
Abstract
Study Design
Retrospective cohort study
Objectives
This study aimed to investigate whether early surgery shortens the duration of opioid use in patients who underwent surgery with lumbar disc herniation.
Methods
We extracted patients who underwent surgery at least 2 weeks after they were diagnosed with lumbar disc herniation between April 2014 and May 2021. Opioid use after surgery was compared between patients who underwent surgery within 90 days (early surgery group) and 90 days or later (late surgery group). Propensity-score-matching analysis and multivariable Cox hazard regression analysis with a restricted cubic spline model were conducted to evaluate the association between the timing of surgery and termination of opioid use after surgery.
Results
A total of 1597 eligible patients were identified, with 807 (51%) in the early surgery group. In the propensity-score-matched cohort, the early surgery group had a significantly lower proportion of opioid use than the control group (28% vs 48%, percent difference −20%, P < .001). Multivariable Cox hazard regression analysis showed that early surgery was significantly associated with the earlier termination of opioid use (HR, 3.13; 95% CI, 1.97-4.97; P < .001). Restricted cubic spline model showed a monotonically decreased hazard ratio and decreased hazard ratio of .50 in patients who underwent surgery 111 days or later after the diagnosis.
Conclusions
Early surgery, especially within 90 days, was associated with earlier opioid use termination after surgery. Regarding the duration of opioid use following surgery, surgical treatment may be preferable to perform within around 4 months after the diagnosis.
Keywords
Introduction
Lumbar disc herniation (LDH) is a well-known cause of low back pain and leg pain with high prevalence among individuals aged 30 to 50 years old. Patients with LDH are initially treated conservatively. Surgery is generally performed for those who do not respond to the conservative treatment,1-4 with a wide variation in its timing. The reported time from the onset of symptoms to surgery is inconsistent, ranging from several weeks to several months.5,6 Despite the common use of surgical treatment for LDH, its optimal timing is not well understood.
Although surgery for LDH is generally associated with favorable outcomes, some patients continue to suffer from residual symptoms after surgery. For such patients, analgesics like opioids are often used to alleviate persistent pain. Recent reports showed that a significant number of patients remained on opioids for a long period after surgery for LDH,7,8 in spite of a growing concern over their adverse effects. It remains unknown whether if the risk of prolonged opioid use after surgery is associated with the timing of surgical treatment.
In this study using a large administrative claims database covering young, middle-aged, and elderly people in Japan, we examined the relationship between the timing of surgery and postoperative opioid use in patients with LDH. This study aimed to clarify the optimal timing of surgery for LDH using the postoperative termination of opioid use as a clinical indicator.
Materials & Methods
DeSC Database
The DeSC database, which consists of the administrative claims data of 3 million insurance subscribers provided by DeSC Healthcare Inc. Tokyo, Japan, was used. This database is constructed based on anonymized medical data gathered by three of the Japanese public health insurers 9 : (1) association/union-administered health insurance for salaried employees in large companies; (2) National Health Insurance for self-employed individuals, retried individuals, and their dependents; (3) and Advanced Elderly Medical Service System for all people aged 75 years or older. Thus, this newly developed database covers young, middle-aged, and elderly people in Japan.
A previous study showed that the population included in the DeSC database represented the whole population of Japan. 10 The database contains encrypted unique identifiers, birth date, sex, height and weight, diagnoses coded according to the 10th revision of the International Classification of Diseases and Japanese tests, information on medications, surgical and nonsurgical procedures, admission and discharge date, and costs of examinations, procedures, surgery, and anesthesia. The pre-existing comorbidities were: diabetes mellitus (E10–E14), hypertension (I10–I15), chronic lung disease (J40–J47), history of cerebrovascular disease (I60–I69), cardiac disease (I20–I25, I30–I52), and hepatic cirrhosis (K74).
The study protocol was approved by the institutional review board of the Graduate School of Medicine, (2021010NI). The study was conducted in accordance with the principles of the Helsinki Declaration. The requirement for informed consent was waived because of the anonymous nature of the data.
Study Design, Covariates, and Outcome
This retrospective observational study used the DeSC database to extract all patients who were diagnosed with LDH from April 2014 to May 2021 and treated with any of the following analgesics (Figure 1): acetaminophen, non-steroidal anti-inflammatory drugs, pregabalin, mirogabalin, and opioids (oxycodone, hydrocodone, morphine, tramadol, hydromorphone, codeine, buprenorphine, and fentanyl). The following patients were excluded: (a) aged 18 years or younger; (b) terminated outpatient visits for at least one months after the diagnosis; (c) treated without opioid prescriptions before surgery; and (d) underwent surgery within 2 weeks because they may have had worse conditions with cauda equina syndrome, altered bladder function, and progressive muscle weakness or neurological deficits. Flowchart of patient selection.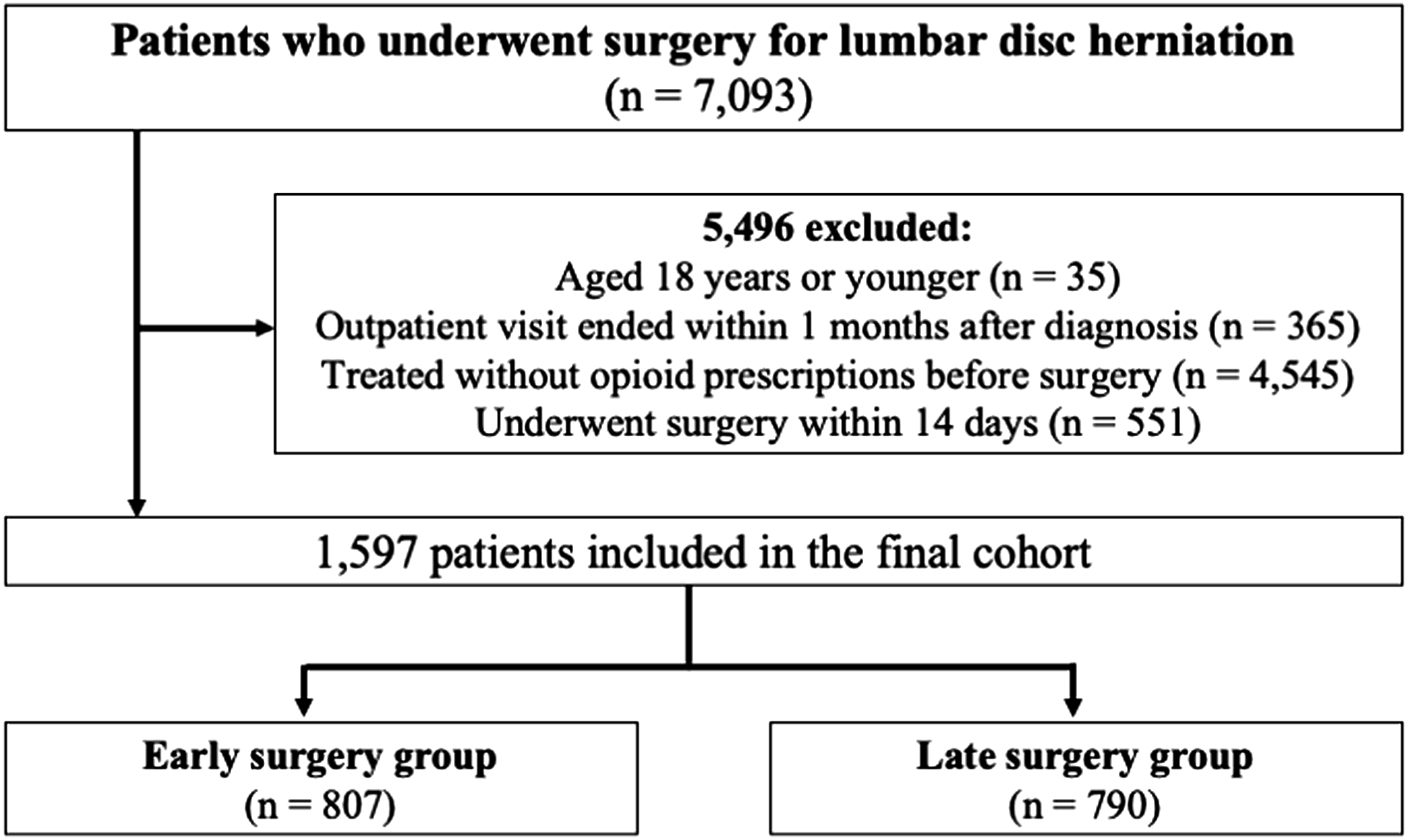
The primary outcome was the termination of opioid use, which is defined as patients terminating opioid use 3 months after surgery, according to previous studies.11,12 This definition is considered as chronic use of pain medications for those requiring prescriptions over a period of 90 days or longer.
Statistical Analysis
The distribution of the baseline characteristics between the early surgery and control groups was described. Early surgery was defined as surgery within 90 days after the diagnosis of LDH, based on the median days from the diagnosis to the surgery. Subsequently, propensity score matching analysis was performed to balance the measured potential confounders between the groups. 13 The propensity scores for receiving early surgery were estimated using a multivariable logistic regression model. All measured baseline covariates were included as predictive variables. The one-to-one nearest neighbor method was used with a caliper width of .2 of the standard deviation of the estimated propensity scores. Each patient in the early surgery group was matched to one patient in the control group without replacement. The absolute standardized differences were calculated for each covariate before and after matching, and the balanced distribution of covariates between the groups was confirmed.
After propensity score matching, the proportion of analgesic prescriptions at 3-month, 6-month, and one year after surgery between the early and late surgery groups were compared. Subsequently, a multivariable cox proportional hazard model was constructed to compare the time of opioid use termination after surgery between the groups. A non-linear relationship between the timing of surgery and opioid use termination was modeled using a restricted cubic spline with standard points of 4 knots placed at the fifth, 25th, 75th, and 95th percentiles. 14 Each model was adjusted for age, sex, and pre-existing comorbidities. Since clinicians are interested in the time when the effectiveness of surgery is not different between the groups regarding opioid use termination after surgery, we set the reference at 42 days (6 weeks) after diagnosis in the restricted cubic spline model because many guidelines suggest an observational period of 6 weeks. The restricted cubic spline model resulted in point estimates using hazard ratios (HRs) and 95% confidence intervals (CIs).
Continuous variables are presented as mean (standard deviation) or median (interquartile range) as appropriate, and categorical variables are described as numbers (%). The outcomes after propensity score matching were compared between the early surgery and control groups using the χ 2 test. A two-sided P-value <.05 was considered statistically significant for all tests. All analyses were performed using Stata/MP version 16 (StataCorp, College Station, TX).
Results
Baseline characteristics of patients who underwent lumbar discectomy by early and late surgery before and after propensity score matching.
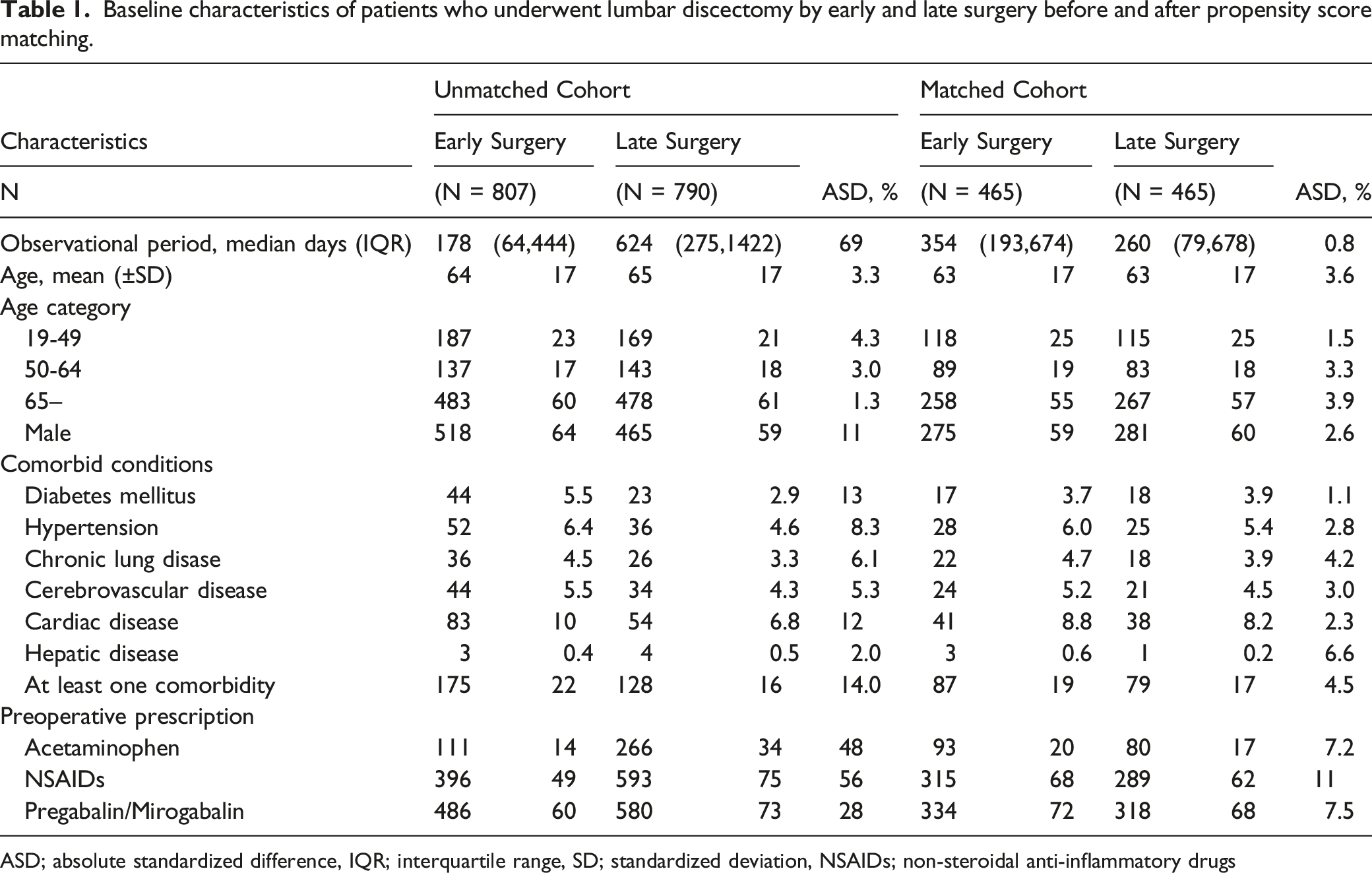
ASD; absolute standardized difference, IQR; interquartile range, SD; standardized deviation, NSAIDs; non-steroidal anti-inflammatory drugs
Comparison of analgesic prescription after surgery between early and late surgery after propensity score matching.
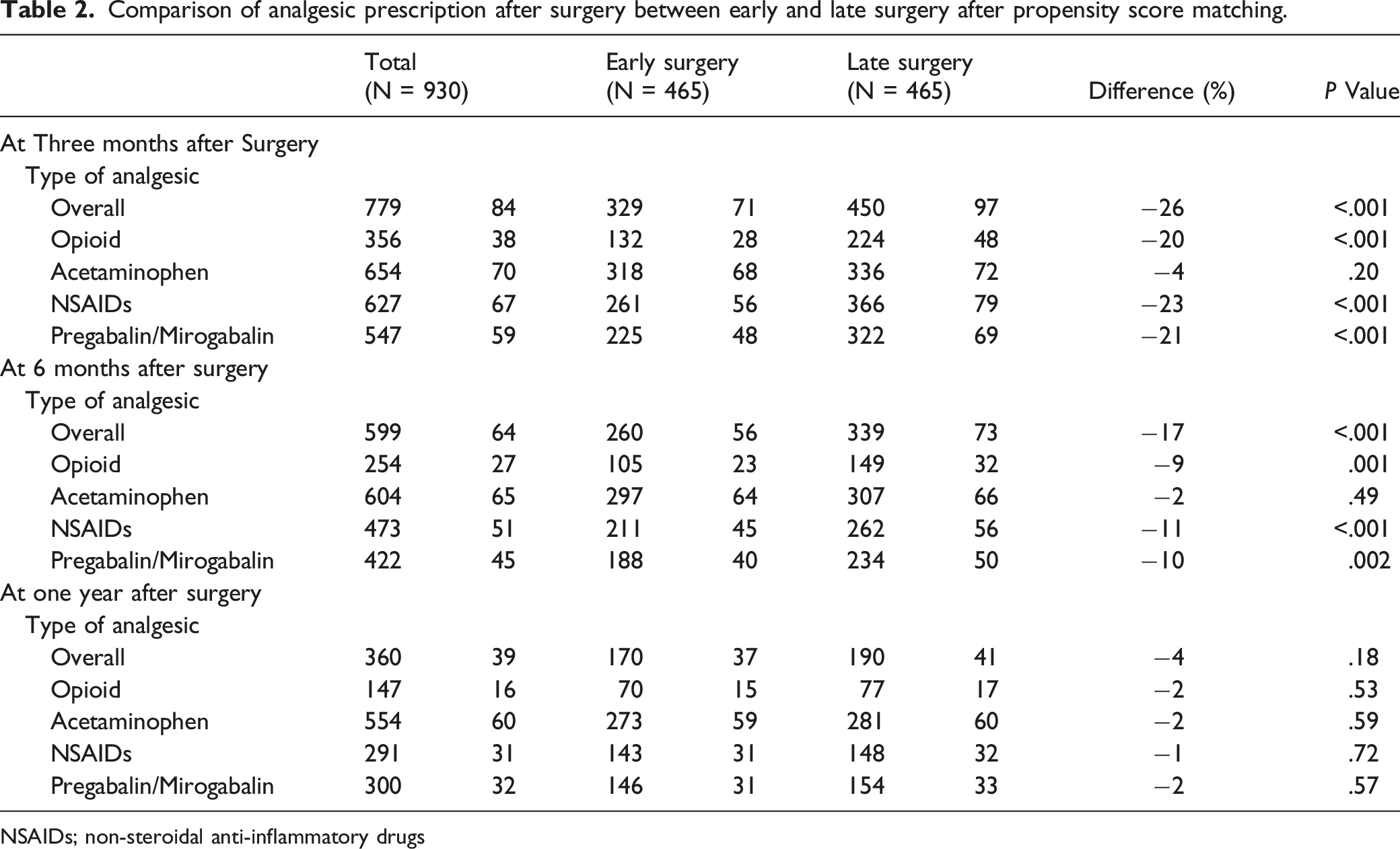
NSAIDs; non-steroidal anti-inflammatory drugs
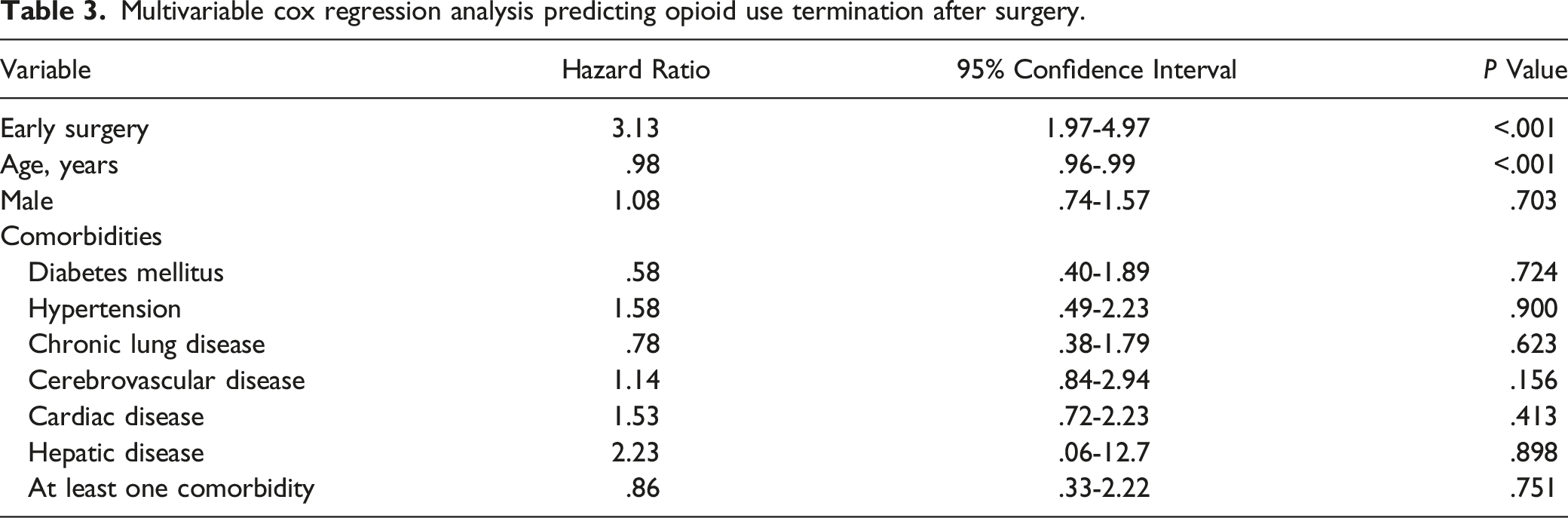
Multivariable cox regression analysis predicting opioid use termination after surgery.
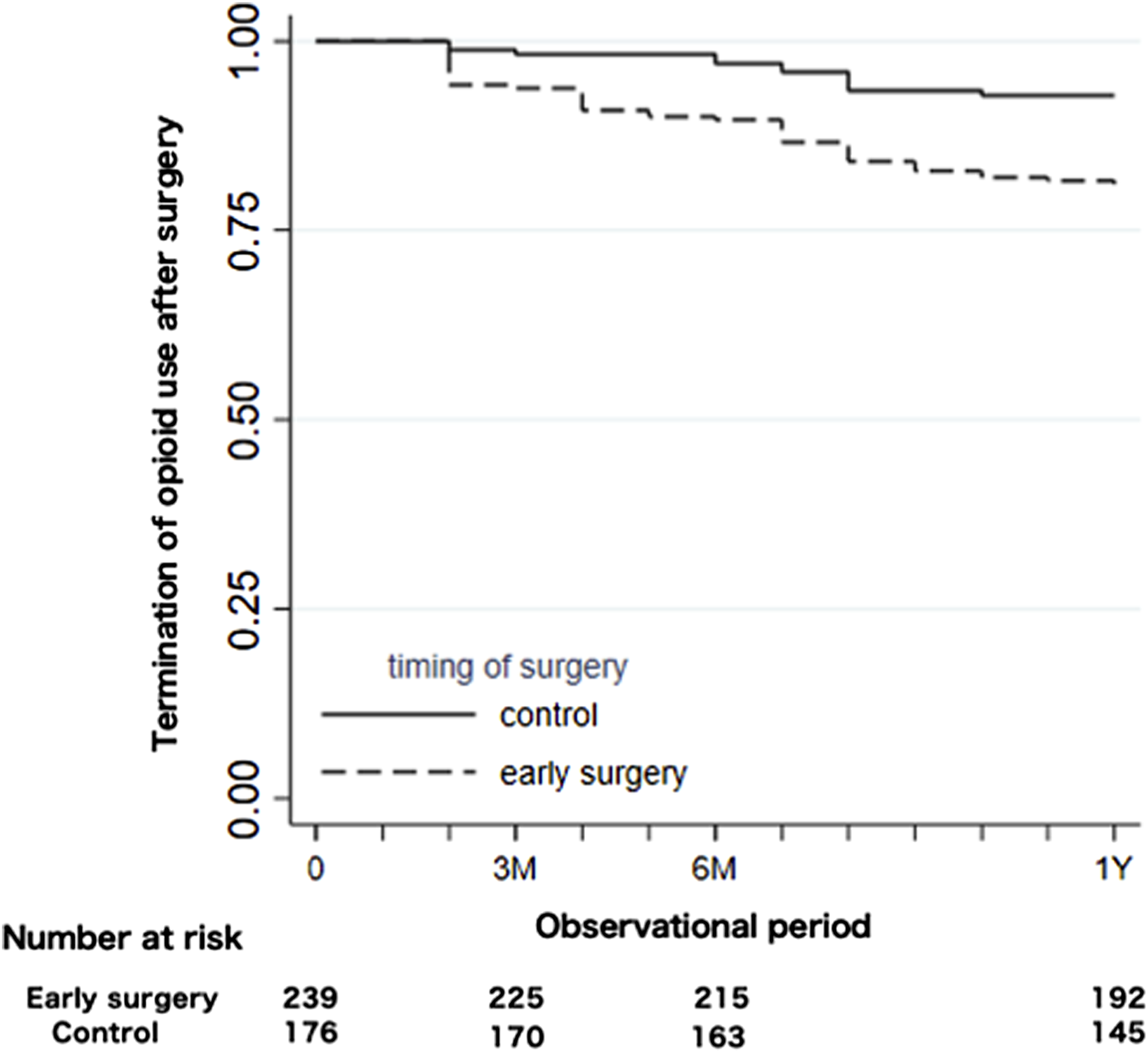
Kaplan–Meier curves of opioid use termination following surgery between the early and late surgery groups during the observational period.
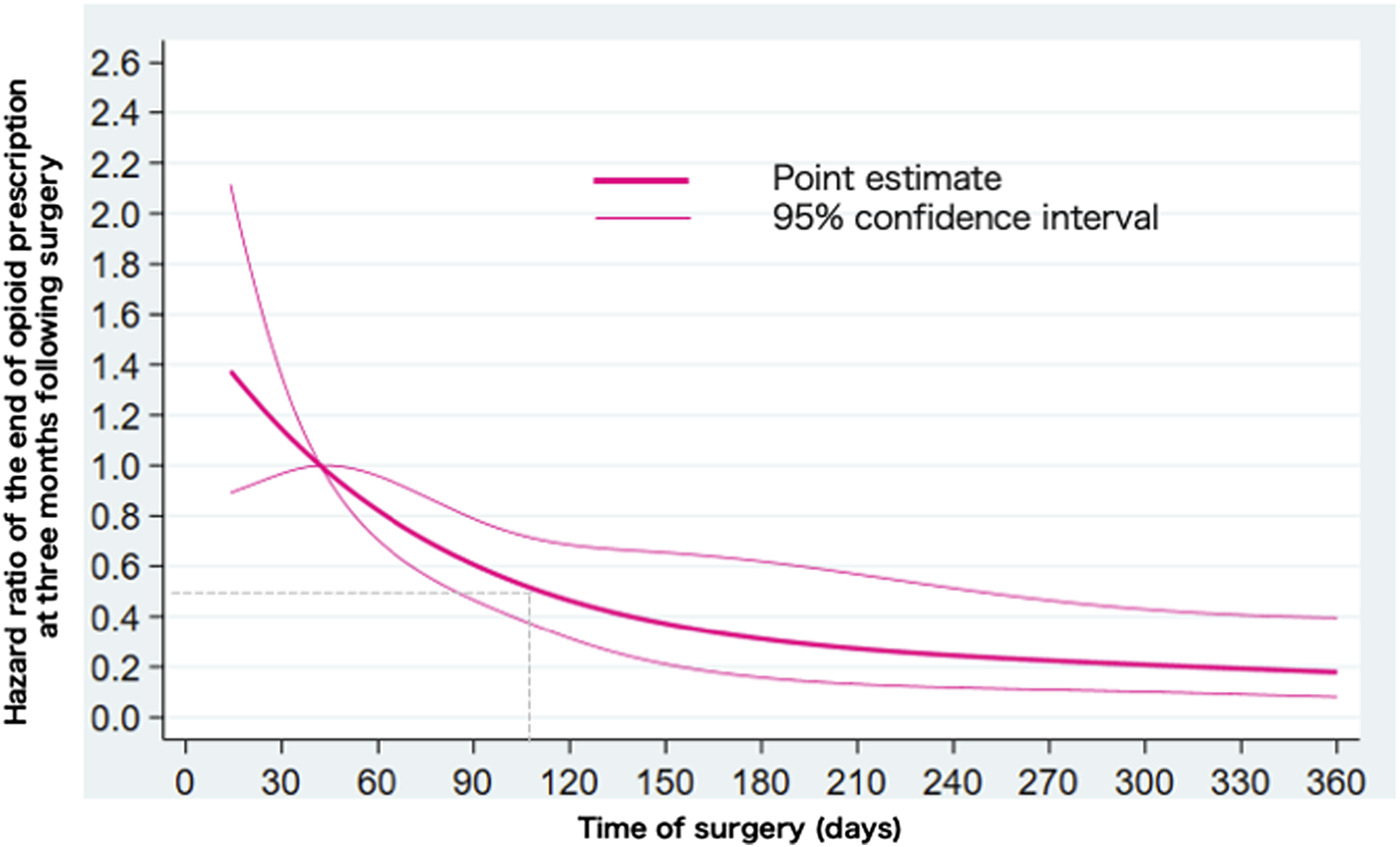
Restricted cubic spline curb showing the association between the time of surgery and opioid use termination following surgery.
Discussion
This study examined whether early surgery shortened the duration of opioid use in patients who underwent lumbar discectomy and found that early surgery, especially within 90 days after the diagnosis of LDH, had higher HR of postoperative opioid use termination than late surgery. The HR decreased monotonically as the time of surgery increased and fell below .50 when the time of surgery was 4 months or later.
Opioids are widely used for neural pain including postoperative pain control. However, they may have several side effects, including increased risk of ileus and infection, prolonged hospital stay, and higher readmission rate.12,15-17 Opioid use is affected by several factors that can substantially differ across countries. 18 In the United States, although the number of chronic opioid use following primary lumbar discectomy has declined, one in 5 patients still use opioids after even surgical treatment. 7 Furthermore, a recent study showed that 33% of patients had opioid prescription before surgery, and 7.6% of patients who underwent lumbar discectomy still used opioids at one year after surgery. 11 In more strictly regulated settings, only 3.3% of Taiwanese patients sustained postoperative opioid use at 90 to 180 days after surgery. 19 In this study, 36% of patients who underwent surgery were treated with opioid preoperatively, which was comparable to those in previous studies. However, 16% of patients, who underwent lumbar discectomy, still used opioids at one year after surgery. Moreover, opioids are not strictly regulated in Japan compared to Western countries. Although the preoperative opioid use in Japan was comparable to those in other countries, clinicians must be vigilant in monitoring patients to avoid chronic opioid use.
Prolonged opioid use is associated with future opioid dependence, which has an enormous societal impact.20,21 Regarding the opioid prescription period, a previous study showed that the proportion of patients who used one or more opioids decreased to under 10% at 9 to 12 months after lumbar discectomy and concluded that a minority of patients who underwent lumbar discectomy continued to use opioids up to 15 months after surgery. 11 However, 90% of acute attacks of sciatica in patients with LDH settle with conservative treatment during the first 6 week. Nevertheless, some patients still use opioids for over one year after surgery. This study showed that early surgery, especially within 90 days, was significantly associated with opioid use termination at 3 months after surgery. Guidelines recommend surgery if patients have prolonged pain despite conservative treatments. 22 According to the restricted cubic spline analysis, the likelihood of opioid use termination may decline to an HR of .5 when patients undergo surgery 4 months after the diagnosis of LDH. This may be one of the possible cut points for the preference for surgery to reduce chronic opioid prescription.
Nevertheless, this study has several limitations. First, we could not obtain information on image findings, and type and severity of LDH. Second, we could not identify indications for surgery. For patients who presented with severe cauda equina symptoms, neurological deficit, and muscle weakness, emergency surgery may be performed even for patients with LDH. Therefore, we excluded patients who underwent surgery within 2 weeks after the diagnosis. Third, unmeasured confounding may not be completely removed even with propensity score analyses. However, we believe that measured confounding was minimized on this cohort through use of propensity matching analysis. Fourth, we could not determine the reasons for prolonged post-operative opioid use, whether it was patient’s dependence on opioids or their doctor’s prescription of opioids. Despite these limitations, the findings from this study may provide additional useful information for surgeons regarding opioid prescription after surgery and prevention of chronic opioid use. Further studies are warranted to clarify whether early surgery is preferable regarding cost effectiveness and long-term prognosis.
In conclusion, early surgery, especially within 90 days, may shorten the duration of postoperative opioid use in patients with LDH. Moreover, postoperative opioid use may decrease when patients undergo surgery in 4 months or later after the diagnosis of LDH.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Ministry of Health, Labour and Welfare, Japan (21AA2007 and 20AA2005) and the Ministry of Education, Culture, Sports, Science and Technology, Japan (20H03907).
Level of Evidence
Prognostic Level Ⅲ