
Abstract
Study Design
Technical Report
Objective
Cerebrospinal fluid (CSF) leak secondary to anterior osteophytes at the cervico-thoracic junction is a rare cause of intracranial hypotension. In this article we describe a technique for anterior repair of spontaneous ventral cerebrospinal fluid leaks in the upper thoracic spine.
Methods
In this technical report and operative video, we describe a 23-year-old male who presented with positional headaches and bilateral subdural hematoma. Dynamic CT myelography demonstrated a high flow ventral cerebrospinal fluid leak associated with a ventral osteophyte at the level of the T1-T2 disc space. Targeted blood patch provided only temporary improvement in symptoms. An anterior approach was chosen to remove the offending spur and micro-surgically repair the dural defect.
Results
The patient had complete resolution of his preoperative symptoms after primary repair.
Conclusions
In select cases, an anterior approach to the upper thoracic spine is effective to repair Type 1 cerebrospinal fluid leaks.
Background and Importance
Anterior approaches to the upper thoracic spine for discectomy in the setting of symptomatic degenerative disc disease have been previously described.1,2 Careful consideration of the sternal and great vessel anatomy in relation to pathological level is critical during patient selection. Cerebrospinal fluid (CSF) leak secondary to anterior osteophyte at the cervico-thoracic junction is a rare cause of intracranial hypotension. We modified the anterior approach to the upper thoracic spine for direct access to repair spontaneous cerebrospinal fluid leaks secondary to anterior osteophyte.
Clinical Presentation
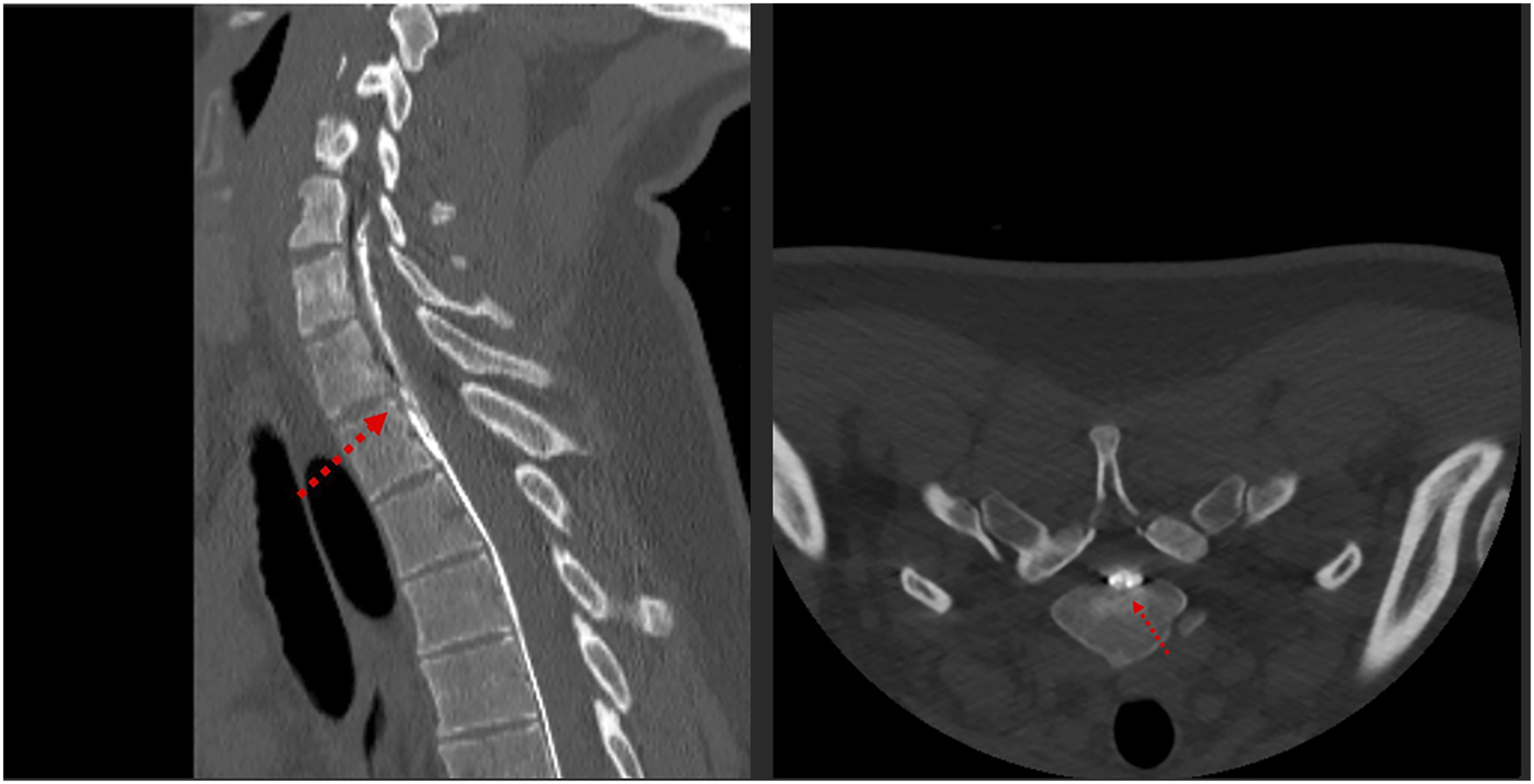
A 23-year-old male with past medical history of childhood tetralogy of Fallot repair developed sudden onset left sided neck and shoulder pain without inciting event. He awoke the next morning with severe headaches, both frontal and occipital, provoked by sitting up from a supine position accompanied by nausea and vomiting. This persisted for two weeks, and he was ultimately seen at an outside facility where CT of the head demonstrated bifrontal subdural hematomas. MRI was subsequently obtained showing stigmata of intracranial hypotension including pachymeningeal enhancement and cerebellar ectopia (Figure 1). The patient was prescribed conservative therapies, including bedrest. Symptoms not only persisted but progressed with development of double vision. The patient was evaluated at our institution where MRI total spine demonstrated the presence of a large, predominantly ventral, extra-dural pseuodmenigocoele extending from the craniocervical junction into the thoracic spine, confirming suspicion of CSF leak. No clear site of leak was identified. The patient underwent high-volume, non-targeted empiric blood patch at the lumbar spine with mild improvement of his symptoms. Nonetheless, symptoms returned, and two weeks later, he underwent dynamic CT myelogram (Figure 2) which was significant for a high flow ventral CSF leak centered around a midline osteophyte at the T1-T2 level. The patient then underwent a targeted CT-guided blood patch at T1-T2, which again provided temporary relief. He returned to the emergency department the following week with incapacitating symptoms and was offered ventral surgical repair. The patient consented to the procedure. (Video 1) The patient had complete resolution of his symptoms following primary repair. He complained of mild hoarseness attributable to recurrent laryngeal nerve irritation. He was discharged on post operative day 3. At 3 months follow up, the patient had resolution of all symptoms and CT imaging revealed complete resolution of his subdural fluid collections. MRI brain showing stigmata of intracranial hypotension including diffuse pachymenengial enhancement, loss of the pontomesencephalic angle, and cerebellar tonsillar ectopia. Sagittal and axial dynamic CT myelogram images showing a Type I CSF leak at the T1-2 disc space.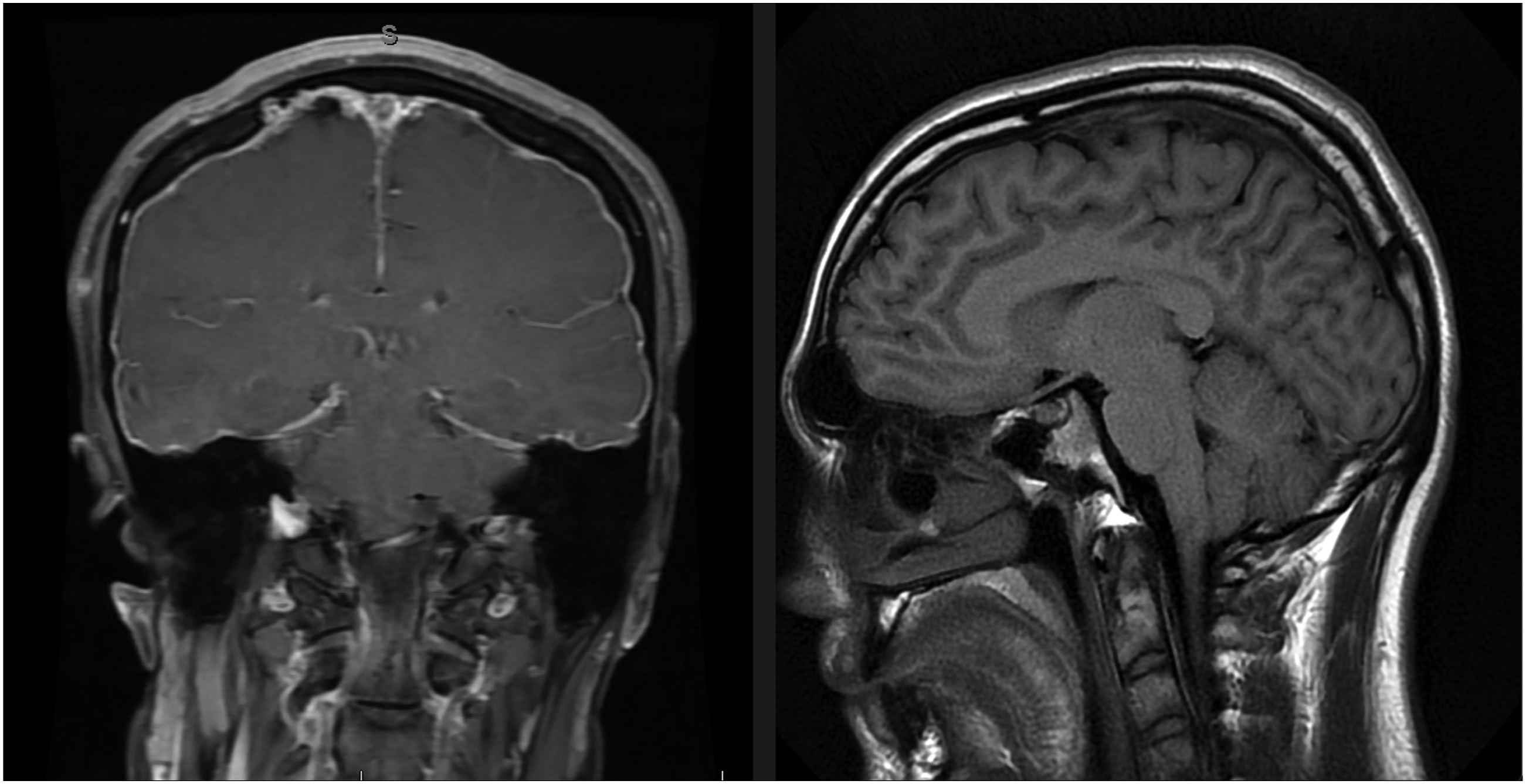
Discussion
Symptomatic spontaneous intracranial hypotension is common, estimated to occur nearly at half the annual incidence of subarachnoid hemorrhage. 1 Causative CSF leak can be classified as previously described in Schievink et al. (type I-III). 2 Symptoms include orthostatic headaches, cranial nerve symptoms, neck pain, nausea, hearing changes, disequilibrium, and in some cases coma/death. Radiographic diagnosis is critical and measures of midbrain sagging can help differentiate between spontaneous intracranial hypotension and related conditions with cerebellar ectopia. 3 Epidural blood patches are typically selected as the first treatment modality once the diagnosis is made, and carry a wide range of reported efficacy (36-90%). 4 Transvenous embolization may be possible if a CSF-venous fistula is identified. 5
This brief report will focus on the operative considerations pertaining to the surgical repair of Type I (Dural tear) thoracic leaks after the failure of conservative management. Posterior approaches for these lesions have been previously described. 6 There are descriptions of anterior approaches to the upper thoracic spine for degenerative disease.7,8 One recent study by Singh et al describes open sternotomy with cardiothoracic assistance and retraction of the great vessels to aid in resection a symptomatic disc at T2-T3. 8 There is a single case report of a sternotomy for the primary repair of a ventral osteophyte associated CSF leak. 9 We were able to avoid this added complexity, with careful attention paid to the preoperative CT scan demonstrating a manubrium just below the T1-2 level, allowing for the appropriate angulation of the fixed retractors in relation to the disc space. Gentle dissection of the great vessels and careful fixed retraction was sufficient to expose the entirety of the disc space. After discectomy and exposure of the posterior longitudinal ligament, the midline osteophyte and the associated dural defect were identified. This was dissected, isolated, and removed. We placed an inlay dural substitute (DuraMatrix). Primary repair was achieved with the use of an automated stitch deployment system (DuraStat®, Austin, Texas, USA), which allowed for primary repair of the dural defect without wrist supination in the confines of the spinal canal at the depth of the disc space. We placed two stitches (cranial and caudal) followed by a muscle patch held in place by a knot of the previously placed stitches. To reinforce our closure, a fibrin sealant was utilized.
Two similar patients from our institutional experience of anterior approaches for ventral osteophyte associated Type I CSF Leaks are shown in (Figure 3). Patients were 39 and 55 years old, and both had near-complete resolution of their preoperative symptoms prior to discharge from the hospital. One leak was not amenable to direct primary repair and was repaired with only dural inlay and fibrin sealant while the other was primarily repaired with a proline stitch and fibrin sealant. A lumbar drain was placed at surgery in one patient and removed on postoperative day two after a clamp trial. Lumbar drains are typically not placed post-operatively in patients with subdural hemorrhage on CT scan, so as to avoid expansion. In all three cases, patient anatomy allowed an anterior approach to access the offending bony pathology and surgically repair this potentially life-threatening condition. CT with axial cuts demonstrating the offending ventral osteophyte responsible for the dural defect and symptomatic CSF leak in our two additional patients undergoing anterior approach repair.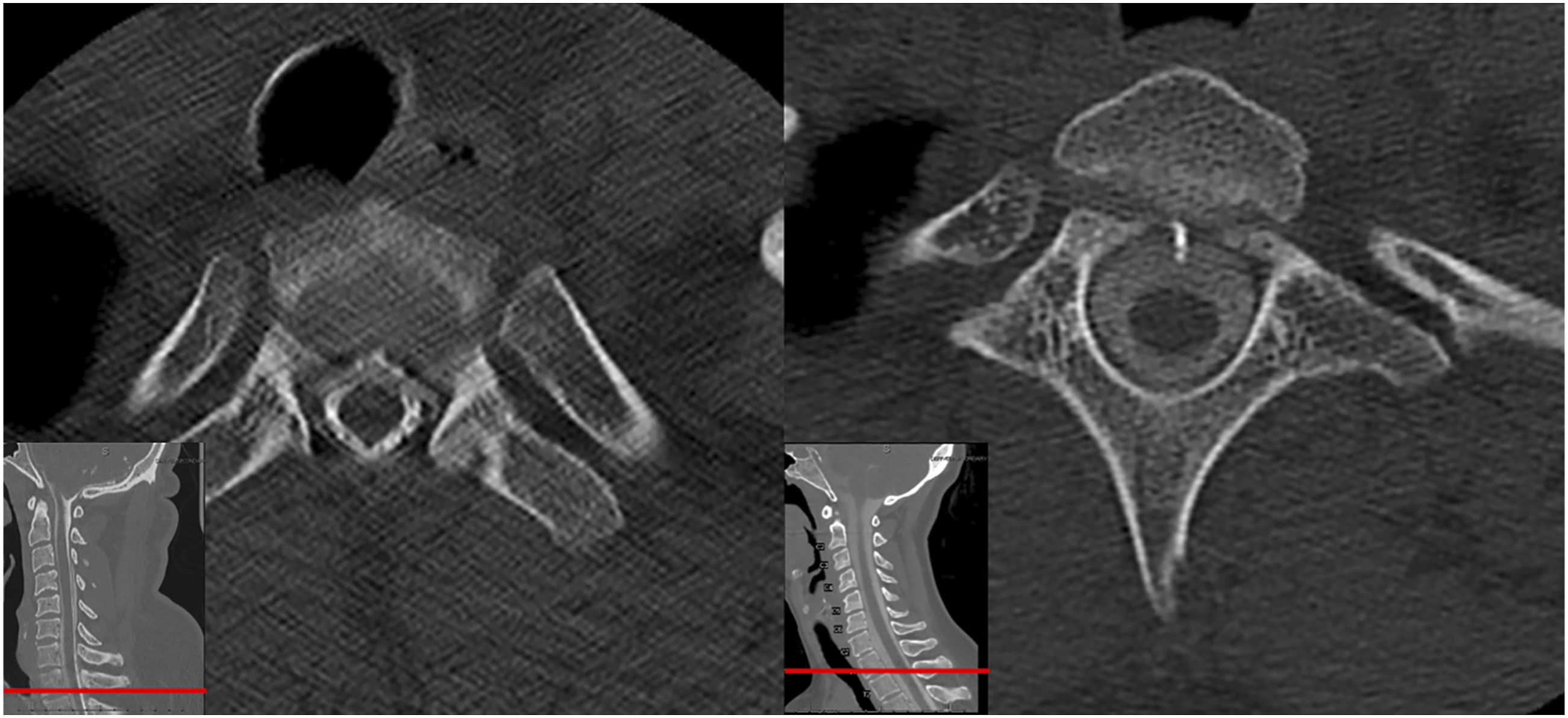
Conclusion
We describe an anterior upper thoracic approach to repair a Type 1 cerebrospinal fluid leak secondary to anterior osteophyte at the cervicothoracic junction and report three cases. If conservative management and targeted blood patch treatment fail, an anterior thoracic approach may be considered for primary repair after careful radiographic evaluation.
Supplemental Material
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consents was obtained prior to the performance of the above described procedures
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.