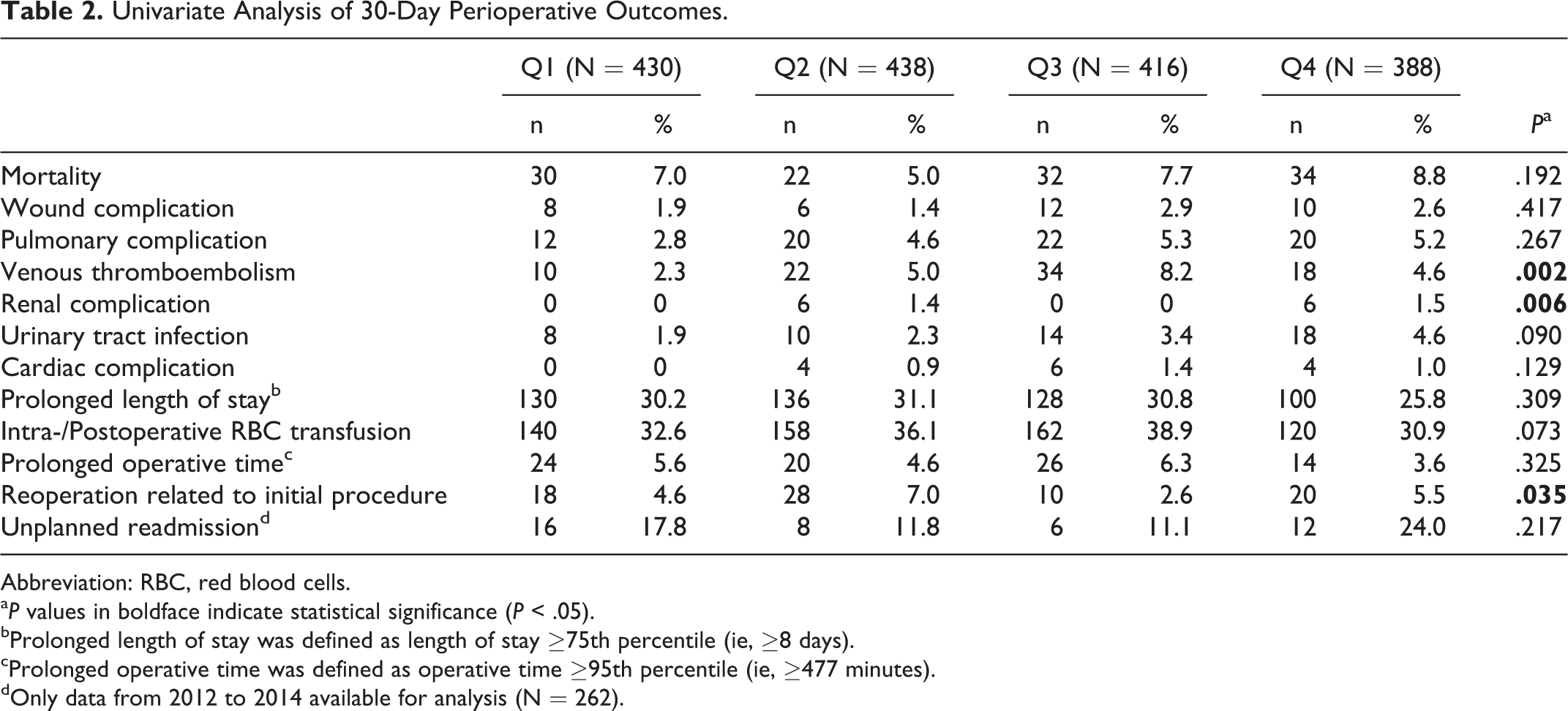
Abbreviation: RBC, red blood cells.
aP values in boldface indicate statistical significance (P < .05).
bProlonged length of stay was defined as length of stay ≥75th percentile (ie, ≥8 days).
cProlonged operative time was defined as operative time ≥95th percentile (ie, ≥477 minutes).
dOnly data from 2012 to 2014 available for analysis (N = 262).
Multivariate Analysis
The results of the multivariate logistic regression analysis are outlined in Table 3. With the youngest quartile as reference, patients aged 50 to 60 years (odds ratio [OR] 2.56, 95% CI 1.18-5.54, P = .017) and patients aged 61 to 69 years (OR 3.97, 95% CI 1.91-8.25, P < .001) had increased odds of perioperative VTE. Patients aged 50 to 60 years (OR 1.99, 95% CI 1.06-3.74, P = .032) and patients aged ≥70 years (OR 2.18, 95% CI 1.06-4.52, P = .036) had increased odds of 30-day reoperation. Patients aged 61 to 69 years, however, were not at increased risk of reoperation.
Multivariate Analysis of Age as an Independent Risk Factor for 30-Day Perioperative Outcomes.a
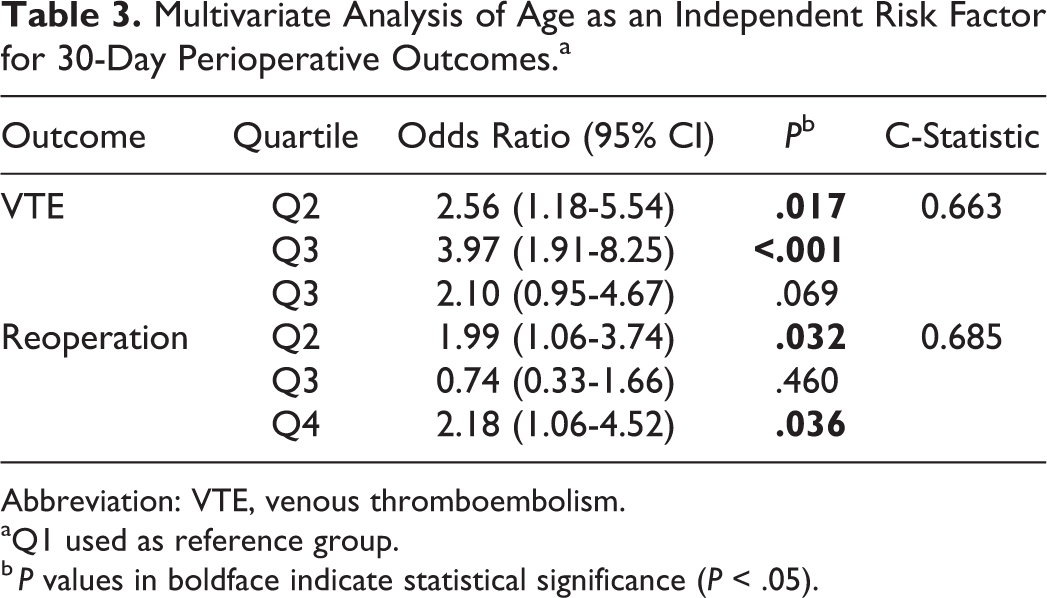
Abbreviation: VTE, venous thromboembolism.
aQ1 used as reference group.
b P values in boldface indicate statistical significance (P < .05).
Discussion
Elderly patients are an increasing demographic in the Western world, and the spine surgery population is no exception. 22 –24 Compared with younger patients, older patients tend to have poorer physiological reserve, increased complications following procedures and restricted access to resources. 36,37 There is also an increase in oncological conditions in the elderly population, with a significant proportion associated with spinal metastasis. Given that the most common location of spinal metastasis are extradural spinal tumors, we sought to investigate age as a risk factor for the perioperative complications following surgical treatment of extradural cervical and thoracic spinal tumors. This information can be used by health care teams to develop and implement strategies to improve surgical patient selection, risk stratification, and safety.
Our analysis of 1673 patients in the ACS-NSQIP database identified age as an independent risk factor for VTE and reoperation within 30 days of surgery. On multivariate analysis, patients aged 61 to 69 years old had the highest odds of VTE, whereas patients aged 50 to 60 years and patients aged ≥70 years old were at increased risk for reoperation. The success of quality improvement initiatives based on ACS-NSQIP data has been validated by decreased mortality rates in the Veterans Affairs (VA) system, as well as decreased surgical site infection rates in the private sector. 38 –40
Surgery for spinal tumors and metastasis is more likely associated with complications compared to elective spinal surgery for degenerative disease. In particular, cancer is a known risk factor for venous thromboembolism given the patient prothrombotic states. 41 This is particularly relevant for extradural cervical and thoracic tumors, the majority of which are metastatic tumors originating from primary lung or breast tumors. In our study, elderly patients aged 50 to 69 years were almost twice as likely to experience VTE following surgery for extradural cervical or thoracic spinal tumors. The oldest age quartile (ie, age ≥70 years) did not have a statistically significant increased risk of VTE, but the OR trended toward significance. The overall VTE rate was 5.0%, but increased to 8.2% for patients aged 61 to 69 years. One contributing factor may be that elderly patients require a longer LOS given their poorer physiological reserve and recovery after surgery. Prolonged hospitalization with likely prolonged immobilization can further increase their risk of VTE due to increased venous stasis.
A similar VTE rate of 4.5% was reported in an analysis of all types of spinal tumors, including both extradural and intradural subtypes, with this complication having the largest contribution to adverse events in this study. 42 Kalakoti et al 43 analyzed the National Inpatient Sample for risk factors of unfavorable outcomes following surgery for benign intradural spinal tumors. They reported a lower rate of thromboembolism (ie, 1.4%) compared with the current study; this may be attributed to the fact that extradural tumors tend to be metastatic in origin, and oncological state is associated with increased prothrombotic state and coagulopathy. 43 An association between patient age and VTE is not limited to only spinal tumor surgery. Similar patterns have been reported in other types of surgery. Hamel et al 44 conducted a prospective cohort study of 26 648 patients and found that patients ≥80 years had a significantly higher incidence of deep vein thrombosis compared to their younger counterparts. Even for smaller, less traumatic spinal procedures such as anterior cervical discectomy and fusion (ACDF), Buerba et al 45 identified patients aged 65 to 74 years as having a 4.14 times greater odds of VTE compared with younger patients. As such, the higher risk of VTE associated with increasing age may not be specific to extradural spinal tumors, but may be generalized across all types of spinal surgery.
Our analysis demonstrated an overall 30-day reoperation rate of 4.5% in patients undergoing excisional laminectomy for cervical and thoracic extradural tumors. Elderly patients ≥70 years old had greater than 2 times the odds of reoperation compared with patients ≤49 years old. Older patients are likely to have poorer physiological reserve to withstand the stresses and complications of surgery, and this may translate into higher rates of reoperation. The reoperation rate in this study is similar to that reported by Karhade et al. 42 In their study, the unplanned reoperation rate was 5.3% across all types of cervical, thoracic, lumbar, and sacral spinal tumors. Their analysis demonstrated that preoperative steroid use and ASA class 4 or 5 were significantly associated with reoperation, but did not assess the influence of age on reoperation. Quraishi et al 46 performed a retrospective review of 289 patients treated over an 8-year period for spinal metastasis and found a higher reoperation rate of 10.7%. However, they found no significant difference in the age of patients requiring revision surgery versus patients not requiring revision surgery.
When comparing reoperation rates among different types of spinal surgery, studies have found similar 30-day reoperation rates for adult deformity spinal surgery (5%), 47 but lower rates for ACDF (1.2%) and cervical disc arthroplasty (0.4%). 48 Age has been shown to be predictive of a higher risk of reoperation following ACDF. 48 Unplanned reoperation is taxing on a patient’s health and also drives increasing health care costs. Under the Affordable Care Act, any cost associated with patient readmission up to 30 days following discharge becomes the financial burden of the hospital. Considering the overall frailty of many elderly patients with extradural spinal tumors, care should be taken to prevent premature discharge of patients following any hospital stay.
In this study, the overall perioperative mortality rate was 7.6%, but age was not a predictive factor for mortality. This finding is in contrast to existing literature that has demonstrated higher mortality rates in older patients undergoing spinal surgery. 26,27 Additionally, literature from multiple surgical subspecialties has demonstrated higher mortality rates in older cancer patients undergoing general, cardiac, oncological, vascular, and orthopedic surgery. 49 –51 One possible explanation for our results is that we only assessed 30-day postoperative mortality, which may not have been a long enough time period to fully capture the effect of age on postoperative mortality. Outcomes following surgery for extradural spinal tumors are not well reported in the literature, and thus, our finding warrants further investigation in future studies.
Limitations
The present study is limited by several constraints. Firstly, the ACS-NSQIP database classified cases based on CPT codes. CPT codes also do not give information on primary tumor location and histology, which are significant prognostic predictors. 52 –54 A patient undergoing excisional laminectomy for an isolated, slow growing vertebral metastasis has a much different disease burden than one with an aggressive, widely disseminated cancer, representing a markedly different type of surgical candidate. The number of vertebral and visceral metastases is an important prognostic indicator that is not accounted for in our data set. 55,56
Second, the ACS-NSQIP database accumulates data that is biased toward predominantly academic centers. As such, this cross-section may not be reflective of surgical practices for surgery for extradural spinal tumors nationwide. Third, only 30-day perioperative outcomes are collected in this database; therefore, our results may reflect long-term outcomes in this population. Last, other relevant parameters including neurological outcomes, functional outcomes, intraoperative complications, tumor characteristics such as size and histology are not collected in this database. Despite these limitations, the ACS-NSQIP database provides a large sample size and allows analysis of risk factors for perioperative complications following extradural spinal tumor surgery, which has previously not been well reported in the literature.
Conclusions
This is the first nation-wide study to evaluate age as a risk factor for 30-day perioperative outcomes following surgical decompression of extradural cervical and thoracic spinal tumors. Age was an independent predictive factor for perioperative VTE and reoperation, although there was no clear age-dependent effect on the risk of these complications. In contrast to previous studies in the literature, age was not a predictive factor for 30-day perioperative mortality.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.