
Abstract
Study Design
Multicenter prospective cohort study.
Objectives
Anxiety in combination with osteoporotic vertebral compression fractures (OVCFs) of the spine remains understudied. The purpose of this study was to analyze whether anxiety has an impact on the short-term functional outcome of patients with an OVCF. Furthermore, a direct impact of the fracture on the patient’s anxiety during hospitalization should be recognized.
Methods
All inpatients with an OVCF of the thoracolumbar spine from 2017 to 2020 were included. Trauma mechanism, analgetic medication, anti-osteoporotic therapy, timed-up-and-go test (TuG), mobility, Barthel index, Oswestry-Disability Index (ODI) and EQ5D-5L were documented.
For statistical analysis, the U test, chi-square independence test, Spearman correlation, General Linear Model for repeated measures, Bonferroni analysis and Wilcoxon test were used. The item anxiety/depression of the EQ5D-5L was analyzed to describe the patients’ anxiousness.
Results
Data from 518 patients from 17 different hospitals were evaluated. Fracture severity showed a significant correlation (r = .087, P = .0496) with anxiety. During the hospital stay, pain medication (P < .001), anti-osteoporotic medication (P < .001), and initiation of surgical therapy (P < .001) were associated with less anxiety. The anxiety of a patient at discharge was negatively related to the functional outcomes at the individual follow-up: TuG (P < .001), Barthel index (P < .001), ODI (P < .001) and EQ5D-5L (P < .001).
Conclusions
Higher anxiety is associated with lower functional outcome after OVCF. The item anxiety/depression of the EQ5D-5L provides an easily accessible, quick and simple tool that can be used to screen for poor outcomes and may also offer the opportunity for a specific anxiety intervention.
Introduction
Anxiety highly influences the outcome of patients after illness.1-5 In some cases, the effects of anxiety almost completely prevent patients from returning to their familiar daily lives, even after successful primary treatment. 6 Previous studies have already emphasized the importance of recognizing deficits in coping strategies as well as tendencies toward depression at an early stage of illness. Preventive measures in this regard could help counteract and prevent high mortality rates and poor outcomes.7,8 To date, there are few studies dealing with the impact of anxiety in conjunction with osteoporotic vertebral compression fractures (OVCFs), although the psychosocial care of every patient is noted as a form of basic therapy in the current guidelines for osteoporosis. 9
Recently, the working group Osteoporotic Fractures of the Spine Section of the German Society of Orthopaedics and Trauma (AG-OF) published the OF classification system for osteoporotic thoracolumbar fractures in 2018. 10 Additionally, a score for treatment decisions and treatment recommendations for each fracture type were developed. 11 With the aim of evaluating the scoring system, the “Clinical Evaluation of the OF-Score for Therapy-Planning and Treatment-Recommendations for osteoporotic fractures of the thoracolumbar spine” study (EOFTT) was conducted and revealed good clinical results for therapy following this recommendation and adapted to fracture severity according to OF classification.12-15
The aim of the present study was to determine the impact of anxiousness on the outcome of patients with OVCFs using data from the EOFTT study.
Materials and Methods
As part of the EOFTT study, patient evaluations were conducted at 17 participating centers from September 2017 to June 2021. The study was approved by the local institutional ethics committees of each participating center (Medical Association of Saxony-Anhalt/Germany: 31/17), all patients gave written informed consent.
Inclusion and Exclusion Criteria
Patients were eligible for the study if they had at least 1 osteoporotic thoracolumbar vertebral fracture of trauma or insufficiency origin. Those who gave informed consent were enrolled. Patients who suffered from spondylodiscitis, tumor disease or polytrauma at the time of admission were excluded. In the case of multiple fractures, the patient’s most severe fracture was considered the index fracture according to the osteoporotic fracture (OF) classification. 10 Measuring of bone density for the diagnosis of osteoporosis was performed by DEXA, q-CT or Hounsfield unit (HU) measurement described by Schreiber et al10,16 or an indication for osteoporosis therapy according to the German Osteology Society guidelines. 17 Furthermore, at least 1 follow-up examination was mandatory 6 weeks to 12 months after discharge.
Data Collection Process
Data were collected at 17 centers in German-speaking countries as part of the EOFTT study10,18 at 6 points in time during treatment and follow-up care: admission (T1), the day of the therapy decision (T2), discharge (T3), and the follow-up examinations after 6 weeks (T4), 12 weeks (T5), 6 months (T6) and 12 months (T7). In the course of this study, an individual follow-up appointment (FU) was scheduled for each patient and carried out closest to T4 (mean ± 8 weeks), to improve evaluability. Additionally, epidemiological data and data on the trauma mechanism were obtained.
The fracture pattern according to the OF classification was determined by the examiner using radiological diagnostics. 10 Pain medication according to the WHO analgesic ladder and antiosteoporotic therapy (aoTh) were documented.17,19,20 The Timed-Up-and-Go Test (TuG) was recorded by the physician at T1 and from T3 to T7, as well as the mobility of the patient at any point in time, using a five-point Likert scale. In addition, assessments such as the Barthel index, 21 ODI 22 and EQ5D-5L 23 were documented at all time points. The item anxiety/depression of the EQ5D-5L was used to determine the level of anxiety.
The treatment decision was made by the physician at T2. The surgical therapy performed at T3 was recorded in 3 levels for invasiveness: level 1 for kyphoplasty or vertebroplasty, level 2 for short-segmental fixation with or without cement augmentation of the screws and augmentation of the index vertebra and level 3 for dorsoventral or long-segmental stabilization.
Finally, the data were analyzed and correlated with the anxiety/depression item of the EQ5D-5L. This item is measured on a five-point Likert scale, describing the subjective anxiousness of the patients: not, slightly, moderately, severely, or extremely anxious/depressed.
Data Analysis
An individual follow-up was planned for shortly after discharge and close to 8 weeks. This also ensured data acquisition from as many patients as possible.
To identify a possible difference in anxiety patterns of patients with OVCF at T1, the chi-square test was used to determine the contingency coefficient. In addition, Spearman correlation was used to detect a correlation between the severity of OVCF and the amount of anxiety at T1.
The effect of measures implemented during hospitalization (T1-T3) on the patients’ anxiety was tested using the General Linear Model for repeated measures (GLM). The aoTh status, which includes the unspecific treatments calcium and vitamin D as well as the specific ones like hormones, bisphosphonates and antibodies, served as a dependent variable. For analysis of the aoTh status, the patients were divided into 3 groups: no aoTh, preexisting aoTh and newly prescribed aoTh. Also the administration of analgesics according to the WHO ladder scheme, the type of therapy and the severity of the surgical intervention were used as dependent variables.
Finally, we tested whether the functional outcome of the individual changed at follow-up, depending on the degree of anxiety at T3. The GLM was applied, and the Bonferroni method was used post hoc to query the individual group differences. The Wilcoxon test was used to determine the significance of the correlation of the parameters that were chosen. TuG, mobility, Barthel index, ODI, and EQ5D-5L were chosen as dependent variables to represent functionality. Since the TuG excludes impossibility in its evaluation, it was supplemented by group 5 “bedriddenness.”
Results
689 patients were screened for this study of whom 534 patients could be initially enrolled. Data from 518 could be used. Reasons for subsequent exclusion were loss in follow-up (n = 15) or subsequent withdrawal of study consent after discharge (n = 1). Of the 518 patients, 75% were female. The mean age was 75 ± 10 years (41–97). An FU beyond discharge was available from 478 patients. If no other explanation is presented, numerical values are always given as the mean values.
In the first results section, the effect of therapeutic interventions such as prescription aoTh, drug pain management, mode of therapy (surgical vs conservative), and invasiveness of surgical therapy on anxiety is presented. In the second part, the relationship between anxiety status at discharge and outcome to FU is presented.
Predictive Factors of Anxiety
There was no significant correlation between anxiety and cause of fracture (trauma vs insufficiency) (P = .416). The variance in anxiety of patients with trauma fracture did not differ significantly from that of patients with OVCF in general (chi-square test: P = .634).
Fracture severity by OF classification and anxiety on admission correlated weakly (r = .087, P = .0496, n = 517).
Influence of Therapeutic Interventions on Anxiety
The analysis of the aoTh of patients was conducted in 3 groups: preexisting aoTh, new aoTh prescribed during hospitalization, and no aoTh at all. Patients with newly prescribed aoTh demonstrated a significant reduction in anxiety (P < .001, n = 485) from T1 (2.432) to T3 (1.975).
Anxiety was significantly higher in patients receiving WHO step III analgesics than in those receiving step II medication (P = .005). Additionally, the anxiety of WHO step II-treated patients was also significantly higher than that of those receiving step I medication (P = .014). A correlation was found between a higher level of anxiety and higher analgesia in accordance with the WHO analgesic ladder (r = .144, P = .001, n = 486) (Figure 1). Influence of analgesic medication (WHO) on anxiety by WHO analgesic ladder group.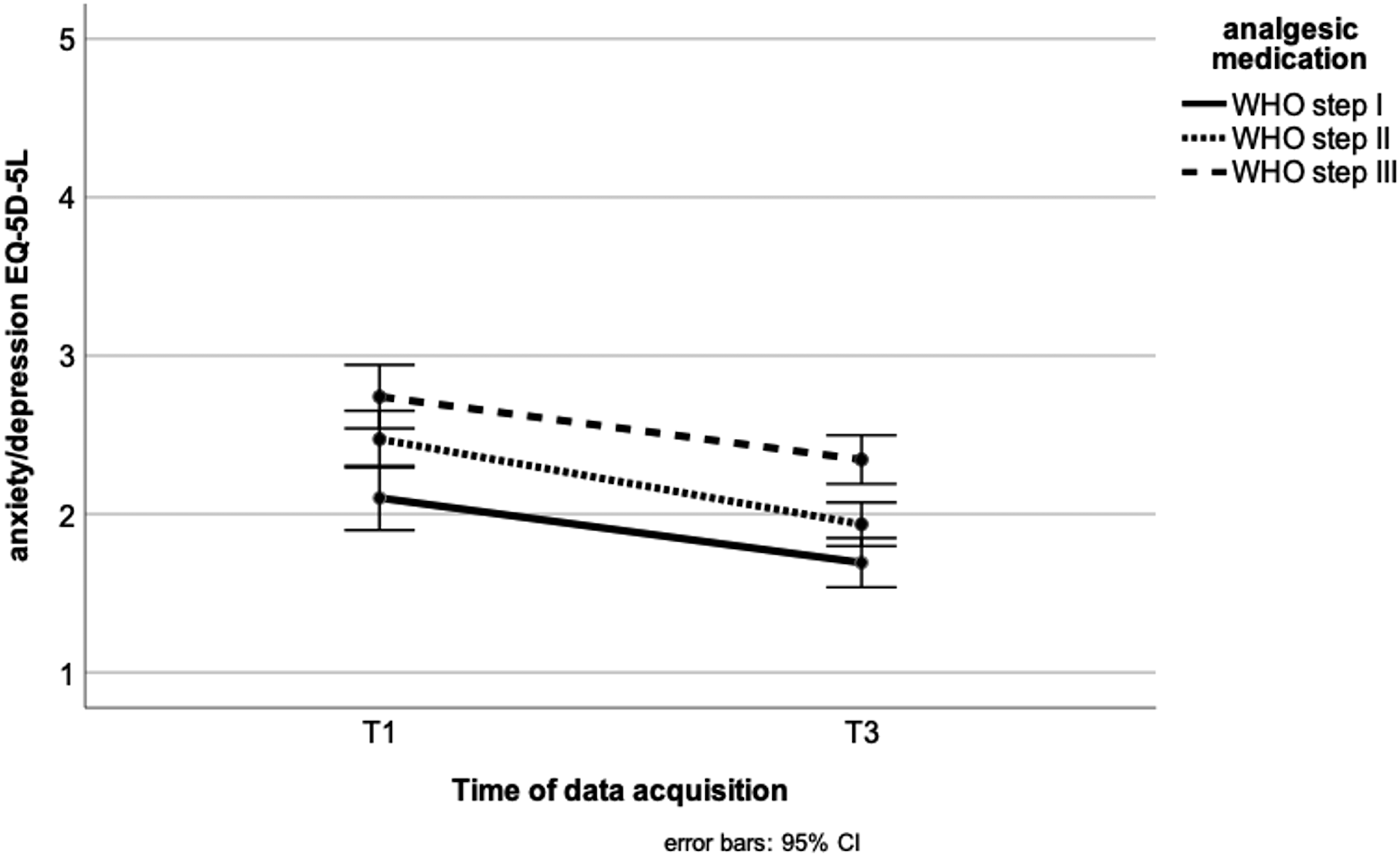
The conservative and surgical groups experienced a significant reduction in anxiety over the given period of time from T1 (mean = 2.400) until T3 (mean = 1.988) (P < .001, n = 488), but surgically treated patients’ anxiety was reduced even further over the course from T1 to T3 (interaction effect (P = .005)) (Figure 2). At T3, both groups reported the same level of pain severity. Influence of the chosen therapy.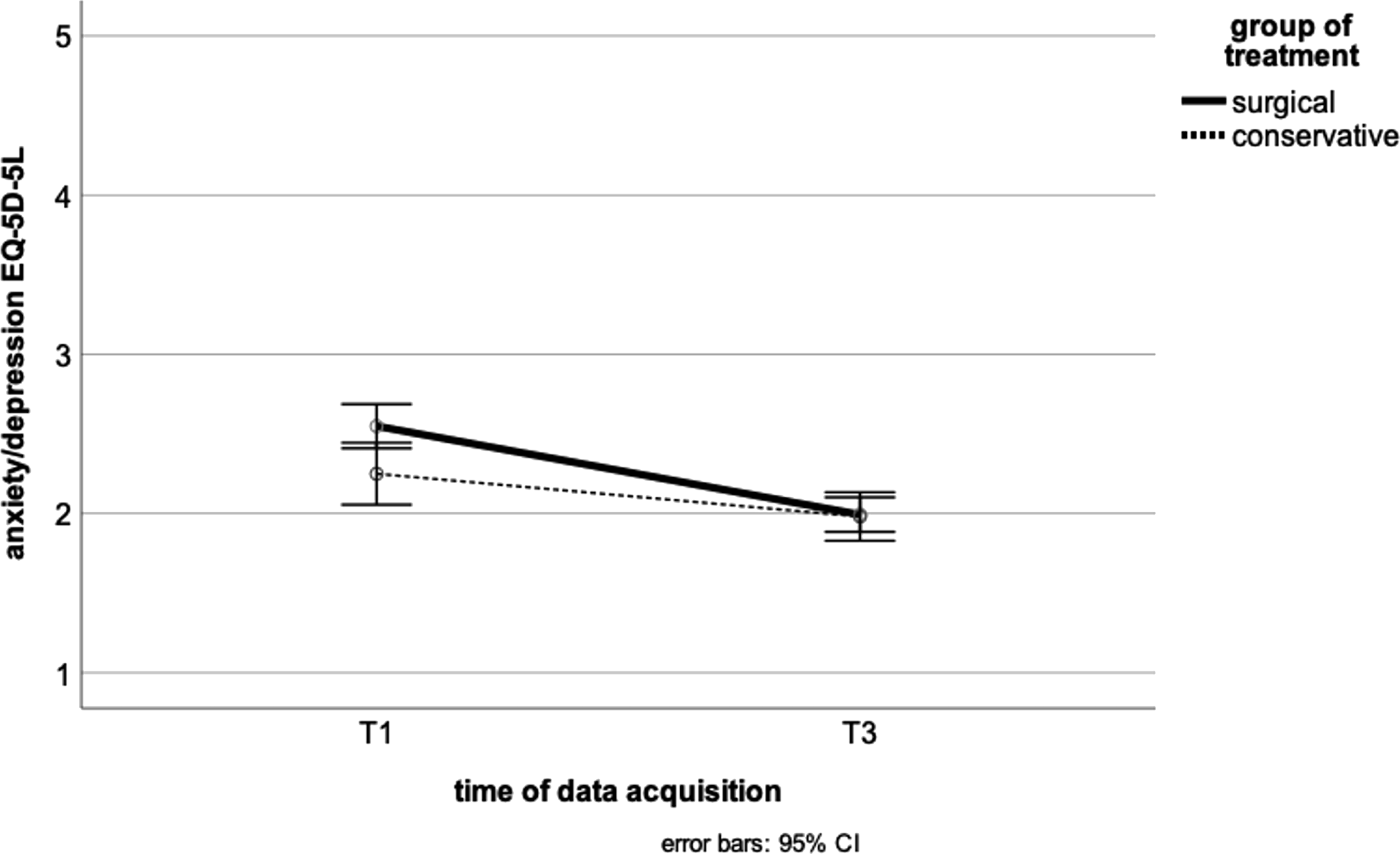
The invasiveness of surgery did not have a significantly different effect on anxiety reduction over time (P = .452, nlevel1 = 120, nlevel2 = 149, nlevel3 = 47). There was an equal reduction in anxiety over a period of time in all 3 groups (P = .493) (Figure 3). Influence of the severity of the surgical procedure.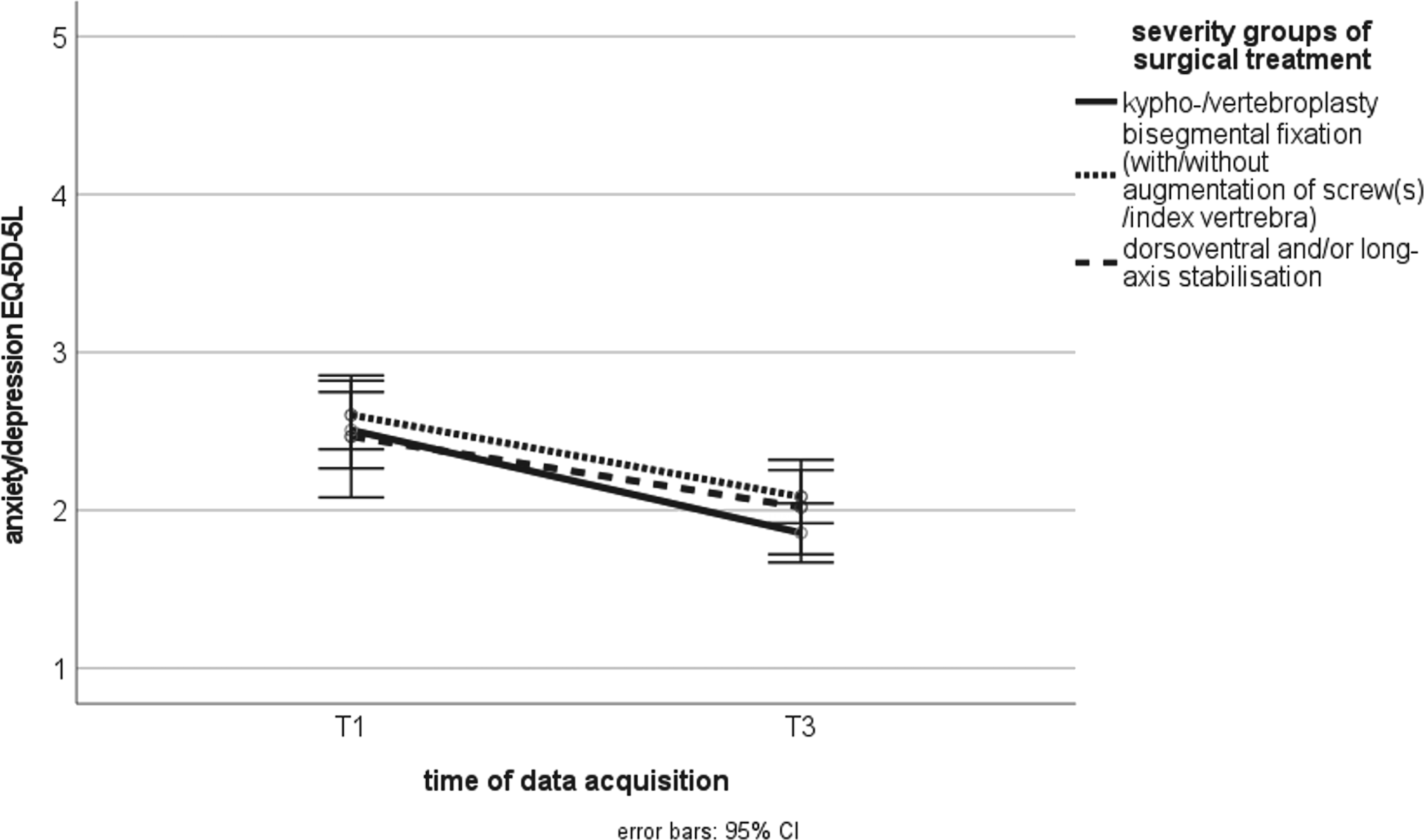
Impact of Anxiety on Outcome
Development of the item “anxiety/depression” at different functional outcome measurements.
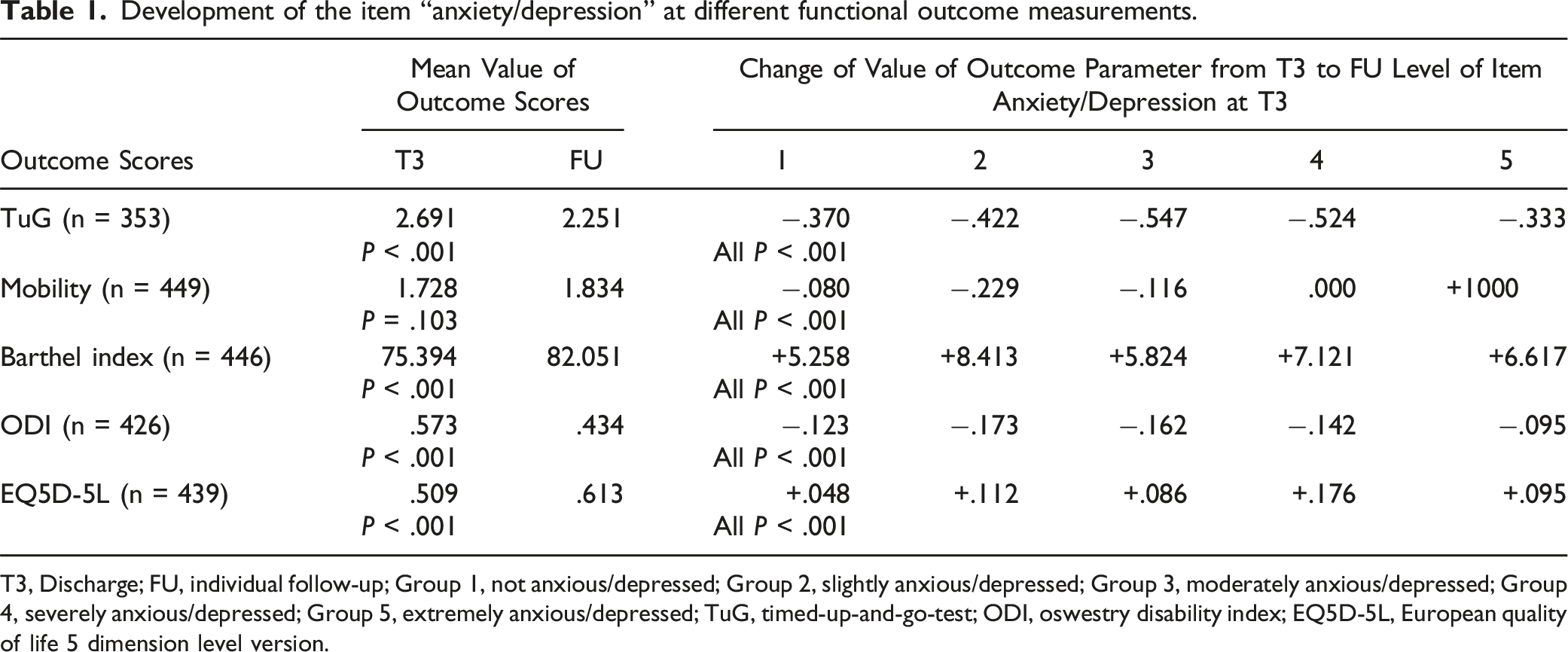
T3, Discharge; FU, individual follow-up; Group 1, not anxious/depressed; Group 2, slightly anxious/depressed; Group 3, moderately anxious/depressed; Group 4, severely anxious/depressed; Group 5, extremely anxious/depressed; TuG, timed-up-and-go-test; ODI, oswestry disability index; EQ5D-5L, European quality of life 5 dimension level version.
TuG Test
All non anxious or non depressed patients showed significantly better functionality in the TuG compared to those who were slightly (P = .002), moderately (P = .037) and severely anxious or depressed (P = .001). No significance could be found in relation to extremely anxious patients (P = 1.000).
Mobility
Patients who were found to be non anxious and non depressed (P = .024) as well as those who were slightly anxious and depressed (P < .001) at discharge improved significantly in mobility over time until follow-up. Moderately anxious (P = .061), severely anxious patients (P = 1.000) and extremely anxious patients (P = .250) plateaued in their level of mobility.
Barthel Index
The analysis revealed 3 groups of patients who had different scores on the Barthel Index depending on the anxiety/depression item: Non anxious patients scored better at follow-up than mildly and moderately anxious patients (P = .008, P = .048) and severely and extremely anxious patients (P < .001).
Oswestry-Disability Index
The improvement in functionality as measured by ODI from T3 to follow-up was significant for all groups except for the extremely anxious patients (P = .406).
EQ5D-5L
Non anxious and slightly anxious subjects did not differ significantly (P = .283), but both achieved significantly better results in functional outcome compared to severely and extremely anxious or depressed patients (P < .001).
The improvement in functionality from T3 to follow-up was significant in all groups except for the extremely anxious or depressed patients (P = .313).
Discussion
Anxiety may play an important role in patients suffering from OVCF. To the best of the authors’ knowledge, this study is the first to investigate whether the functional outcome of inpatients with OVCF is influenced by anxiety and depression. The assessment of the item “anxiety/depression” on the EQ5D-5L was used for the qualitative determination of anxiety in 518 patients included in a prospective multicenter study. The high number of 518 patients has the power to reveal significant correlations and dependencies even with low correlation coefficients.
The 17 participating hospitals, including level I and II trauma centers as well as spine specialty clinics, represents the broad range of hospitals performing spine surgery in German-speaking countries. Outpatient facilities are lacking.
The results should also provide information on whether a single item, which is fast and easy to assess, is suitable for a prospective state and determining functional outcome after osteoporotic vertebral body fracture.
The sex distribution, which is three-quarters women, corresponds to the respective proportion of patients with osteoporosis. 24
It seems interesting that fracture genesis (trauma vs insufficiency) has no relationship to anxiety at admission. Although there are no data on this in the literature, it seems plausible that patients with spontaneous fractures are more anxious because they fear further spontaneous fractures.
The significant and positive correlation between fracture severity by OF classification and anxiety suggests fracture severity as a risk factor for anxiety. However, this can only be used clinically to a limited extent because of the extremely weak correlation (r = .087), especially with regard to conflicting findings in the literature. 25
Patient anxiety decreased during inpatient treatment. A more nuanced view could reveal interesting details. In summary, anxiety could be influenced by treatments, such as aoTH, analgesia, conservative or surgical treatment during hospitalization, but it was not possible to delineate specific measures within the study.
According to the empirical impression during the patient interviews at the time of the study, anxiety decreased with the administration of aoTh. Statistically, this effect can be shown but it is also evident in other subgroups.
When examining the relationship between anxiety and the use of painkillers, patients with a high consumption of analgesics were found to have a high level of anxiety. This correlation among patients with chronic pain is well documented in the literature. 26
Regarding therapy, whether a patient was finally treated surgically or conservatively, it was clear that the anxiety of the surgically treated patients decreased significantly more in the inpatient setting. This may be caused by the intervention effect of the operation per se and/or due to increased discussions during the hospital stay, for example, acquiring additional surgical information. The influence of a longer hospital stay compared to conservative therapies had previously been excluded.
The examination of the relationship between the invasiveness of the surgical procedure and anxiety showed that there was no significant relationship, which seems surprising, as 1 would assume that a more invasive operation would cause more anxiety. It is interesting in this context that vertebro- or kyphoplasty is equivalent to anterior-posterior fixation from the patient's point of view. The operation causes patient anxiety.
The results also show that the level of anxiety of patients at the time of discharge has an influence on the functional outcome at follow-up. According to the TuG index, Barthel index, ODI and EQ5D-5L, significantly poorer functionality in the groups suffering from severe anxiety (level 4 and 5) was revealed. Regarding mobility, the patients with anxiety level 4 and 5 were also worse, patients with level 4 showed little improvement until the follow-up examination, and the patients with level 5 anxiety had the worst outcome. The more anxious a patient was at the time of discharge, the worse his functional outcome was at follow-up. This was also shown in the context of hip fractures. 5
The present analyses provide the opportunity to close a gap in the current state of research. Osteoporosis as an underlying disease is increasing annually 27 and subsequently the probability of an osteoporotic fracture. 28 However, anxiety as an influencing parameter on the outcome of patients suffering from OVCF has not yet been conclusively calculated. In particular, patients in this age group suffer from anxiety and depression. The meta-analysis by Cole and Dendukuri in 2003 identified “disability” and “female gender” in 58- to 85-year-olds as significant influencers for depression.29,30 This would imply an increased risk for the expression of a depressive disorder for at least three-quarters of the patients included in the present study.
It is well known that depressive symptoms can delay healing processes or even intensify disability.30–32 Similarly, the prospective cohort study by Becher et al. in 2014 showed a rate of depressive moods of 52.7% in trauma patients at the time of hospitalization after their accidents. 7 In addition, the follow-up examinations in the comparative study showed that depression is a significant factor for poorer outcomes.
As Dubljanin Raspopović et al (2014) and Trief et al (2000) have already confirmed, screening for anxiety and depression can filter patients at increased risk for poor functional outcome.5,8 In addition, consideration should be given to specifically addressing these psychological factors to generate the best possible outcome for the patient. 33
Limitations
For the heterogeneous collective, the choice of a randomized, controlled study would have been more favorable for homogenization. However, all patients received access to the best therapy possible and guideline-adapted interventions, according to the expertise of the practitioner or examiner. The questions asked about the ability to influence the anxiety of a patient with an OVCF could not be clarified. The influence of anxiety on the functional outcome of those patients could therefore only be answered with reservations. In particular, the insufficiently proven validity of the item anxiety/depression of the EQ5D-5L as a stand-alone predictive parameter requires further clarification. For validation, the inclusion of another assessment that evaluates the general mental state of patients would be a desirable addition to the questionnaire.
Further, no testing of anxiety before hospital stay was examined. The effect of chronical illnesses was not included in the analysis. Also the pre- and post-stationary social environment was not investigated.
The follow-up period of up to 12 months is limited but sufficient to answer the research question formulated at the beginning of this study.
Conclusion
Patients suffering from OVCF with high and extreme anxiety have an increased risk for a worse outcome.
The item for anxiety and depression on the EQ5D-5L is easy to measure and shows significant correlations with the need for analgesics and the outcome, which may serve as a reference for clinical practice. Whether supportive psychological measures improve outcomes for anxious patients requires further investigation in prospective studies.
Footnotes
Author Contributions
The working group Osteoporotic Fractures of the Spine Section of the German Society for Orthopaedics and Trauma (DGOU) conceived and designed the study. F. Schwarz, E. Klee, and B. W. Ullrich wrote the manuscript, searched the literature, and managed the data. P. Schenk performed statistical analyses and managed the data. Additional coauthors were responsible for data collection and patient management at the respective spine centers.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the research ethics committee of the Medical Association of Saxony-Anhalt Germany (14 June 2017, file number 31/17) and was performed in accordance with the principles laid down in the current revision of the Declaration of Helsinki.
Informed Consent
The authors give consent for publication of this manuscript.
Data Availability Statement
The datasets used and analyzed in this study are available on reasonable request from the corresponding author.