
Abstract
Study Design
International survey.
Objectives
C5 palsy (C5P) is a neurological complication affecting 5-10% of patients after cervical decompression surgery. Most cases improve with conservative treatment; however, nearly 20% of patients may be left with residual deficits. Guidelines are lacking on C5P management and timing of surgical intervention. Therefore, we sought to survey peripheral nerve surgeons on their management of C5P.
Methods
An online survey was distributed centered around a patient with C5P after posterior cervical decompression and fusion. Questions included surgeon demographics, diagnostic modalities, and timing and choice of operation. Responses were summarized and the chi-squared and Kruskal-Wallis H tests were used to examine differences across specialties.
Results
A total of 154 surgeons responded to the survey, of which 59 (38%) indicated that they manage C5P cases. Average time prior to operating was 4.5 ± 2.2 months for complete injuries and 6.6 ± 3.2 months for partial injuries, with neurosurgeons significantly more likely to wait longer periods for complete (P = .01) and partial injuries (P = .03). Foraminotomies were selected by 19% of surgeons, while 92% selected nerve transfers. Transfer of the ulnar nerve to the musculocutaneous nerve was the most common choice (81%), followed by transfer of the radial nerve to the axillary nerve (58%).
Conclusion
Consensus exists among peripheral nerve surgeons on the use of nerve transfers for surgical treatment in cases with severe motor weakness failing to improve. Most surgeons advocate for early intervention in complete injuries. Disagreement concerns the type of nerve transfer employed, timing of surgery, and efficacy of foraminotomy.
Introduction
Cervical spine decompression is associated with the development of postoperative C5 palsy (C5P) in approximately 5-10% of cases.1,2 Symptoms can include new onset weakness of the deltoid or biceps brachii muscle that can occur alongside shoulder pain and sensory deficits, usually within a week after surgery.3,4 The diagnosis is primarily a clinical diagnosis, with electrophysiological and imaging studies aiding workup. 5 Although most patients can improve over several months with conservative treatment, nearly 20% are left with residual weakness.5-7
The pathophysiology of C5P is not completely understood and likely reflects several heterogeneous etiologies, including iatrogenic injury from instrumentation, nerve root traction injury from posterior shifting of the cord after decompression, spinal cord ischemia, and reperfusion injury.3,8,9 C5 Palsy has been reported most commonly following posterior procedures but has also been noted after anterior surgery, and it can present in a delayed fashion, complicating theories about causes.2,6 Given the uncertainty about pathophysiology, the optimal treatment regimen and role of surgical intervention remains unclear. 10 Nerve transfers and foraminotomies have been described, but surgeons considering operative intervention must balance the potential for spontaneous recovery over time with the reduced improvements in functional outcomes after delayed treatment. 1 Patients with severe motor weakness are least likely to recover with conservative treatment alone. 11
Given the lack of consensus in the literature over optimal management regimens, we conducted an international survey of peripheral nerve surgeons to determine treatment of C5P following cervical spine surgery in patients with severe motor weakness. Our objectives were to (a) determine the percentage of peripheral nerve surgeons treating this pathology; (b) understand management strategies for these injuries, indications and timing of treatment, and specific operative approaches used; and (c) analyze the extent of disagreement and variability in management of C5P.
Materials and Methods
Institutional Review Board approval (IRB00209287) was obtained by the [blinded for review] Institutional Review Board. The IRB deemed the present study as not meeting the definitions of human subjects research and informed consent was not required. The RedCAP Database (Research Electronic Data Capture, Nashville, TN) was used to generate, distribute, and collect responses from an online survey to expert peripheral nerve surgeons in 2020. Surgeons from the Sunderland Society for International Peripheral Nerve Study and international collaborative peripheral nerve researchers were invited to participate. The study was exempt from informed consent requirements as it posed negligible risk to survey participants. Questions included surgeon demographics, diagnostic modalities for C5P, timing of operation, and choice of surgical intervention. After the demographic questions, the survey focused on the case described below: A 55-year-old man with no past medical history undergoes a C3-6 posterior cervical decompression and fusion for compressive spondylotic myelopathy and mild 4+ intrinsic hand weakness. On postoperative day 2, he awakens with deltoid and biceps weakness 2/5. Imaging is unremarkable with post-surgical changes and well-decompressed cervical cord.
Data were analyzed using STATA version 16 (College Station, TX). Descriptive statistics including counts and proportions were used to summarize survey responses, while mean ± standard deviation were used to summarize the timing of surgery. The chi-squared and Fisher exact tests were used to examine associations between surgical specialty and survey responses for categorical and dichotomous variables, while the Kruskal-Wallis H test was used to examine differences in timing of operation.
Results
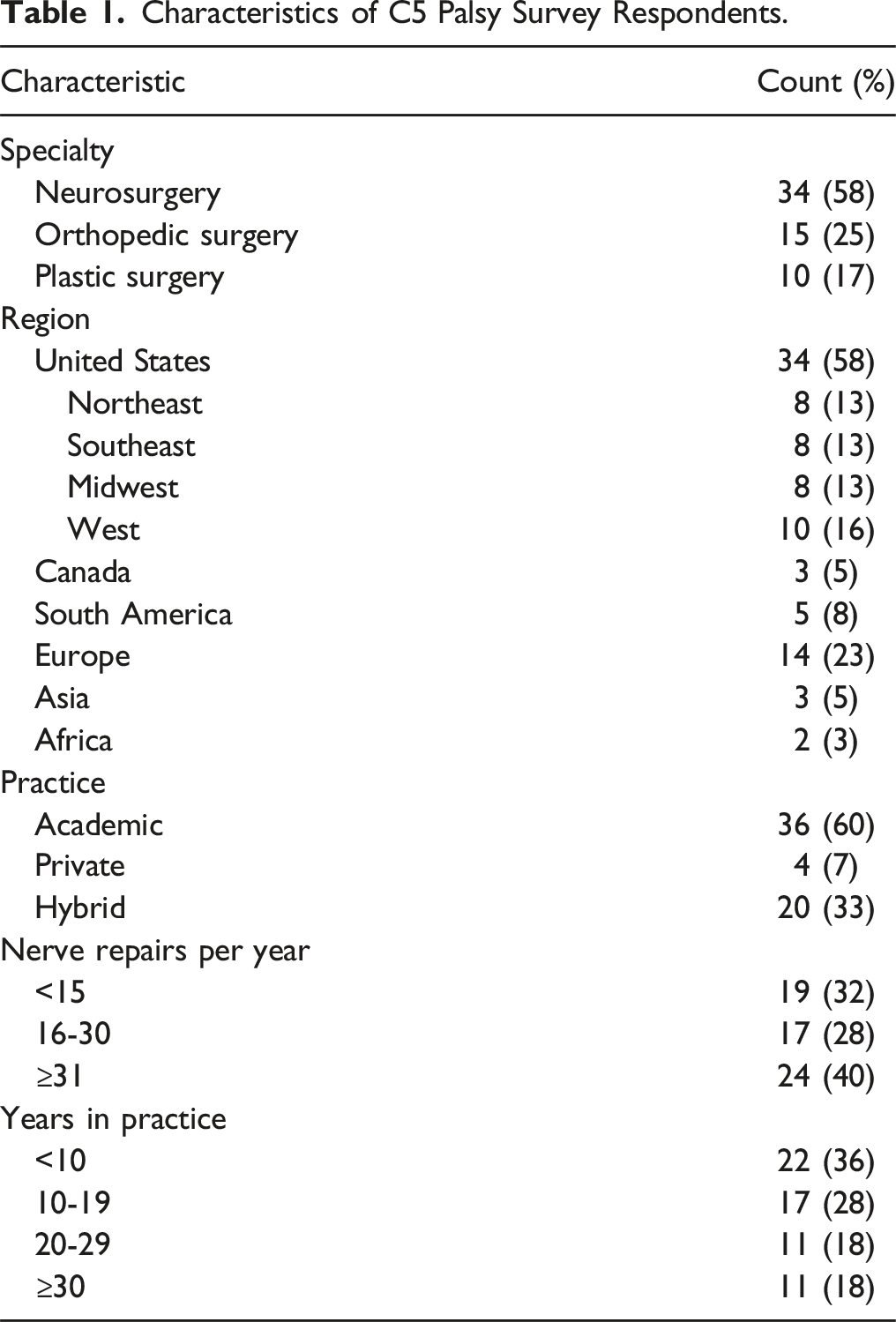
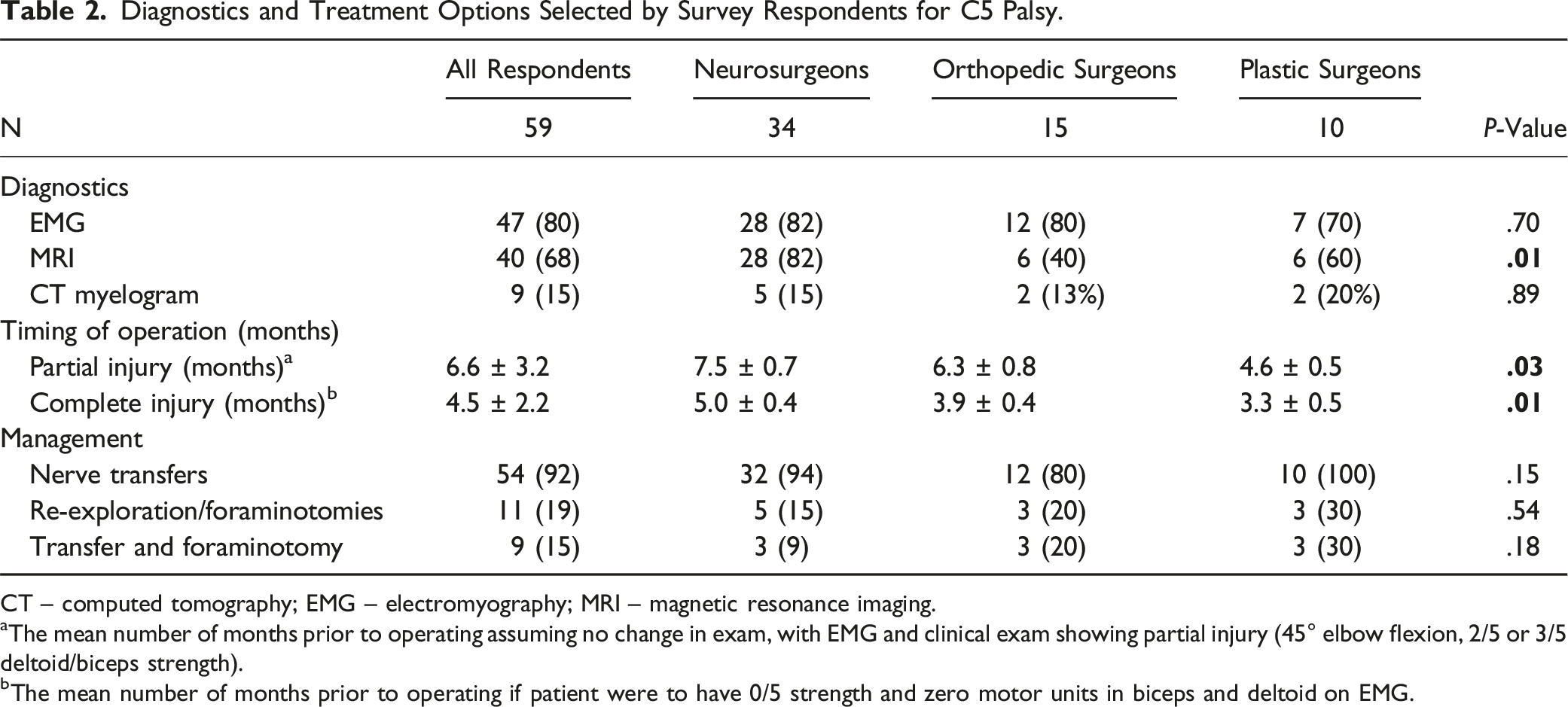
The survey was distributed to 294 peripheral nerve surgeons. Out of 154 respondents, 59 (38%) indicated that they manage cases of C5P, including 34 (58%) neurosurgeons, 15 (25%) orthopedic surgeons, and 10 (17%) plastic surgeons (Figure 1). Most respondents practice in North America (63), followed by Europe (23%), and the majority (60%) were employed in academic practices (Table 1). Twenty-four respondents (40%) indicated performing over 30 nerve repairs per year. The most common diagnostic modality for the C5P case was electromyography (EMG) (80%), followed by Magnetic Resonance Imaging (MRI) (68%) and Computed Tomography myelography (15%) (Table 2). The use of MRI differed significantly by surgical specialty, with 82% of neurosurgeons using MRI compared to 60% of plastic surgeons and 40% of orthopedic surgeons (P = .01). Flowchart illustrating distribution of survey and responses. Characteristics of C5 Palsy Survey Respondents. Diagnostics and Treatment Options Selected by Survey Respondents for C5 Palsy. CT – computed tomography; EMG – electromyography; MRI – magnetic resonance imaging. aThe mean number of months prior to operating assuming no change in exam, with EMG and clinical exam showing partial injury (45° elbow flexion, 2/5 or 3/5 deltoid/biceps strength). bThe mean number of months prior to operating if patient were to have 0/5 strength and zero motor units in biceps and deltoid on EMG.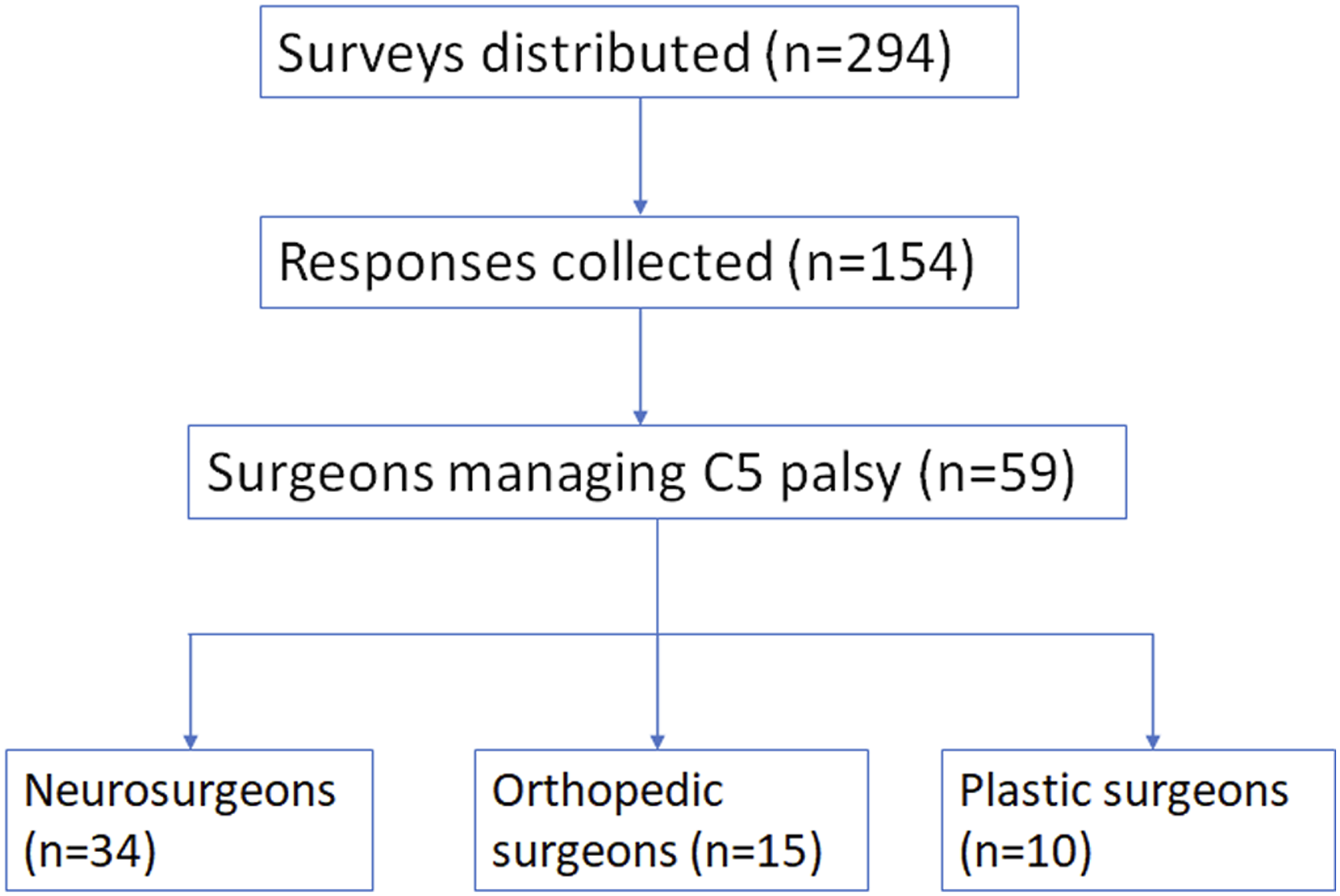
Choice of Donor-Recipient Nerve Transfers Among 54 Respondents Selecting Nerve Transfer as a Management Strategy.
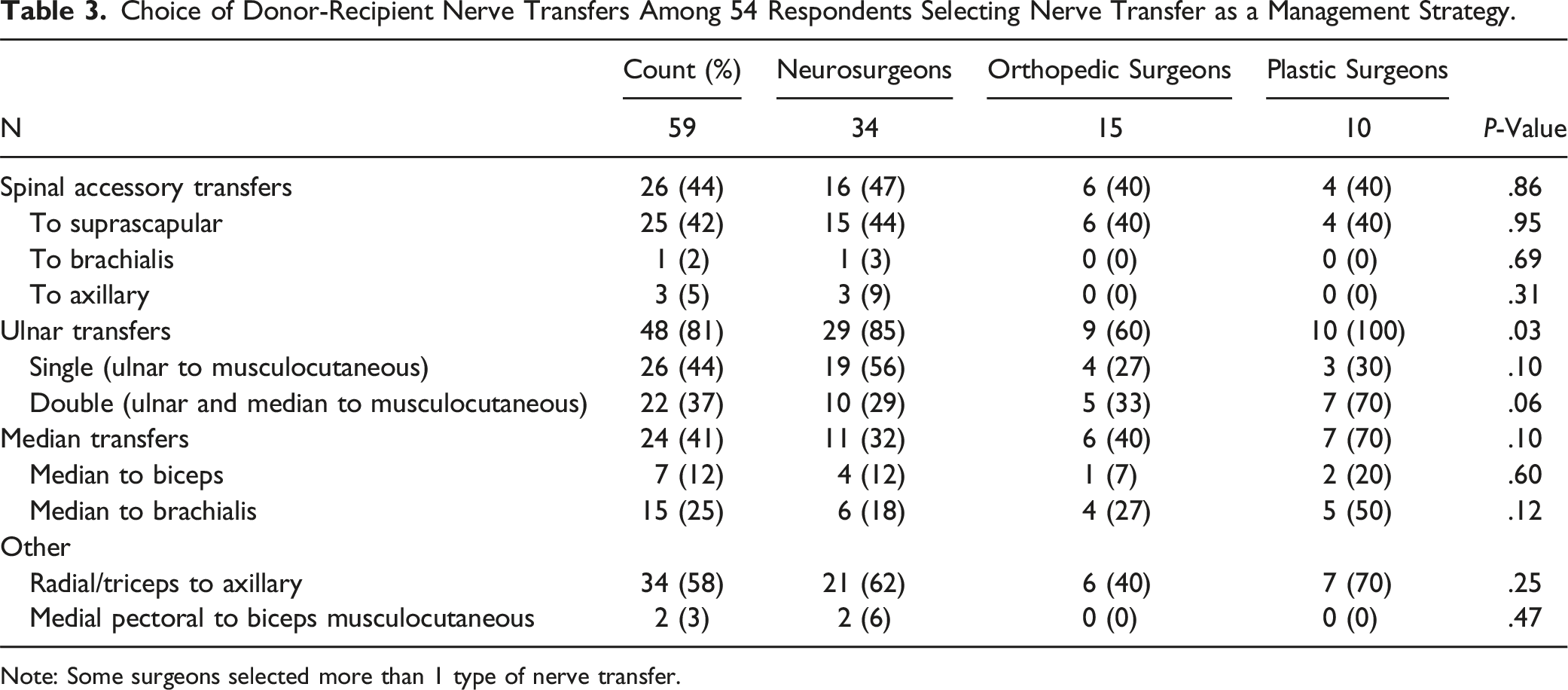
Note: Some surgeons selected more than 1 type of nerve transfer.
Surgeons selecting nerve transfers for surgical treatment differed across their choice of nerve transfer (Table 3). Ulnar/median nerve transfers to the musculocutaneous (biceps/brachialis branches) nerve were most frequently selected, with 48 (81%) surgeons choosing either a single (44%) or double (37%) fascicular transfer. Plastic surgeons were significantly more likely to select double fascicular transfers compared to neurosurgeons and orthopedic surgeons (100% vs 85% and 60%, respectively; P = .03). Plastic surgeons selected double fascicular transfers most frequently (70%) while neurosurgeons selected single fascicular transfers most frequently (56%). Transfer of the radial to axillary nerve was selected by 34 (58%) of respondents, while 25 (42%) selected spinal accessory transfer to the suprascapular nerve and 24 (41%) selected transfers of the median nerve.
Discussion
Postoperative C5P usually occurs within 1 week of cervical decompression surgery, including both anterior and posterior approaches.3,12 The underlying pathophysiology is not completely understood but is likely heterogeneous in etiology, reflecting iatrogenic injury, posterior spinal cord migration, ischemia, and reperfusion injury.10,13 Although most patients improve, some are left with residual motor weakness, an outcome whose incidence appears greatest in patients with post-operative strength less than grade 3/5. 11 These patients may benefit from surgical treatment; however, consensus guidelines on treatment strategies and optimal timing are lacking. 10 Here we surveyed an international cohort of peripheral nerve surgeons to identify treatment paradigms for C5P. We found that only 40% of peripheral nerve surgeons manage C5P following spine surgery, and most are in high volume academic practices. Electromyography is the most common diagnostic modality employed, although neurosurgeons are also significantly more likely to obtain an MRI. Nerve transfers were widely selected as standard-of-care in patients with post-operative strength less than grade 3/5, and timing of intervention varied based on severity. Additionally, neurosurgeons are significantly more likely to operate in a more delayed fashion for both partial and complete C5P injuries compared with orthopedic surgeons and plastic surgeons. Heterogeneity emerged in the choice of nerve transfers. The most common choice of donor-recipient nerve transfer is the single or double fascicular transfer for elbow flexion (81%), followed by the radial/triceps to axillary nerve (58%) and the spinal accessory to suprascapular nerve (42%).
Diagnostics and Surgical Timing
Diagnostic modalities such as EMG are employed as clinical tools to monitor recovery of C5P patients. Lubelski et al found that early use of EMG could predict the likelihood of recovery from post-operative C5P, with the presence of ≥2+ fibrillation portending poorer recovery, while normal motor unit recruitment suggested increased odds of a complete recovery. 5 A study of 77 patients by Pennington et al found that those with an abnormal EMG between 6 weeks and 6 months after injury were most likely to receive multimodal treatment and to be referred to peripheral nerve surgeons for nerve transfers. 1 They note that early use of EMG data can help ensure a speedy referral to peripheral nerve surgeons. Indeed, EMG was favored by a plurality of respondents in our survey, highlighting its use in identifying patients at risk of failing to recover. Electromyography data is considered more objective than the physical exam, which is subject to interrater variability and misinterpretation.5,10 Magnetic Resonance Imaging was also selected by a plurality of surgeons, as often expected for the occurrence of new neurological deficits, although there was greater disagreement compared to EMG. Houten et al argue that MRI is of little clinical value in patients whose clinical presentation is consistent with C5P, as it will not reveal pertinent actionable findings. 14 Such a presentation includes patients with new-onset difficulty lifting 1 arm without distal upper-extremity weakness or other symptoms of myelopathy.
Complicating the decision for surgical intervention in postoperative C5P is difficulty in predicting patients least likely to recover from C5P. Several predictors for the occurrence of C5P have been identified in the literature, including foraminal stenosis,4,7,15 preoperative C5 radiculopathy, 4 preoperative cord rotation, 16 and number of levels fused. 17 However, a systematic review of 16 studies by Jack et al did not find evidence that C5P is consistently associated with specific demographic, clinical, or surgical factors. 16 Prophylactic foraminotomy has been shown in some studies to reduce the risk of C5P, particularly in patients with preoperative foraminal stenosis.12,18-20 However, the potential reduction in the incidence of C5P must be balanced with the increased risk of iatrogenic injury. 21 Moreover, Bydon et al found that wider laminectomies can increase the risk of C5P, highlighting the discrepant results in the literature. 22
Factors predicting time to recovery in patients with C5P have been underexplored in the literature, although a muscle strength grade <3/5 is generally considered a poor prognosis which may benefit from surgical intervention. For example, Lim et al found that motor grade less than 3/5 predicted increased time to recovery for C5P on multivariable analysis. 23 Similarly, Pennington et al found that only numbness and baseline deficits predicted time to recovery, while patients with strength <3/5 at time of symptom onset had under a 50% chance of achieving a complete recovery. 11 They also found that while nerve surgery is the least routinely employed treatment strategy, patients with no functional recovery are most likely to be recommended for peripheral nerve transfers, a finding highlighted in this study as well, with 92% of surgeons opting for nerve transfers in cases without recovery. Furthermore, Saadeh et al reviewed 72 patients with post-operative C5P and found that 70% of patients with strength <3/5 at time of discharge after cervical spine surgery recovered to strength ≥3/5 within a year. However, the likelihood of recovering useful motor strength decreased as symptoms persisted over time, with only 50% of patients with strength <3/5 at 3-month follow-up recovering useful strength within a year, further decreasing to only 25% of those with persistent C5P after 6 months. Consequently, they suggest referring patients to peripheral nerve surgeons if they fail to improve 3 months after surgery. 24
The timing of surgical intervention for C5P should balance the potential for natural recovery from conservative treatment with the decreased efficacy from delayed operations. 5 Conservative treatment includes physical and occupational therapy to maintain range of motion and avoid stiffening. 1 Hofler et al found that 76% of patients with C5P recovered to baseline strength with a median recovery time of 2 months. 17 However, studies have noted that full recovery in select patients can take a few years.8,11 In the absence of functional recovery, survey respondents indicated waiting around 4-6 months prior to operating, with a reduced time for patients with complete injury, reflecting the lower likelihood of natural recovery and need for early intervention to produce greatest chance of successful outcome. Our survey found that neurosurgeons tend to wait longer than orthopedic and plastic surgeons prior to operating, potentially reflecting the greater exposure that neurosurgeons have to C5P after treating spinal pathology. Consequently, they may see the mostly positive natural history of the disease and choose to wait longer prior to operating; however, further exploration is warranted to determine the optimal time to intervene surgically.5,7
Surgical Treatment Paradigms
Postoperative foraminotomy and surgical re-exploration has been described in a few case studies as a treatment for C5P. Nakashima et al described 4 cases of C5P treated with C4-5 foraminotomy, of which 3 improved by 2 manual muscle test grades. 25 Kim et al reported 2 patients treated with foraminotomies, of which 1 fully recovered while the other failed to improve. 26 Imagama et al have also recommended foraminotomy in C5P patients with severe pain and motor paralysis. 27 Similar to recommendations for prophylactic foraminotomy, postoperative foraminotomy may be useful in patients with documented foraminal stenosis, however the findings of these prior studies may also just reflect the natural history of C5P. Overall, the use of postoperative foraminotomy for treating C5P has not been extensively reported in the literature, and was selected as a stand-alone option by only 19% of respondents.
In contrast, consensus emerged across all surgical specialties on the use of nerve transfers for C5P cases exhibiting poor motor strength and no recovery, although the choices of donor-recipient nerves exhibited greater heterogeneity. Nerve transfers can help restore elbow flexion, arm and shoulder abduction, and external rotation. 5 Few transfers have been described in the literature specifically for C5P; however, lessons from treatment of brachial plexus injuries can be applied. The choice of donor-recipient nerve transfer should account for the prioritized motor movement and muscle recovery of interest. Donor nerves that are expendable, capable of being transferred without an intervening nerve graft, have synergistic function with the recipient nerve, and contain sufficient motor axons to allow nerve in-growth should be selected.1,28 Elbow flexion is generally given greatest priority in treatment of brachial plexus injuries. 29 Single fascicular transfer of the ulnar nerve to the biceps branch of the musculocutaneous nerve to restore elbow flexion was most frequently selected by surgeons for C5P treatment.30-33 A meta-analysis by Sneiders et al found that single and double fascicular transfers are equally effective for attaining grade 3/5 or higher strength in elbow flexion, although the double transfer may improve the proportion of patients attaining grade 4/5. 34 Similarly, surgeons in our study were fairly split between the single and double fascicular transfer.
Other common nerve transfers selected included the triceps to axillary transfer and spinal accessory to suprascapular transfer. These transfers assist in improving shoulder abduction and external rotation. 29 For example, Songcharoen et al analyzed 577 cases of spinal accessory nerve transfers, finding that transfers to the suprascapular nerve resulted in useful motor recovery of 80% compared to only 60% for transfers to the axillary nerve. Indeed, Leechavengvongs et al recommend combining transfer of the radial nerve to the long head of the triceps with transfer of the spinal accessory nerve to the suprascapular nerve to improve shoulder abduction, an option selected by 16 (27%) of respondents. 29 Brown et al reported a dual spinal accessory to suprascapular nerve and radial to axillary nerve transfer for a case of Parsonage-Turner syndrome after cervical decompression with minimal improvement at 6 months. The patient improved in shoulder abduction and external rotation over the subsequent 9 months. 35 Lubelski et al described 9 patients with C5P successfully treated with nerve transfers between 3-8 months after the injury, while a 10th patient treated after 11 months failed to improve, illustrating the importance of early intervention. 13 However, the literature is overall limited in describing choices of nerve transfers for C5P, and the present survey’s results should be followed by studies assessing outcomes after nerve transfers for C5P.
Limitations
A limitation of this study is that the surgeons surveyed represent only a fraction of peripheral nerve surgeons, and selection bias may be present amongst those choosing to respond. Although the survey was distributed to an international organization, respondents mainly originated from North America or Europe, and future surveys should include a larger cohort in other geographic territories. Additionally, case scenarios cannot account for the wide array of clinical presentations and patient-specific factors that may affect surgical decision-making, such as comorbidities, patient preferences, and psychosocial factors. However, this is the first such survey report and provides insight into peripheral nerve surgeons’ perspective on the workup and treatment of C5P after spine surgery. Future surveys and retrospective chart reviews should also assess the nature and rate of complications associated with surgical intervention for C5P.
Conclusion
The present survey found that 38% of peripheral nerve surgeons manage cases of C5P, including neurosurgeons, orthopedic surgeons, and plastic surgeons. Electromyography was most frequently selected for diagnostic workup of C5P, followed by MRI. Average time to surgical intervention was 4.5 months for patients with 0/5 strength vs 6.6 months for those with 2-3/5 deltoid and/or biceps strength. Nerve transfers, particularly the double fascicular transfer for elbow flexion, were widely selected by most respondents. Somewhat less popular were the radial to axillary nerve transfer and spinal accessory to suprascapular nerve transfer for restoration of shoulder abduction and stability. Fewer surgeons selected postoperative foraminotomies. The results highlight consensus amongst peripheral nerve surgeons of the usefulness of nerve transfers for C5P cases with severe motor weakness exhibiting failure to improve, with longer observation periods for those that show some evidence of early recovery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.