
Abstract
Study Design
Retrospective cohort study
Objectives
Preoperative mental state has been reported as one of the factors affecting the surgical outcomes of spine surgery, but few studies have examined in detail how patients’ mental state is affected by spine surgery. The purpose of this study was to investigate using the Hospital Anxiety and Depression Scale (HADS) whether surgery improves preoperative depression and anxiety in patients with degenerative cervical myelopathy.
Methods
We investigated patient-reported outcomes (Mental Component Summary, Physical Component Summary of SF-12 Health Survey, and EQ-5D, Neck Disability Index, JOACMEQ, satisfaction with treatment) and HADS one year after surgery, comparing them before and after surgery between April 2017 and February 2020. Among the cases diagnosed as preoperative anxiety and depression, we additionally compared the patient-reported outcomes based on the presence or absence of postoperative improvement in mental state, having also investigated the correlation between patient-reported outcomes and HADS for sub-analysis.
Results
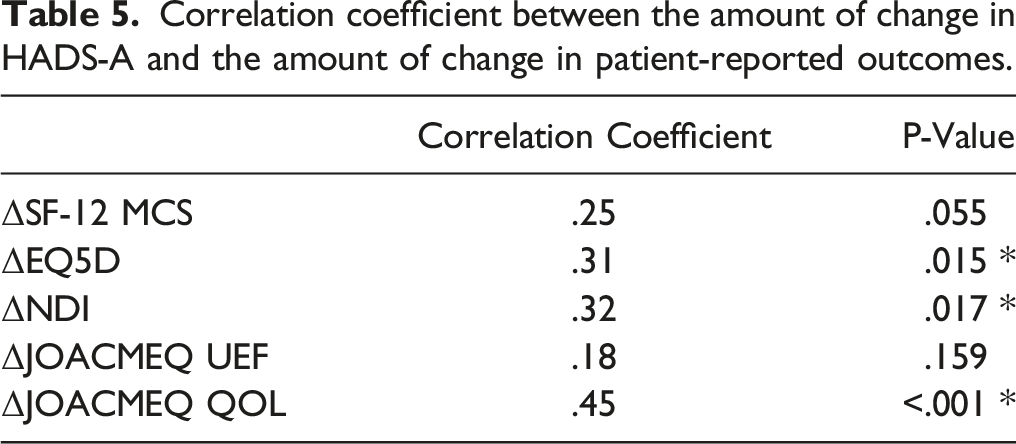
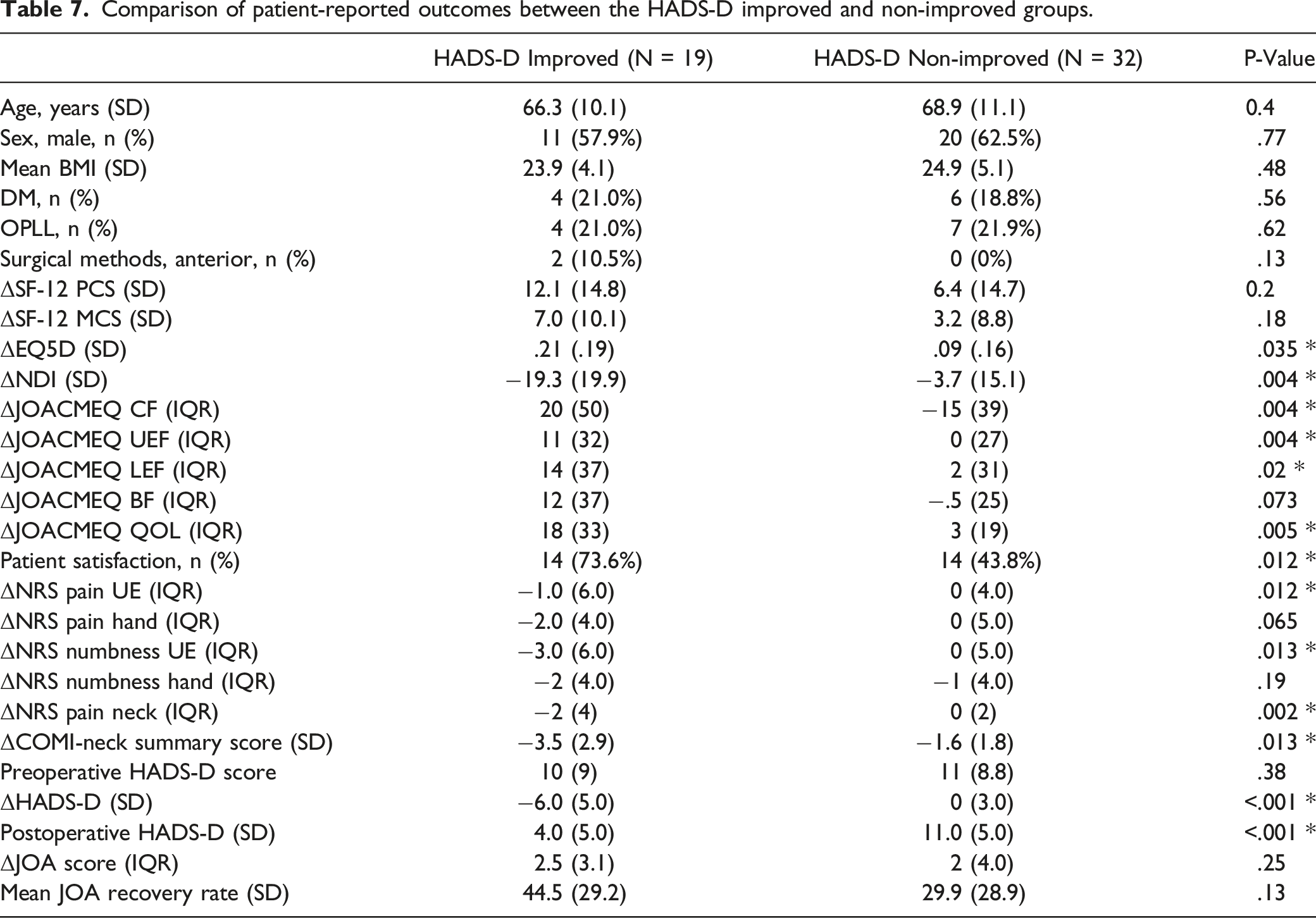
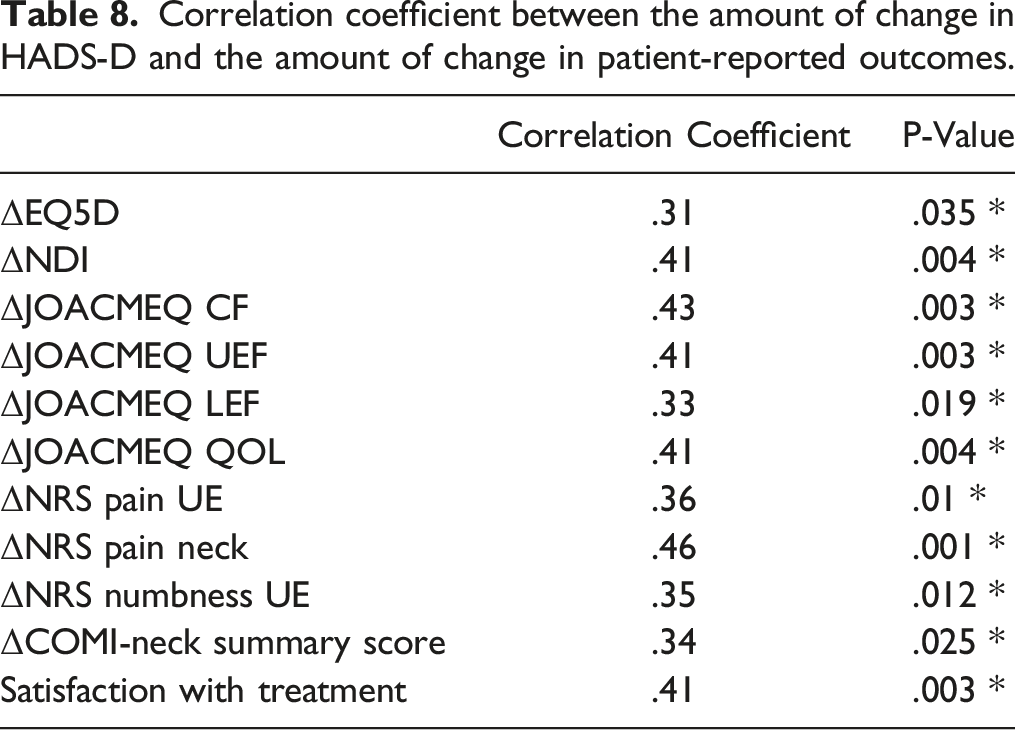
Among the 99 patients eligible for inclusion in the present study, we found that patient-reported outcomes and the HADS scores improved significantly after surgery. There was a moderate correlation between the amount of change in HADS-D score before and after surgery and the amount of change in NDI (moderate, r = .41), NRS of neck (moderate, r = .46), and JOACMEQ (cervical spine function; moderate, r = .43, upper extremity function; moderate, r = .41, QOL; moderate, r = .41).
Conclusions
We found that surgical treatment for patients with degenerative cervical myelopathy may improve postoperative anxiety and depression as well as other patient-reported outcomes.
Keywords
Introduction
Degenerative cervical myelopathy is one of the most common diseases of cervical spine and is caused by aging, instability, and genetic factors. 1 Patients with degenerative cervical myelopathy have significantly reduced their quality of life due to pain, numbness, paralysis, gait disturbance, and dysuria. When neurological symptoms worsen, surgery is often selected to improve the patient’s quality of life. However, surgical outcomes depend on various factors such as the patients’ age, the duration of illness, preoperative neurological symptoms, and imaging findings.2-7
Preoperative psychophysiological state has been reported to affect surgical outcomes of spine surgery.8-10 Hospital Anxiety and Depression Scale (HADS) is a self-administered scoring system for assessing anxiety and depression developed by Zigmond and Snaith, 11 which allows surgeons to evaluate each patient’s anxiety and depressive state conveniently. Because this questionnaire has a merit in that somatic items relating to such emotional or physical disorders as insomnia or anorexia can be excluded, 12 it has often been used in the psychometric assessment of patients with spinal disorders.13-15 Indeed, several reports have demonstrated an association between preoperative anxiety or depression and surgical outcomes in patients with cervical radiculopathy 16 or myelopathy. 15 However, how the degree of preexisting anxiety or depression will change after cervical surgery remains uncertain. The purpose of this study is to investigate whether surgical intervention affects the degree of depression and anxiety in patients with degenerative cervical myelopathy. We also examined the relationship between pre- and postoperative HADS scores and other patient-reported outcomes.
Material and Methods
Subjects
This study was a retrospective cohort study between April 2017 and February 2020. The protocol for this study was approved by the ethics committee of our institution. We obtained written informed consent from all patients for all procedures. We reviewed the aggregated data of 344 patients who underwent cervical spine surgery. We excluded the patients with radiculopathy, tumors, rheumatoid arthritis, or a history of trauma and past spine surgery. Of the 208 patients with degenerative cervical myelopathy (cervical spondylotic myelopathy or ossification of the posterior longitudinal ligament of the cervical spine) remaining after exclusion, 162 patients completed the preoperative HADS questionnaire. Finally, 99 cases who answered the HADS questionnaire 1 year after surgery were examined in this study. (Figure 1) Lastly, we have obtained written informed consent from all patients included in this study. Flowchart of the patient recruitment in the present study.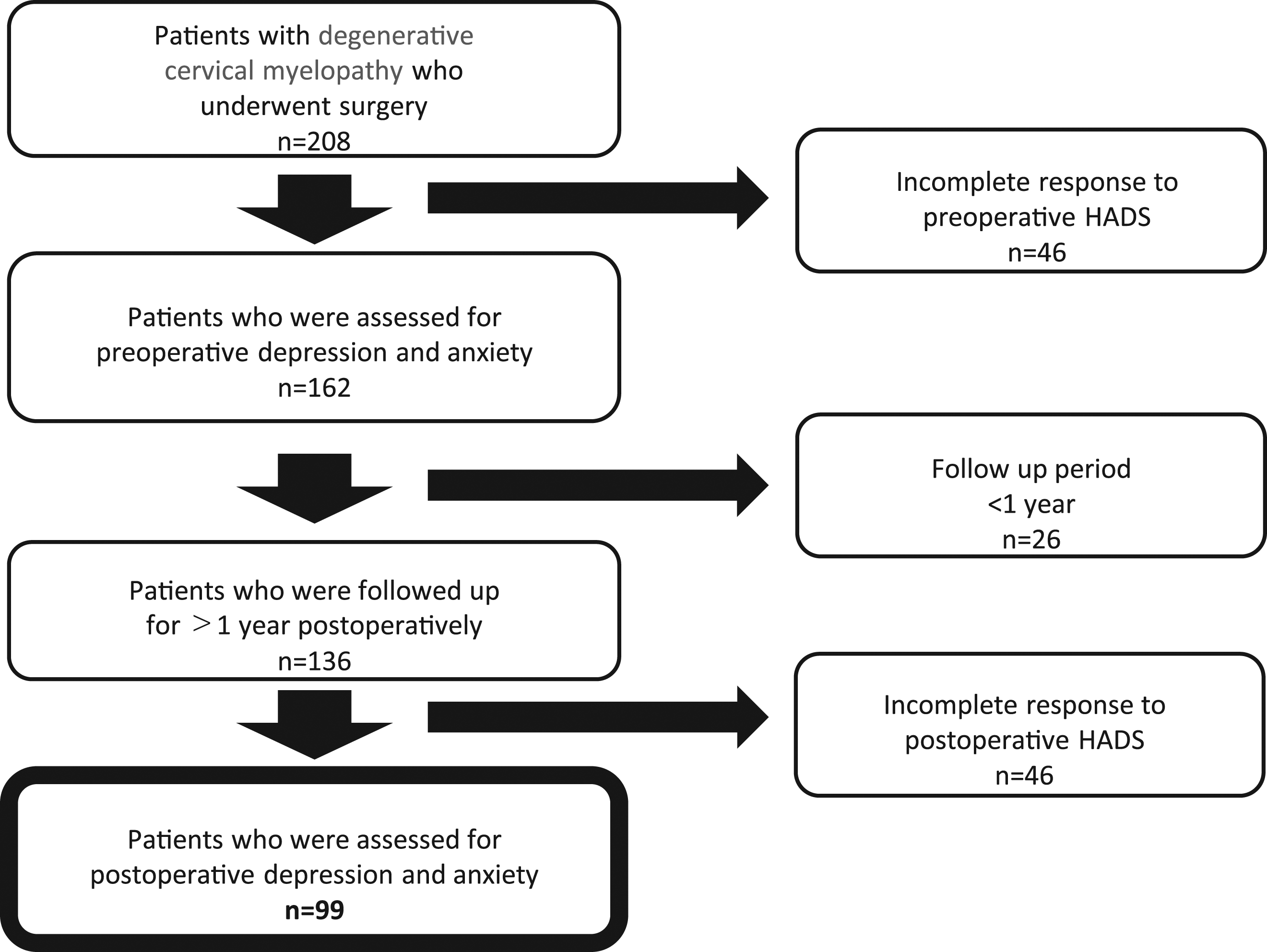
We investigated patient-reported outcomes including HADS scores before and 1 year after surgery. We also used preoperative HADS scores to determine the presence or absence of preoperative anxiety and depression and compared the improvement in patient-reported outcomes with and without anxiety and depression. In addition, we compared the patient-reported outcomes among the cases diagnosed as having anxiety and depression preoperatively based on the presence or absence of postoperative improvement in the HADS scores, and investigated the correlation between patient-reported outcomes and HADS scores.
Measurements of Preoperative Mental State
HADS consists of 14 questions, 7 of which evaluate anxiety (HADS-A) and the rest for depression (HADS-D). Each HADS question is rated on a 4-point scale of 0-3, and both HADS-A and HADS-D are distinguished between 0 and 21. We defined 8 points or more for both HADS-A and HADS-D as anxiety and depression respectively, with reference to previous reports.15,16 We defined the patients whose postoperative HADS-A score improved to less than 8 points as the HADS-A improved group, and the patients whose postoperative HADS-A score did not improve to less than 8 points as the non-improvement group. Regarding the HAD-D score, we also classified it into the HADS-D improved group and the non-improved group according to whether the postoperative HADS-D score improved to less than 8 points. To put it simply, we have asked patients to complete a HADS questionnaire within 7 days prior to surgery and evaluated the results, and we requested the patients to fill out an HADS questionnaire and evaluated the results at the return visit one year after surgery.
Clinical Outcome Measures
We compared the patients’ Mental Component Summary (MCS), Physical Component Summary (PCS) of SF-12 Health Survey, EuroQol health survey of five dimensions (EQ-5D), Neck Disability Index (NDI), Japanese Orthopaedic Association score, Japanese Orthopaedic Association Cervical Myelopathy Evaluation Questionnaire (JOACMEQ), and Core Outcome Measures Index (COMI)-neck summary scores before and after surgery. We evaluated the patient-reported outcomes preoperatively (within 1 week before surgery) and 1 year after surgery, having collected the patient’s questionnaire at the return visit one year after surgery. Additionally, according to a previous study, 17 we surveyed the patients using a questionnaire, regarding their satisfaction with treatment. The answers were made using a 7-point Likert scale, interpreted as follows: (1), very satisfied; (2), satisfied; (3), somewhat satisfied; (4), unsure; (5), somewhat dissatisfied; (6), dissatisfied; and (7), very dissatisfied. Of these, the respondents who answered “somewhat satisfied,” “satisfied,” and “very satisfied” were determined to be satisfied with treatment.
Statistical Analysis
We used the paired t-test and Mann-Whitney U test for continuous variables to compare pre- and postoperative outcomes, and the chi-square test or Fisher’s exact test for categorical variables. In the sub-analysis comparing the presence or absence of improvement in the HADS score after surgery, t-test and Mann-Whitney U test were used for continuous variables, and chi-square and Fisher’s exact test were used for categorical variables. We used Spearman’s correlation coefficient to investigate the correlation between HRQOL and HADS. We used IBM SPSS Statistics version 19 (IBM, Armonk, New York, United States), and we defined a P-value <.05 as statistically significant.
Results
Patient backgrounds.
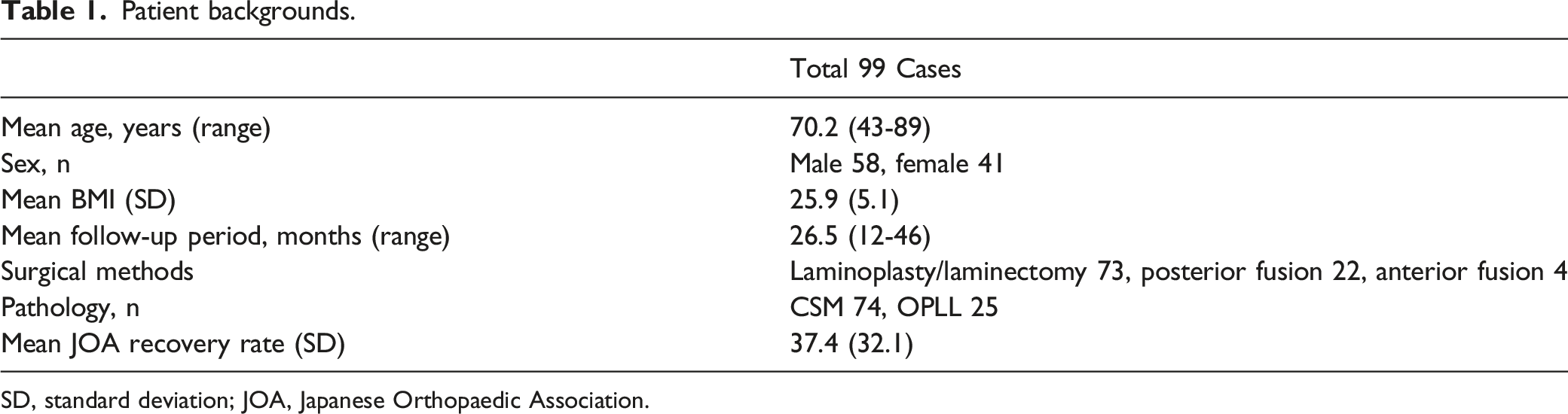
SD, standard deviation; JOA, Japanese Orthopaedic Association.
Comparison of HADS score and patient-reported outcomes before and after surgery for the patients with degenerative cervical myelopathy.
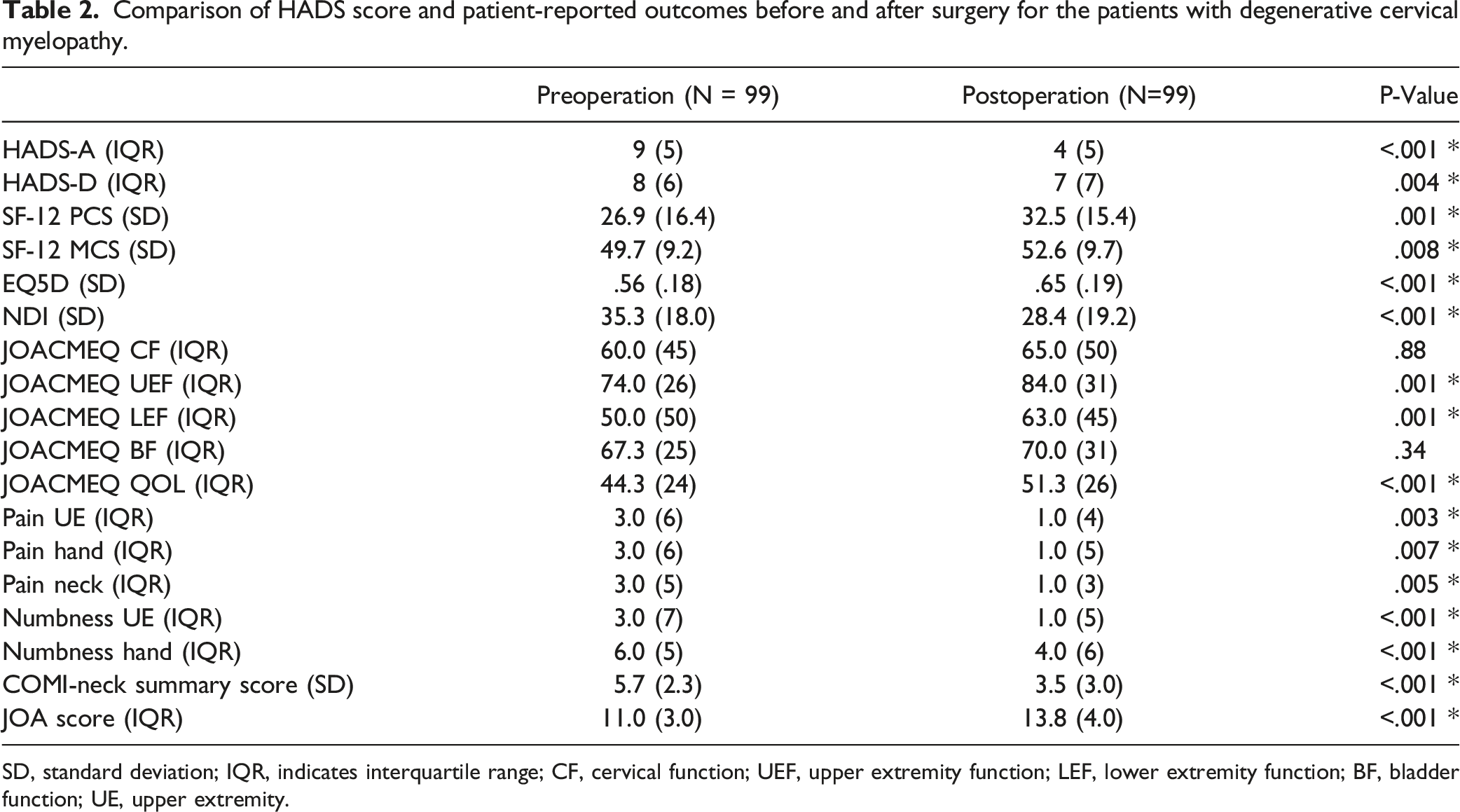
SD, standard deviation; IQR, indicates interquartile range; CF, cervical function; UEF, upper extremity function; LEF, lower extremity function; BF, bladder function; UE, upper extremity.
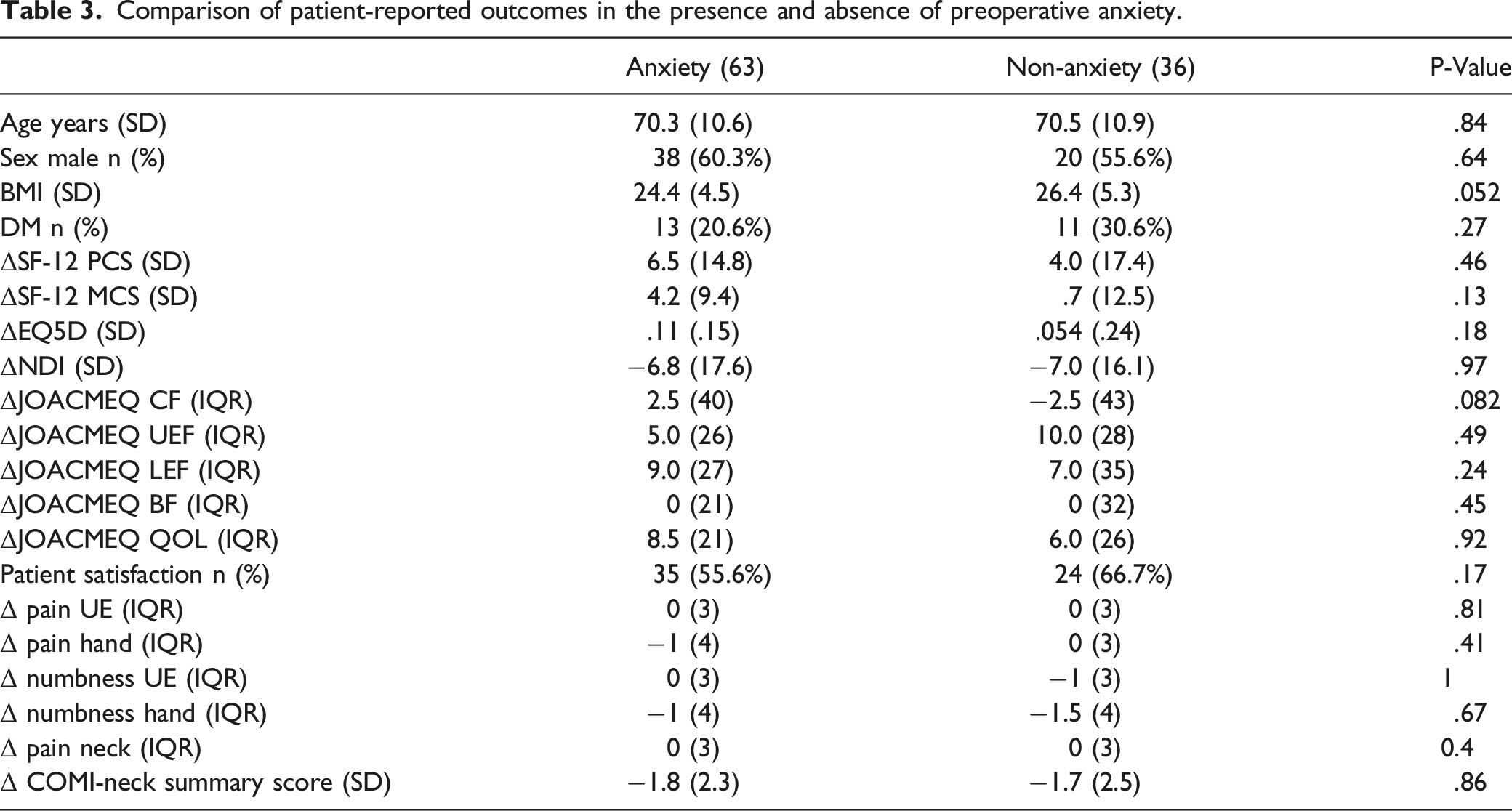
Comparison of patient-reported outcomes in the presence and absence of preoperative anxiety.
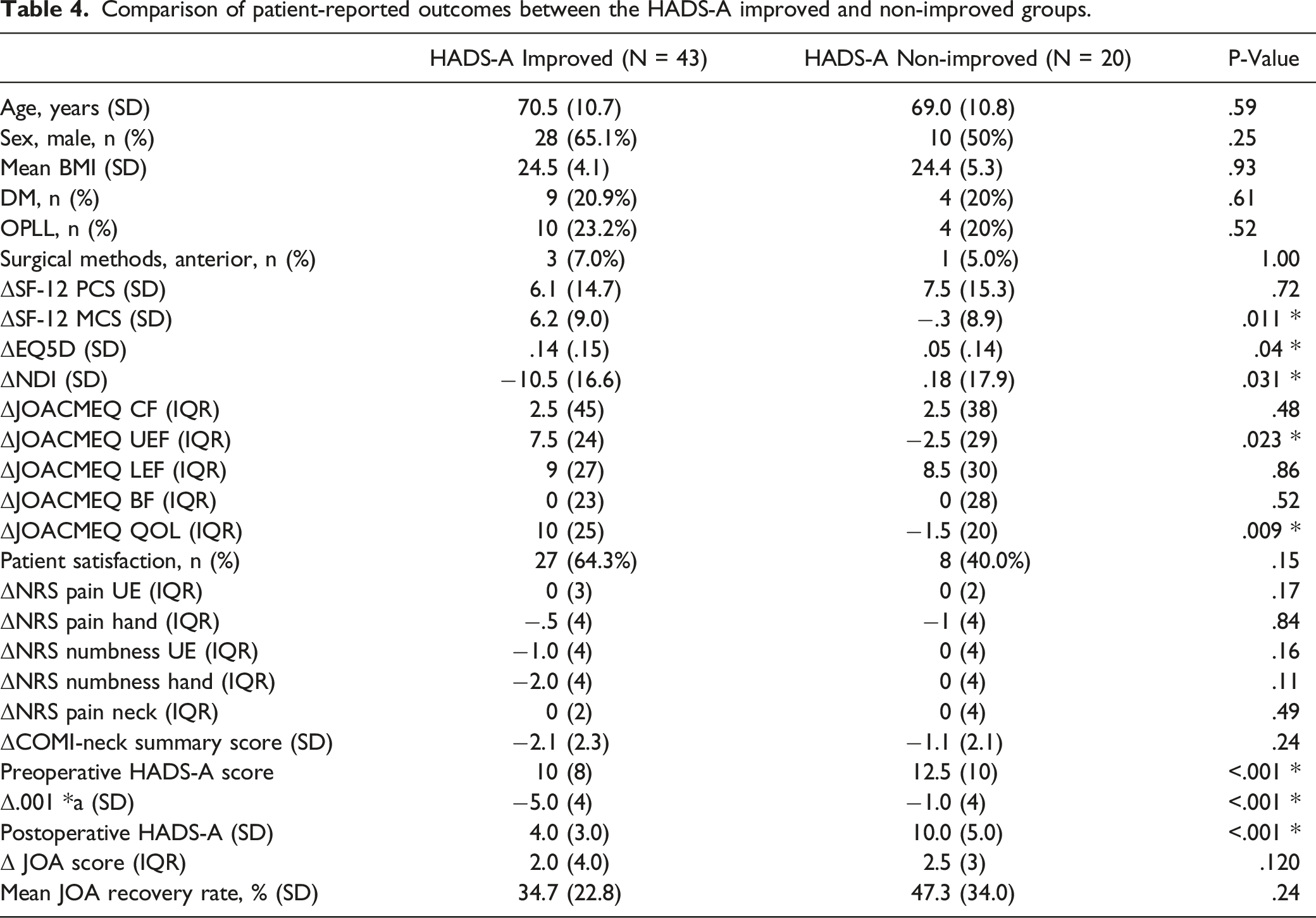
Comparison of patient-reported outcomes between the HADS-A improved and non-improved groups.
Correlation coefficient between the amount of change in HADS-A and the amount of change in patient-reported outcomes.
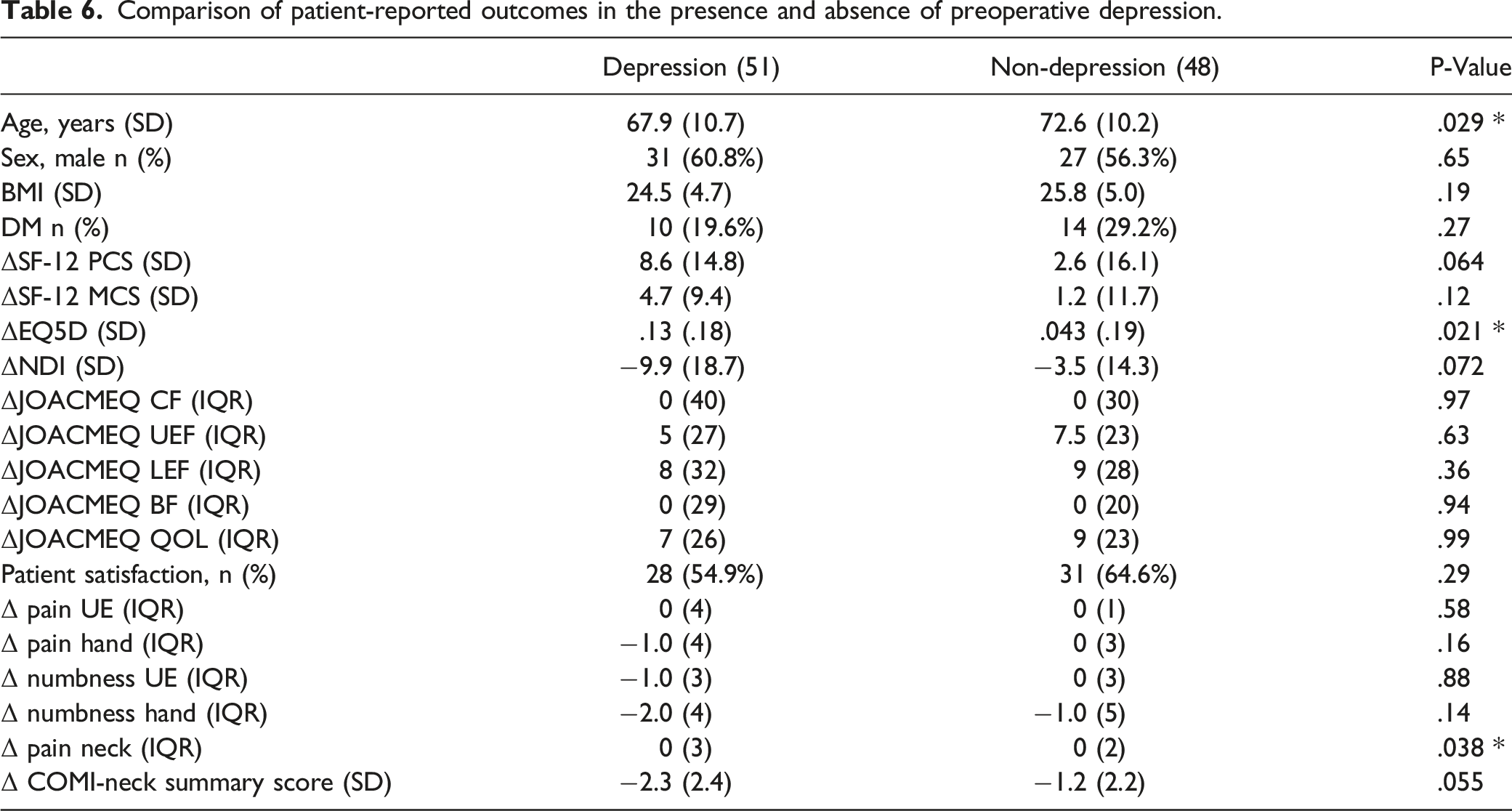
Comparison of patient-reported outcomes in the presence and absence of preoperative depression.
Comparison of patient-reported outcomes between the HADS-D improved and non-improved groups.
Correlation coefficient between the amount of change in HADS-D and the amount of change in patient-reported outcomes.
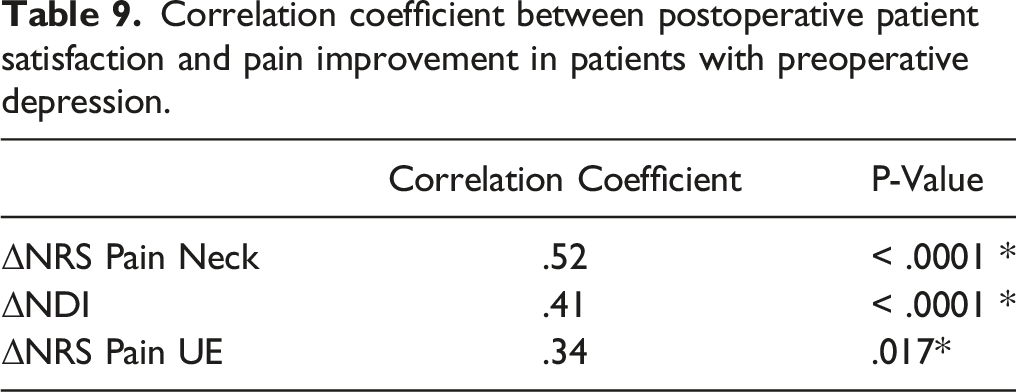
Correlation coefficient between postoperative patient satisfaction and pain improvement in patients with preoperative depression.
Discussion
To the best of our knowledge, this was the first study to evaluate changes in HADS scores before and after spine surgery, and to prove correlation between the changes in HADS scores and other patient-reported outcomes. Our study yielded the following findings: (1) HADS score of the patients with degenerative cervical myelopathy improve postoperatively; (2) preoperative anxiety and depression did not influence the improvement of the patient-reported outcome; and (3) postoperative changes in HADS scores were correlated with those in other patient-reported outcomes.
In this study, HADS scores of patients with degenerative cervical myelopathy improved postoperatively. Although it is still controversial,8-10,15,18,19 many previous studies had investigated the relationship between preoperative mental state and postoperative surgical outcomes in spine surgery. For example, postoperative axial pain was reported to be related with the mental state as measured by MCS of SF-36. 20 The improvement of MCS was also additionally reported after cervical laminoplasty, 21 which indicated an influence of mental health on HRQOL in patients with cervical myelopathy. Regarding anxiety and depression in patients with cervical myelopathy, Doi et al 15 had reported that good surgical results could be expected even if the preoperative psychophysiological condition was poor in patients with degenerative cervical myelopathy even though postoperative changes in HADS scores were not examined. As for changes in HADS before and after surgery in musculoskeletal disorders, improvement in the HADS score was reported to be correlated with functional recovery after treatment for hip joint pathology. 22
The present study thus confirms and extends the findings of the previous studies. Due to the fact the patients’ anxiety or depression was improved after surgery in several patients, we speculate that the existence of preoperative anxiety or depression was partly related to functional disorders owing to cervical myelopathy. On the other hand, in this study, as in some previous reports, there was no difference in the improvement of patient outcomes between patients with and without preoperative anxiety and depression. Therefore, surgery should be considered when indicated in terms of neurological disorders and regardless of the presence or absence of anxiety/depression.
The present study has shown that postoperative patient-reported outcomes have significantly improved in patients who showed an improvement in HADS scores postoperatively in contrast to with those who did not. Moreover, there was a significant correlation between the amount of change in HADS-D score before and after surgery and the amount of change in NDI, NRS of neck, and JOACMEQ in the present study. It is broadly known that depression is associated with pain, ADL, and HRQOL.23,24 In addition, Peterson et al 25 reported that patients with cervical myelopathy have a worse mental state than patients with non-cervical myelopathy. Therefore, patients with cervical myelopathy may tend to have psychological problems as well as physiological ones. We speculate that anxiety/depression, pain, ADL, and HRQOL are mutually affected in patients with cervical myelopathy, as the improvement in HADS scores were correlated with other patient-reported outcomes.
The rate of improvement in HADS-A (68.3%) after surgery was higher than that in HADS-D (37.3%). In addition, patients with postoperatively improved HADS-A scores had significantly lower preoperative HADS-A scores than those who did not, while there was no significant difference in preoperative HADS-D score between patients whose HADS-D score improved after surgery and those who did not. The results in HADS-A were compatible with a previous report by Tamai et al, 21 which showed that MCS in SF-12 in patients with cervical spondylotic myelopathy tended to improve postoperatively, especially in patients with mild preoperative MCS.
Although we do not fully understand the discrepancy of improvement between HADS-A and HADS-D, it is possible the anxiety in patients with low preoperative HADS-A scores reflected the patients’ feelings of anxiety related to hospitalization or surgical treatment before surgery, that is, patients waiting for surgery may tend to be anxious rather than depressive. Indeed, there were some cases in which HADS-D improved postoperatively regardless of the preoperative HADS-D scores. We also found that the changes in HADS-D score were more correlated with those in other patient-reported outcomes as compared with HADS-A scores. The HADS-D score showed correlation not only with patient-reported outcomes but also with treatment satisfaction. In contrast, no significant difference in treatment satisfaction was observed between HADS-A scores with and without improvement in HADS-A scores. Therefore, the HADS-D score may be more useful in evaluating treatment outcomes in degenerative cervical myelopathy. In this case series, posterior surgery was by far the most common. Reports have shown that neck pain, including axial pain, was more common in posterior surgery. 26 In this study, no significant difference was observed between the presence or absence of improvement in HADS-D and the surgical technique; however, the number of cases of anterior surgery in the target patients may have been small. For the HADS-D score, a correlation was found between the degree of improvement in the score and patient satisfaction with treatment. For patients who were determined to be preoperatively depressed, a correlation was observed between treatment satisfaction and NRS and NDI. Many patients in this study underwent posterior surgery, and the residual neck pain associated with posterior surgery may have influenced the difference in improvement degree between the HADS-D and HADS-A scores. Nevertheless, both HADS-A and HASD-D will be improved after cervical surgery to some extent. Further studies are necessary to clarify the difference between anxiety and depression.
This study has several limitations. First, the effects of psychiatric drugs were not considered, and there was a selection bias in this study as we only evaluated patients who responded to the questionnaire. Second, as mentioned in the Discussion section, there was a bias in the surgical procedures in this study. Third, this study was a retrospective study and the follow-up period was relatively short. A previous study has reported that evaluation of patient-based outcomes may be sufficient up to 1 year after surgery. 27 Moreover, there was no examination of preoperative image evaluation or illness period that may affect the surgical results. We consider that further studies such as prospective studies with an increased number of cases and a longer follow-up period would be not only necessary but ideal.
Conclusions
We have found surgical treatment for patients with degenerative cervical myelopathy may improve preexisting anxiety and depression as well as other patient-reported outcomes. Even if the mental condition is poor before surgery in patients with degenerative cervical myelopathy, our results suggest surgery should be considered if there is a neurological indication for such.
Footnotes
Author Note
The relevant EQUATOR Network reporting guidelines should be followed depending on the type of study. For example, all randomized controlled trials submitted for publication should include a completed CONSORT flowchart as a cited figure and the completed CONSORT checklist should be uploaded with your submission as a supplementary file. Systematic reviews and metaanalyses should include the completed PRISMA flowchart as a cited figure and the completed PRISMA checklist should be uploaded with your submission as a supplementary file. The EQUATOR wizard can help you identify the appropriate guideline. Other resources can be found at ![]() .
.
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: YT has received personal fees from ZOZO, Inc., outside the submitted work. ST has received honoraria from Amgen, Inc., ASAHI KASEI PHARMA CORPORATION, Amgen Astellas BioPharma K.K., KYOCERA Medical Corporation, DAIICHI SANKYO COMPANY, LIMITED, TEIJIN PHARMA LIMITED., Eli Lilly Japan K.K., and Pfizer Japan Inc., endowments from Astellas Pharma, Inc., AYUMI Pharmaceutical Corporation, Bristol Myers Squibb, Pfizer Japan, Inc., DAIICHI SANKYO COMPANY LIMITED, and Chugai Pharmaceutical Co, Ltd, and grants from the Japan Agency for Medical Research and Development (AMED), Japan Society for the Promotion of Science (JSPS)/Grant-in-Aid for Scientific Research (A), and the Japan Society for the Promotion of Science (JSPS)/Grant-in-Aid for Exploratory Research., outside the submitted work. YO is supported by grants from DePuy Synthes, grants from Medtronic Japan, grants from Olympus Terumo Biomaterials Corp., grants from Stryker Japan K.K., and grants from Nuvasive Japan Inc., outside the submitted work. Others have nothing to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All procedures involving human participants were performed according to the 1964 Helsinki Declaration. The study protocols were approved by the Institutional Review Board of University of Tokyo (IRB No 10335). We obtained written informed consent from all patients for all procedures.