
Abstract
Study Design
Retrospective cohort study.
Objective
Lumbosacral transitional vertebra (LSTV) results in numerical alterations of the lumbar and sacral segments. Literature concerning true prevalence, associated disc degeneration, and variation in numerous anatomical landmarks concerning LSTV is lacking.
Methods
This is a retrospective cohort study. The prevalence of LSTV was determined in whole spine MRIs of 2011 poly-trauma patients. LSTV was identified as sacralization (LSTV-S) or lumbarization (LSTV-L) and further sub-classified into Castellvi’s and O’Driscoll’s type respectively. Disc degeneration was evaluated using Pfirmann grading. Variation in important anatomical landmarks was also analysed.
Results
Prevalence of LSTV was 11.6% with 82% having LSTV-S
Conclusion
The overall prevalence of LSTV was 11.6%, with sacralization accounting for more than 80%. LSTV is associated with disc degeneration and a variation in the levels of important anatomical landmarks.
Keywords
Introduction
Lumbosacral transitional vertebrae (LSTV) is a common congenital anomaly of the lumbosacral (LS) spine, 1 which manifests either as sacralization of the lowest lumbar vertebra (LSTV-S) or lumbarization of the upper sacral vertebra (LSTV-L). Sacralization refers to variable assimilation of the fifth lumbar vertebra to the sacrum, whose presentation ranges from enlarged transverse processes to complete assimilation. Lumbarization refers to transformation of the first sacral vertebra to varying degrees of lumbar configuration, with presentations ranging from squared appearance to well-formed lumbar facet joints. 2 The prevalence of LSTV varies between 4% and 30%3-8 with a mean prevalence of 12.3%. Sacralization is reported to be more frequent with a 7.5% prevalence, while lumbarization is seen in 5.5% of the population. 9 This substantial variation observed in the literature is due to the large heterogeneity in the imaging modalities and techniques employed in identifying these anomalies. While certain studies used plain pelvic radiographs for identifying LSTV, 4 others employed KUB,1,5 plain lumbosacral radiographs, 6 films of cervicothoracic and thoracolumbar spine, 9 and lumbosacral MRI. 10 Morphologically, LSTV includes varied presentations with complete transition resulting in numerical alterations of the lumbar and the sacral segments. Accurate recognition of LSTV is hence crucial to prevent spinal surgery performed at an incorrect level. Whole spine MRIs have enabled us to utilize the most accurate method of determining LSTV by counting distally from the C2 vertebra. 5 MRI of the lumbo-sacral spine alone is unreliable as reported by Bernhard et al. 11 In their study, there was a 7.7% increase in the rate of transitional vertebra when numerical variation was determined from whole spine MRI as compared to identification of LSTV through morphological changes in the lumbosacral spine MRI. The incidence of disc degeneration in patients with LSTV ranges from 10% to 39%. 12 The disc immediately cephalic to a LSTV has a significantly higher risk of degeneration.12,13 Whole spine MRIs enabled us to accurately analyze the status of the caudal 3 discs immediately cephalic to the transition vertebra in the study population. Various specialties in the medical field have used anatomical relations of vital neurovascular structures in reference to the spine. The termination of the conus medullaris, the level of the right renal artery, and the bifurcation of the abdominal aorta are among the most frequently used Ref. 14 Recognition of the TLCM is of clinical importance in diagnosing patients with neurological injuries due to fractures or tumors at the thoracolumbar junction (T12–L2) and while performing spinal needle insertion for spinal anesthesia or myelography. 15 The knowledge of variations in origin of renal arteries at different levels of vertebra is important before the kidney transplantation, as it has technical limitation in selecting the appropriate kidney (left or right) for laparoscopic procurement. 16 Generally both renal arteries originate from abdominal aorta at right angle below the origin of Superior Mesenteric Artery (SMA) between L1 and L2 vertebral intervertebral disc space. Identifying the level of bifurcation of the abdominal aorta accurately is important in surgical procedures involving the pelvis and in anterior surgical approaches to the lumbar vertebra. 14 There is a lacuna in the literature concerning the exact prevalence of LSTV based on whole spine MRIs and the variation in its relation to the different anatomical structures. Few studies have reported on the LSTV based on whole spine MRI, however, they are limited by a smaller study population and variable results11,17 With these in the background, the study proposes to determine (a) the prevalence of LSTV in asymptomatic patients on the whole spine MRI, and (b) to determine whether LSTV modifies the anatomical relationship of the vertebral column to the termination level of conus medullaris (TLCM), right renal artery (RRA) and abdominal aorta bifurcation (AA).
Materials and Methods
This retrospective observational analysis was conducted in a tertiary care center after obtaining approval from the institutional review board (Ref. No. IRB/TA/GH/ORTHO/11/2018/008), permitting a waiver of informed consent as this was a retrospective observational analysis of only the radiological images.
Skeletally mature poly-trauma patients (>18 years) who underwent whole spine magnetic resonance imaging (MRI) between 2009 and 2018 were enrolled in the study. All the radiological images were obtained from the hospital picture archiving and communication system (PACS). All MRI scans were screened for the presence of LSTV counting from C2 caudally. MRIs suggestive of lumbosacral injuries were excluded from evaluation. The enumeration was done starting from C2 vertebra distally irrespective of the type of transition. The sacralised L5 was still enumerated as L5 and the lumbarized S1 as S1 itself, with a mention of the type of transition. The sacralized and lumbarized vertebrae were classified using Castellvi’s [2] (on plain AP LS radiographs) and O’ Driscoll’s (on sagittal whole spine MRI) classifications, respectively.18,19 Based on the morphological characteristics and clinical relevance, Castellvi classified LSTV into 4 groups, Type 1- dysplastic transverse process: a, unilateral: b, bilateral, Type 2- incomplete lumbarization/sacralization: a, unilateral: b, bilateral, Type 3- complete lumbarization/sacralization: a, unilateral: b, bilateral, Type 4: mixed. O’Driscoll developed a classification system based on T1 and T2 weighted MRI images and the disc morphology of the uppermost sacral segment and the remainder of sacrum, where in Type 1 had no disc material, Type 2 had a small residual disc, and Type 3- well-formed disc. Type 4 had a well-formed disc extending along the entire AP diameter of the sacrum. The 3 discs immediately cephalic to the transition vertebra which includes, L2-L3, L3-L4 and L4-L5 incase of sacralization of L5 and L3-L4, L4-L5, and L5-S1 in case of Lumbarization of S1, were graded for degeneration by Pfirrmann’s grading using sagittal sections on MRI. The discs were labelled C, B, A cranio-caudally (Figure 1). ‘Positive disc degeneration’ was defined as Pfirrmann’s grading ≥3. The TLCM and the Ostia of the RRA were assessed on sagittal sections of the whole spine MRI while the AA was assessed on coronal sections. The height of posterior wall of the vertebra was divided into 3 equal parts and the anatomical structure was described in relation to the upper 1/3rd, middle 1/3rd and the lower 1/3rd of that vertebra. All the radiological assessments were separately done by an orthopedic resident and a spine fellow; which were further ratified by a senior spine surgeon. Degeneration assessed in the distal 3 mobile segments labelled as A, B, and C from the transition vertebra proximally.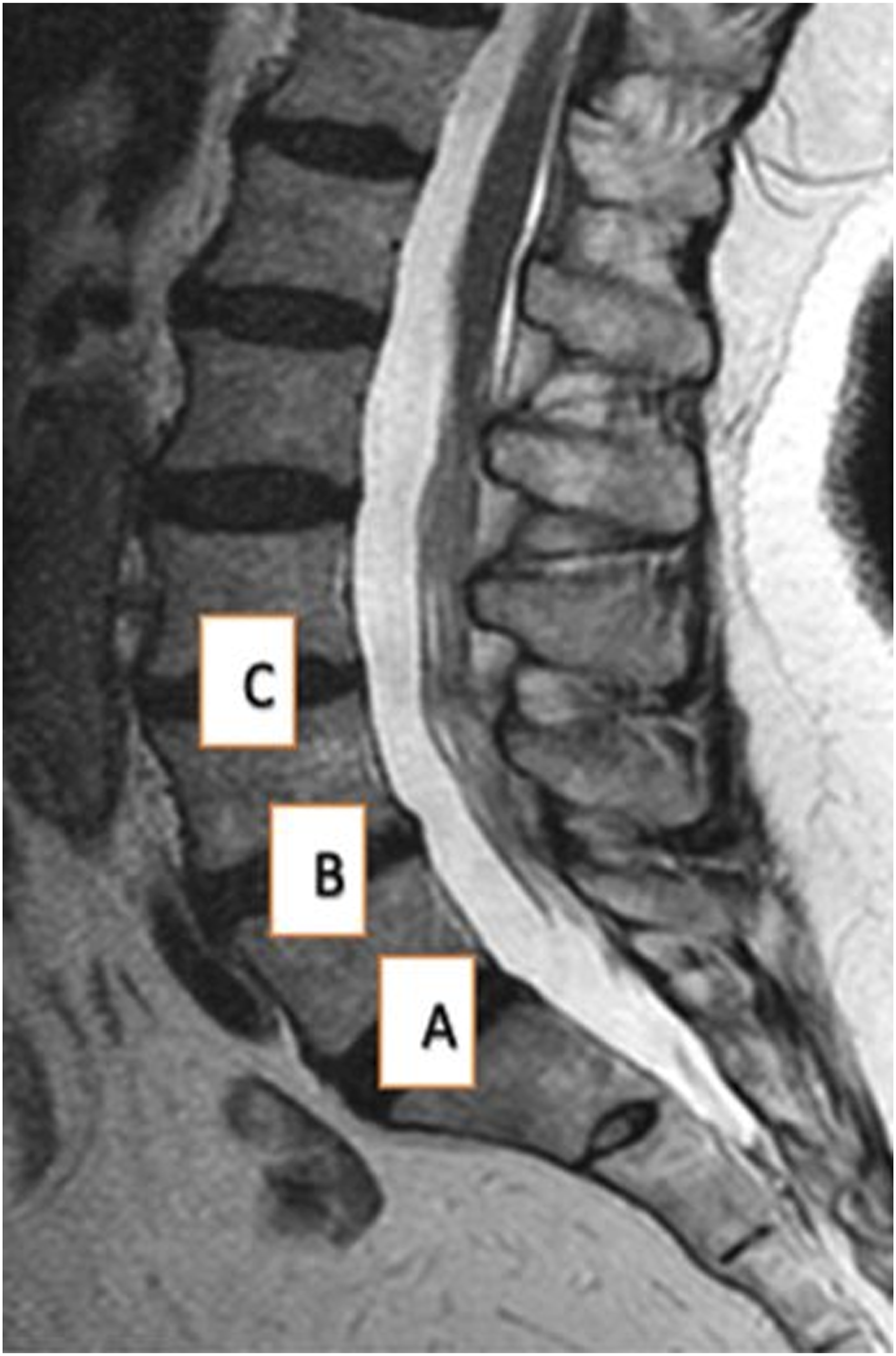
Data were analyzed using SPSS v21. The categorical data were presented as percentages and frequencies, and continuous data were presented as mean and standard deviation. The Chi-square test was used as a test of significance for categorical data. P value less than .05 was considered statistically significant.
Results
Prevalence of LSTV
The study included 1408 males and 603 females with a mean age of 48.5 ± 8.2 years. Two hundred and thirty-three patients (140 males and 93 females) had LSTV demonstrating an overall prevalence of 11.6%. Forty-two patients had LSTV-L; while 191 had LSTV-S. The prevalence of sacralization among female and male patients with LSTV was 86/93 (92.4%) and 105/140 (75.0%) respectively, and the prevalence of lumbarization in female and male patients with LSTV was 7/93 (7.5%) and 35/140 (25%) respectively.
Castellvi’s type 2A (Figure 2) was the most common type (33.6%). Castellvi types 1A, 1B, 2B, 3A, 3B, and 4 were prevalent at a rate of 6.3%, 9.4%, 16.2%, 6.2%, 27.2% and 1.1% respectively. The O’Driscoll type 4 (Figure 3) was the commonest sub-type (54.8%), while types 3 and 2 were observed in 38.1% and 7.1%, respectively. Castellvi’s type 2A-most common type of sacralization found in the study. O’Driscoll type 4- most common type of lumbarization found in the study.

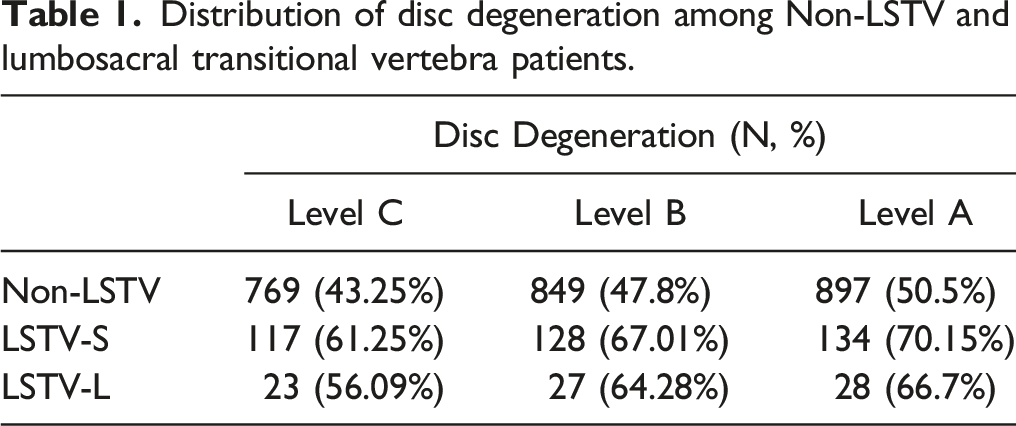
Distribution of disc degeneration among Non-LSTV and lumbosacral transitional vertebra patients.
Anatomical Relation of Termination of Conus Medullaris, Right Renal Artery, and Abdominal Aorta Bifurcation
Termination of Conus Medullaris
L1 vertebra was the TLCM in 92.1% of non-LSTV (upper L1- 19.2%, middle L1- 48.1%, lower L1- 24.1%), in 82.7% of LSTV-L (upper L1- 21.2%, middle L1- 40.2%, lower L1- 20.2%) and in 70.2% of LSTV-S patients (upper L1-47.2%, middle L1- 15.2%, lower L1- 7.2%).
Right Renal Artery
The level of RRA was at L1 vertebra in 71.02% of non-LSTV (upper L1- 20.02%, middle L1- 40.01%, lower L1- 10.01%), and 78.05% of LSTV-S patients (upper L1- 56.02%, middle L1- 15.02%, lower L1-6.02%). However, the RRA was seen at the L2 vertebral level in 77.06% of LSTV-L patients (upper L2- 35.02%, middle L2- 21.02%, lower L2- 20.07%).
Bifurcation of Abdominal Aorta
The abdominal aorta bifurcated at the L4 vertebral level in 83.03% of non-LSTV and 52.04% of LSTV-S patients, while the bifurcation was seen at the L5 vertebral level in 53.6% of LSTV-L patients.
Discussion
Since the initial description by Rosenberg et al. in 1876, LSTV has been well-acknowledged as the most common developmental anomaly of the vertebral column.20-22 The relevance of this anatomical variation in different clinical scenarios and its role in the causation of lower back or radicular pain has been debated over decades.9,20,21,23,24 LSTV also has its implications for various aspects of patient care like a poorer response to conservative treatment and interventions like epidural injections, poorer outcomes after decompression-only procedures, and a higher need for instrumented fusion.21,25-29 However, an important yet less emphasized-upon implication of this condition in clinical situations is in the context of the enumeration of the vertebral levels. 30 Any ambiguity in identifying LSTV or other discrepancies in the numbering of vertebral segments can lead to substantial confusion in identifying the level of true pathology. 31 If not carefully considered, this can pave the way for serious complications, including wrong-level surgeries. With this background, the importance of our current study cannot be understated. Despite the existence of a significant volume of published research on the epidemiological aspects of LSTV, its true prevalence, clinical relevance, or variations in anatomical structures with respect to the vertebral segments is largely unknown.10,32 The present study addressed these concerns using whole spine MRIs.
There is a substantial variation in the prevalence of LSTV in literature, which has been reported to vary between 4% and 30% across various studies.3-8 This is attributed to the large heterogeneity in the imaging modalities and techniques employed in identifying these anomalies. Various modalities including radiographs, 4 and lumbosacral MRI 10 allow for a limited visualization of the particular segment of the spine and identification of the transition largely depends on identifying the morphology of the transition vertebra using the criteria described by O’Driscoll et al. 19 However, this has undermined the true prevalence due to the subjective errors in accurately identifying the morphological changes. Whole spine MRIs enabled us to utilize the most accurate method of determining LSTV by counting distally from the C2 vertebra. 5
The current study demonstrates an 11.6% overall prevalence of LSTV with sacralization in 81.9%, and lumbarization in 18.1%. Castellvi 2 A was the most common sub-type (33.6%), followed by 3B (27.2%) and 2B (16.2%) similar to previously reported literature. 1 O’ Driscoll type 4 was the commonest subtype of LSTV-L (54.8%) in our study, which was more than that reported previously. 7 Though LSTV was more prevalent in men, sacralization had an overall higher incidence in women.
Various studies in the past had reported a higher prevalence of disc degeneration in patients with LSTV.33,34 A majority of these studies reported higher degeneration only at the levels immediately proximal to the transitional levels 33 Such a pattern was explained by the higher distribution of stresses at these specific disc levels and the instability of the spinal segment proximal to the transition due to the weak ilio-lumbar ligament, which is expected in the mobile segments immediately proximal to the transitional vertebra. Luoma et al. 33 revealed that degeneration was significantly higher at the level immediately cephalad to transitional level, while it was lower at the caudad level. However, Hanhivaara 32 reported that increased disc degeneration was restricted not only to the lower lumbar levels but also extended across the upper lumbar vertebrae (L1-2 or L2-3). Our study demonstrates significantly advanced degeneration of the 3 discs immediately cephalad to the transitional vertebra in both the LSTV-S and LSTV-L groups as compared to the non-LSTV group (P < .05).
LSTV can result in distinct anatomical changes at the lumbosacral junction and in the surrounding structures. The anatomical markers including abdominal aortic bifurcation, right renal artery, and termination of conus medullaris level have been reported to be reliable landmarks for determining lumbar vertebral segments on MR imaging. 14 The accurate identification and assessment of these anatomical structures in relation to the spinal segments play a crucial role in eliminating anesthetic, surgical, and various procedural errors. Chang 14 studied the lumbo-sacral MRI of 210 patients to evaluate the anatomical significance and sites of aortic bifurcation, right renal artery and conus medullaris when locating lumbar vertebral segments on MRI. He concluded that aortic bifurcation, the right renal artery and the combination of these structures are reliable landmarks for determining the lumbar vertebral segments on MRI or CT. Chithriki similarly performed a prospective study of 441 patients to determine the reliability of aortic bifurcation concerning the lumbar levels. 35 The study however, concluded that the stability of the aortic bifurcation as a landmark was disturbed by the significant high incidence of lumbosacral transitional segments.
Recognition of the TLCM is of clinical importance in diagnosing patients with neurological injuries resulting from fractures or tumors at the thoracolumbar junction (T12–L2). It is also vital during spinal needle insertion for spinal anesthesia or myelography 15 as interventions concerning epidural injections are performed distal to the TLCM. Hence knowledge of this land mark would aid in administration of the injection at the appropriate spinal level. Our study determined that the median TLCM in the non- LSTV group and the lumbarization group was at middle L1 (48.1% and 40.2%) while in the sacralization of L5 group, it was at upper L1 (47.2%). These results suggest that the presence of LSTV affects the relation of the TLCM with the vertebral segments. Kim et al 36 studied the MRI of 690 patients aged less than 20 years and reported similar results. However, their study was based on an MRI of the lumbar spine.
Knowledge of anomalous origin of renal arteries serves as the road map before surgery. If surgeons have knowledge about this, they can minimize the trauma to the vessels during various surgical procedure like donor nephrectomy, repair of renal artery aneurysm and endourological procedures. 16 The RRA arises from the anterolateral part of the aorta and is easy to assess on the sagittal MRI scan. Generally, the ostium of the RRA lies between the lower third of the L1 vertebra and the upper third of the L2 vertebra, slightly below the level of the superior mesenteric artery16,37,38 which may be useful to identify lumbar levels on sagittal MRI. Our study shows that the median level of RRA in non- LSTV patients was most common at middle L1 (40.0%) while in the LSTV-L and LSTV-S patients, it was more common at upper L1 level (35.2% and 56.2% respectively).
Literature classically describes the bifurcation of the aorta into the 2 common iliac arteries at the level of the L4 vertebral body. 14 Identifying the level accurately is important in surgical procedures involving the pelvis and in anterior surgical approaches to the lumbar vertebra. The main complications of the anterior transperitoneal approach and anterolateral retroperitoneum approach of lower lumbar vertebra are the vessels injuries mainly at the level of aortic bifurcation. These approaches access the lumbosacral spine distal to the confluence of the aortic bifurcation however, distal bifurcations may result in inadverent injuries to these vessels.39,40 Accurate identification of the bifurcation also plays a role on the extent of spine surgeries that may be performed. In a study by Thomas et al, L4-S1 resulted in ejaculatory dysfunction in 63% of patients in whom the bifurcation occurred distal to the L4-L5 disc space, while none of the patients in whom the bifurcation of the aorta occurred proximal to the disc space developed ejaculatory dysfunction. 41 Our study shows that the median level of AA in non-LSTV patients and LSTV-S patients was most common at middle L4 (83.3% and 52.04% respectively). However, in LSTV-L patients, the most common level was middle L5 (53.6%). It is, therefore, necessary to review whole spine MRIs accurately to identify the aortic bifurcation during pre-operative planning. The strength of our study lies in the utilization of whole spine MRIs of poly-trauma patients which is a better indicator of the true prevalence among the general population but is limited by its retrospective nature and lack of clinical correlation.
Conclusion
LSTV is the most common developmental anomaly of the lumbosacral spine with an overall prevalence of 11.4% of which sacralization constituted 82%. The most common type of sacralization was Castellvi’s type 2A while the O’Driscoll type 4 ranked first in the lumbarization group. There is significant disc degeneration affecting the 3 levels adjacent to LSTV. There was variation in the anatomic relation of vital landmarks including termination of the Conus medullaris, ostium of the right renal artery, and the bifurcation of the abdominal aorta in patients with LSTV. It is important to recognize the enumeration of the spinal segments as well as alteration of the important anatomic landmarks to prevent wrong-level surgery, aid in surgical approaches, and decide the extent of specific surgeries.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.