
Abstract
Study Design
Finite element analysis (FEA).
Objective
This study aimed to explore the effects of cage elastic modulus (Cage-E) on the endplate stress in different bone conditions: osteoporosis (OP) and non-osteoporosis (non-OP). We also explored the correlation between endplate thickness and endplate stress.
Methods
The FEA models of L4-L5 with lumbar interbody fusion were designed to access the effects of Cage-E on the endplate stress in different bone conditions. Two groups of the Young’s moduli of bony structure were assigned to simulate the conditions of OP and non-OP, and the bony endplates were analyzed in 2 kinds of thicknesses: .5 mm and 1.0 mm, with the insertion of cages with different Young’s moduli including .5, 1.5, 3, 5, 10, and 20 GPa. After model validation, an axial compressive load of 400 N and a flexion/extension moment of 7.5Nm was performed on the superior surface of L4 vertebral body in order to analyze the distribution of stress.
Results
The maximum Von Mises stress in the endplates increased by up to 100% in the OP model compared with non-OP model under the same condition of cage-E and endplate thickness. In both OP and non-OP models, the maximum endplate stress decreased as the cage-E decreased, but the maximum stress in the lumbar posterior fixation increased as the cage-E decreased. Thinner endplate thickness was associated with increased endplate stress.
Conclusion
The endplate stress is higher in osteoporotic bone than non-osteoporotic bone, which explains part of the mechanism of OP-related cage subsidence. It is reasonable to reduce the endplate stress by reducing the cage-E, but we should balance the risk of fixation failure. Endplate thickness is also important when evaluating the cage subsidence risk.
Introduction
Lumbar degenerative diseases (LDD) are considered to be a series of age-related diseases with low back pain and sciatica as the main clinical manifestations caused by the degenerative changes of the lumbar intervertebral, facet joints and the surrounding ligaments. They are the leading cause of worldwide productivity loss and the top cause of years lived with disability in 126 countries. 1 With the aging of world population, an increasing number of elderly patients with LDD suffer from poor quality of life and dysfunction, therefore need to receive lumber fusion surgery. Osteoporosis (OP) is also a common disease characterized by low bone mineral density (BMD) in the aging population, which affects nearly one-third of people aged 50 years and older. 2 It can also reduce the strength of the lumbar spine, and frequently cause the vertebral compression fractures.3,4 OP was very common in patients aged≥50 years undergoing lumbar fusion surgery, with the prevalence of up to 53.4%. 5 Accordingly, it’s essential to give attention to postoperative complications caused by OP.
Lumbar interbody fusion routinely requires the implantation of interbody cages to provide axial support for the intervertebral space. Cage subsidence is a common complication after lumbar interbody fusion, it may affect the clinical outcomes of lumbar fusion surgery, leading to reduced fusion rate and reoperation.6,7 OP is a well-known risk factor for cage subsidence.8,9 It has been reported that low BMD leads to compromised bone strength and decreased failure loads of the bony endplates.4,10 The elastic modulus of fusion cages is also believed to affect the subsidence risk. For example, the titanium cage tends to have higher rate of subsidence than polyetheretherketone (PEEK) cages because of the high Young’s modulus of titanium cages. 11 The Young’s modulus of human bone usually decreases as the increasing of age and bone loss. 12 In this case, another possible reason for the high risk of cage subsidence in osteoporotic spine is the mismatch in biomechanical characteristics between fusion cages and osteoporotic vertebral bone. The fusion cages used in clinical practice are always designed according to the elastic modulus of normal bone. We hypothesized that the fusion cages with low elastic modulus can better match the elastic modulus of osteoporotic lumbar spine, and decrease the stress on cage-endplate interface.
Finite element analysis (FEA) allows for the alteration of various parameters to systematically understand the role of each structure and condition on the spine’s biomechanical response. 13 In our study, we established 2 FE models according to different bone conditions: OP and non-osteoporosis (non-OP). We aim to access the effects of cage elastic modulus (Cage-E) on the endplate stress in different bone conditions, to guide the design of low elastic modulus cages for osteoporotic patients in our future work.
Methods
Images Data Acquisition and Reconstruction
This study was approved by Peking University Third Hospital Medical Science Research Ethics Committee (M2022083). The informed consent was waived because this was a retrospective study using patients’ computed tomography (CT) images. The lumbar CT scan of a 39-year-old man was used to develop the model geometry. The data were imported into the Mimic 23.0 software (Materialise Inc, Leuven, Belgium) in the DICOM format. According to the different gray-scale value (HU) range of the vertebral bone, the 3D geometric models of the bony part of the lumbar spine were reconstructed by using threshold selection, mask, 3D region growing and calculation.
The 3D models of L4-L5 were then imported into the Geomagic Studio 2015 (3D Systems, Ltd, USA) in the STL format. According to the original CT images, error correction and surface smoothing were performed with the STL data. The parametric surface of the entity model was further optimized to build the L4-L5 geometric model. The 3D geometric models of cage, rod and screws were created by the UG 12.0 software (Siemens PLM Software, USA). Finally, the 3D geometric models of L4-L5, cage, rods and screws were exported in the STP format.
FEA Model Establishment
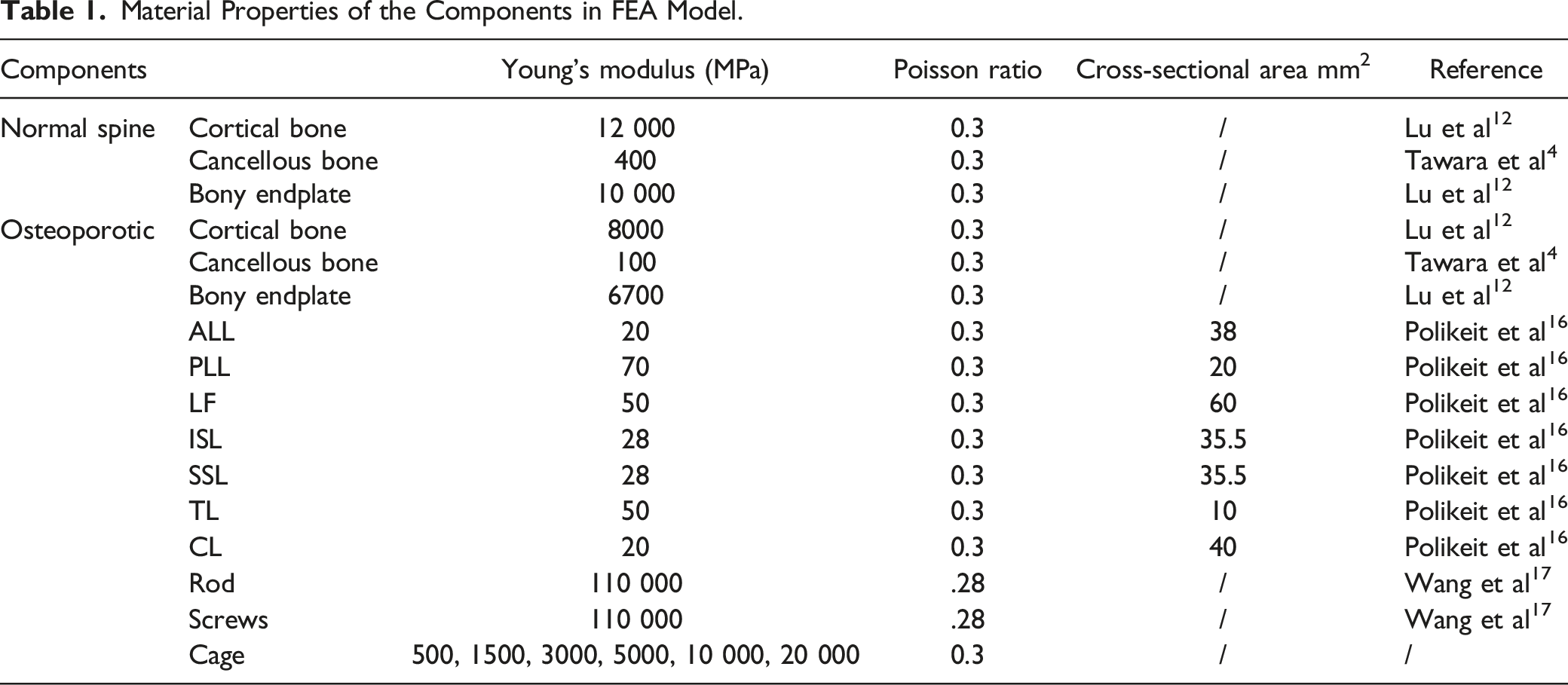
The geometric model STP file was meshed in Hypermesh 14.0 (Altair, USA). The bony part, cage, screws and rods were divided into tetrahedral mesh elements with the size of 1 mm. The ligaments were divided into beam elements. The meshed model was saved as INP form and imported into Abaqus 6.13 software (SIMULIA, French) for further static analysis. Each vertebral body was divided into 3 parts: cortical bone, cancellous bone and bony endplate. Especially, the cortical bone was 1.0 mm thick while the endplate was analyzed in 2 kinds of thickness: .5 mm and 1.0 mm.14,15 A total of 7 kinds of ligaments were included: anterior longitudinal ligament (ALL), posterior longitudinal ligament (PLL), ligament flava (LF), interspinous ligament (ISL), supraspinous ligament (SSL), intertransverse ligament (ITL), and capsular ligament (CL). The bullet-shaped cage (29 mm in length, 12 mm in width, 11 mm in height) was transversely placed into the middle of intervertebral space. A total of 4 simulated pedicle screws (6 mm in diameter and 45 mm in length) were inserted through the pedicles of L4 and L5, and connected by 2 rods (5.5 mm in diameter and 50 mm in length). The cage and endplates were assigned to be bonded, ensuring there is no relative displacement between the cage-endplate interfaces, which could simulate the condition of complete fusion. Similarly, the connection between the screws and the bone was set up as binding contact. The FEA model was showed in Figure 1. The material properties for each component in the FEA model are listed in Table 1. In particular, the Young’s moduli of cortical bone and bony endplates in OP and non-OP models were determined by reference to the work of Lu et al.
12
The Young’s modulus of cancellous bone in the 2 models were determined by reference to the BMD cut-off values of quantitative computed tomography (QCT) for identifying OP and non-OP patients, and the correlation between QCT BMD and Young’s modulus.
4
The FEA model of L4-5 lumbar interbody fusion with pedicle screw fixation. Material Properties of the Components in FEA Model.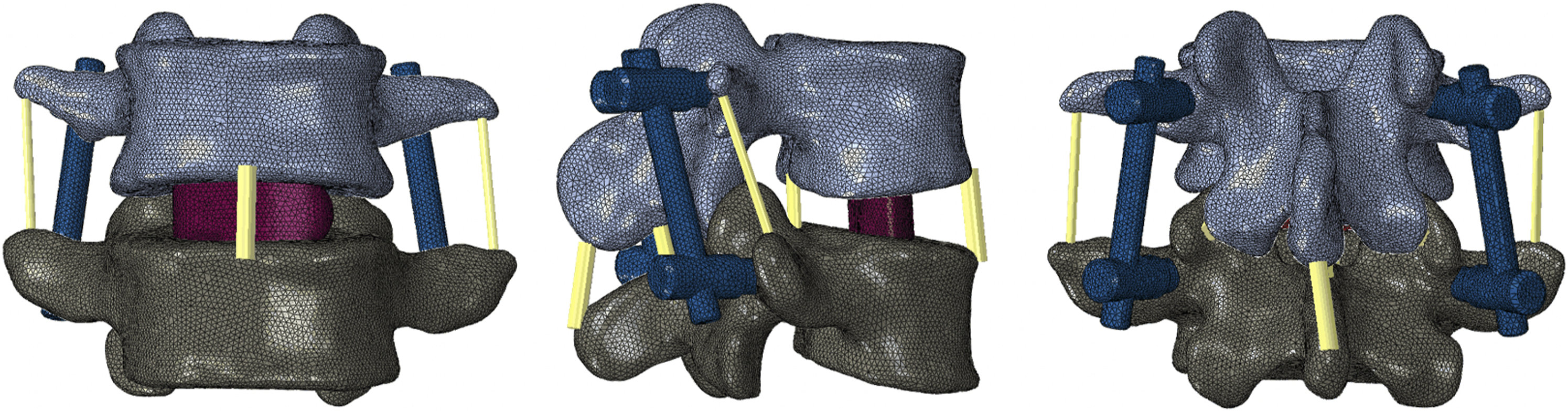
Validation and Load Condition
This FE model was validated by comparing the range of motion (ROM) results with those of the cadaveric study conducted by Shim et al under similar loads.18,19 In the model for validation, the intervertebral disc was complete and the material properties for annulus fibers, nucleus pulposus, and annulus fibrous substance were similar to previous research.20,21 The range-of-motion (ROM) results from this study were compared with those from the cadaveric study conducted by Shim et al after applying similar loads to current model. A good agreement between the results and the reported data was shown in Figure 2. Thus, our model can offer effective information for further analysis. Comparison of the ROM results between this study and the cadaveric study conducted by Shim et al. L, left; R, right.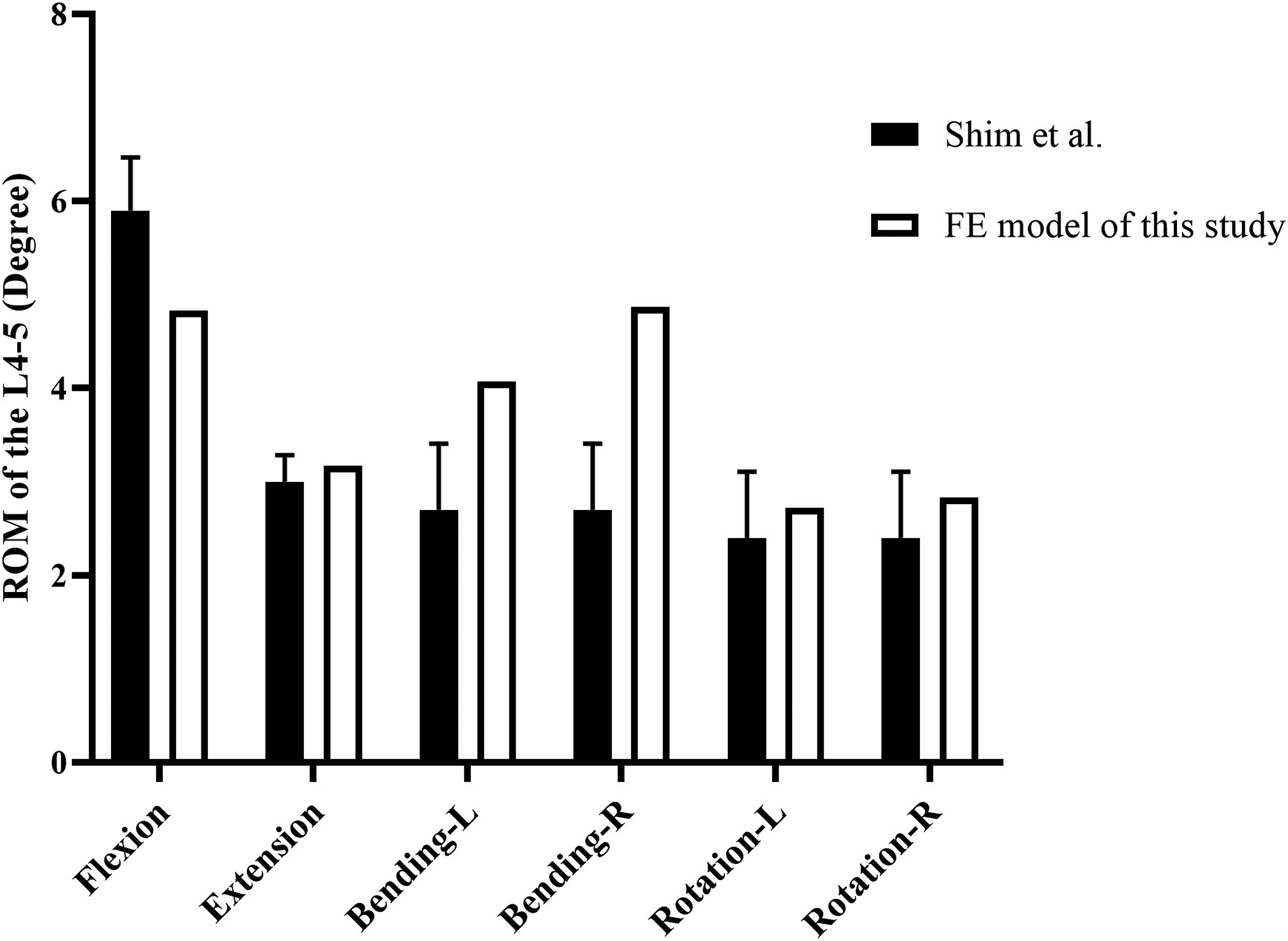
In this study, we only analyzed the lumbar flexion and extension conditions. A reference point was created and constrained to the surface nodes of the L4. 14 To simulate the upper torso of a normal adult and flexion-extension movement, an axial compressive load of 400 N and a flexion or extension moment of 7.5Nm were assigned to the superior surface of L4 vertebral body.14,22 The inferior surface of L5 vertebral body in the model was fixed rigidly. The von Mises stresses in L4/L5 vertebral body, endplates, cage and screws were calculated.
Results
Effect of OP on the Endplate Stress
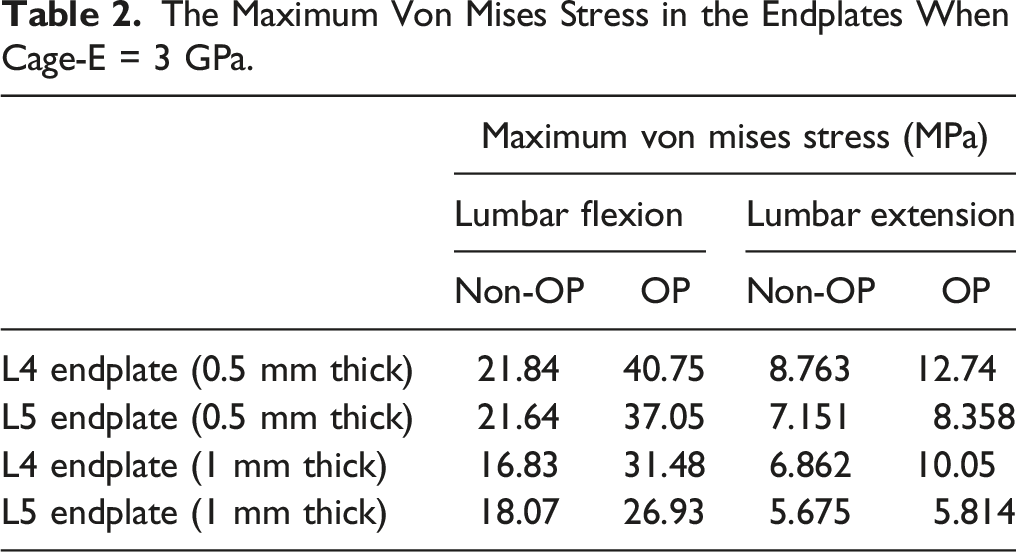
The Maximum Von Mises Stress in the Endplates When Cage-E = 3 GPa.
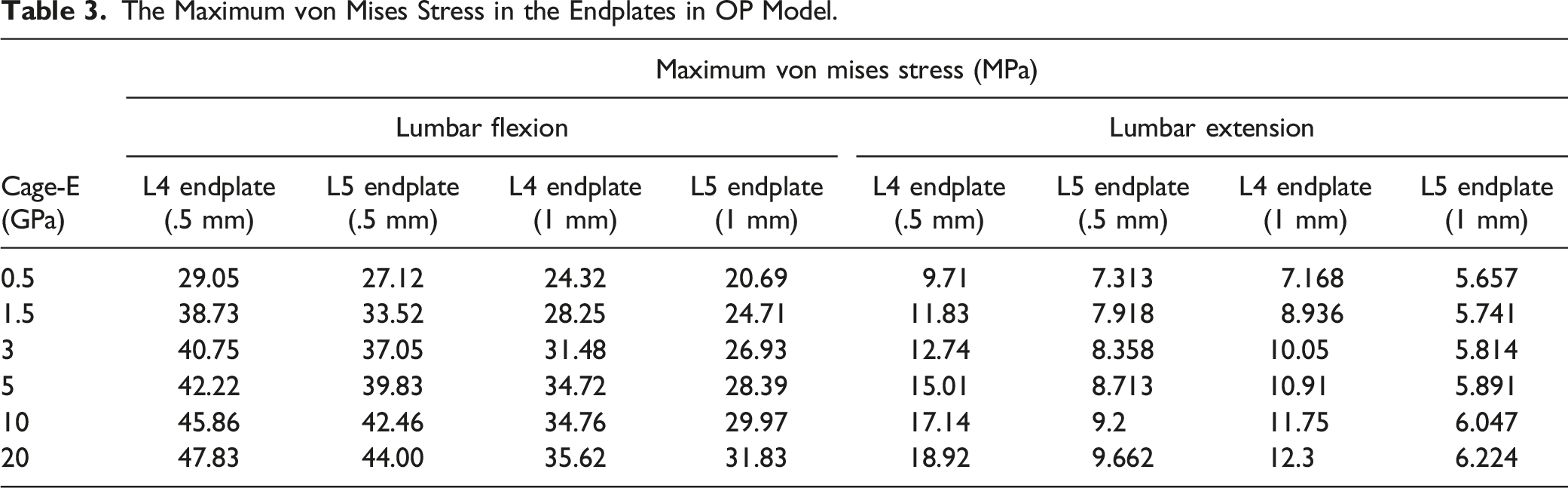
The Maximum von Mises Stress in the Endplates in OP Model.
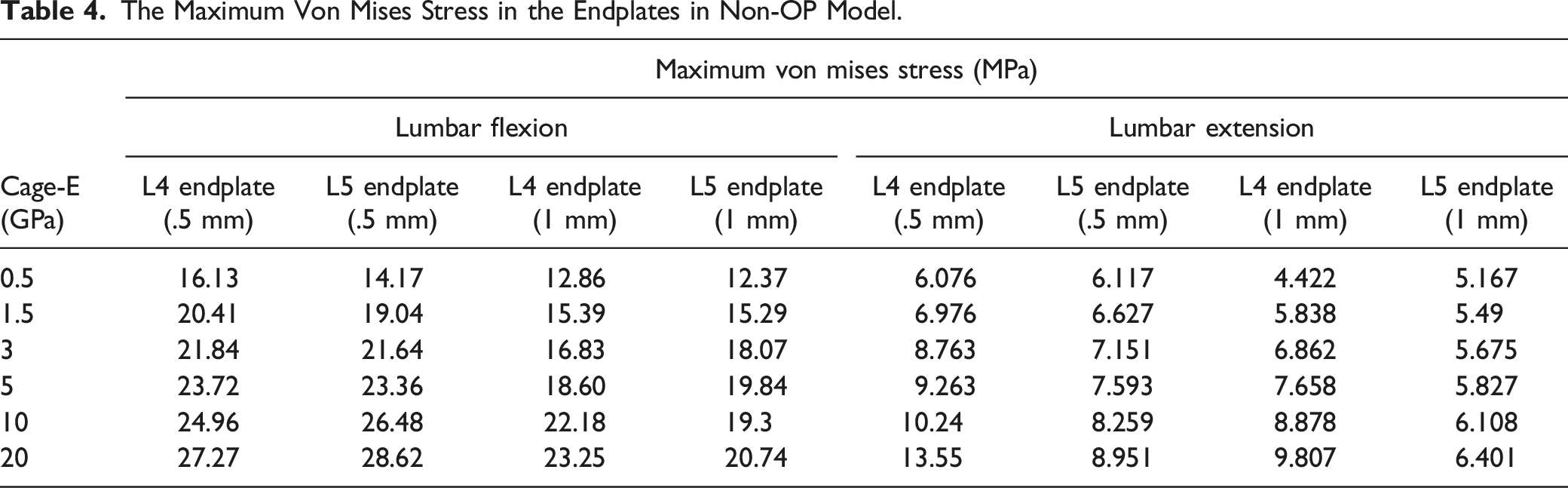
The Maximum Von Mises Stress in the Endplates in Non-OP Model.
Effect of Cage-E on Endplate Stress
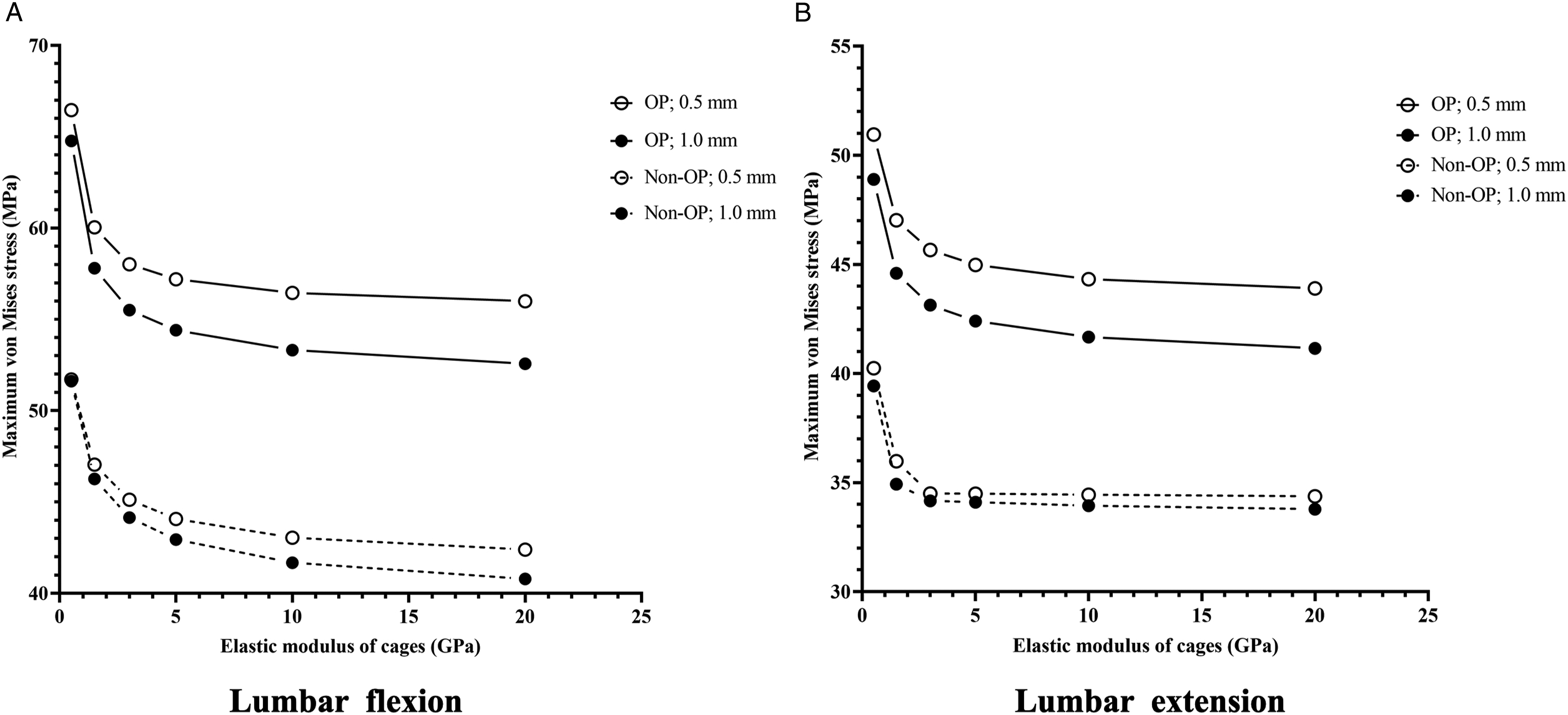
The results in Table 3 and Table 4 showed the maximum von Mises stress in the endplates decreased as the cage-E decreased in both OP and non-OP model. As illustrated in Figure 3, OP and thinner endplates are related to higher endplate stress under the conditions of different levels of cage-E. The maximum von Mises stress in the endplates of L4 and L5 with different Young’s modulus of cages. “OP/Non-OP; L4/L5; .5/1.0 mm” means “L4/L5 endplate with .5/1 mm-thick in the OP/Non-OP model”.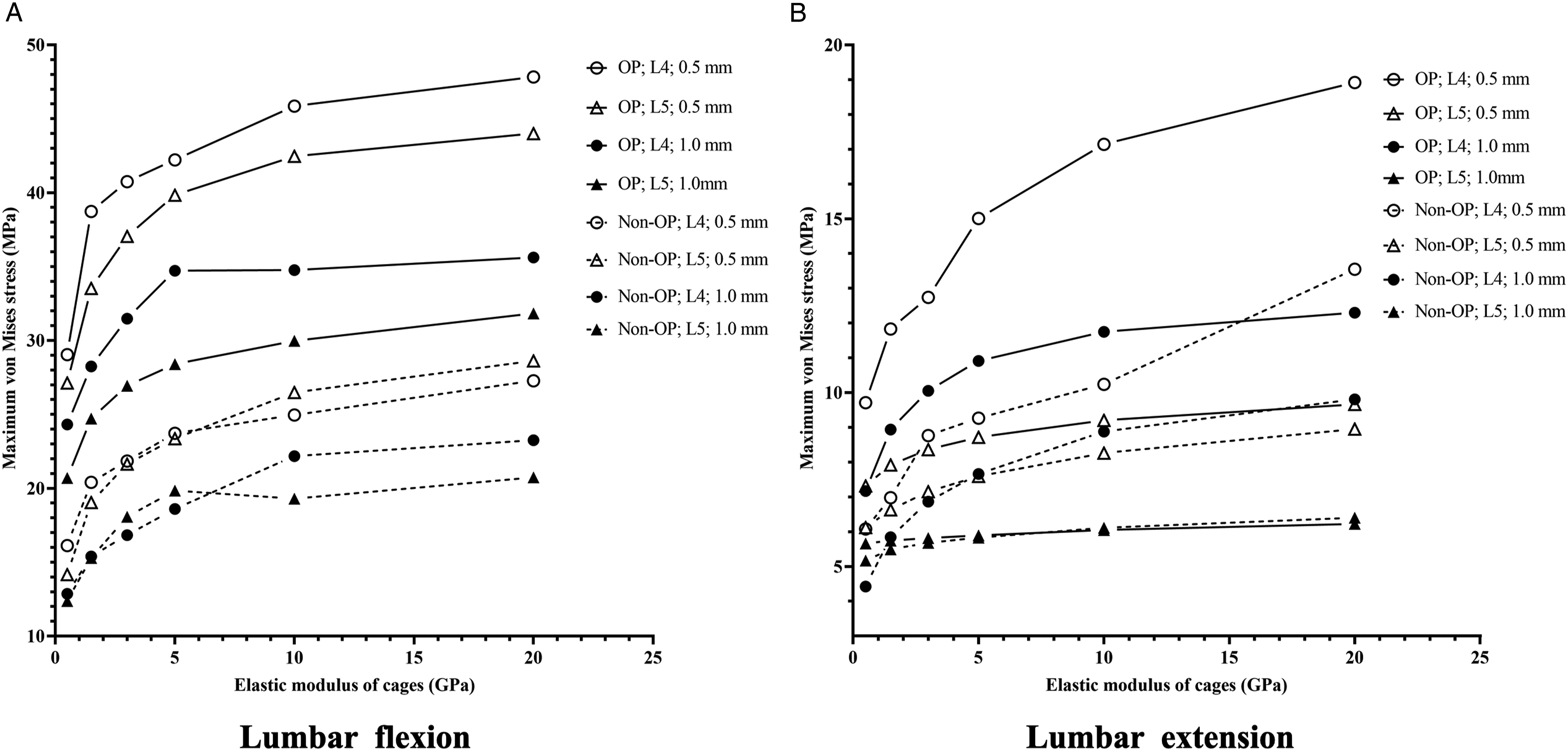
Effect of Cage-E on the Stress in the Lumbar Posterior Fixation
The maximum von Mises stress in the lumbar posterior fixation.
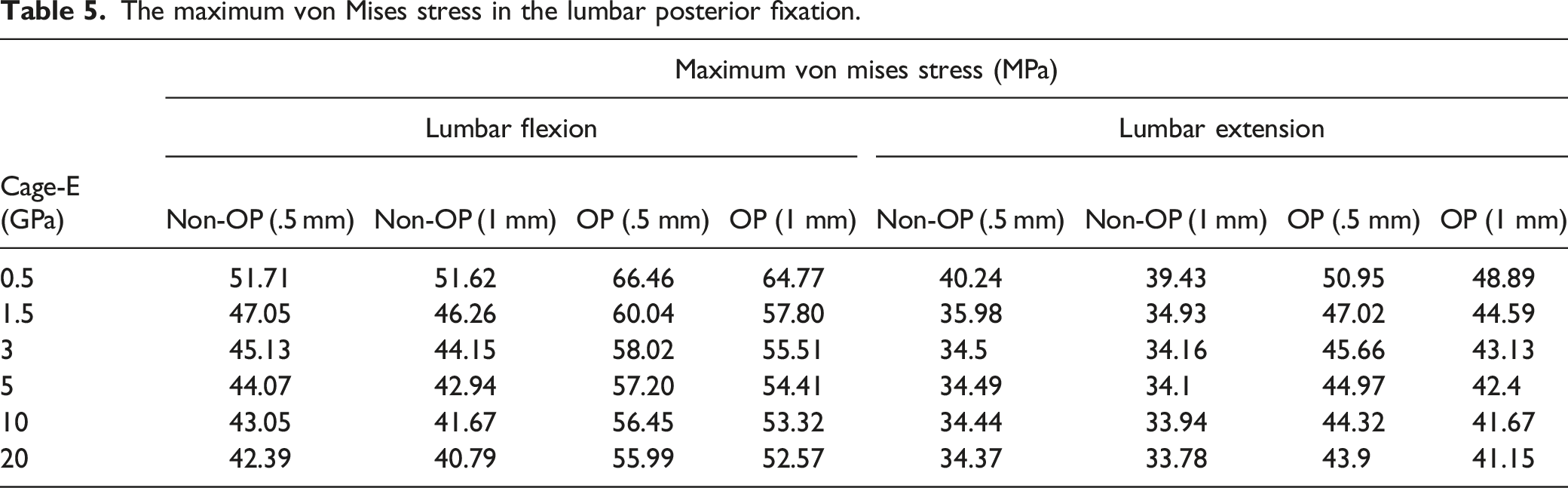
The maximum von Mises stress in the lumbar posterior fixation with different cage-E, different thicknesses of endplate and different bone conditions in the FE model. “OP/Non-OP; .5/1.0 mm” means “OP/Non-OP model with .5/1 mm-thick endplate”.
Discussion
FEA has been widely used to simulate the mechanical environment of lumbar interbody fusion with the insertion of interbody cages. However, previous studies have mostly established the FEA models of lumbar spine with normal BMD, few studies have focused on the condition of interbody fusion in osteoporotic lumbar spine.12,23 Cage subsidence is 1 of the serious complications worthy of attention in lumbar spine surgery. Various studies have reported that OP is an important risk factor of cage subsidence, and associates with poor clinical outcomes.24,25 Considering the worldwide rapid aging process, it is urgent to put more emphasis on the elderly patients with high risk of OP-related cage subsidence. This study explored the influence of OP, cage-E and endplate thickness on biomechanical behaviors of the bony endplates and posterior fixation system. The results can help spine surgeons understand the mechanism of cage subsidence in osteoporotic patients, and provide evidence for designing cages with low elastic modulus which matches the mechanical properties of osteoporotic bone.
For osteoporotic patients, the Young’s modulus generally decreased by 66% for cancellous bone and by 33% for cortical bone and bony endplates.12,23 In the 1990s, Mizrahi et al first proved that the decrease of bone modulus could significantly increase peak stress in endplates. 26 Lu et al also compared the FEA model of osteoporotic vertebral bone with normal bone, and found that the cortical shell stress was sensitive to the decrease of bone modulus during aging process. 12 However, their FEA models had no surgical implants like fusion cages. The results of current study revealed that endplate maximal stress increased by up to 100% in OP model compared to non-OP model, especially for L4 endplates under the condition of lumbar flexion. The cage-E was set to be 3 GPa when we performed the comparison between OP and non-OP model, because Young’s modulus of the most common cages used in clinical practice was about 3 GPa. 27 Therefore, the increase of endplate stress in osteoporotic bone explains part of the mechanism of OP-related cage subsidence.
The high modulus of certain kinds of fusion cages, such as titanium cages, is also the risk factor of cage subsidence. 11 PEEK cages are preferred by most spine surgeons because the modulus of PEEK cages is similar to that of normal bone, but they may not match the biomechanical properties of osteoporotic bone. The mismatch between the modulus of cages and that of the bony tissue may cause stress shielding effects and bone remodeling, thus increasing subsidence rate.28,29 A few previous studies found that endplate maximal stress significantly decreased as cage-E decreased,29,30 which was in agreement with our results. However, there studies only analyzed the non-OP model. Our work indicates that the decrease of cage-E can also reduce endplate stress in osteoporotic bone. Especially, the endplate maximal stress decreased sharply when the cage-E was of ≤1.5 GPa. Of note, we found that the side effect of reducing cage-E was increasing the stress in posterior fixation system, which was also observed by Lu et al. 29 The high stress in fixation system is the risk factor of postoperative complications like pedicle screw loosening. Thus, it is important to keep the balance between reducing cage subsidence risk and maintaining the fixation strength.
The bony endplates have direct contact with fusion cages and therefore play a significant role in supporting the cages. Apart from the elastic modulus of bony endplates, the endplate thickness also decreases in aging and bone loss process. 31 Furthermore, the endplate thickness varies among different positions of the same endplate and different endplates of different vertebral levels. 32 In literature of FEA, the endplate thickness ranges from .5 mm to 1 mm.12,22,29 The effect of endplate thickness on endplate stress in interbody fusion system is still unknown. In this regard, this study found that thinner endplate was associated with higher endplate stress. Therefore, the endplate thickness in the planned position of cage also needs to be assessed when we evaluate the cage subsidence risk.
There are several limitations of our work. First, the shape and size of cages and fixation implants may also influence the stress in cage-endplate interface, we did not include such variables in the analysis. Second, there is no standard FEA model for osteoporotic lumbar spine, the FEA models in our study are unable to represent the patients with various degrees of osteoporosis. Third, considering that lumbar flexion-extension is the most common daily actions, and the endplate stress reaches a maximum in flexion position, 19 we only simulated the lumbar flexion-extension postures. The loading conditions of lateral bending and axial rotation were not analyzed. Forth, the FEA model is only a simplified system used to simulate the human body environment, more in vitro biomechanical tests and clinical research are needed to verify the effect of using cages with low elastic modulus. Lastly, many other material properties of cages are related to their performance in interbody fusion, such as the compressive strength. We should guarantee that the cages have enough compressive strength to prevent cage broken when reducing the cage-E.
In conclusion, this study reveals that higher endplate stress in osteoporotic condition is the possible mechanism of OP-related cage subsidence. Lower cage-E is associated with lower endplate stress. In this case, it is reasonable to design BMD-matched or modulus-matched cages for osteoporotic patients. One kind of BMD-matched cage has been reported in recent literature. 33 Such cages are designed to match the BMD T-score measured by dual energy x-ray absorptiometry (DXA), but it has been reported that DXA results are less accurate than BMD measured by CT Hounsfield units (HU) in older patients requiring lumbar fusion.5,34 Instead, we propose to design customized cages matching the biomechanical properties of patients with various degrees of osteoporosis measured in CT HU (mild OP:≤110HU; severe OP: 50-80 HU; extremely severe OP:≤50HU).35,36 In future, the biomechanical-matched cages may benefit more older patients. Besides, thinner endplate can also lead to higher risk of cage subsidence, we should pay attention to endplate thickness assessment when we design customized cages and choose where to place the cages.
Supplemental Material
Supplemental Material - Biomechanical Analysis of Lumbar Interbody Fusion Cages With Various Elastic Moduli in Osteoporotic and Non-osteoporotic Lumbar Spine: A Finite Element Analysis
Supplemental Material for Biomechanical Analysis of Lumbar Interbody Fusion Cages With Various Elastic Moduli in Osteoporotic and Non-osteoporotic Lumbar Spine: A Finite Element Analysis by Da Zou, MD, Lihao Yue, BS, Zheyu Fan, BS, Yi Zhao, BS, Huijie Leng, PhD, Zhuoran Sun, MD, and Weishi Li, MD in Global Spine Journal
Supplemental Material
Supplemental Material - Biomechanical Analysis of Lumbar Interbody Fusion Cages With Various Elastic Moduli in Osteoporotic and Non-osteoporotic Lumbar Spine: A Finite Element Analysis
Supplemental Material for Biomechanical Analysis of Lumbar Interbody Fusion Cages With Various Elastic Moduli in Osteoporotic and Non-osteoporotic Lumbar Spine: A Finite Element Analysis by Da Zou, MD, Lihao Yue, BS, Zheyu Fan, BS, Yi Zhao, BS, Huijie Leng, PhD, Zhuoran Sun, MD, and Weishi Li, MD in Global Spine Journal
Supplemental Material
Supplemental Material - Biomechanical Analysis of Lumbar Interbody Fusion Cages With Various Elastic Moduli in Osteoporotic and Non-osteoporotic Lumbar Spine: A Finite Element Analysis
Supplemental Material for Biomechanical Analysis of Lumbar Interbody Fusion Cages With Various Elastic Moduli in Osteoporotic and Non-osteoporotic Lumbar Spine: A Finite Element Analysis by Da Zou, MD, Lihao Yue, BS, Zheyu Fan, BS, Yi Zhao, BS, Huijie Leng, PhD, Zhuoran Sun, MD, and Weishi Li, MD in Global Spine Journal
Footnotes
Acknowledgment
We thank Xinyu Li and Shengqiang Liu at Beijing AKEC Medical Company Ltd For their valuable input on the FEA model for this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Natural Science Foundation of China (Grant No.82202779), and the Research and Application of Clinical Diagnosis and Treatment Technology Foundation of Beijing (Grant No. Z201100005520073).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.