
Abstract
Study Design
Retrospective Study.
Objectives
The selection of floating fusion or lumbosacral fusion arises when treating patients with instability or stenosis of the lower lumbar spine concomitantly radiographic degeneration of L5-S1. This study aimed to investigate the preoperative anatomical or morphological factors affecting the survivorship of the L5-S1 after floating fusion.
Methods
This study included 77 patients who had undergone floating fusion surgery through the TLIF approach. Preoperative radiographic parameters were evaluated using anteroposterior and lateral lumbar spine radiographs. The patients were divided into two groups according to the Modified Pfirrmann Grading and total endplate score. Multivariable regression analysis was performed to explore the relationships between the anatomical or morphological characteristics of L5 and the degeneration of L5-S1.
Results
The disc degeneration group exhibited a smaller height ratio of the iliac crest (H i ) and a less L5 deep position. Furthermore, the right/left height of L4 (H r /H l ) and the right/left width of transverse process of L5 (C Rt /C Lt ) were significantly higher in the disc and endplate degeneration groups. Multiple logistic regression analysis revealed that H i and C Rt were independently associated with L5-S1 disc degeneration, whereas H r was a significant risk factor for L5-S1 endplate degeneration.
Conclusion
Anatomical and morphological characteristics of L5, such as smaller H i , higher C Rt and H r , were associated with an increased risk of L5-S1 degeneration in patients after floating fusion. These findings may indicate the fusion level when addressing lower lumbar degenerative diseases and the concurrent radiographic degeneration of L5-S1.
Introduction
Harms first proposed transforaminal lumbar interbody fusion (TLIF) as a standard spinal fusion procedure that the spine surgeons have widely accepted for lumbar degenerative diseases or pathologic conditions. 1 The common denominator of floating fusion in lumbar spinal fusion is excluding the lumbosacral joint from the fusion mass, which means fusion stops at L5 segment. 2 However, long-term follow-up of patients with lumbar fusion has revealed several complications, including adjacent segment degeneration (ASD), which occurrs in more than 15% of the population. 3 Floating fusion is a risk factor for adjacent segment degeneration and adjacent segment disease after lumbar spinal fusion surgery.3-5 Patient outcomes and satisfaction levels deteriorated after the onset of adjacent segment degeneration. 6 Therefore, lumbosacral fusion was suggested in patients with sagittal imbalance and lumbar hyperlordosis, even with minimal L5-S1 disc degeneration simultaneously. 7 Nevertheless, lumbosacral fusion leads to a reduction in the range of spinal motion, generally no less than 20°. 8 Furthermore, several recent studies have suggested that in the absence of severe lumbar degeneration or neurological symptoms, it is unnecessary to routinely extend the fusion to sacrum when treating patients with instability or stenosis of the lower lumbar spine.9-11 Currently, there is a lack of conclusive evidence regarding the superiority of floating fusion over lumbosacral fusion.
Notably, innate characteristics of the lumbosacral junction may determine the site of disc degeneration. 12 Although some previous studies demonstrated that the position of the L5 vertebra relative to the intercrestal line was not correlated with the subsequent L5–S1 segment degeneration 13 or curve progression, 14 other studies have revealed the intercrestal line passing through the L5 vertebra can exacerbate the progression of degenerative lumbar scoliosis.15,16
However, no prior studies have investigated the preoperative anatomical and morphological factors of L5 that affect the survivorship of disc and endplate of L5-S1 after lumbar floating fusion surgery through the TLIF approach. Therefore, we aimed to (1) evaluate the preoperative anatomical and morphological factors of L5 vertebra in patient undergoing floating fusion and (2) explore the potential preoperative risk factors affecting the survivorship of disc and endplate of L5-S1 after lumbar floating fusion surgery.
Methods
Study Design and Patient Population
We conducted a retrospective study and examined the data of patients with degenerative lumbar diseases who underwent spinal surgery through the TLIF approach at our institution between March 2008 and December 2018. This study was approved by the Independent Ethics Committee (IEC) of Zhangjiagang Hospital affiliated to Soochow University (RL-202209001). The procedures were proformed according to the guidelines of the ethics review board.
The inclusion criteria were as follows: (1) age > 40 years, (2) fusion levels < 3, and (3) follow-up time > 36 months. The exclusion criteria were as follows: (1) abnormalities or fractures at the lumbosacral spine, (2) revision procedures; (3) lumbosacral transitional vertebra, and (4) pre-existing infective lesions. Demographic information of patients including gender and age, and radiographic parameters were recorded for further analysis.
Radiographic Measures
Basic radiographic parameters were measured preoperatively on anteroposterior and lateral lumbar spine radiographs. The following radiographic parameters of spinal alignment in the coronal and sagittal plane were measured on anteroposterior and lateral radiographs, respectively (Figure 1): 1. The height and width of the iliac crest (H
i
and B
i
): the distance from the intercrestal line to the midpoint of the superior margin of the sacrum, the distance through the intermediary caudal margin of the two transverse processes of L5 between the iliac crests on both sides. 2. Width, right, and left height of the L4 vertebral body (B
v4
, H
r
, and H
l
). 3. Interpediculate distance, right and left width of the transverse process of the L5 vertebra (A, C
Rt
and C
Lt
). 4. The depth of the L5 vertebra (D): the vertical distance from the center of the L5 pedicles to the intercrestal line. 5. Lumbar lordosis and L5-S1 lordosis (LL and LSL). Anterior-posterior lumbar spine radiograph (A). Views of high magnification of red box (B) (C). This radiograph demonstrates the measurements of the left width of the L5 vertebra (C
Lt
), the right width of the transverse process of the L5 vertebra (C
Rt
) and the inter pediculate distance of the L5 vertebra (B). This radiograph illustrates the measurements of the height of the iliac crest (H
i
), the width of the iliac crest (B
i
), the width of the L4 vertebral body (B
v4
), the left height of the L4 vertebral body (H
l
) and the right height of the L4 vertebral body (H
r
) (C).
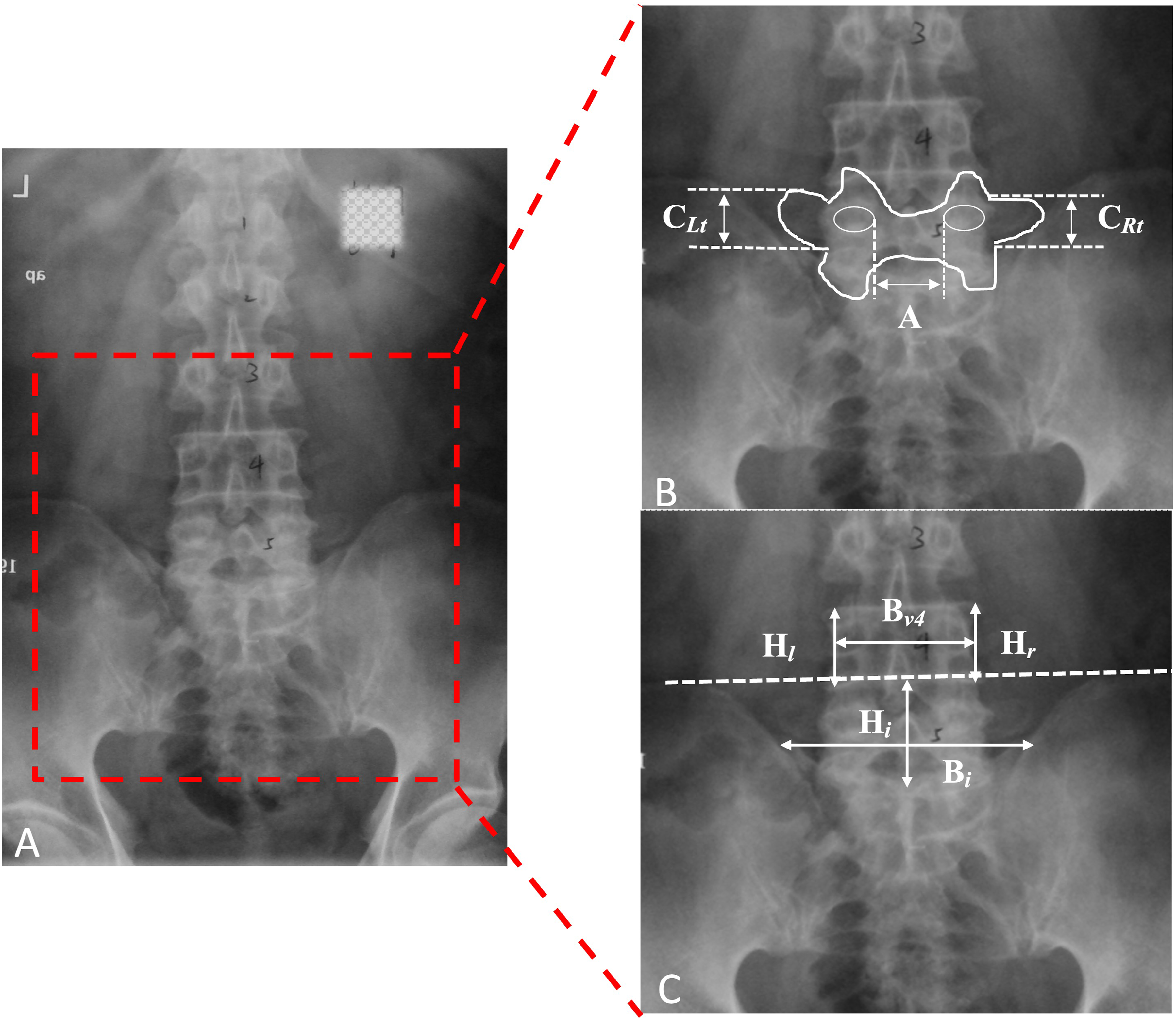
When the L5 pedicles were located below the intercrestal line, the depth was defined as negative (−), and vice versa. For all sagittal alignments, the angle was defined as negative (−) if the curve exhibited lordotic characteristics, whereas positive (+) for kyphotic. An orthopedic surgery recorded measurements in triplicate using Surgimap software (Nemaris, Inc, USA) and the average value was included in the study.
Lumbar Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) scans were acquired using a Siemens 1.5-T superconducting magnet (Munich, Germany), including sagittal T1/T2 weight images and axial T2 weight images. Grading was performed on sagittal T2 weight images that were obtained using a slice thickness of 4 mm and a time to recovery 3000-3600/time to echo (TE) 112. Endplate defect grade was calculated on a scale of 1-6 according to the study by Rajasekaran et al. 17 As described by Rajasekaran et al, 17 total endplate (TEP) scores for L5-S1 disc were conducted by summing the endplate defect score of both cephalic and caudal endplates. Disc degeneration was discriminated from grade 1 to grade 8 according to the Modified Pfirrmann Grading System proposed by Giffith et al. 18
The patients were divided into two groups according to the Modified Pfirrmann Grading and TEP scores of L5-S1, respectively. The non-degenerated group was defined as patients who did not experience a change in the Modified Pfirrmann Grading or TEP scores during the follow-up period.
Anatomical and Morphological Characteristics of the Low Lumbar Area
According to the previous study, the width and height of the L4 vertebral body could be measured as an alternative because the morphological characteristics of the L5 vertebrae were difficult to distinguish on anteroposterior radiographs. 19 The height ratio of the iliac crest of L4 (HR), width ratio of the iliac crest of L4 (WR), and relative thickness of the transverse process of the L5 vertebra (RT) were calculated using the following formulas: HR = 2H i /(H l + H r ), 19 WR = B v4 /B i , and RT = (C Lt + C Rt )/2A.12,20
Statistical Analysis
All analyses were performed using the IMB SPSS Statistics software (version 24.0, SPSS Inc., USA). Normality was determined using the Shapiro–Wilk test. Normally distributed parameters with homogeneity of variance data are expressed as mean ± standard deviation. The independent sample t-test was used to compare the differences between the non-degenerated and degenerated groups (disc or endplate). Categorical variables in two groups were compared using the chi-square test or Fisher’s exact test. Logistic regression analysis determined the associations between preoperative anatomical and morphological characteristics of the L5 vertebra and degeneration of the disc and endplate, respectively. Logistic regression was performed using the stepwise forward method. A P < 0.05 was considered statistically significant.
Results
The Demographic Data and Radiographic Parameters of Patients.
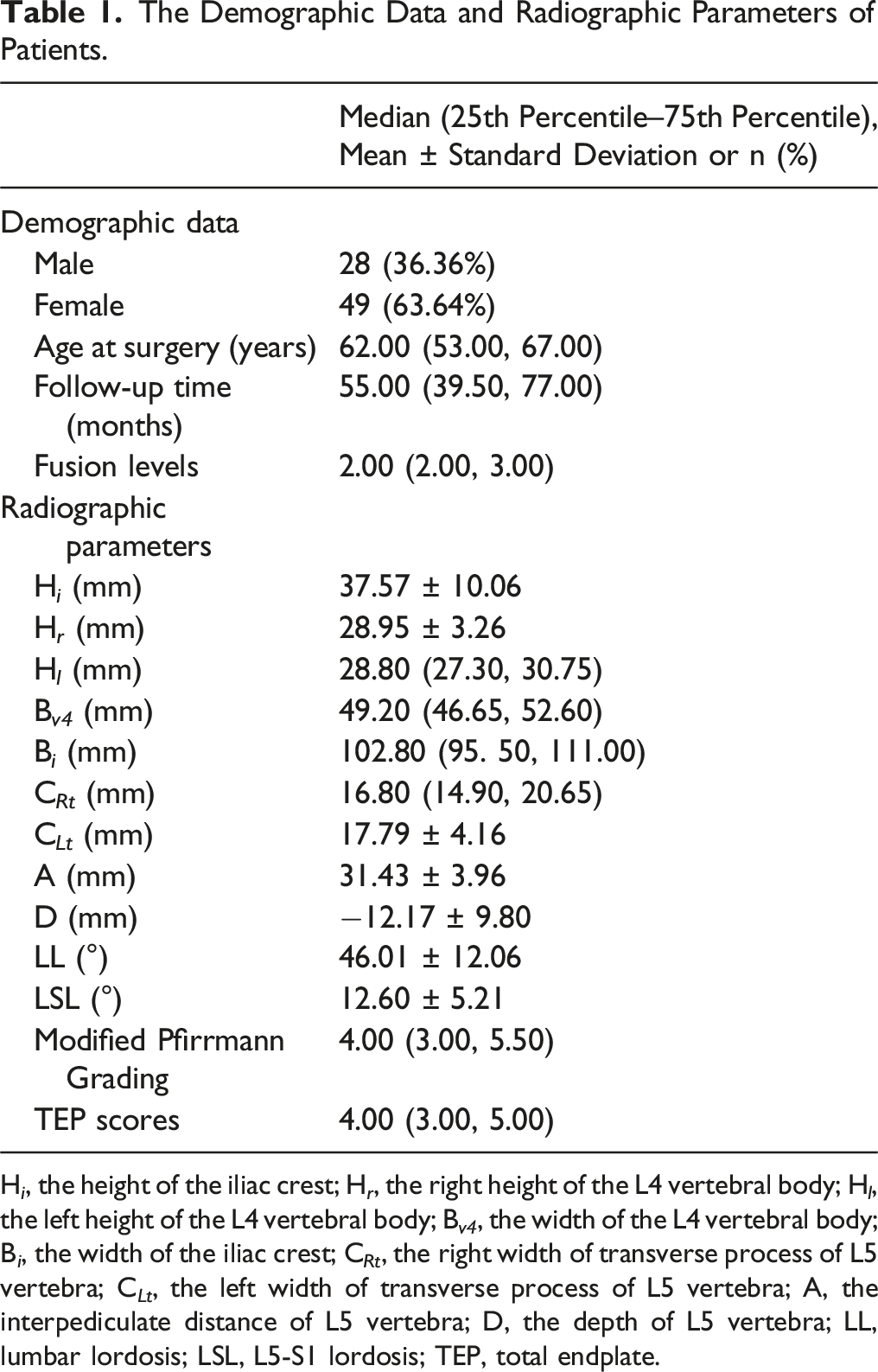
H i , the height of the iliac crest; H r , the right height of the L4 vertebral body; H l , the left height of the L4 vertebral body; B v4 , the width of the L4 vertebral body; B i , the width of the iliac crest; C Rt , the right width of transverse process of L5 vertebra; C Lt , the left width of transverse process of L5 vertebra; A, the interpediculate distance of L5 vertebra; D, the depth of L5 vertebra; LL, lumbar lordosis; LSL, L5-S1 lordosis; TEP, total endplate.
Comparisons of Demographic Data and Preoperative Radiographic Data of Patients Between Subgroups of Disc Degeneration.
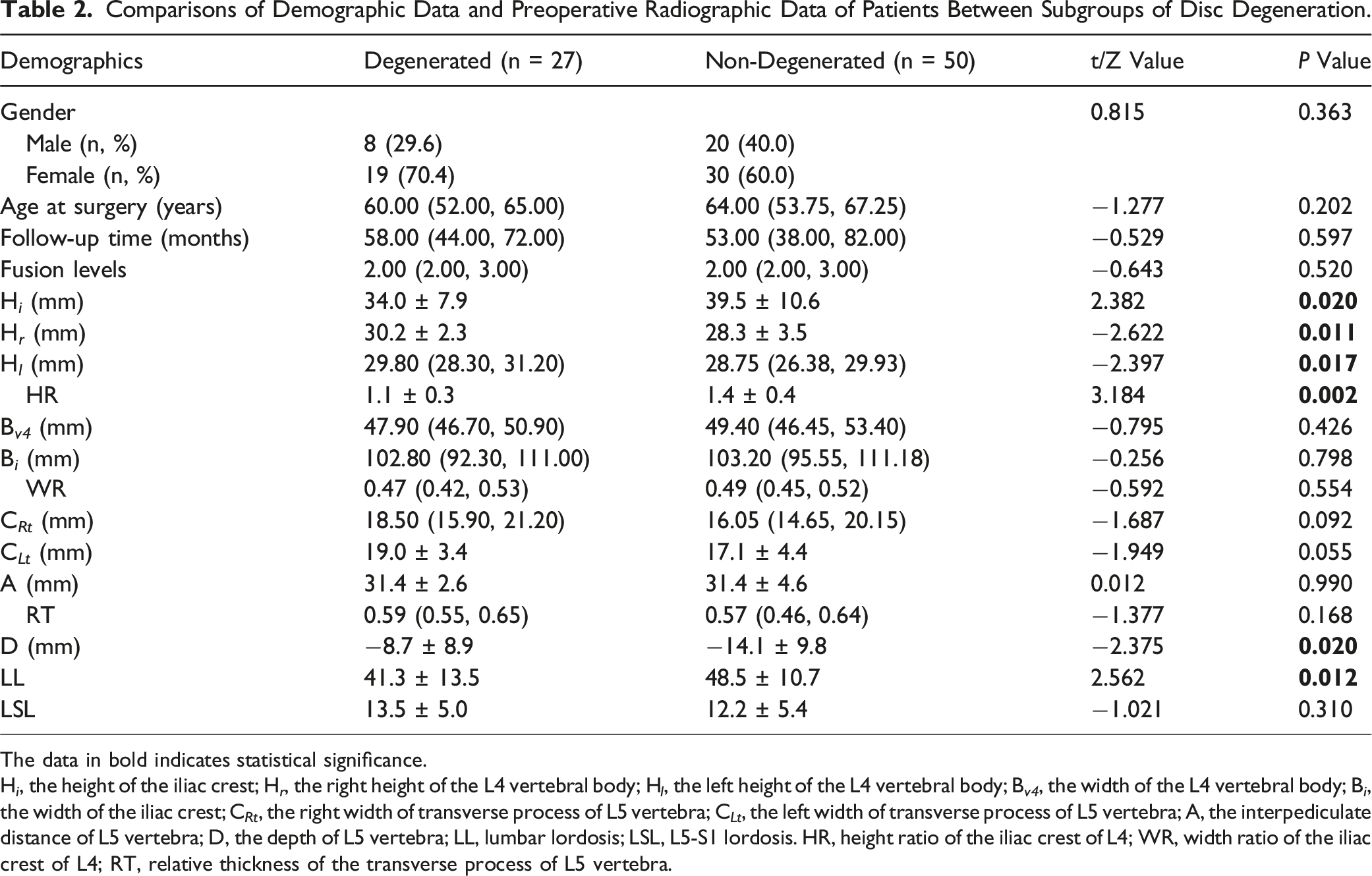
The data in bold indicates statistical significance.
H i , the height of the iliac crest; H r , the right height of the L4 vertebral body; H l , the left height of the L4 vertebral body; B v4 , the width of the L4 vertebral body; B i , the width of the iliac crest; C Rt , the right width of transverse process of L5 vertebra; C Lt , the left width of transverse process of L5 vertebra; A, the interpediculate distance of L5 vertebra; D, the depth of L5 vertebra; LL, lumbar lordosis; LSL, L5-S1 lordosis. HR, height ratio of the iliac crest of L4; WR, width ratio of the iliac crest of L4; RT, relative thickness of the transverse process of L5 vertebra.
Comparisons of Demographic Data and Preoperative Radiographic Data of Patients Between Subgroups of Endplate Degeneration.
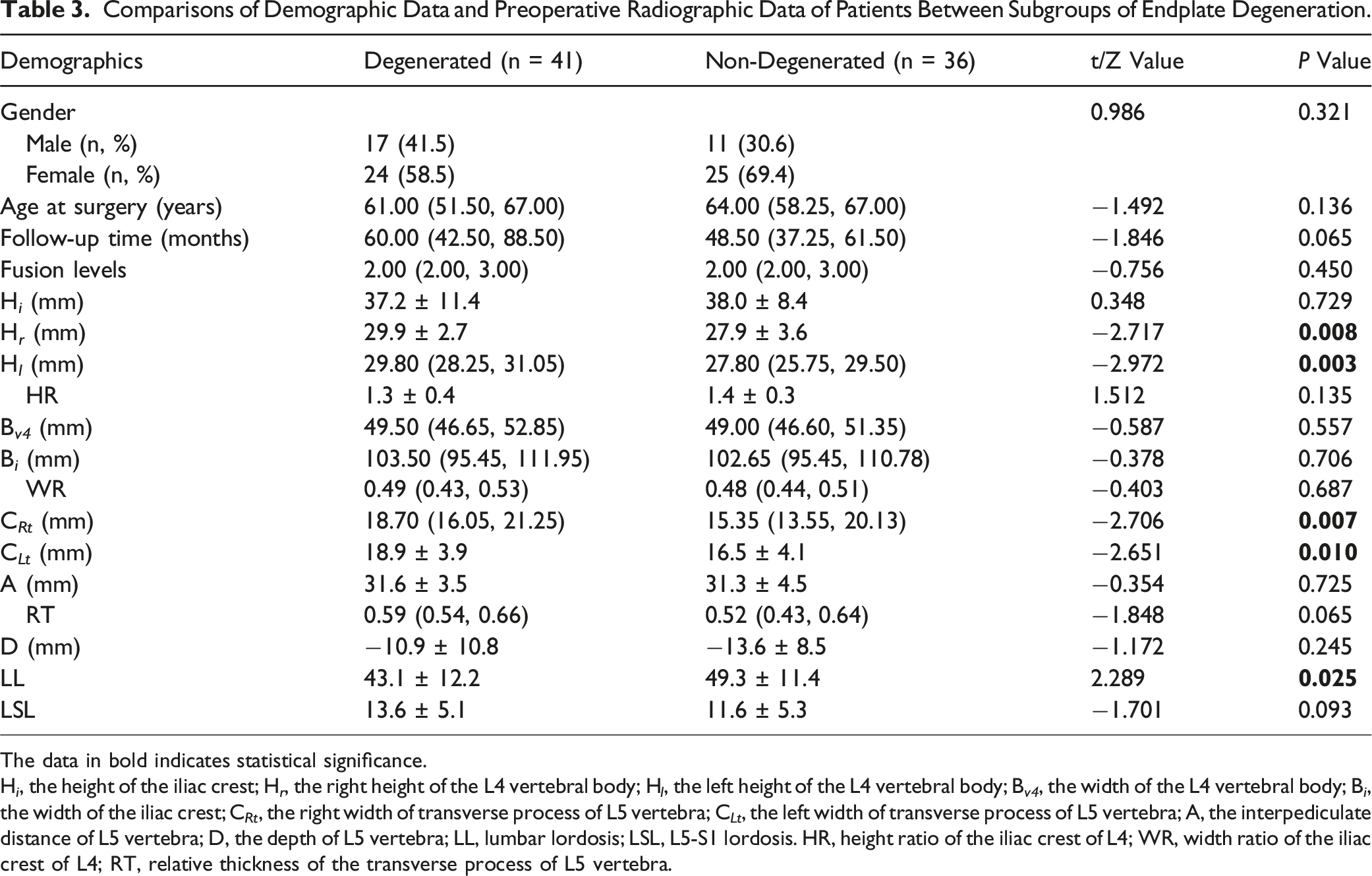
The data in bold indicates statistical significance.
H i , the height of the iliac crest; H r , the right height of the L4 vertebral body; H l , the left height of the L4 vertebral body; B v4 , the width of the L4 vertebral body; B i , the width of the iliac crest; C Rt , the right width of transverse process of L5 vertebra; C Lt , the left width of transverse process of L5 vertebra; A, the interpediculate distance of L5 vertebra; D, the depth of L5 vertebra; LL, lumbar lordosis; LSL, L5-S1 lordosis. HR, height ratio of the iliac crest of L4; WR, width ratio of the iliac crest of L4; RT, relative thickness of the transverse process of L5 vertebra.
Logistic Regression Analyses to Study the Effect of Preoperative Radiographic Data on Disc Degeneration and Endplate Degeneration.
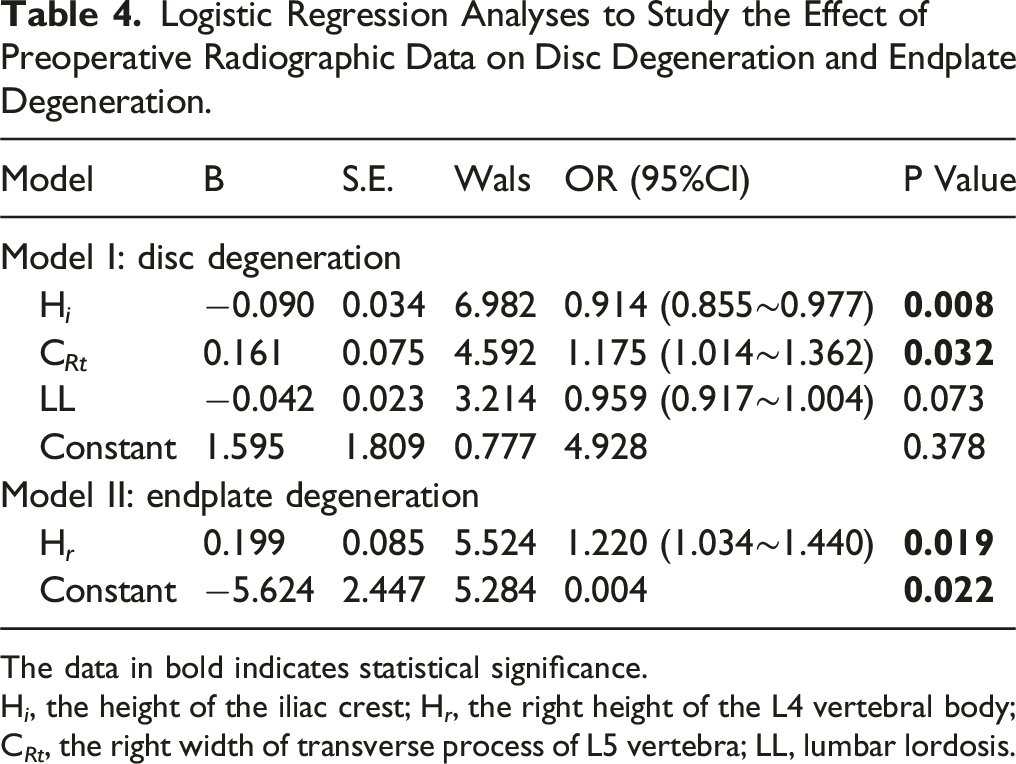
The data in bold indicates statistical significance.
H i , the height of the iliac crest; H r , the right height of the L4 vertebral body; C Rt , the right width of transverse process of L5 vertebra; LL, lumbar lordosis.
Discussion
As initially described by Harms 1 in 1982, TLIF has been the most effective approach to achieving interbody fusion for the surgical treatment of numerous degenerative spinal diseases. 21 TLIF is an excellent and effective procedure that can simultaneously provide decompression and fusion, even correction of spinal deformity. However, there is still controversy over fusion stopping at L5 or the sacrum when performing TLIF for patients with degenerative spinal diseases such as instability or stenosis at the lower lumbar spine, concomitantly radiographic degeneration of L5-S1. The characteristics of the lumbosacral junction significantly influence the L5-S1 degeneration.12,15,16,22 Therefore, it remains unclear whether the characteristics of L5 are potential preoperative risk factors affecting survivorship of the L5-S1 disc after lumbar floating fusion surgery through the TLIF approach. The major findings of this study were as follows: (1) In terms of disc degeneration, both H r and H l were simultaneously higher in the degeneration group, whereas H i was smaller. Consequently, HR in the non-degenerated group was significantly greater than in the degenerated group. (2) For endplate degeneration, C Rt and C Lt were wider in the degeneration group than in the non-degeneration group, while H r and H l were significantly higher. (3) H i and C Rt were independently related to L5-S1 disc degeneration, whereas H r acted as a risk factor for L5-S1 endplate degeneration after floating fusion in degenerative spinal diseases.
The Debate of Floating Fusion and Lumbosacral Fusion
Floating lumbar spinal fusion, defined as fusion stopping at the L5 segment by Brodsky et al, 2 was developed to treat degenerative diseases of the lower lumbar spine. Bydon et al 3 investigated the long-term outcomes of patients undergoing instrumented lumbar arthrodesis, which indicated that the patients who underwent floating fusion were more susceptible to developing ASD requiring reoperation than those with lumbosacral fusion. Disch et al 5 concluded that floating fusions of the segment L4-5 were more likely to develop degenerative radiologic changes in adjacent segments than fusion L4-S1 or L5-S1. Therefore, lumbosacral fusion was recommended in patients with sagittal imbalance and lumbar hyperlordosis, even with minimal L5-S1 disc degeneration. 7 Other researchers have also proposed similar conclusions. Orita et al. identified that higher wedging angle, the smaller foraminal ratio in the L5-S1, multilevel fusion, and male gender were recognized as predictive risk factors for the incidence of L5 spinal nerve disorder. Patients with these risk factors should consider lumbosacral fixation additionally, even though they have few symptoms attributed to the lumbosacral level. 23 Nevertheless, lumbosacral fusion gave rise to the loss of range of motion in spine, which is generally more than 20°. 8 Yamasaki et al 10 recommend the preservation of the L5-S1 segment on condition that there are no serious sign of degeneration or neural encroachment. A very low rate of subsequent degeneration was observed in the L5–S1 segment when the floating fusion was performed, regardless of the initial intervertebral disc degeneration amount. 9 Therefore, it is unnecessary to routinely extend the fusion to sacrum when performing a lumbar fusion for patients with instability or stenosis at L4-L5 segment if no symptoms are due to the degeneration in lumbosacral region. 9 Miyakoshi et al 11 investigated L5-S1 degeneration after isolated L4-L5 posterior lumbar fusion but did not observe any correlation between the narrowing of the L5–S1 disc and clinical outcome. The decision of strategy for the lumbar fusion segment is challenging and confusing for surgeons in patients with radiographic degeneration of L5-S1 without clinical symptoms.
Relationship Between the Position of L5 and Degeneration in L5-S1
In this study, a higher H
i
and deeper of the depth of the L5 vertebra (D) were observed in the disc non-degeneration group, indicating that the position of the L5 vertebra body played an important role in the L5–S1 disc degeneration process (Figure 2). The role of the position of the L5 vertebra body relative to the intercrestal line, previously studied in degenerative spondylolisthesis of the lumbosacral junction, is consistent with our findings.
22
Owing to the difficulty in distinguishing the borders of the L5 vertebral body on the lumbar anteroposterior radiographs, the L4 vertebral body was measured according to the previous study.
19
The innate characteristics of the lumbosacral junction may determine the site of disc degeneration.
12
Asymmetry of superior and inferior endplates in the mid-sagittal plane is a risk factor for lumbar disc degeneration.
24
At the L4-L5 and L5-S1 levels, a decrease in endplate sagittal concave depth and an increase in endplate sagittal concave angle were detected in the group with herniated lumbar discs.
25
Wang et al
19
demonstrated Low HR and (or) WR were the risk factors for L5-S1 disc degeneration. Furthermore, the degeneration of paravertebral muscle was correlated with the spinal-pelvic sagittal parameters in the patients with lumbar disc herniation (LDH).
26
Miyakoshi et al
11
identified no correlation between the narrowing of the L5–S1 disc and clinical outcomes after lumbar floating fusion. Liao et al. demonstrated that extended fusion to the sacrum did not provide a better clinical outcome or reduce the incidence of revision surgery at the L5–S1 segment. However, it has increased the incidence of cephalic ASD.
27
Although some previous studies have demonstrated that the position of the L5 vertebra body relative to the intercrestal line did not correlate to subsequent L5–S1 segment degeneration
13
or curve progression,
14
others have identified that the intercrestal line passing the L5 vertebra is a risk factor for curve progression in degenerative lumbar scoliosis.15,16 Hosoe et al. illustrated that the position of the L5 vertebra in patients with a slip must have been even shallower in the pelvis before the onset of the slip.
22
Comparably, we observed that H
i
, which partially represented the position of the L5 vertebra body, was independently associated with L5-S1 disc degeneration after floating fusion. In this study, we believed that the deeper-seated position of the L5 vertebra body has a protective effect on L5-S1 disc degeneration progress. However, the correlation between the position of the L5 vertebra body and L5-S1 endplate degeneration has not been disclosed. 68-year-old male patient with intractable degenerative spondylolisthesis at L4/L5 underwent a series of radiographs before surgical intervention, including preoperative anteroposterior (A), lateral lumbar spine radiograph (B), and magnetic resonance imaging scans (E). After a complete preoperative assessment, the patient underwent a TLIF with floating fusion. Anteroposterior (C) and lateral (D) lumbar spine radiographs were taken before discharge. After 85 months of follow-up, the patient underwent an imaging evaluation including anteroposterior (G), lateral (H) lumbar spine radiograph, and magnetic resonance imaging scans (F). Although cranial adjacent segment disease occurred, the modified Pfirrmann Grading and endplate defect score of L5-S1 at the last follow-up were similar to the preoperative scores.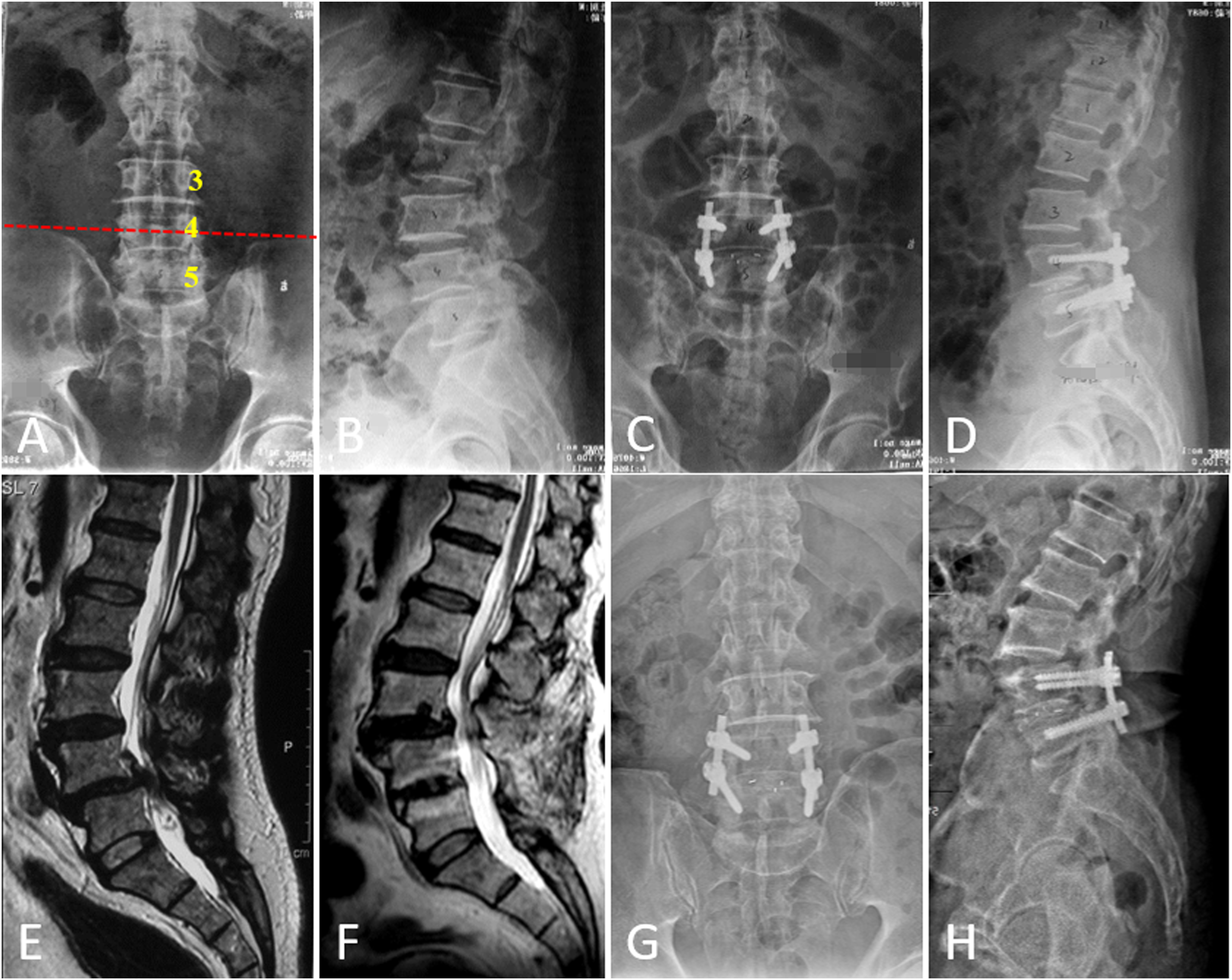
Relationship Between the Transverse Process of L5 and Degeneration in L5-S1
Ohmori et al 20 demonstrated that the relative thickness of the L5 transverse process (RT) was considered to be related to the functional strength of the ligament. Moreover, the flexion of L5-S1 was mainly determined by the posterior and anterior bands of the ligament. 28 Presumably, RT may have some influence on the flexion of L5-S1. Notably, there was an inverse correlation between RT and lumbosacral flexibility. The lumbosacral motion was minimal in radiographs with a high RT, whereas it was high with a small RT. 8 Furthermore, the L5 transverse process was extremely slender in patients with L5 degenerative spondylolisthesis. 22 Moreover, Kim et al 29 demonstrated that a small RT and a low iliac crest height index (IHI) were biomechanical risk factors of recurrent lumbar disc herniation (rLDH) in patients who underwent microdiscectomy for LDH at L5–S1. However, the lumbar lordotic angle-induced inclination of the transverse process of L5 has not been fully considered. Lower lumbar lordosis provided the 2/3 of the total lumbar lordosis.30,31 As an integral part of lower lumbar lordosis in the sagittal plane, the L5 vertebra body often showed a state of anteversion, which caused inclination of the transverse process of L5 on the anteroposterior lumbar spine radiographs. Consequently, the transverse process of L5 was visually perceived as a “slenderer” in the coronal plane owing to its inclination. In the current study, patients with greater LL exhibited a “slenderer” transverse process of L5 and vice versa. Consistent with previous research, we observed that lumbar lordosis was significantly more lordotic in the non-degenerated group than in the degenerated group in both disc and endplate aspects. Moreover, a greater LL indicated a narrower width of the transverse process of L5, eventually leading to less RT. Interestingly, logistic regression analyses revealed that C Rt , which is the width of the transverse process of the L5, was independently associated with the degeneration of L5-S1 disc. The interpretation of these findings indicated that a great LL with a “slenderer” transverse process of L5 plays a crucial part in preventing the degeneration of L5-S1 after floating fusion.
This study has several limitations. First, this study primarily enrolled a small number of patients with lumbar degenerative diseases who underwent surgical intervention in our centers. However, the relatively long follow-up period can be considered an important strength of this study. Second, the lack of standard long-cassette standing upright radiographs, including the spine and pelvis, might lead to inaccurate estimation of the influence of coronal and sagittal alignment of the spine. Therefore, there is a high scope for further studies.
Conclusion
In conclusion, H i and C Rt were independently related to L5-S1 disc degeneration, whereas H r was a significant factor for L5-S1 endplate degeneration after floating fusion in degenerative spinal diseases. A high H i with a “slenderer” transverse process of L5 plays a crucial role in preventing the degeneration of L5-S1 after floating fusion. The significant relationship between anatomical and morphological characteristics of L5 and the degeneration of L5-S1 can be an indicator for determining whether to perform floating fusion when treating patients with instability or stenosis at the lower lumbar spine concomitantly radiographic degeneration of L5-S1 with posterior TLIF.
Footnotes
Acknowledgments
We would like to thank Dr Xu Sun, Dr Liang Xu and Dr Qingshuang Zhou for their invaluable comments on the manuscript.
Author contributions
X.L. and J.Z.: Investigation, analyze the data and writing original draft. J.S.: Collect the data and methodology. J.G.: Supervision. W.S.: Supervision. L.W.: Conceptualization, project administration. X.L. designed the study and coordinate the draft of the manuscript. All authors read and approve the fnal manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Jiangsu Commission of Health (Z2021086), Science and Technology Program of Suzhou (SYSD2020008, SKYD2022012) and Suzhou Municipal Health Commission (KJXW2020058).
Consent for Publication
Written informed consent was obtained from the patient for publication of this study and accompanying images.
Ethical Statement
Data Availability Statement
The data are available at a reasonable request from email