
Abstract
Study Design
Retrospective cohort study.
Objective
The primary objective was to evaluate the impact of the upper instrumented level (UIV) being at C2 vs C3 in posterior cervical construct on patient reported outcomes (PROs) up to 24 months after surgery for cervical degenerative myelopathy (DCM). Secondary objectives were to compare operative time, intra-operative blood loss (IOBL), length of stay (LOS), adverse events (AEs) and re-operation.
Methods
Patients who underwent a posterior cervical instrumented fusion (3 and + levels) with a C2 or C3 UIV, with 24 months follow-up were analyzed. PROs (NDI, EQ5D, SF-12 PCS/MCS, NRS arm/neck pain) were compared using ANCOVA. Operative duration, IOBL, AEs, and re-operation were compared. Subgroup analysis was performed on patient presenting with pre-operative malalignment (cervical sagittal vertical axis ≥40 mm and/or T1slope- cervical lordosis >15°).
Results
173 patients were included, of which 41 (24%) had a C2 UIV and 132 (76%) a C3 UIV. There was no statistically significant difference between the groups for the changes in PROs up to 24 months. Subgroup analysis of patients with pre-operative malalignment showed a trend towards greater improvement in the NDI at 12 months with a C2 UIV (P = .054). Operative time, IOBL and peri-operative AEs were more in C2 group (P < .05). There was no significant difference in LOS and re-operation (P > .05).
Conclusion
In this observational study, up to 24 months after surgery for posterior cervical fusion in DCM greater than 3 levels, PROs appear to evolve similarly.
Keywords
Introduction
Degenerative cervical myelopathy (DCM) is 1 of the most common causes of nontraumatic spinal cord impairment.1-5 Multiple prospective studies have reported that spinal cord decompression in DCM improves patient’s functional and neurological outcomes.6-8 Cervical spine posterior decompression and instrumented fusion plays a major role in the treatment of DCM. The goal of the surgery is adequate spinal cord decompression while maintaining or obtaining satisfactory alignment. Despite the high number of posterior cervical decompression and fusion surgeries performed every year, questions regarding the optimal surgical technique remain, especially surrounding the choice of upper and lower instrumented levels.
Multiple factors are considered when selecting the cephalad and caudad fixation levels in a posterior cervical fusion. These include levels of spinal cord compression, degenerative changes, bone quality, the presence of a mal-alignment and patient-specific anatomy. Most of the literature has focused on the impact of the lower instrumented vertebra (LIV) in posterior cervical fusion.9-12 Recent studies have shown that ending the construct in the cervico-thoracic junction does not negatively impact the Patient-reported outcomes (PROs).9,10 Proponents of thoracic LIV report a lower rate of distal adjacent level disease. 12 Conversely, little has been reported on the upper instrumented level. Ending the proximal construct at C2 has the advantage of 3 column stability and substantial segmental control in both cadaveric and clinical studies. 13 On the other hand, fixation in the subaxial cervical spine is technically simple, associated with less bleeding and risk to the vertebral artery, and does not require sophisticated image guidance.
There is a lack of consensus in the existing literature regarding the choice of the upper instrumented level. Using the DCM prospective multicentric Canadian observational cohort, the primary objective of this study was to evaluate the impact of ending the construct proximally at C2 vs C3 on PROs (NDI, EQ-5D, PCS-12, MCS-12) for patients undergoing multilevel posterior instrumented fusion (≥3 levels) up to 24 months after surgery (3-12 and 24 months). Secondary objectives were to evaluate change in modified Japanese Orthopaedic Association (mJOA) rating, to compare operative time, length of stay (LOS), satisfaction, adverse-event occurrence, and re-operation between the 2 groups. Lastly, we sought to compare the percentage of patients reaching minimally clinical importance difference in PROS and mJOA up to 24 months.
Methods
Study Design
In this retrospective analysis, the data used was collected prospectively from an on-going multicenter observational cohort study of patients with DCM. Since January 2015, nine participating centers from the Canadian Spine Outcomes and Research Network (CSORN) have been enrolling consecutive patients with a clinical diagnosis of DCM and confirmed evidence of compressive pathology on imaging. CSORN is a Canadian Research Network that monitors the outcomes of spine surgery across 22 centers and includes over 75 Neurosurgeons and Orthopaedic spine surgeons. Standardized data collection pre-operatively and at specific post-surgical time points was performed by trained research assistants. Local research ethics board was obtained at each center prior to data collection (IRB approval number H22-00699). Informed consent was not required as per IRB for CSORN.
Patient Sample
Patients enrolled in the CSORN-DCM observational cohort between January 2015 and October 2020 who were greater than 18 years old, who underwent a multilevel posterior cervical decompression and fusion (≥3 levels) with the UIV being either C2 or C3 and who have reached the 24 months post-operatively were included. Patients who underwent a fusion of less than 3 levels, had a UIV other than C2 or C3, a non-fusion procedure (decompression alone or laminoplasty), a revision surgery, a major deformity correction surgery requiring either a combined approach or a cervical osteotomy, and patients who had not yet reached 24 months post-operatively were excluded from this study. Enrolled patients were divided according to the UIV of their construct in two groups, 1) C2 UIV and 2) C3 UIV.
Patient, Clinical, and Surgical Variables Considered
Patient variables (age, gender, number of comorbidities, tobacco use, education level, marital status, body mass index (BMI), pain medication use, symptom duration, working status, province of surgery, and active worker or insurance claim information) were collected prospectively. These variables were self-reported by the patient at baseline. Surgical variables considered were the UIV and LIV, the number of levels instrumented and/or decompressed. Presence of pre-operative T1 and/or T2 cord signal change on the magnetic resonance imaging was recorded. At baseline, the C2-C7 angle (negative values indicate lordosis and positive values, kyphosis), T1 Slope and the cervical sagittal vertical axis (cSVA) were measured on upright cervical radiographs (Figure 1). Malalignment was defined by a pre-operative cSVA ≥40 mm and/or T1 slope- cervical lordosis >15°.
14
Lateral cervical spine radiograph illustrating radiologic measurements of malalignment.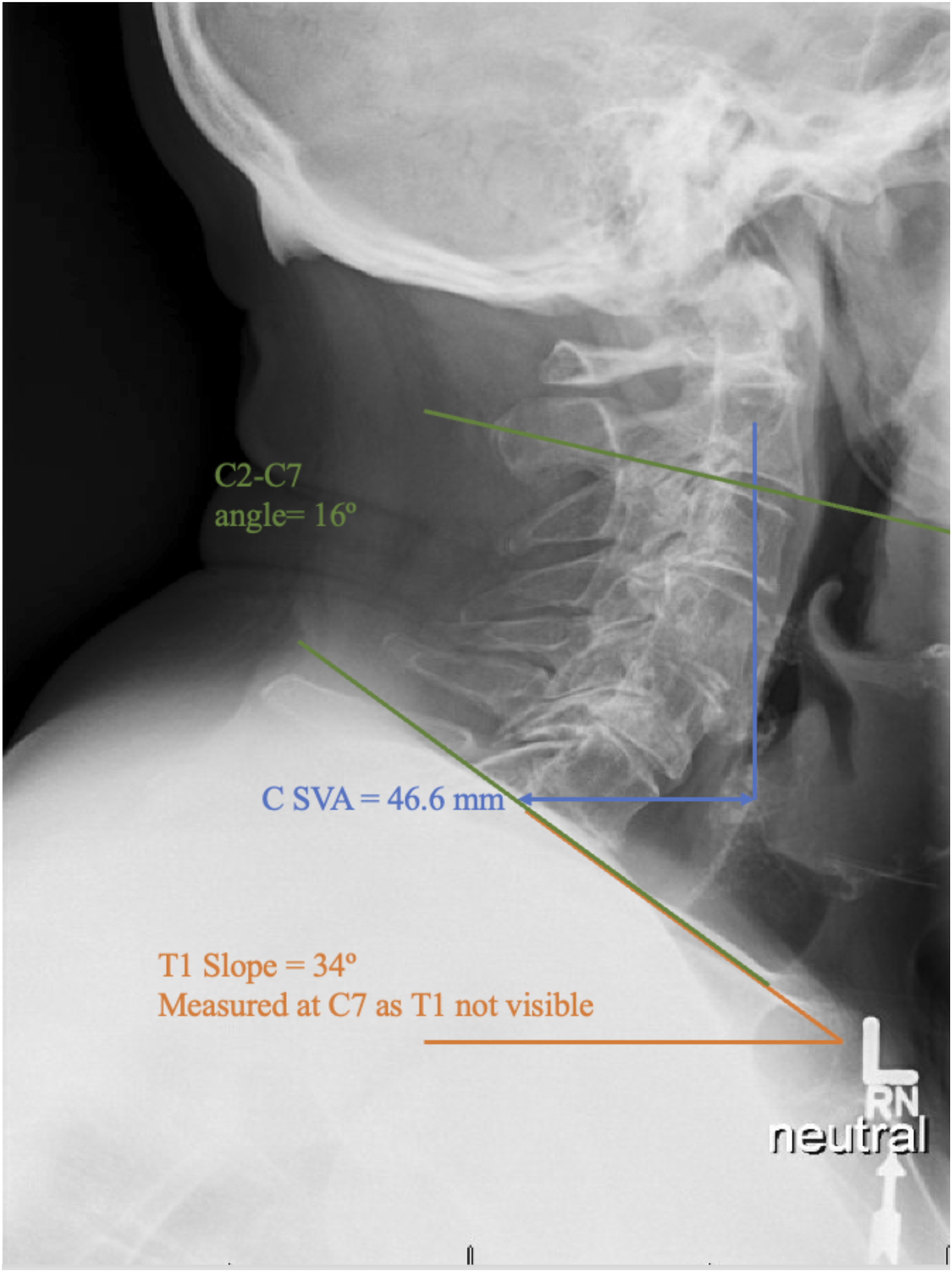
Outcome Measures
Patient reported outcomes included Neck Disability Index (NDI), EuroQol-5D (EQ-5D), the Short Form (SF-12) Survey Physical Component Score (PCS) and Mental Component Score (MCS) and the neck and arm pain numeric rating scale (NRS neck and arm). Analyses were focused on change in PROs between pre-op to 12 months post-op with secondary outcome endpoints of 3 and 24 months post-op also considered.
Additional outcomes considered included operative time duration, intra-operative blood loss, LOS, intra-operative and peri-operative (AEs), satisfaction and re-operation up to 24 months after surgery. Adverse events were collected prospectively using The Spine Adverse Event Severity System (SAVES). 15 Neurological impairment at baseline was assessed using the modified Japanese Orthopaedic Association (mJOA) score and classified based on its severity (severe: mJOA 0-11, moderate: mJOA 12-14, mild: mJOA15-17). 16
To determine the percentage of patient achieving the minimum clinically important difference (MCID), the threshold used were: 7.5 points for the NDI, 17 2.5 points for the NRS neck and arm pain, 17 4 points for the SF-12 PCS and MCS 18 and .0485 points for the EQ-5D. 19 The MCID for the mJOA score changes based on the baseline disease severity: 3, 2 and 1 point changes were required in patients with severe disease, moderate disease, and mild disease, respectively. 16
Statistical Methods
Baseline demographics, radiologic measurement, surgical details, pre-operative PROs and mJOA were compared between the 2 groups using chi-square test for categorical variables and independent samples t-tests for continuous variables.
Mean values for each outcome measure were calculated for the entire cohort and for each group (C2 UIV and C3 UIV) at baseline, 3,12 and 24-months post operatively. Within group mean values at each of these time points were compared to baseline using paired sample t-tests; between group mean values were assessed using analysis of covariance (ANCOVA), adjusting for baseline significant differences between the 2 groups (province of surgery and symptoms duration). A subgroup analysis was performed for patients presenting with pre-operative malalignment.
Assessment of a clinically significant improvement at each time point was measured on the selected MCID for each outcome measures. Responder analysis for each group was performed by calculating the proportion of patients who met the MCID for each outcome measure. These proportions were compared between the 2 groups using chi-square tests. A subgroup analysis was performed for patients presenting with pre-operative malalignment. A multivariable logistic regression analysis was performed for predictors of reaching MCID of 7.5 point for the NDI at 12 months. Variable included in the model were: age, presence of malalignment, baseline NDI, symptom duration and the UIV. The variables included in the model were assessed for collinearity.
A P-value <.05 (2 tailed) was considered statistically significant for all tests. Analyses were conducted with IBM SPSS for Windows release 28.
Results
A total of 173 patients were included in this study (Figure 2). Of these, 41 patients (24%) had a UIV at C2 and 132 (76%) had the UIV at C3. The follow-up rate was 83% and 70% at 12 and 24 months. The baseline characteristics did not differ between those who were lost to follow-up and those who completed the 24 months follow-up. Flowchart of patient enrollment. UIV, Upper Instrumented Vertebra.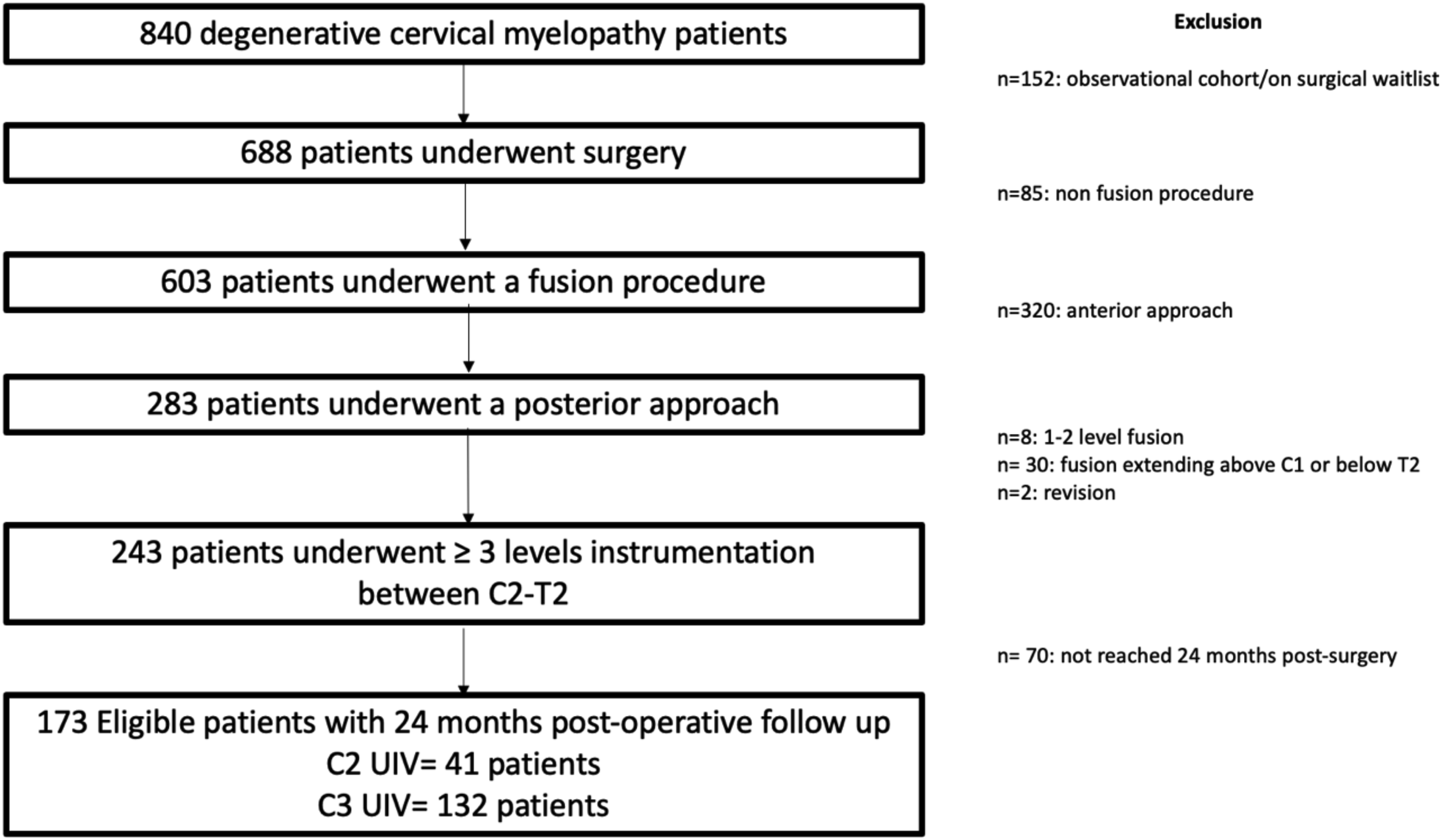
Mean age was 64 (SD 9.9) and most patients were male (71%). Symptoms duration >2 year (P < .024) and surgery done in western provinces (P < .001) were significantly more prevalent in the group with C3 UIV. Other baseline demographic variables were not statistically different between the groups. There was no significant difference between the groups in the baseline PROs and mJOA (P > .05).
Cohort Characteristics.
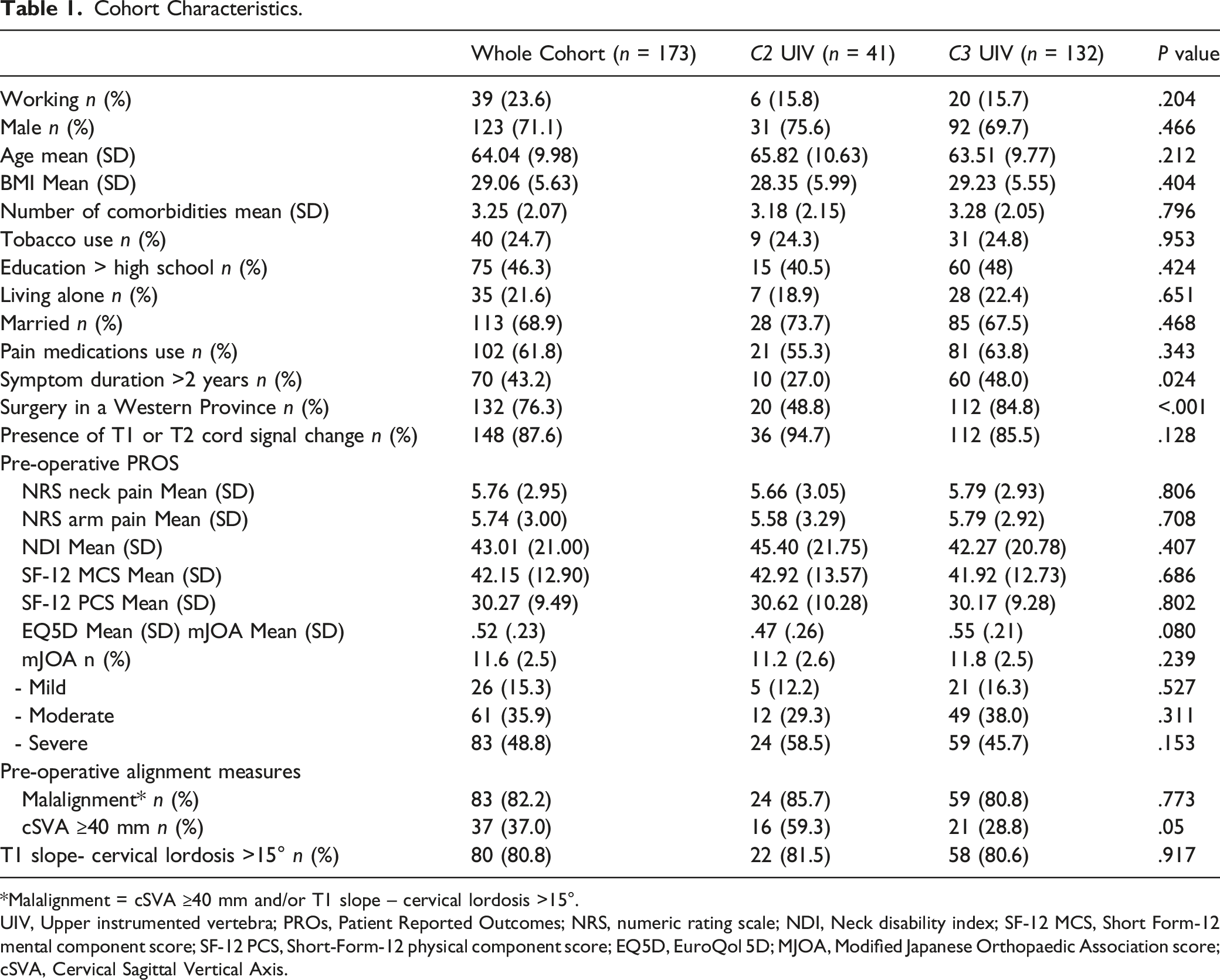
*Malalignment = cSVA ≥40 mm and/or T1 slope – cervical lordosis >15°.
UIV, Upper instrumented vertebra; PROs, Patient Reported Outcomes; NRS, numeric rating scale; NDI, Neck disability index; SF-12 MCS, Short Form-12 mental component score; SF-12 PCS, Short-Form-12 physical component score; EQ5D, EuroQol 5D; MJOA, Modified Japanese Orthopaedic Association score; cSVA, Cervical Sagittal Vertical Axis.
Descriptive table of the proximal and distal Instrumentation vertebra.
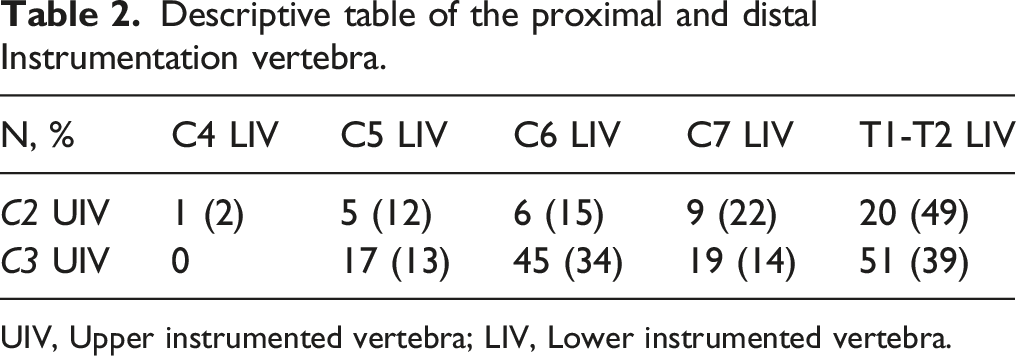
UIV, Upper instrumented vertebra; LIV, Lower instrumented vertebra.
Primary Outcome
Within groups, PROs (NRS neck pain, arm pain, NDI, EQ5D, SF-12 MCS and PCS) improved significantly from baseline to 3, 12 and 24 months post-operatively (P < .001). At 12 months, the mean change in the NDI was −17.26 (SD 3.74) for the C2 UIV group vs −9.44 (SD 2.36) for the C3 UIV group (P < .079). The PCS improved by a mean of 6.58 points (SD 2.77) in the C2 UIV cohort compared to 3.56 (SD 1.48) for the C3 UIV cohort at 12 months (P = .343). Up to 24 months after surgery, no significant difference in PROs was observed between the 2 groups (Figure 3). Patient Reported Outcomes and modified Japanese Orthopaedic Association scores at baseline, 3, 12, and 24 months. cSVA, Cervical Sagittal Vertical Axis; UIV, Upper Instrumented Vertebra.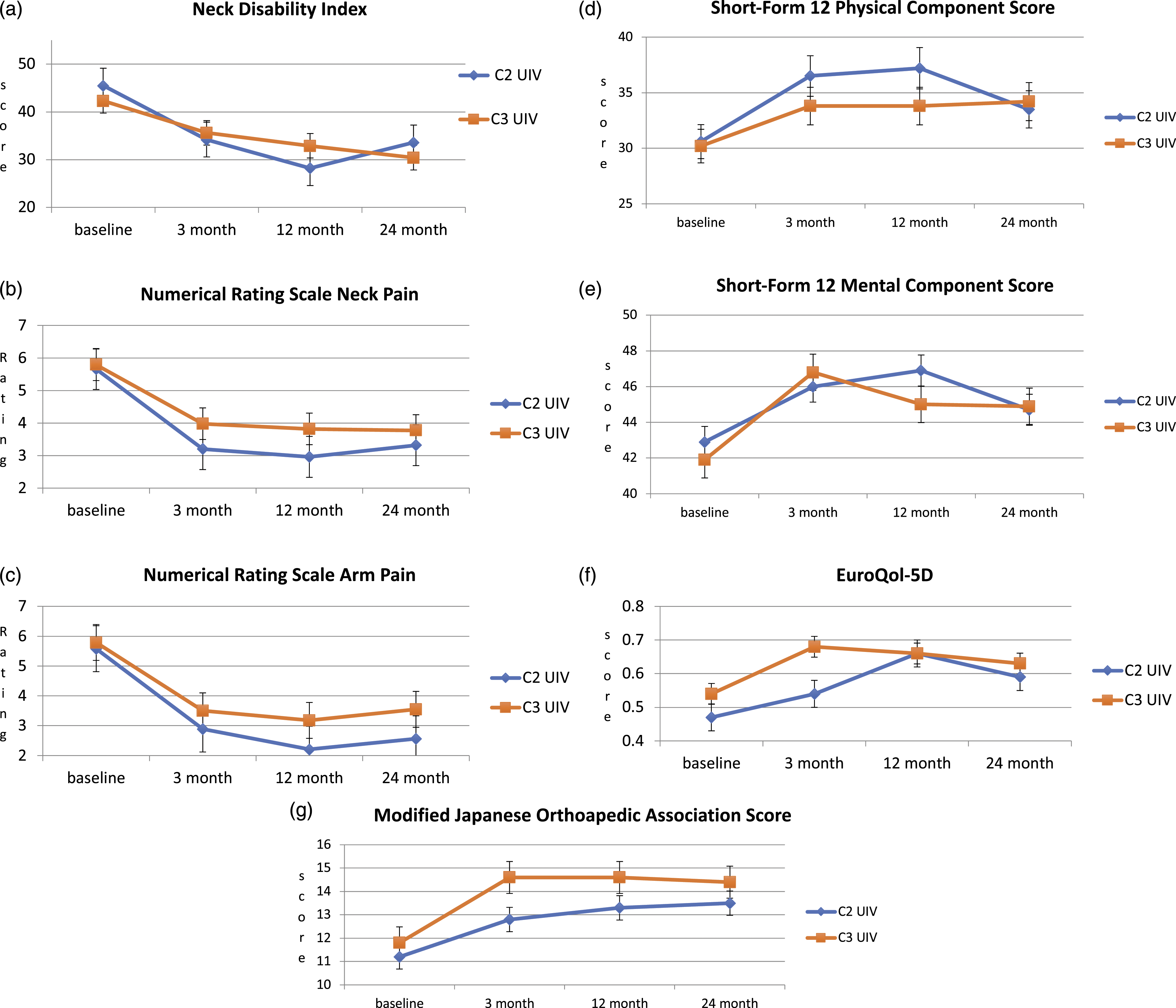
A subgroup analysis of 83 patients presenting with pre-operative malalignment showed that the EQ-5D at 3 months was worse in the C2 UIV cohort (−.09 vs .12, P = .043). This association was lost at further follow-up. At 12 and 24 months, patients with a C2 UIV had a trend towards greater improvement in the NDI compared to the patient with a C3 UIV: −20.21 (5.51) vs −6.49 (3.67), P = .054 and −18.25 (6.13) vs −6.52 (3.73), P = .134. Similar trends were observed with the NRS neck pain, PCS and the EQ5D (P > .05) (Figure 4). Subgroup analysis of patients presenting with malalignment (cSVA ≥40 mm and/or T1 slope – cervical lordosis >15°): Patient Reported Outcomes and modified Japanese Orthopaedic Association scores at baseline, 3, 12, and 24 months. cSVA, Cervical Sagittal Vertical Axis; UIV, Upper Instrumented Vertebra.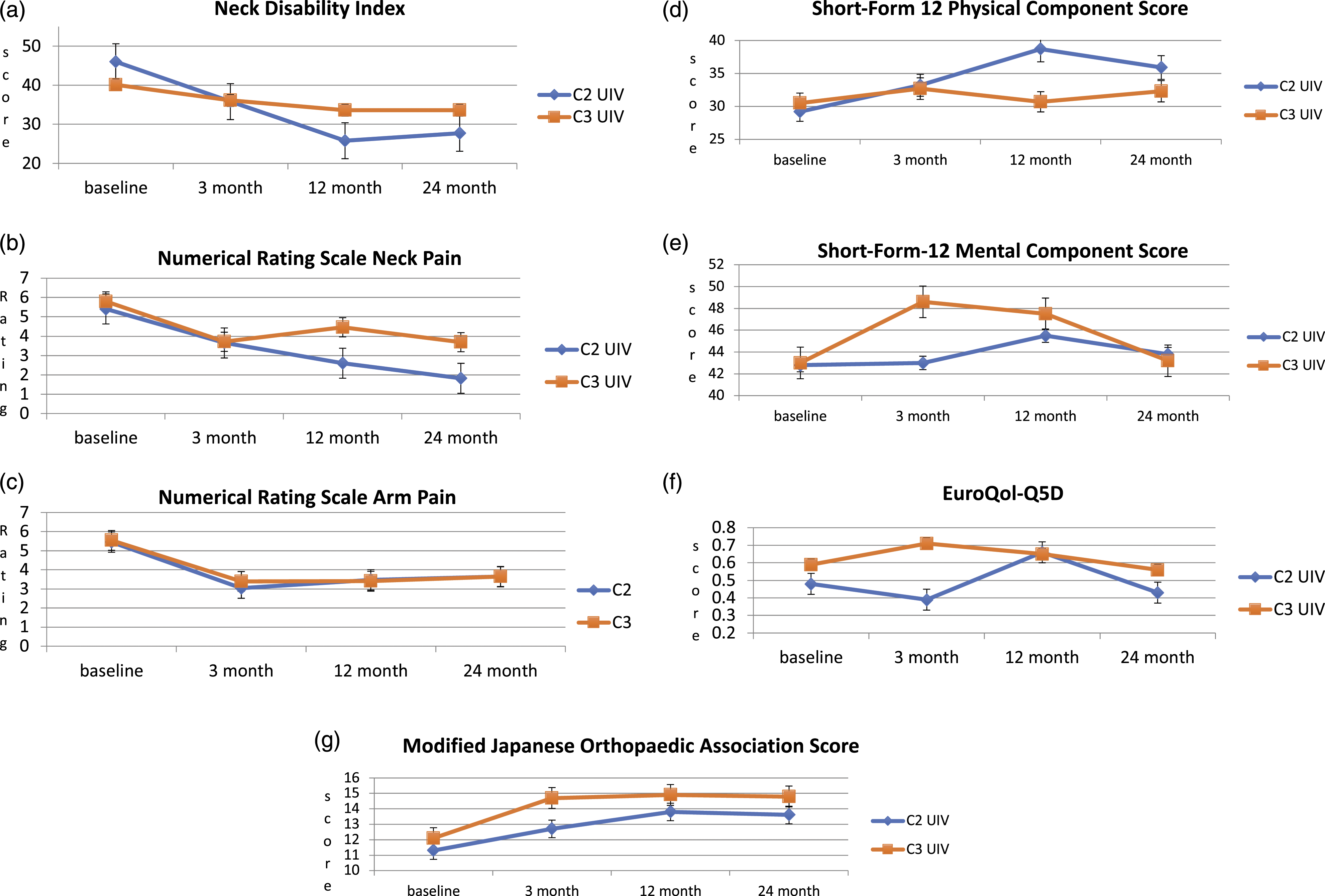
Secondary Outcomes
Secondary outcomes.
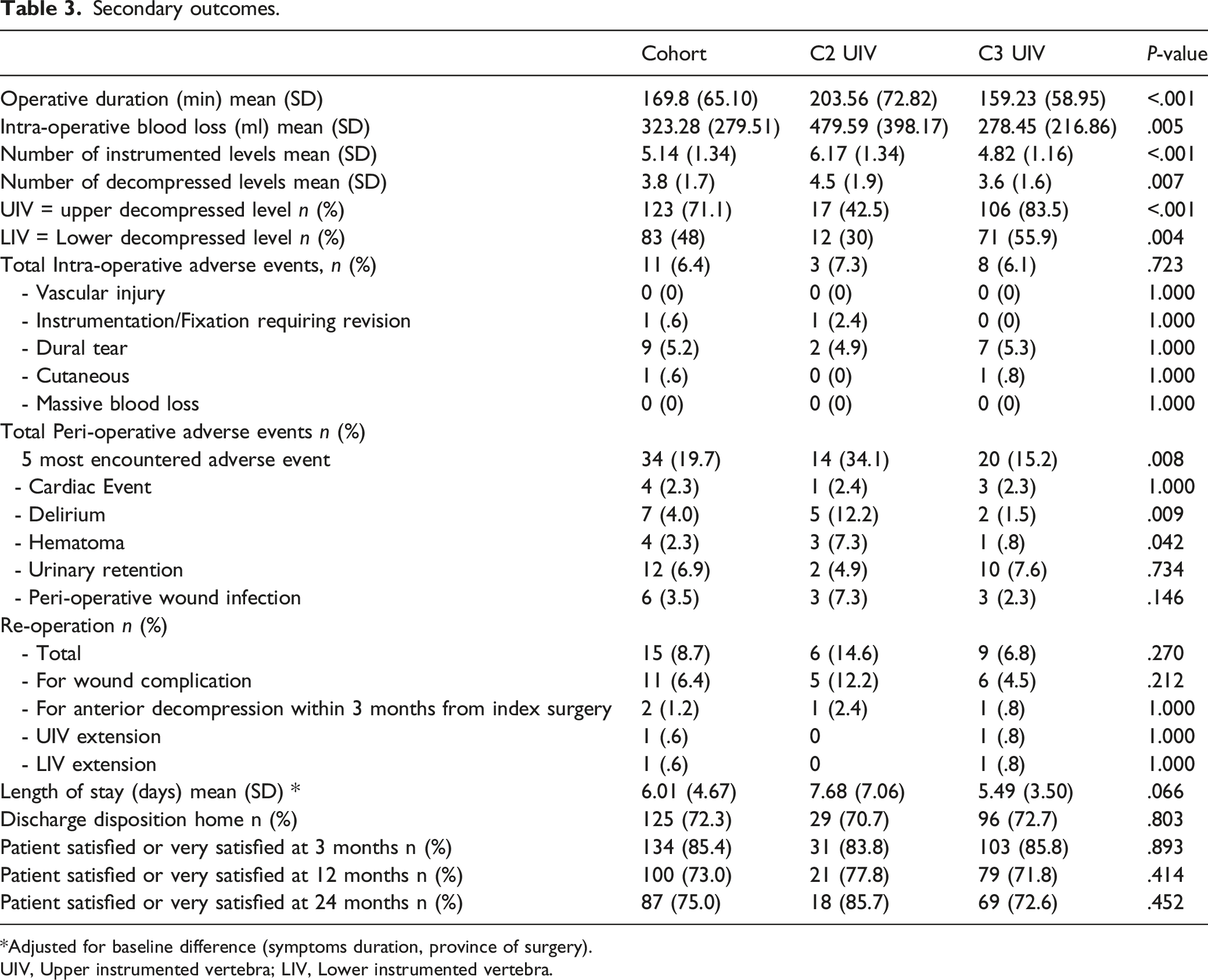
*Adjusted for baseline difference (symptoms duration, province of surgery).
UIV, Upper instrumented vertebra; LIV, Lower instrumented vertebra.
Up to 24 months after surgery, there were 15 re-operations: 6 in the C2 UIV group and 9 in the C3 UIV group (P = .270). Ten patients had a wound complication requiring 11 returns to the operative room (5 in C2 UIV and 6 C3 UIV, P = .212). One patient in each group underwent an anterior decompression within 3 months of the initial surgery. Two patients with a C3 UIV underwent an extension within 2 years (1 proximal and 1 distal). No patients in the C2 UIV group required an extension.
Within groups, mJOA improved significantly from baseline to 3, 12 and 24 months post-operatively (P < .001). When adjusted for baseline difference (symptoms duration, province of surgery), there was a significant difference in the mJOA score at 3 months, favoring the C3 UIV group (P < .019) (Figure 2).
Patients reaching the minimally clinically important difference in Patient Reported Outcomes and Modified Japanese Orthopaedic association scores.
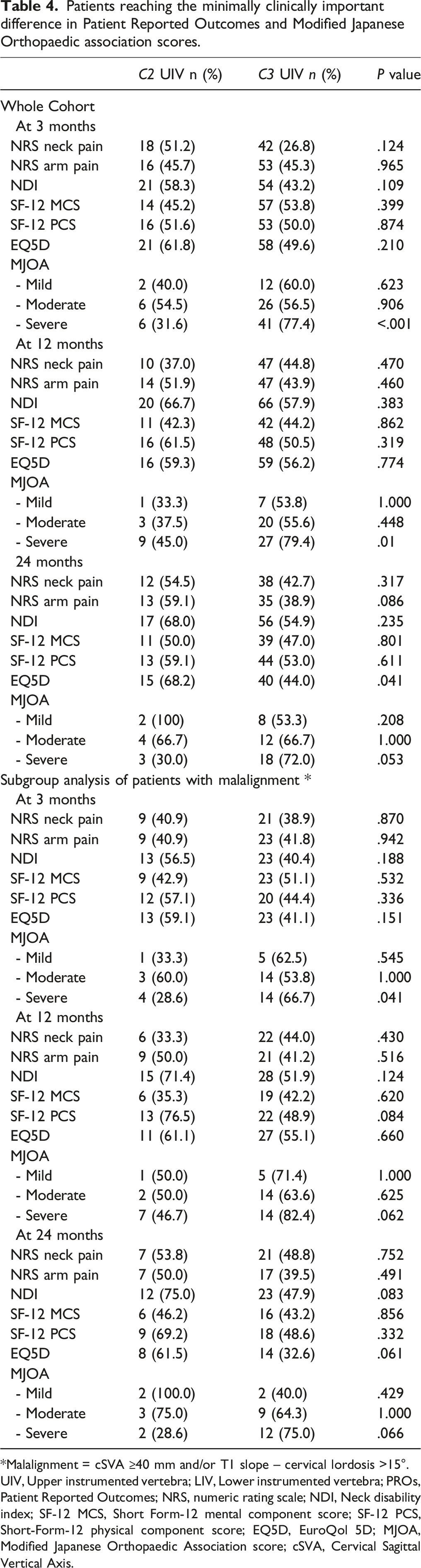
*Malalignment = cSVA ≥40 mm and/or T1 slope – cervical lordosis >15°.
UIV, Upper instrumented vertebra; LIV, Lower instrumented vertebra; PROs, Patient Reported Outcomes; NRS, numeric rating scale; NDI, Neck disability index; SF-12 MCS, Short Form-12 mental component score; SF-12 PCS, Short-Form-12 physical component score; EQ5D, EuroQol 5D; MJOA, Modified Japanese Orthopaedic Association score; cSVA, Cervical Sagittal Vertical Axis.
Multivariable logistic regression model for predictive factors of reaching the minimally clinical important difference of 7.5 points for the Neck Disability Index at 12 months.
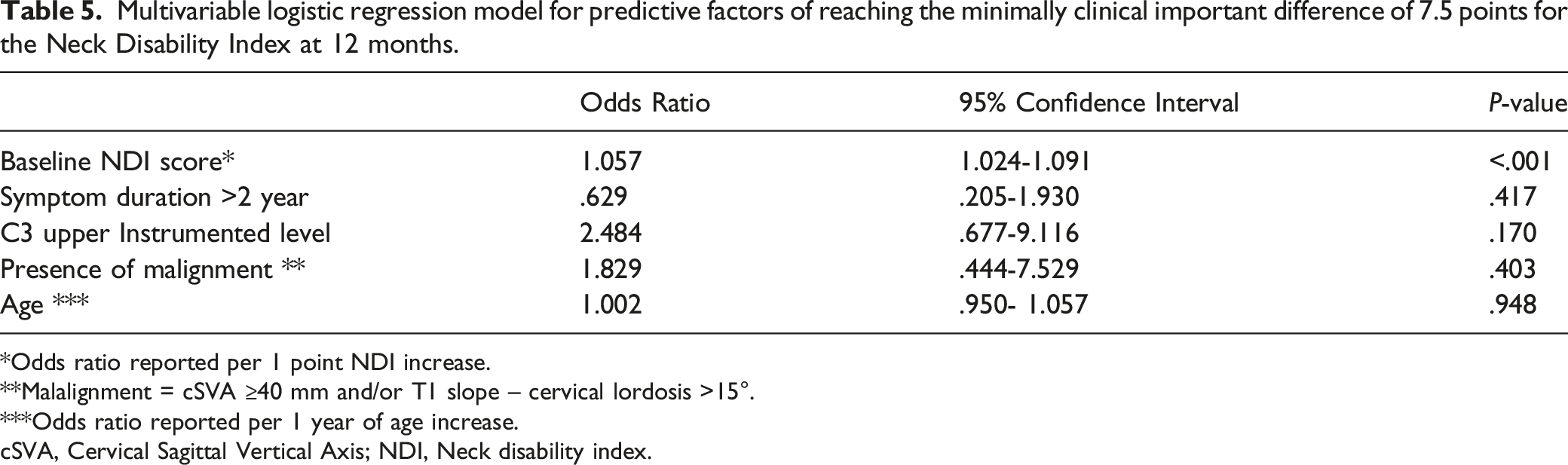
*Odds ratio reported per 1 point NDI increase.
**Malalignment = cSVA ≥40 mm and/or T1 slope – cervical lordosis >15°.
***Odds ratio reported per 1 year of age increase.
cSVA, Cervical Sagittal Vertical Axis; NDI, Neck disability index.
Discussion
This study is the largest study in the current literature comparing C2 to C3 UIV in cervical posterior decompression and fusion in the setting of DCM. Up to 24 months after surgery, when adjusting for the baseline difference, there was no statistically significant difference in the PROs between the C2 and C3 UIV. At 3 months post-operatively, the patients with a C3 UIV had greater improvement in the mJOA, but that difference did not persist at 12 and 24 months. Operative time was longer and intra-operative blood loss was greater in the patients with a C2 UIV. This can be explained by the additional dissection required to instrument C2 and by the fact that patients who had a C2 UIV generally had more levels instrumented than patients who had a C3 UIV. The rate of intra-operative AEs did not differ but the C2 UIV group had a greater rate of peri-operative AES. Patients who presented with baseline malalignment showed a trend toward a greater improvement in the NDI score at 12 months when a C2 UIV was chosen.
While there is an abundant literature on the distal instrumented level in posterior instrumented fusion, there is a limited number of reports on the upper level of fixation, mainly focused on the biomechanical aspects.13,20,21 The biomechanical superiority of C2 has been used to justify the additional surgical time and dissection. Recently, Roth et al compared C2 UIV to C3/C4 UIV in a cohort of one hundred and seventeen patients. 22 Similar to our cohort, there was no difference in the PROs between the 2 groups at 1 year following surgery. Longer operative time but no difference in estimated blood loss was observed for the C2 UIV cohort. Our study adds to this literature by providing a larger cohort and adding pre-operative radiologic measures of malignment.
Traditionally, the focus of the literature in the DCM population has been around the neurologic outcomes but recently cervical alignment has been getting more attention. 23 High cSVA has been associated with worse NDI in the cervical deformity population. 24 Additional measures such as the T1 slope minus cervical lordosis has been added to the cervical deformity definition. 14 Other measures like the chin brow angle are not captured in the CSORN-DCM study. Using the cSVA and the T1 slope-CL measures, we are reporting that cervical mal-alignment is prevalent in the DCM population. Patients with a combined antero-posterior approach were excluded of the analysis which is suggesting that patients with severe kyphotic deformity were excluded. Despite this, 80 out of 101 patients with available pre-operative radiologic measures had malalignment. In a cervical deformity population, Passias et al reported improved horizontal gaze at 1 year in patients with a C2 UIV compared to a subaxial 1. 25 Woodrofe et al reported increased post-operative cSVA and T1 slope in patients who had C2 UIV compared to a subaxial UIV. 26 Two limitations of this study were that the pre-operative radiologic measures were missing for a significant portion of the cohort and post-operative alignment measures were not available.
The subgroup analysis of patient with malalignment showed that the NDI improvement at 12 months was 3 times better if the UIV was C2 but this was not statistically significant (P = .054). Similar trends were observed with the PCS, NRS neck pain and EQ-5D, although these differences did not reach statistical significance. Considering the effect size difference, this may be explained by a lack of power related to the small sample size, rather than a true lack of significance. While preoperative surgical planning algorithms for cervical spine deformity correction surgery exist in the literature, little emphasis is placed on the optimal fusion length and upper instrumented vertebra UIV.27-30
In surgeries where the C3 was the UIV, the lamina of C3 was removed in over 80% of the time whereas the C2 lamina was removed roughly 40% of the time in the C2 UIV group. The theorical advantage of preserving the upper lamina and superior ligament attachment is to prevent junctional kyphosis and decrease adjacent level disease. The impact of having the UIV and upper decompressed level the same yet remains to be determined. In this series, only 1 patient in the C3 UIV (.8%) had to be extended to C2 within 2 years of the surgery and in that case, the C3 lamina was removed during the index surgery. This rate of proximal re-operation with the C3 UIV compares favorably with the 5% re-operation for proximal junctional failure rate at a minimum of 12 months of follow-up. 31
The impact of the spinal cord decompression on the neurologic outcomes has been the focus of many studies.6,8 As expected, patients myelopathic symptoms (mJOA) improved with decompressive surgery. The C3 UIV patients had greater improvement in the mJOA at 3 months and were more likely to reach MCID at 3 and 12 months than the C2 UIV patients. Predictive factors of poor neurologic outcomes following surgery such as age, symptoms duration and the severity of the myelopathy were not different between the groups. 32 There was no statistically significant difference in the number of patient presenting with T1 and/or T2 cord signal change between the groups. While T1 cord signal change on pre-operative MRI has been associated with poor outcomes, the registry does not differentiate between T1 or T2 associated changes and their grading. 33 Lastly, this study did not assess the quality of the decompression.
This study has several limitations. We are reporting that in carefully selected patient, PROS evolves similarly whether the UIV is C2 or C3. Because this is an observational study, the level of fixation and decompression were chosen by the attending surgeon. It is unknown whether the extent of the construct to C2 or to the cervico-thoracic junction was a result of cervical alignment, extent of spinal stenosis, or surgeon preference, for example. This study examined several clinical and radiological variables but other factors such as presence of pre-existing osteoporosis diagnosis or fragility fracture, extent of the degenerative changes and presence of instability are not captured in the database and might have impacted the choice of the upper fixation level. The type of fixation performed in C2 (pars, pedicle, laminar screws) was not recorded in our database. However, a recent study did not show difference in PROs associated with the choice of fixation. 22 While this study is the largest in the literature to date, it has a small sample size and will need to be validated with larger cohort to improve statistical power. Longer term follow-up and post-operative radiologic measures will be required to determine the longevity of the construct and the ability to achieve optimization of the alignment.
Conclusion
Up to 24 months after surgery for posterior cervical fusion in DCM ≥3 levels, PROs change is similar in patients having a C2 or C3 UIV. Increased operative time, estimated blood loss and peri-operative adverse events were more common with a C2 UIV construct. Early mechanical failures were uncommon in either group. When malalignment was present, the C2 UIV patients showed a trend toward greater improvement in the NDI compared to the C3 UIV patients. These findings suggest that a C2 UIV should be considered in presence of malalignment, but this decision will need to be examined in a larger cohort.
Footnotes
Acknowledgments
The authors thank all of the subjects who participated in the study and the support staff, research coordinator staff, and investigators from the Canadian Spine Outcomes and Research Network (CSORN) contributing sites: Calgary Foothills Medical Centre, Winnipeg Health Sciences Centre, Vancouver General Hospital, Victoria Hospital - London Health Sciences Centre, Queen Elizabeth II – Halifax Sciences Centre, Quebec Hopital de L’Enfant Jesus, Edmonton University of Alberta Hospital, the Ottawa Hospital Civic Campus.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Correction (March 2024):
This article has been updated to correct the first author’s affiliation.