
Abstract
Study Design
Retrospective
Objective
To compare the rate of positive pathology on thoracic MRI ordered by surgical spine specialists to those ordered by nonsurgical spine specialists.
Methods
Outpatient thoracic MRIs from January–March 2019 were evaluated from a single academic health care system. Studies without a known ordering provider, imaging report, or patients with known presence of malignancy, multiple sclerosis, recent trauma, or surgery were excluded (n = 320). Imaging studies were categorized by type of provider placing the order (resident, attending, or advanced practice practitioner) and department. MRIs were deemed positive if they showed relevant pathology that correlated with indication for exam as determined by a radiologist. One-sided chi-squared analysis was performed to determine statistical significance.
Results
Overall, our data demonstrated 17.2% of studies with positive pathology. Compared to nonspecialty clinicians, subspecialists showed 35/184 (19.0%) positivity rate versus the non-specialist with 20/136 (14.7%) positivity rate (P = .156). Posthoc analysis demonstrated that surgical specialists who order thoracic MRIs yield significantly higher positivity rates at 19/79 (24.0%) compared to nonsurgical specialists at 36/241 (14.9%) (P < .05). Overall, neurosurgery demonstrated the highest rate of positive thoracic MRIs at 14/40 (35.0%). Comparison between the rate of positivity between physicians and advanced practitioners was insignificant (P > .05).
Conclusions
Clinical diagnosis of symptomatic thoracic spine degenerative disease requires an expert physical exam combined with careful attention to radiology findings. Although the percent of relevant pathology on thoracic MRI is low, our data suggests evaluation by a surgical specialist should precede ordering a thoracic spine MRI.
Introduction
The incidence of thoracic spine disease is uncommon relative to cervical and lumbar disease, estimated to be around 16% of the general adult population with a lifetime prevalence as high as 13%. 1 The lower incidence of pathology compared the cervical and lumbar spine may be explained by additional mechanical support attributable to the rib articulation leading to less axial force and increased stability. Consequently, the rate of thoracic disc herniation has been estimated at .1 to 3% of all herniations and comprise less than 2% of disc procedures.2,3 However, the symptoms of thoracic spine disease can be as equally debilitating as this region can also be affected by a multitude of degenerative and traumatic processes resulting is spinal cord or nerve root compression, progressive pain, and deformity. These pathologies can translate to severe morbidity for the patient and health care costs onto the system.4,5, 6
However, accurate diagnoses of thoracic spine pathologies rely on a careful correlation to clinical exam and history as the more common findings on imaging studies are often nonspecific and nondiagnostic. The thoracic spine exam is difficult, as there is no myotomal exam and sensory distribution may be difficult to discern. Further, retrospective analysis of thoracic MRI imaging has shown that asymptomatic patients may exhibit positive findings on thoracic MRI to be as high as 70%. 7 Diagnosis can further be confounded by the simultaneous presence of lumbar or cervical disease that may more commonly manifest as referred pain to the thoracic region.
This study aims to compare the rate of relevant, positive pathologic findings on thoracic MRI ordered by surgical spine specialists to those ordered by nonsurgical spine specialists within a single academic health system. We further compared the results of thoracic MRIs across different specialties and levels of training. We hypothesized that health providers who specialize in surgical spinal pathology with surgical intervention (ie orthopaedic surgery and neurosurgery), would be more judicious in obtaining thoracic spine MRIs for patients in the outpatient setting.
Methods
A retrospective review was performed of thoracic spine MRI radiology reports dating from January 2019 to June 2019 at a single academic health system. This study was approved by the Institutional Review Board (#832364) and granted a waiver of informed consent. The reports were obtained using the Montage™ radiology report search tool to obtain MRI of the thoracic spine without contrast, including orthopaedic and neurologic spine protocols. Inclusion and exclusion criteria were evaluated using history from the radiology report and the electronic health record. Inclusion criteria were defined as adult patients in the outpatient setting presenting with back pain, radiculopathy, or myelopathy. Studies were excluded if there was no known ordering provider or imaging report from the database search. Studies in which the patient had a known presence of malignancy, multiple sclerosis, recent trauma, history of neurologic lesion, or prior spine surgery were excluded. Imaging studies were categorized by type of provider placing the order (resident, attending, or advanced practice practitioner) and department. A positive MRI examination was defined by the radiology report containing any of the following findings which correlated with the indication for the study: moderate or severe neuroforaminal or spinal canal stenosis, cord compression, acute vertebral fracture, syringomyelia, or multifocal signal cord abnormalities. One-sided chi-squared analysis was performed to determine statistical significance. RStudio software (Vienna) was used to perform all statistical analysis.
Results
Indication and Classification of Positive Thoracic MRI Findings.
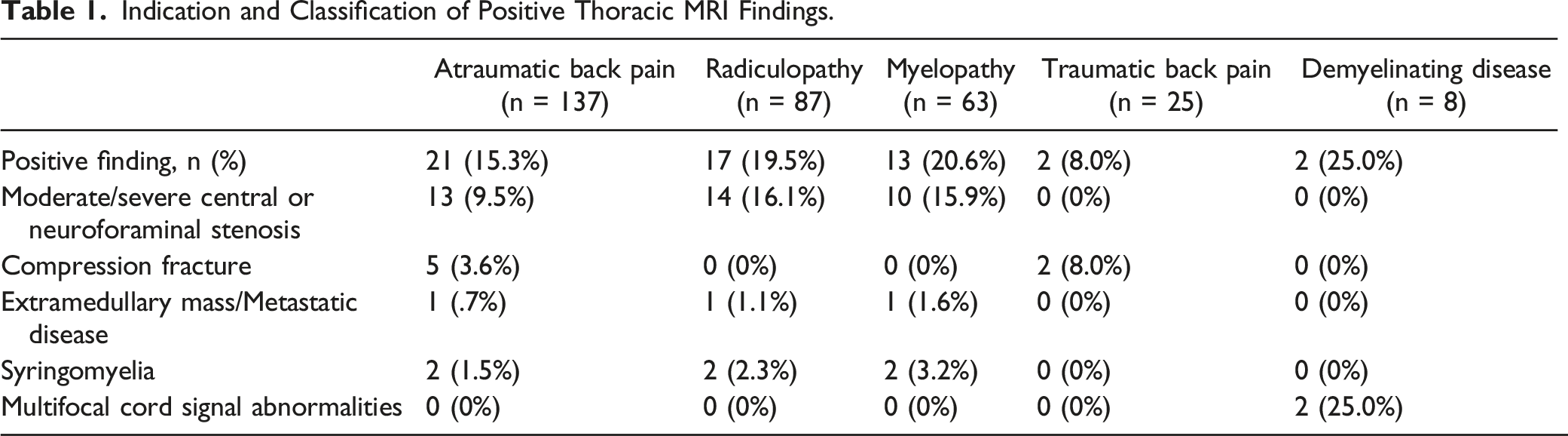
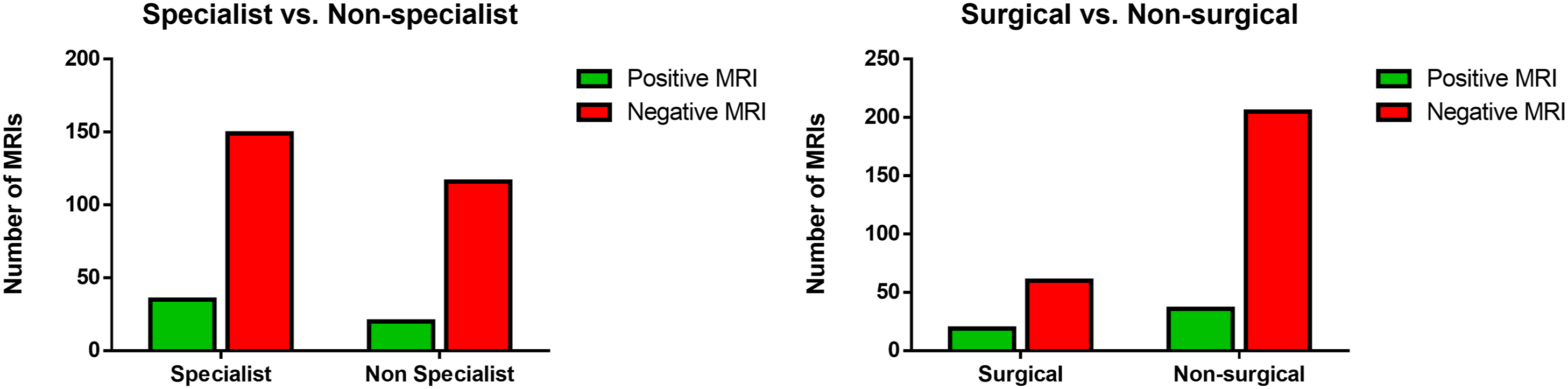
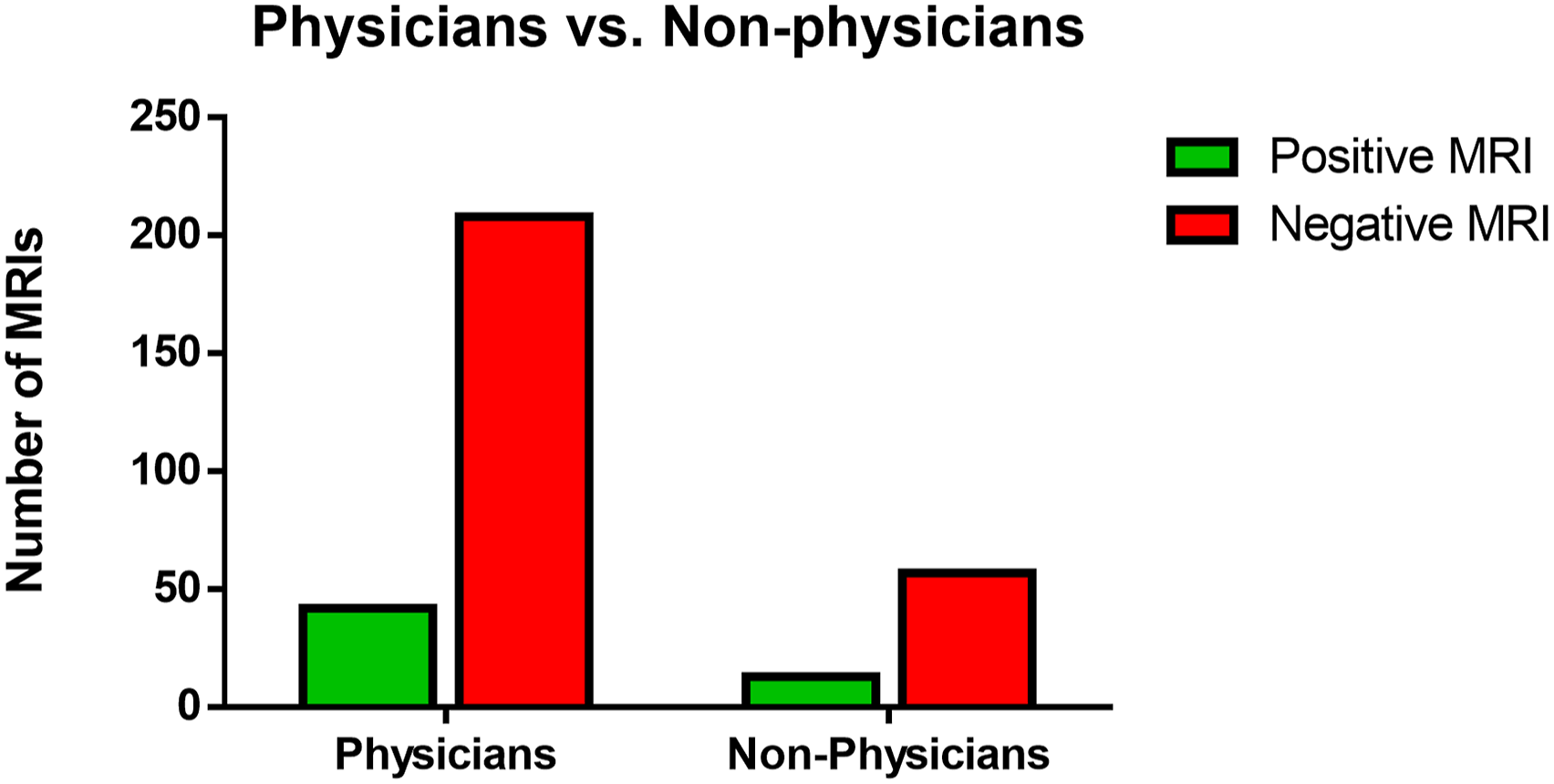
There were overall 16 different ordering departments (Figure 1). Neurosurgery, Orthopaedic Surgery, Neurology, and Physical Medicine and Rehabilitation were categorized as subspecialists given their subspecialty training in spine pathology. Compared to nonspecialty clinicians, subspecialists showed 35/184 (19.0%) positivity rate versus the non-specialist with 20/136 (14.7%) positivity rate (P = .156). Posthoc analysis showing that surgical specialists who order thoracic MRIs yield significantly higher positivity rates at 19/79 (24.0%) compared to nonsurgical specialists at 36/205 (14.9%) (P < .05) (Figure 2). Overall, neurosurgery providers demonstrated the highest rate of positive thoracic MRIs at 14/40 (35.0%). Finally, comparison between the rate of positivity between physicians and advanced practitioners was also insignificant (P > .05) (Figure 3). Rate of positive and negative thoracic MRI findings by specialty. (a) Rate of positive and negative thoracic MRI ordered by specialists compared to nonspecialists. (b) Rate of positive and negative findings ordered by surgical specialists to nonsurgical specialists. Rate of positive and negative thoracic MRI ordered by physicians versus non-physicians.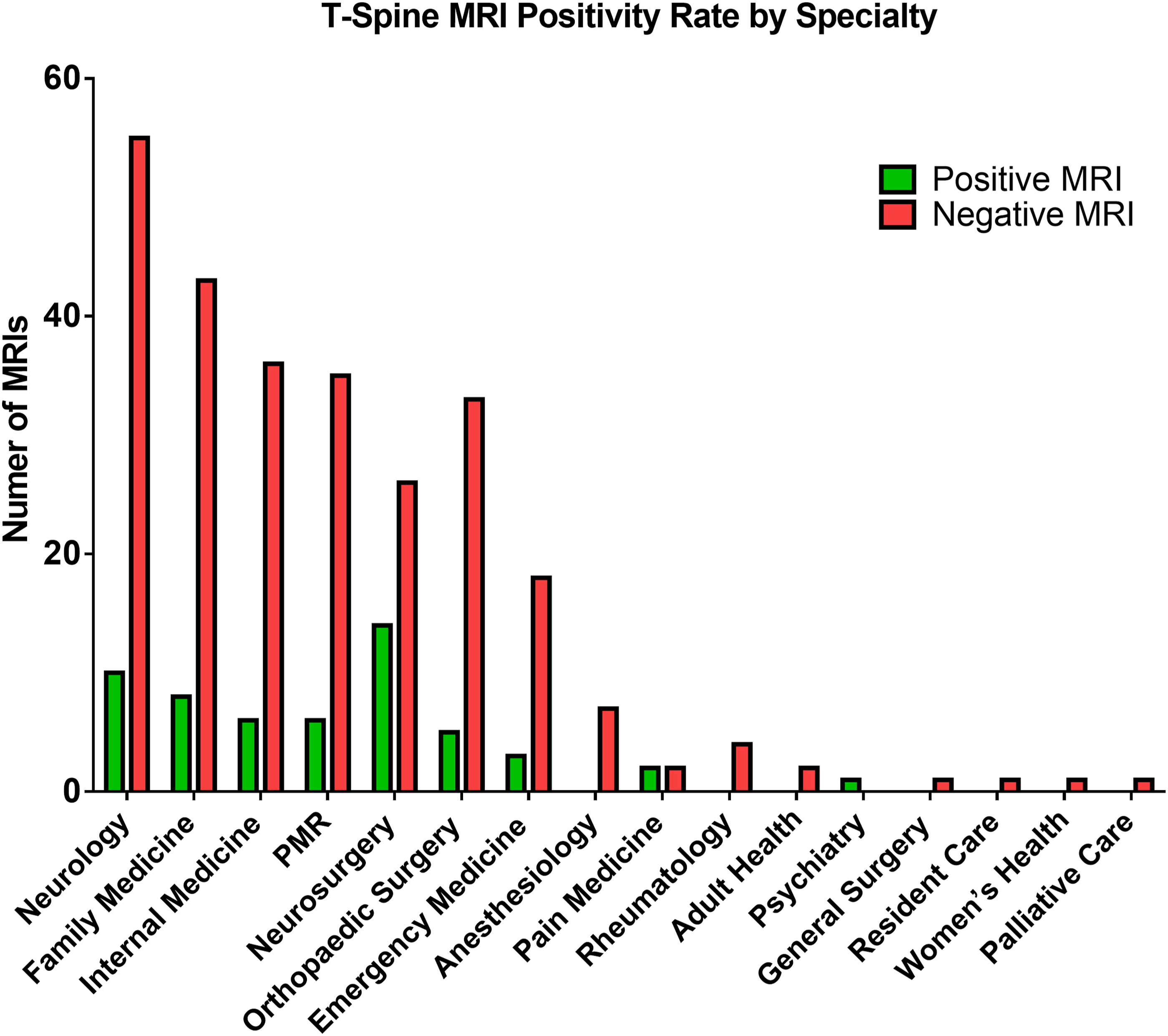
Discussion
The pattern of degenerative changes in the thoracic spine and utilization of thoracic spine MRI is poorly understood and studied, especially compared to lumbar spine MRI, which has been extensively studied.7,8,9,10,11 Multiple studies have found that lumbar spine MRI is overutilized and may lead to higher patient risk and increased healthcare costs.8,12,13 These findings have driven the Center for Medicare and Medicaid Services (CMS) to add these ordering metrics as one of the quality measures in the Hospital Outpatient Quality Reporting Program. Although the incidence of symptomatic degenerative disease in the thoracic spine is less than the lumbar spine, the difficulty in accurate diagnosis that may benefit from intervention still remains. The clinical diagnosis of symptomatic thoracic spine degenerative disease requires an expert physical exam and specific history taking skills. For example, a C5 radiculopathy may present as shoulder pain and may be interpreted to originate from the thoracic spine. A low number of imaging studies have been performed evaluating incidence of degenerative thoracic spine findings [8], and there is little evidence in the literature evaluating the cost or utility of thoracic spine MRI for degenerative disease. 14 A majority of symptomatic patients that undergo a thoracic spine MRI have mild disc degeneration. 10 Additionally, a reduction in unnecessary imaging studies can reduce healthcare cost.
Our objective in this study was to evaluate the outpatient utilization of thoracic spine MRI across ordering departments. This analysis may reveal scenarios in which the number of thoracic spine MRIs ordered could be reduced or ordering criteria could be developed based on evidence correlating physical exam findings and imaging findings. We approached this problem evaluating for a difference in positive findings for spine specialist providers (orthopeadic surgery, neurosurgery, neurology, and physical medicine and rehabilitation) against all other ordering departments. There was no significant difference in positivity rate between the spine specialist group and all other ordering departments, although there was a significant difference with more positive findings from spine surgery orders (orthopeadic surgery and neurosurgery) versus all other departments. This finding was driven by a high positivity rate in the Neurosurgery department.
The results suggest that spine surgical specialist may have a higher threshold for ordering imaging of the thoracic spine. Additionally, it may be proposed that spine surgery providers may better differentiate cervical and lumbar referred pathology from thoracic by history and physical exam. It could also be postulated that the results are related to the patient populations for the spine surgical specialists being more neurologically complicated with higher likelihood of neurologic disease. Even if referral patterns are a causative factor in the difference in positivity rate for the spine surgical specialist, this would demonstrate appropriate use of healthcare resources with specialty providers ordering high end imaging studies with a higher rate of utility in the findings. In the case of patients with atraumatic thoracic back pain, the data from this study supports initial conservative management followed by evaluation by a surgical specialist before ordering a thoracic spine MRI.
Thoracic spine MRI is a relatively low-utility study in the outpatient setting with our data demonstrating 17.2% of studies reporting relevant pathology by radiology report. A challenging aspect of this study was to isolate a patient population within our inclusion criteria based on the history within the radiology report and electronic medical record. The retrospective nature of this study and the subjectivity in exclusion of imaging studies shows a need for more high-level evidence to confirm the findings in our data set. Overall there are very few studies in the literature evaluating the utility of thoracic spine MRI and further investigations are needed to ensure high-value ordering of this advanced imaging study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.