
Abstract
Study Design
Longitudinal study.
Objectives
Intravoxel incoherent motion (IVIM), a magnetic resonance imaging (MRI) scanning technique that applies diffusion-weighted imaging (DWI), is effective for the quantitative assessment of malignant tumors of the vertebral bone. We hypothesized that IVIM parameters of vertebral bodies are associated with the prognosis of osteoporotic vertebral fracture (OVF). We aimed to explore the relationships between IVIM parameters for vertebral collapse and non-union after OVF and calculate the cut-off values of these parameters for vertebral collapse and non-union.
Methods
A total of 150 patients with acute OVF (150 women; mean age: 79.1 ± 7.4 years) were included and treated conservatively with bracing. MRI was performed at the time of injury. IVIM parameters, such as apparent diffusion coefficient (ADC), molecular diffusion coefficient (D), and perfusion-related diffusion (D*) were recorded. The patients were classified into 3 groups: low-collapse (height loss of ≤50%), high-collapse (height loss of >50%), and non-union. We compared ADC, D, and D* among the low-collapse, high-collapse, and non-union groups and performed a receiver operating characteristic (ROC) curve analysis to determine the boundary values of the high-collapse and non-union groups.
Results
The low-collapse, high-collapse, and non-union groups had no significant differences in ADC and D. However, D* differed significantly among the 3 groups. ROC analysis revealed cut-off values of 19.0 × 10-3 mm2/s and 12.3 × 10-3 mm2/s for the high-collapse and non-union groups, respectively.
Conclusions
D* is a significant prognostic indicator for high-collapse and non-union groups with OVF. This suggests that D* should be considered when assessing OVF.
Introduction
Vertebral fractures (VF) are 1 of the most common skeletal fractures associated with osteoporosis. 1 In general, the outcomes of conservative management of osteoporotic vertebral fracture (OVF) with a bed rest period, pain control with analgesics, bracing, and early rehabilitation have yielded good results, with excellent functional recovery and without pain. 2 However, recent studies have revealed that some patients develop vertebral collapse and non-union, leading to unfavorable outcomes, such as residual pain, decreased activities of daily living, and decreased quality of life. 3
The importance of investigating the risk factors associated with vertebral collapse and non-union has been emphasized. Several recent studies have examined the potential risk factors associated with vertebral collapse and non-union.3-5 The major risk factors that were statistically predictive of the following complications were as follows: (1) vertebral collapse, existence of intravertebral clefts, total-type fractures on magnetic resonance (MR) T1-weighted image (WI), and hypertension-wide-type fractures on T2-WI; and (2) non-union: middle-column injury, involvement of the thoracolumbar vertebrae, limited high-intensity pattern on MR T2-WI, and widespread low-intensity pattern. 5 These MR imaging (MRI) patterns are qualitative, visually detectable, and reflect inflammatory edematous reactions with restrained trabecular destruction, hematoma, and fluid accumulation. 5 There is a report on the quantitative evaluation of vertebral bone marrow perfusion in acute OVF using dynamic contrast-enhanced MRI. 6 However, contrast media should be used with caution, considering several factors, such as age, renal function, and presence of allergies. 7
Intravoxel incoherent motion (IVIM) is an MRI scanning technique that applies diffusion-weighted imaging (DWI). It has recently been demonstrated to be an attractive approach for the quantitative assessment of tissue water diffusivity and microcapillary perfusion using signal decay at large (200-1000 s/mm2) and relatively small (0-200 s/mm2) b-values, respectively. 8 Both water molecular diffusion and perfusion-related diffusion can be monitored by extracting the molecular diffusion coefficient (D) and perfusion-related diffusion (D*). These IVIM-derived quantitative parameters have been widely used in studies of the central nervous system and the abdomen.9-11 Moreover, recent studies have reported the usefulness of IVIM for the quantitative assessment of malignant tumors of the vertebral bone.12,13 However, to the best of our knowledge, the effects of intramedullary perfusion on VF analysis have not yet been investigated using IVIM.
Prediction of the occurrence of vertebral collapse and non-union at the initial treatment stage may enable therapeutic interventions, such as vertebroplasty and surgery, at an early phase. We hypothesized that the IVIM parameters of vertebral bodies are associated with OVF prognosis. In this study, we aimed to explore the relationships between IVIM parameters and vertebral collapse and non-union after OVF and to calculate cut-off values for vertebral collapse and non-union.
Materials and Methods
The institutional review board of the Sapporo Maruyama Orthopaedic Hospital approved this study (IRB approval no., 32). All participants were provided with written and verbal explanations of the study, and their consent was obtained prior to participation.
Participants
Acute OVF was considered when the interval between the onset of back pain and the initial visit was <1 week and an MRI examination showed abnormal signal changes in the vertebral body, such as high signal changes on short tau inversion recovery and low signal changes on T1-WIs. All patients were treated conservatively with bracing (tailor-made elastic brace). The exclusion criteria were as follows: i) prior or multiple VF, ii) systemic inflammatory disease, iii) neoplasm or infection, iv) images of motion or metal artifacts, v) high-energy injuries, and vi) a radiological follow-up period of <3 months.
IVIM
MRI was performed using a GE Signa Creator 1.5T (GE Healthcare, Wauwatosa, MI, USA) and we simultaneously obtained IVIM parameters. The IVIM parameters apparent diffusion coefficient (ADC), D, and D* were obtained from the IVIM data using the scan technique of Park et al (TR 3300 ms; TE 85 ms; b-values = 0, 10, 20, 30, 50, 80, 120, 200, 300, 500, and 800 s/mm2; voxel size .45 × .55 × 5 mm).
14
All maps were created using SYNAPSE VINCENT (FUJIFILM, Tokyo, Japan). The regions of interest (ROIs) were independently set and measured by an experienced research scientist (H.T.) and MRI technologist (R.I.) blinded to the identification of the patients (Figure 1). The additional imaging time was 125 s with the addition of IVIM to a regular MRI in our hospitals. Vertebral height was measured at the point of maximal collapse of the affected vertebral body and height loss (%) was calculated using the following formula: ([{lower vertebral height + upper vertebral height}/2 − affected vertebral height]/[{lower vertebral height + upper vertebral height}/2]) × 100.
15
Set of the regions of interests (ROIs) for vertebral bodies.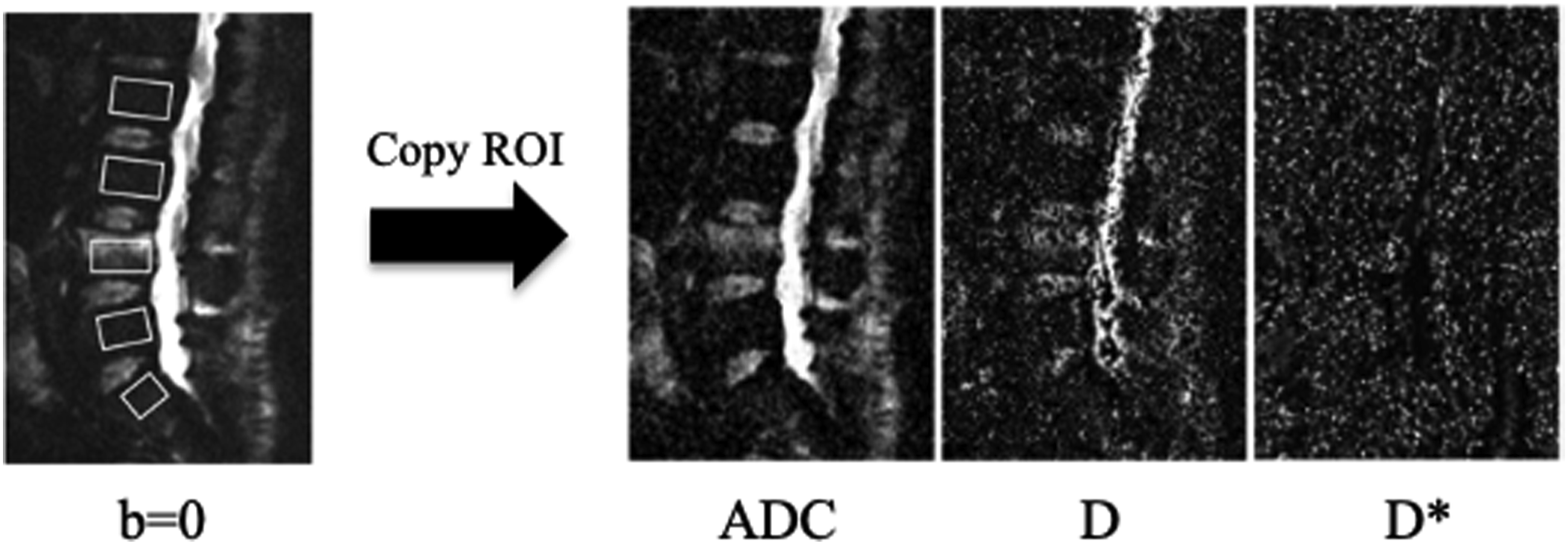
Assessment of Vertebral Collapse and Non-union
Height loss was measured initially and at 3 months follow-up using lumbar radiography. The difference between the initial and final height losses was recorded as the height loss difference. Based on the findings of previous reports, 16 a height loss of ≤50% was classified as a low degree of vertebral collapse (low-collapse group), whereas that of >50% was classified as a high degree of vertebral collapse (high-collapse group). Non-union was defined as a recognizable intravertebral cleft and apparent segmental motion on dynamic plain radiographs (≥5° between the supine and weight-bearing positions), 3 and these patients were classified as the non-union group.
Statistical Analysis
Multiple group means were compared using one-way factorial measures of analysis of variance, and Tukey-Kramer test was used for pair-wise comparisons. The distribution of injured vertebral levels was analyzed using chi-squared test. We also performed a receiver operating characteristic (ROC) curve analysis of the significant variables to determine the boundary values of high-collapse and non-union. We used the Youden index to determine the optimal cut-off point for testing. 17 The Youden index is defined as the maximum vertical distance between the ROC curve and the diagonal or chance line and is calculated as Youden index = maximum (sensitivity + specificity −1). Using this measure, the cut-off point on the ROC curve that corresponds to the Youden index, that is, at which (sensitivity + specificity −1) is maximized, was taken to be the optimal cut-off point, and statistical significance was set at P < .05. SPSS (version 27.0; IBM Corp, Armonk, NY, USA) was used for all statistical analyses. Numerical data are expressed as mean ± standard error of the mean.
Results
We found that 150 patients (mean age 79.1 ± 7.4 years) satisfied the inclusion criteria. This study analyzed the following 3 groups: low-collapse (n = 74), high-collapse (n = 61), and non-union (n = 15) groups. The details of the injured vertebral levels among the participants are shown in Figure 2; no significant differences were found in the distribution of the injured vertebral level by the chi-squared test. All fractures were classified using osteoporotic fracture (OF) classification
18
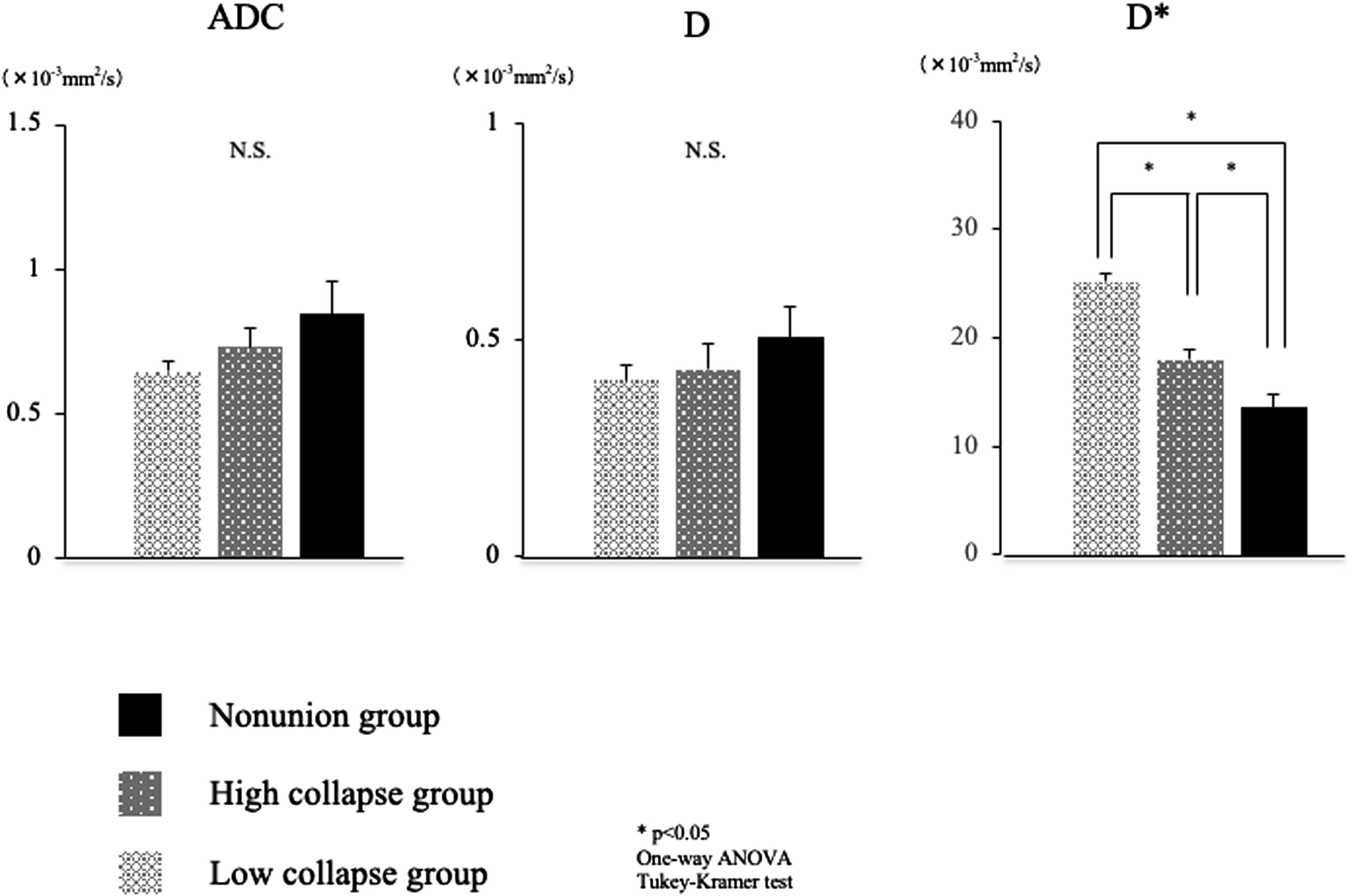
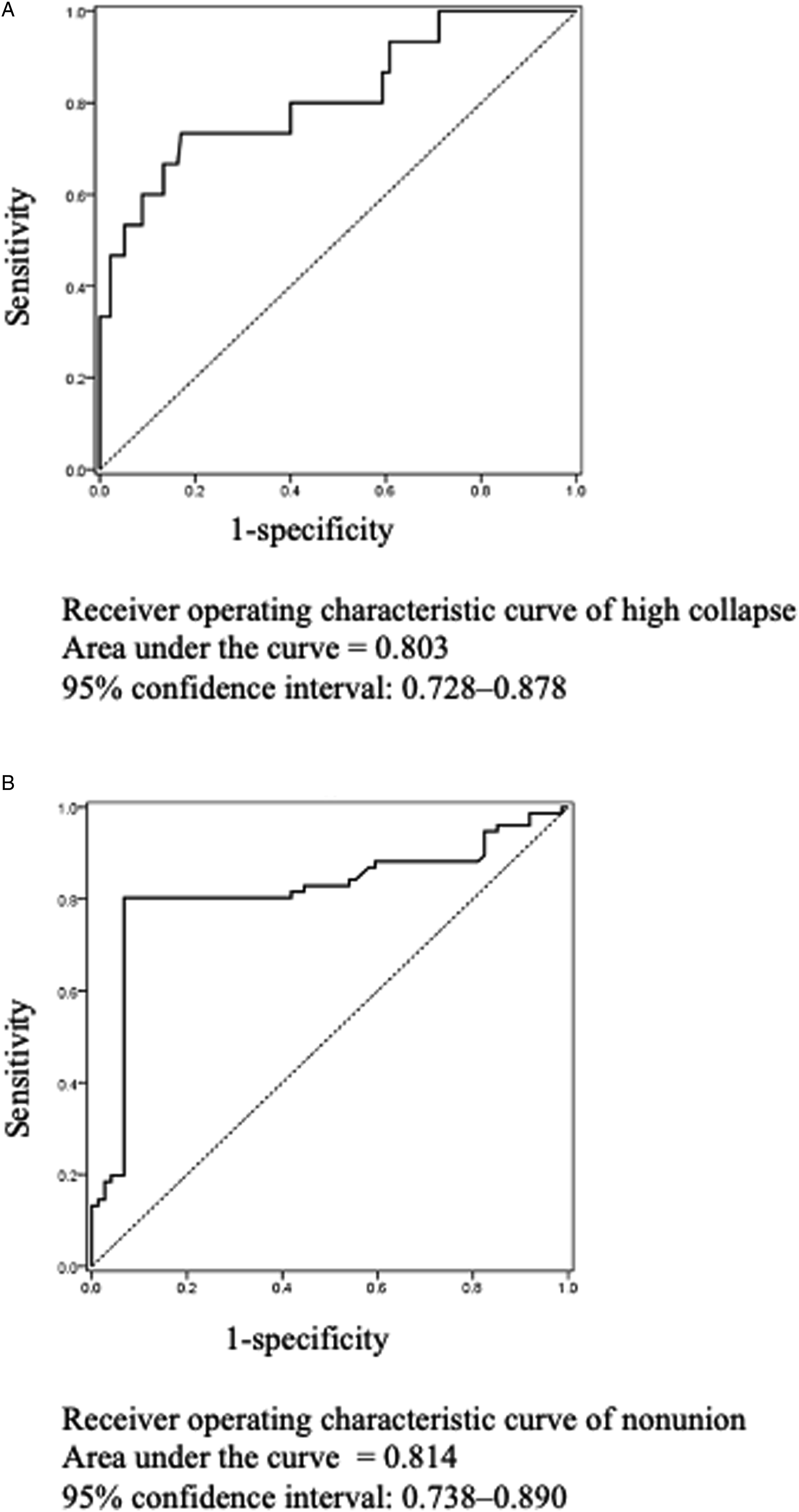
including 49 OF type-II fractures which is deformation with no or only minor involvement of the posterior wall (<1/5) (32.7%), 83 OF type-III fractures which is deformation with distinct involvement of the posterior wall (>1/5) (55.3%), and 18 OF type-IV fractures which is deformation of both endplates with or without lesion of the posterior wall (21.3%). As shown in Figure 3, the low-collapse, high-collapse, and non-union groups had no significant differences in ADC (.64 ± .03 × 10−3 mm2/s vs .73 ± .06 × 10−3 mm2/s vs .84 ± .11 × 10−3 mm2/s, respectively) and D (.41 ± .05 × 10-3 mm2/s vs .43 ± .09 × 10−3 mm2/s vs .51 ± .10 × 10−3 mm2/s, respectively). However, D* differed significantly among the low-collapse, high-collapse, and non-union groups (25.2 ± .7 × 10−3 mm2/s vs 18.0 ± .9 × 10−3 mm2/s vs 13.5 ± 1.2 × 10−3 mm2/s, respectively). D* was significantly lower in the non-union group than those in the low- and high-collapse groups and was significantly lower in the high-collapse group than that in the low-collapse group. The cut-off values of D* obtained using ROC analysis of high-collapse and non-union are shown in Figure 4. The cut-off value, sensitivity, specificity, and area under the curve (AUC) for the high-collapse group were 19.0 × 10−3 mm2/s, 73.3%, 83.0%, and .803, respectively (Figure 4A). The cut-off value, sensitivity, specificity, and AUC for the non-union group were 12.3 × 10−3 mm2/s, 80.3%, 93.2%, and .814, respectively (Figure 4B). The distributions of the OVF levels of the low-collapse, high-collapse, and non-union groups. No significant differences were found in the distribution of injured vertebral level. OVF, osteoporotic vertebral fracture. Comparison of ADC, D, and D* among the low-collapse, high-collapse, and non-union groups. D* was significantly lower in the non-union group than those in the low- and high-collapse groups and significantly lower in the high-collapse group than that in the low-collapse group. ADC, apparent diffusion coefficient; D, molecular diffusion coefficient; D*, perfusion-related diffusion. Receiver operating characteristic curves of high-collapse and non-union. (A) The cut-off value for high-collapse was 19.0 × 10−3 mm2/s. (B) The cut-off value for non-union was 12.3 × 10−3 mm2/s.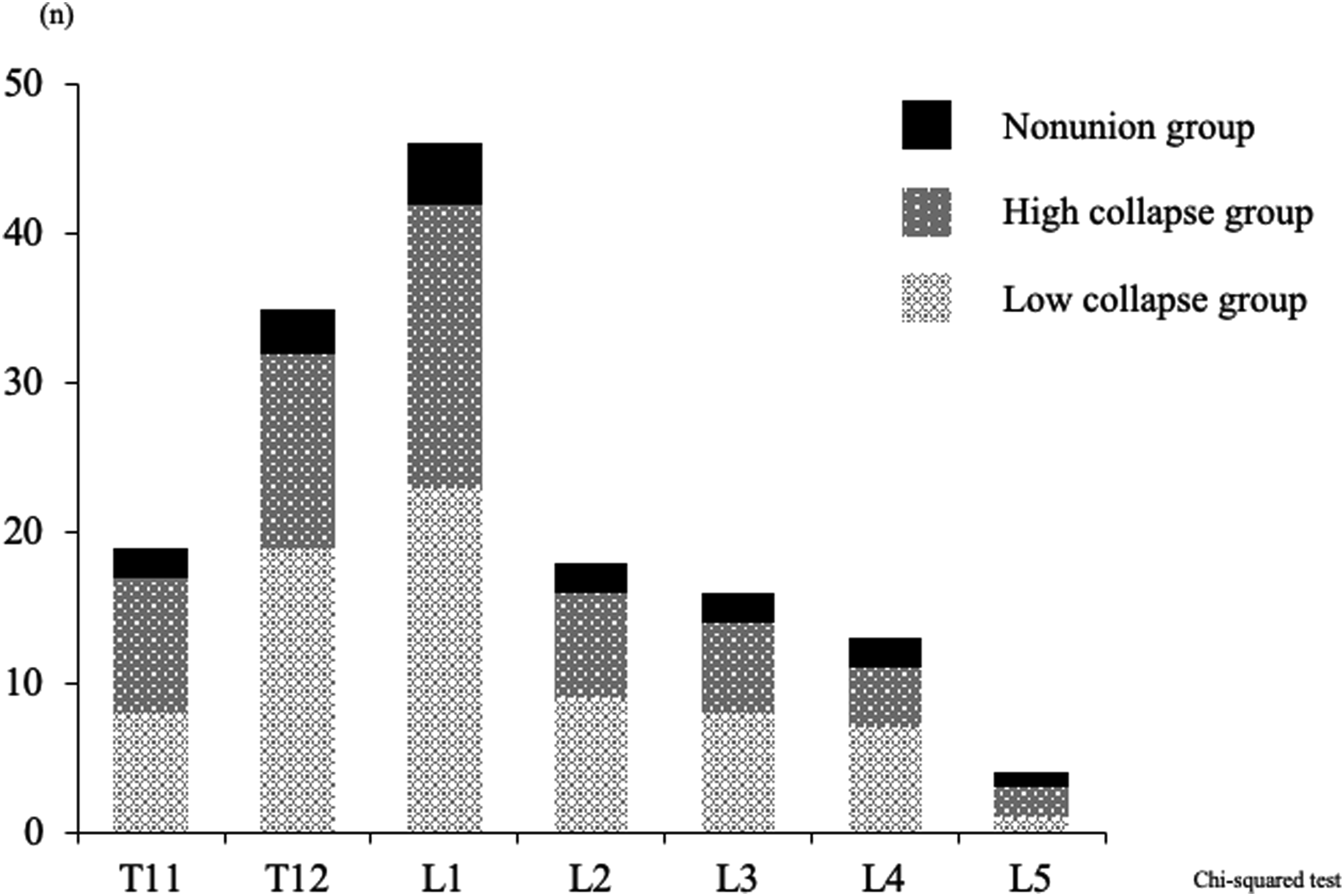
Discussion
When treating OVF, prediction of the prognostic factors for the progression of vertebral collapse and non-union in the early stages is important. For this purpose, some reports have analyzed and evaluated blood flow in the VFs using contrast media to assess intramedullary perfusion disorders.6,19,20 However, contrast media may not be desirable because of its side effects, such as nephrogenic systemic fibrosis. DWI, which reflects cell density, has been used to identify vertebral bone marrow lesions.21,22 The use of conventional DWI to derive ADC involves both microcirculation perfusion and diffusion of water molecules. Simultaneous assessment of water diffusion and perfusion is possible with the use of IVIM, 23 which is a technique that can extract vascularity-related parameters, such as D and D*.8,24 To the best of our knowledge, most previous studies on IVIM for vertebral lesions focused on the differentiation between malignant and benign lesions,12,25,26 and have not yet investigated OVF using IVIM.
This study investigated the relationships between IVIM parameters for non-union after OVF and showed that the non-union group had a significantly lower D* than the high- and low-collapse groups. Our findings also showed that the high-collapse group had a significantly lower D* than the low-collapse group. The D* parameter is considered to be a perfusion-related coefficient and has been previously reported to be relatively high in malignant spinal tumors, suggesting restricted true diffusion and greatly-increased perfusion in malignant tumors. 12 The vertebral body is supplied directly by a pair of segmental arteries, 27 and artery impairment due to OVF is considered to be 1 of the mechanisms of non-union. We hypothesize that decreased D*, indicating impaired vertebral body blood flow, would be 1 of the mechanisms of a high degree of vertebral collapse and non-union. Meanwhile, this study showed that ADC and D had no association with the low- and high-collapse and non-union groups. ADC and D were considered to affect the diffusion coefficients due to edematous changes, fluid exudation, and the disruption of microvessels and trabecular bones.14,28 The D and ADC parameters reflect these conditions and would have no effects on collapse or non-union. We considered that D* might be a quantitative predictor of a high degree of vertebral collapse and non-union when using IVIM.
Typically, vertebroplasty or kyphoplasty is considered for patients with intractable, intense pain from OVF, despite at least 6 weeks of conservative medical therapy. 29 In recent years, there have been scattered reports on the effectiveness of early surgical treatment for OVF.30,31 Minamide et al 30 reported that kyphoplasty for thoracolumbar OVF could prevent progressive collapse and kyphosis, and patients who underwent early kyphoplasty (within 4 weeks after the occurrence of OVF) demonstrated better spinal alignment, better lower back pain scores, and reduction in subsequent adjacent fractures. Liu et al 31 reported that early kyphoplasty performed at emergency or within a week after injury demonstrated good results in terms of visual analog scale scores, Oswestry disability index, and compression rates of anterior vertebral height and kyphosis angle compared with kyphoplasty performed a month or more after injury. The present study showed that D* might be a prognostic predictor for high-collapse and non-union and this would be useful for early surgical intervention. We believe that the cut-off points of 19.0 × 10−3 mm2/s for high-collapse and of 12.3 × 10−3 mm2/s for non-union at the time of injury may serve as prognostic indicators for OVF, and early option of conservative or surgical treatment based on D* might lead to better outcomes for OVF.
Because IVIM parameters are considered to change based on age, sex, and bone density, it is a limitation of this study that it does not consider these factors. A detailed analysis considering these factors is required in the future. However, to the best of our knowledge, this study is the first to demonstrate that IVIM findings could potentially be used to predict non-union and a high-degree of vertebral collapse in OVF. In future, the association between D* and clinical symptoms such as low back pain, and the effectiveness of anti-osteoporotic drugs should be established.
Conclusions
This study investigated the relationships between IVIM parameters for non-union after OVF and showed that the non-union group had a significantly lower D* than the high- and low-collapse groups. Our findings also revealed that the high-collapse group had a significantly lower D* than the low-collapse group. ROC analysis revealed cut-off values of 19.0 × 10−3 mm2/s for high-collapse and 12.3 × 10−3 mm2/s for non-union. Our results indicate that D* is a significant prognostic indicator for high-collapse and non-union of OVF. This suggests that D* should be considered when assessing OVF.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.