
Abstract
Study Design
A retrospective case-control study.
Objective
This study aimed to compare the effects of the Wiltse approach of pedicle screw fixation (PSF) either in combination with or without vertebroplasty (VP) in the treatment of Genant III degree osteoporotic thoracolumbar fractures (Genant III-OTLFs).
Methods
A retrospective study of Genant III-OTLFs was performed from January 2018 to December 2019, including 54 cases of PSF + VP and 56 cases of PSF. Clinical indicators [visual analog scale (VAS) score, Oswestry disability index (ODI)], radiographic parameters [local kyphosis angle (LKA), percentage of anterior, central, and posterior vertebral heights (AVH%, CVH%, and PVH%, respectively)] and follow-up complications [adjacent vertebral fracture (AVF), residual pain (RP), vertebral height loss (VHL), and internal fixation failure (IFF)] were compared between the 2 groups.
Results
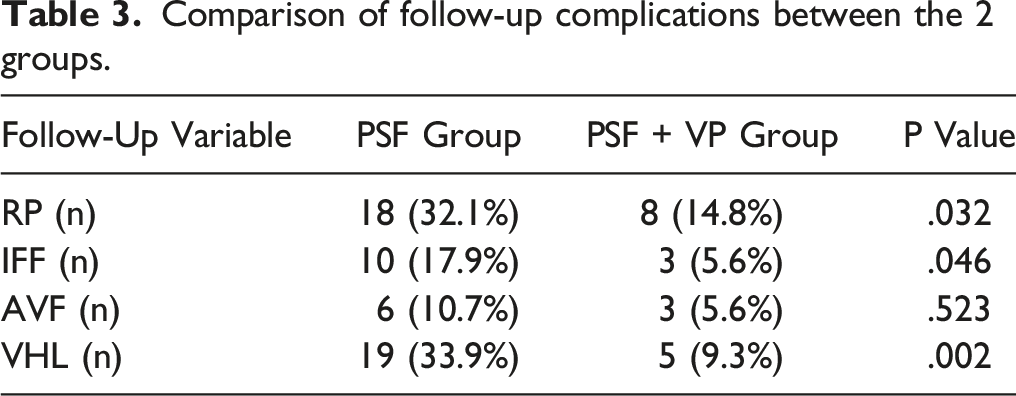
No differences in surgical outcomes, clinical indicators, and radiographic parameters were observed between the 2 groups during the preoperation period and 7 days post-operatively (P > .05). However, the VAS score [2.0 (.6), 1.9 (.5)], ODI [23.7 (4.0), 22.6 (3.0)], LKA [9.5 (1.8), 10.6 (3.0)], AVH% [90.1 (2.7), 87.7 (6.0)], CVH% [92.5 (2.6), 91.3 (3.7)], and PVH% [93.4 (2.0), 92.7 (2.4)] at 1 year post-operatively and last follow-up of the PSF + VP group were better than those of the PSF group [2.5 (.8), 3.1 (1.1), 26.6 (3.8), 29.6 (4.6), 12.2 (1.6), 16.6 (3.2), 84.9 (4.0), 69.9 (6.6), 88.1 (3.1), 78.2 (5.1), 89.7 (2.3), 84.8 (4.6)], respectively (P < .001). During follow-up, the incidence of AVF had no difference (P > .05), while that of RP (32.1 vs 14.8%), VHL (33.9 vs 9.3%) and IFF (17.9 vs 5.6%) had statistical differences between them (P < .05).
Conclusion
The Wiltse approach of PSF combined with VP for Genant III-OTLFs can not only effectively relieve pain, restore vertebral height, and correcte kyphosis, but also better maintain vertebral height, delay kyphosis progression, and reduce complications during follow-up.
Keywords
Introduction
A rapidly aging population in China has led to an increase in the rate of osteoporosis, 1 and consequently, the incidence of osteoporotic thoracolumbar fractures (OTLFs) caused by osteoporosis is rising every year.2,3 Owing to the high rates of disability and death, 4 OTLFs have become a major public problem endangering the quality of life in the elderly population. 5 Currently, OTLFs have various kinds of classification, such as DGOU-OF, EVOSG, Kanchiku, Heini and TLOFSAS classifications. However, they lack the quantitative classification of vertebral height, which is a crucial surgical factor for severely compressed OTLFs. It is to be noted that the Genant visual classification method, based on the compression degree of the vertebral body on the lateral radiograph, 6 is more appropriate and convenient for clinical applications. According to this classification, 6 vertebral height compression >40% is classified as III degree for severe compression fractures. In recent years, minimally invasive surgeries, represented by vertebroplasty (VP) and kyphoplasty (KP), have widely been used for the treatment of Genant I and II degree OTLFs for effectively relieving pain and correcting disabled conditions. However, for Genant III degree OTLFs (Genant III-OTLFs) with severe vertebral collapse, KP or VP is ineffective in restoring the vertebral height or eliminating the kyphosis,7,8 which may lead to a high risk of revision surgery such as spinal nerve injury if not handled properly. 9 The mini-open Wiltse approach of pedicle screw fixation (PSF) is an innovative and minimally invasive technique, the advantages of which in the treatment of thoracolumbar fractures have been reported.10,11 However, a cavity-like phenomenon related to the PSF may lead to vertebral height loss (VHL), internal fixation failure (IFF) and even kyphosis under continuous loading for Genant III-OTLFs treated with PSF after the reduction of the injured vertebra by pedicle screws.12,13 Currently, no consensus on the treatment options for this disease exists. Therefore, the clinical data of single-segment Genant III-OTLFs that underwent PSF + VP or PSF are summarized below to explore their effectiveness.
Materials and Methods
This study was performed in accordance with the Helsinki Declaration and received approval of the ethics committee of the fourth affiliated hospital of Nanjing Medical University (Approval number: 20221208-k066). The clinical data of single-segment Genant III-OTLFs from January 2018 to December 2019 were retrospectively analyzed, including 54 cases of PSF + VP and 56 cases of PSF.
The inclusion criteria were as follows: (1) T score of bone mineral density (BMD) <−2.5; (2) Magnetic resonance imaging (MRI) confirmed fresh single segment OTLFs; (3) VHL >40%, classification of Genant III degree; (4) No spinal cord injury.
The exclusion criteria were as follows: (1) Pathological fractures, such as tumors and tuberculosis; (2) Poorly healed fractures, such as Kummell’s disease; (3) Inability to tolerate general anesthesia because of serious diseases; (4) Combined with issues including three-column injury, and pedicle fracture displacement; (5) With chronic pain caused by severe degenerative diseases; (6) Incomplete follow-up data.
Surgical Procedures
PSF + VP
After successful general anesthesia, the injured vertebra was located and marked in the prone hyperextension position. First, skin and subcutaneous tissue were cut layer by layer along an approximately 8 cm incision after disinfection. The intermuscular space between the multifidus and longissimus muscles (Wiltse intermuscular space) was exposed under the lumbar dorsal fascia. Then, the facet joints were exposed by the blunt separation of the Wiltse intermuscular space with fingers. Four pedicle screws were placed in the upper and lower vertebrae according to the pedicle placement technique. After the pre-bending rods were installed, the injured vertebra was reduced with the reduction device, the height of the vertebra was restored, and the kyphosis was corrected by fluoroscopy. Second, VP was performed by bilateral puncture technique. The puncture point was located at the base of the transverse process and close to the rod edge. When the puncture channel was established, the gelatin sponge was inserted into the vertebra. Once mixed bone cement was qualified, it was injected into the injured vertebra through fluoroscopy and bone cement leakage was monitored during the operation. Finally, the wound was rinsed and sutured.
PSF
After successful general anesthesia, the above steps (position, fluoroscopy, marking, disinfection, incision, surgical approach) were the same as those in the PSF + VP group. Then, a total of 6 pedicle screws were inserted into 3 vertebrae. When the height of the injured vertebra was restored and kyphosis was corrected by fluoroscopy, the rods were fixed. Finally, the wound was rinsed and sutured.
Postoperative Management
(1) Patients were routinely given anti-inflammatory, and anti-nociceptive medications after surgery. (2) At 1 day post-operatively, the patient got out of bed with a brace for rehabilitation exercise. (3) All patients were examined by X-ray at 7 days post-operatively. (4) Basic medication (calcium + vitamin D) and anti-osteoporosis medication (intravenous zoledronic acid once a year) were given during the perioperative period.
Clinical and Radiologic Assessment
Back pain was recorded and evaluated by the visual analog scale (VAS) score. Oswestry disability index (ODI) represented the impact on the daily life of patients. Kyphosis was estimated by local kyphosis angle (LKA) and the height of vertebra was assessed by the percentage of anterior, central, and posterior vertebral height (AVH%, CVH%, and PVH% respectively), which were measured on a standard lateral radiograph (Figure1.). All of the above data were measured and averaged by two experienced spinal surgeons preoperatively, 7 days post-operatively, 1 year post-operatively, and at the last follow-up. VHL was defined as VHL ≥15% or LKA increase ≥10° after surgery.
7
Moderate to severe pain (VAS score ≥4) was assessed as residual pain (RP). The criteria for IFF included loosening or breakage of internal fixation. Perioperative complications included pulmonary infection, cardiac dysfunction, wound infection or poor healing, postoperative delirium, and lower extremity venous thrombosis. Long-term follow-up complications included RP, VHL, AVF and IFF. Measurement of imaging parameters. LKA was formed by two vertical lines erpendicular to the lines parallel to the superior endplate of the upper vertebra of the injured vertebra and to the inferior endplate of lower vertebra of the injured vertebra. AVH%, MVH% and PVH% were respectively measured by (2 times of injured vertebral height)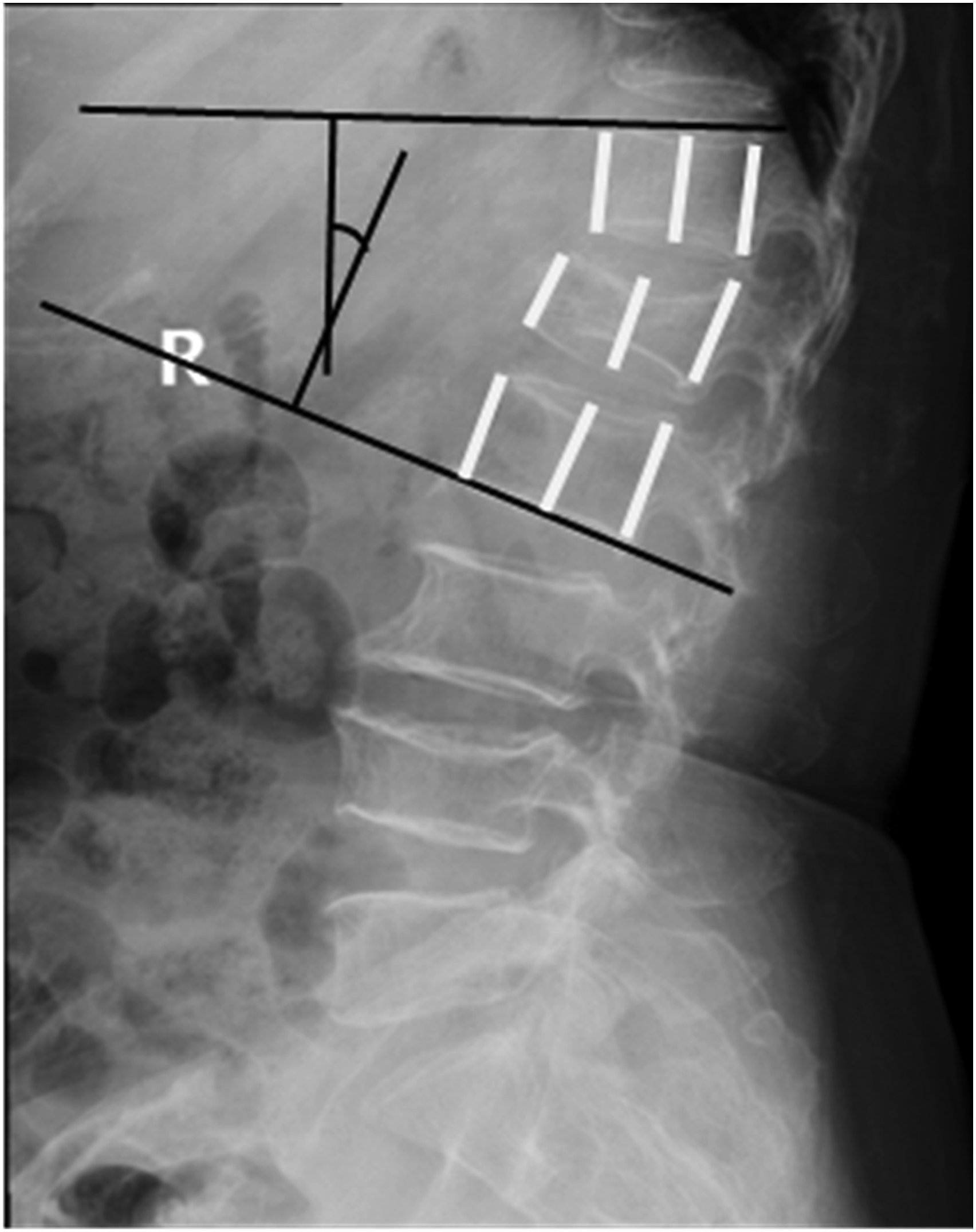
Statistical Analysis
SPSS26 statistical software was used for data analysis. The data obtained from measurements were expressed as mean ± standard deviation. When the data were normally distributed, an independent sample t test was used for comparison between groups. Count data were expressed as frequency, and comparison between groups was performed by chi-squared test. P < .05 was considered statistically significant.
Results
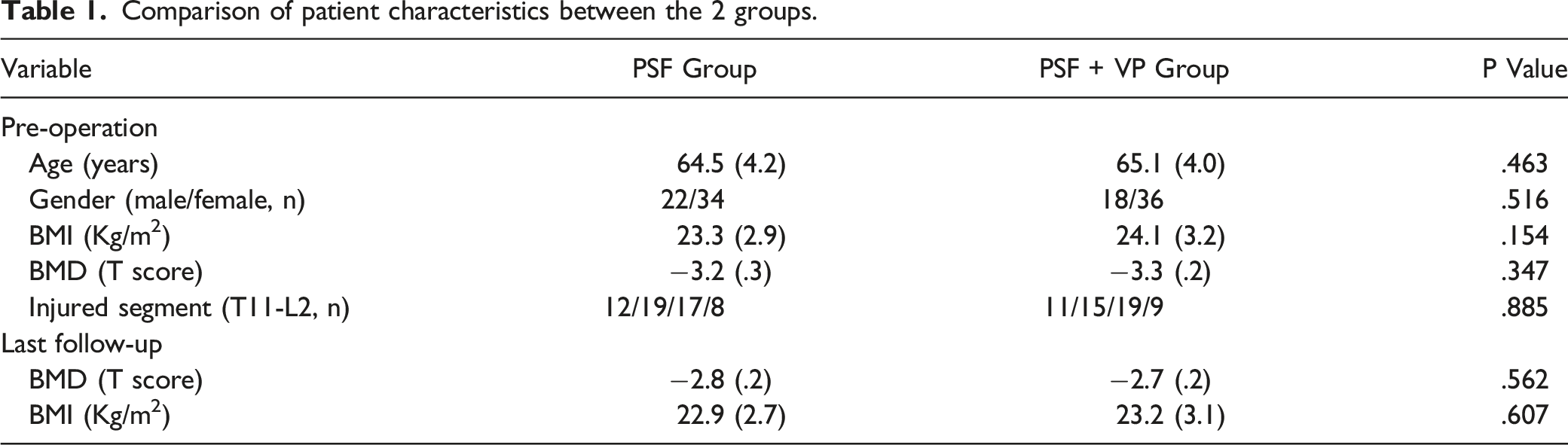
Patient Characteristics
Comparison of patient characteristics between the 2 groups.
Surgical Outcomes
Comparison of surgical outcomes between the 2 groups.

Clinical Indicators
The preoperative VAS score and ODI of the 2 groups significantly decreased at 7 days post-operatively. In the PSF + VP group, the VAS score and ODI at 1 year post-operatively were 2.5 (.8) and 26.6 (3.8), but they increased to 3.1 (1.1) and 29.6 (4.6) at the last follow-up, respectively. While in the PSF + VP group, they were similar with no visible trend at 1 year post-operatively and last follow-up. No significant differences were found at the preoperation period and 7 days post-operatively in VAS scores and ODI between the 2 groups ( The comparison of clinical indicators between the two groups.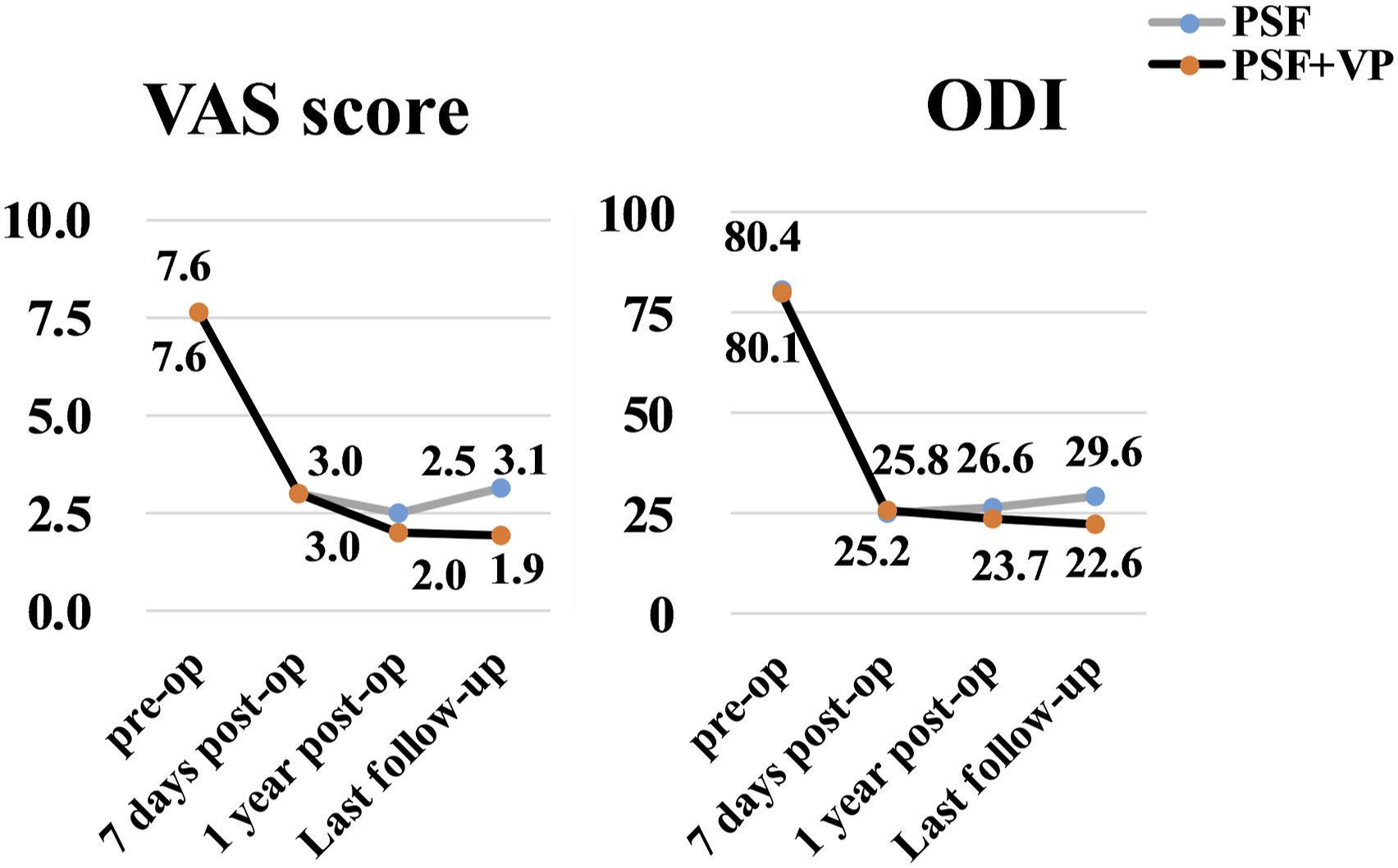
Radiological Parameters
The radiological parameters of the 2 groups are presented in Figure 3. Both groups demonstrated significant improvement in the preoperative radiological parameters (LKA, AVH%, CVH%, PVH%) at 7 days post-operatively. The comparison of radiological parameters between the 2 groups showed no differences at preoperation and 7 days post-operatively The comparison of radiological parameters between the two groups. A 72-year-old male underwent PSF with Genant III-OTLFs (L1). (A-D) X-ray and CT (computed tomography, CT) showed sever vertebral collapse, sparse bone trabecula, cavity-like phenomenon and vertebral wall breakdown. T1 phase of magnetic resonance imaging (MRI) (E) suggested low signal and T2 phase (F) suggested high signal. Postoperative X-rays (G-H) showed the height of the vertebra has been restored and the kyphosis has been corrected. VHL, IFF and kyphosis were observed on X-rays at last follow-up (I-J). A 73-year-old female underwent PSF+VP with Genant III-OTLFs (L1). (A-D) X-ray and CT showed vertebral collapse, sparse bone trabeculae, vertebral wall damage and vertebral cavity-like lesions. (E-F) MRI showed low signal in T1 phase and mixed signal in T2 phase. (G-H) Postoperative X-ray showed vertebral height recovery, good diffusion of bone cement and no bone cement leakage. (I-J) No VHL or IFF was observed on X-ray radiograph at last follow-up.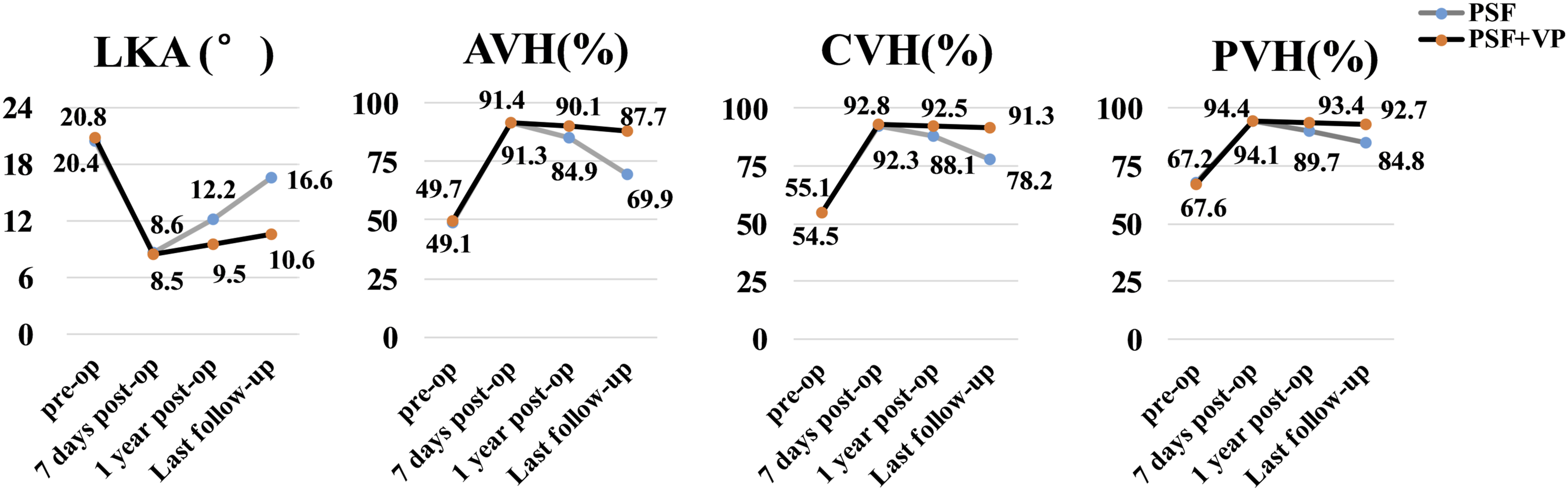


Long-Term Follow-Up Complications
Comparison of follow-up complications between the 2 groups.
Discussion
Genant III-OTLFs often occur at the thoracolumbar vertebrae because of their anatomical characteristics and biomechanical properties.14,15 The imaging of Genant III-OTLFs is characterized by severe vertebral height loss, vertebral wall breakage and sagittal imbalance, which decrease vertebral stability. In addition, radiological imaging shows osteopenia and the destruction of bone microarchitecture caused by osteoporosis. Consequently, the loss of stability owing to radiographic features of the injured vertebra significantly increases the occurrence of VHL. 16 Therefore, the treatment of Genant III-OTLFs remains an intractable problem.
The principles of treatment for Genant III-OTLFs focus on restoring vertebral height and maintaining stability. In previous studies, surgeons tended to pay more attention to pain and disability in elderly patients, and only performed vertebral augmentation, but neglected to the restoration of vertebral height and correct kyphosis,7,8 leading to insufficient restoration. PSF can effectively restore the vertebral height and physiological curvature,10,11 but not strengthen the injured vertebral body.12,13 Therefore, long-segment fixation has been proposed to enhance screw-holding power and stability to reduce complications. 17 Nevertheless, owing to common comorbidities of other chronic diseases in the elderly population, long-segment fixation is likely to increase surgical trauma and complications, as well as the loss of more motion segments. 18 Meanwhile, the cement-reinforced pedicle screws have also been applied to avoid IFF, 19 but it can result in severe degeneration of adjacent segments that may require spinal revision surgery. Therefore, this study aimed to explore the effectiveness and feasibility of Genant III-OTLFs treatment by combining the advantages of PSF and VP.
Reconstruction and restoration of vertebral height and stability are critical points in the treatment of Genant III-OTLFs. Herein, both methods both used pedicle screws to reduce the injured vertebra, which played a positive role in restoring the vertebral height and correcting the kyphosis, but also led to vertebral cavity-like lesions. The difference between the 2 procedures was in the management of cavity-like lesions, with PSF performing no treatment and PSF + VP performing cement augmentation. The pedicle screw stability is absolutely related to osteoporosis and the internal fixation exhibits disadvantages such as insufficient grip. A biomechanical study demonstrated that the stability of pedicle screws was significantly deficient in vertebral bone mineral content (<80 mg/cm3), and the imposition of methods is needed to enhance screw stability. 20 Thus, for Genant III-OTLFs treated with PSF, the injured vertebra is mechanically fragile after reduction and involves high risks of VHL, kyphosis, and biomechanical alteration in the future. 21
As the pathological basis of OTLFs is osteoporosis, surgery only temporarily restores vertebral height and bone mass must be increased to maintain spinal stability. Therefore, postoperative anti-osteoporotic treatment must be administered to promote bone formation and reduce bone loss. 22 In this study, all patients underwent standardized anti-osteoporosis treatment and the BMD was significantly better compared with that of the pre-operation. However, regarding long-term complications, the incidences of IFF and VHL in the PSF group were higher than those in the PSF + VP group. Moreover, the VAS score and ODI in the PSF group were significantly worse than that in PSF + VP group during follow-up, which resulted in an increased incidence of RP. More seriously, the radiological parameters of the PSF group were inferior to that of the PSF + VP group at 1 year post-operatively and last follow-up. Therefore, the deficiency of biomechanical stability might appear in Genant III-OTLFs treated with PSF.
It was concluded that bone cement altered the biomechanical properties of vertebra. 23 If the bone cement is uniformly distributed in the upper and lower endplates and the anterior column of the vertebra, the stiffness and strength of the injured vertebra can be improved, which can effectively minimize the incidence of VHL.24,25 Simultaneously, a good distribution of bone cement can augment the carrier load, which is conducive to reducing the pressure of internal fixation and crucial to maintaining the stability of the spine. 26 Therefore, the effective performance of bone cement infusion and avoidance of poor bone cement distribution have become the keys to surgery. Herein, the bilateral puncture technique was applied in VP and the average volume of bone cement was as high as (5.6 ± .4) mL. Importantly, the continuous anchoring technique with temperature gradient injection 27 and the application of gelatin sponge to seal the breach 28 were adopted, which considerably reduced the bone cement leakage and led to good diffusion of bone cement in the stress concentration area of the front column and the center of the vertebra.
Postoperative complications associated with spinal surgery are more common in elderly patients. 29 Herein, the incidence of complications was about 13.6% probably because the study included elderly patients with chronic diseases. However, no serious complications were observed in this study. All patients were subjected to effective preoperative evaluation and trauma reduction procedures during surgery. In addition, early postoperative functional exercise and active prevention of complications were also implemented. More importantly, timely and effective treatment was also provided when complications occurred.
This study has some limitations. First, it is a retrospective, single-centered study and the data obtained may be biased, which needs further validation by prospective, randomized and multi-centered studies. Second, the sample size in this study is small and a larger-sample is essential to reduce statistical errors. Third, there are other interference factors, such as the effects of degeneration of low back muscle on RP and influences the of BMI on VHL and IFF. In addition, the follow-up period of this study is short and needs to be increased for deriving more crucial insights. Finally, the biomechanical study of Genant III-OTLFs treated with PSF + VP was not explored, and hence, further researches are necessary.
Conclusion
For the treatment of Genant III-OTLFs, the Wiltse approach of PSF combined with VP can not only effectively relieve pain, restore vertebral height and correct the kyphosis, but also better maintain vertebral height, delay kyphosis progression, and reduce complications during long-term follow-up.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the General Project of Natural Science Foundation of Jiangsu Province, China (No. BK20201130)