
Abstract
Study Design
Non-randomized prospective controlled study
Objectives
To compare the safety and perioperative outcomes between patient-specific template-guided and fluoroscopic-assisted freehand techniques in transforaminal lumbar interbody fusion (TLIF) using cortical bone trajectory (CBT).
Methods
The subjects consisted of 94 consecutive patients who underwent single-level TLIF using CBT. The standard trajectory was set so as to start from the pars interarticularis, pass the inferior border of the pedicle, and end around the middle of the vertebral endplate. Template guide technique was performed in 66 patients (Guide group), and fluoroscopic-assisted freehand technique was performed in 28 patients (Freehand group). Intraoperative parameters, screw placement accuracy, and complications were compared between the two techniques.
Results
The Guide group had significantly shorter operative and radiation exposure times than the Freehand group (operative time 84.6 ± 16.7 vs 93.0 ± 15.0 minutes; P = .023, radiation exposure time 7.0 ± 6.0 vs 20.4 ± 11.8 seconds; P < .001, respectively). The screw diameter and the screw insertion depth in the vertebra in the Guide group were significantly greater than those in the Freehand group. The degree and incidence of facet joint violation were comparable between the two groups, while the accuracy of screw placement was significantly different, with no perforation rate of 97.7% in the Guide group vs 82.1% in the Freehand group (P < .001). No significant difference was found in the rate of clinically relevant complications between the two groups.
Conclusions
The template-guided technique provided a safe and highly accurate option for CBT screw placement.
Keywords
Introduction
Cortical bone trajectory (CBT) has been increasingly used as an alternative to the traditional lumbar pedicle screw trajectory because of its rigid fixation and less invasive nature.1,2 Contrary to the traditional trajectory, which follows the anatomical axis of the pedicle, CBT starts at the pars interarticularis and follows a mediolateral and caudocranial screw path through the pedicle, increasing purchase with cortical bone. 3 More recently, the long CBT is recommended for deeper screw placement within the vertebral body, as compared to the original CBT.2,4,5 The long CBT can achieve both increasing engagement with the denser region and effective loads distribution within the vertebra, thereby promoting bone fusion. Meanwhile, to create an optimal long screw path is technically challenging because of a novel and unfamiliar entry point and screw path with less anatomical landmarks, the narrow safety zone of this strict trajectory, and the difficulty of traversing dense cortical bone. Therefore, a high-level surgical skill and intraoperative support devices are required to enhance the accuracy.
Various technologies are introduced in spine surgery to improve the surgical accuracy and safety. Optical navigation and robot-assisted systems are the most advanced technologies.6,7 The advantages include high accuracy of screw placement with minimal invasiveness. However, limitations include the high cost for installation and maintenance, the space and personnel required for operation, and the additional time and intraoperative radiation exposure for registration, for which these innovative devices are not broadly available. Three-dimensional (3D) printed patient-specific template guide system has also been developed to facilitate spinal surgery.8,9 The guide is produced to fit precisely to the posterior bone surface of the corresponding vertebra based on the preoperative computed tomography (CT) bone information and is equipped with tubular drill guides for creating screw holes according to the preoperative planned trajectory. In contrast to spinal navigation system, the template guide fits onto the individual vertebrae, which is independent of intervertebral motion, and does not require great expense and extra space and personnel. This technology has been proposed as a promising option for screw placement for the entire spine from the cervical to the pelvic region, including divergent screw trajectory of CBT.
Patient-specific template guide technique for pedicle screw insertion has reportedly not only improved screw placement accuracy, but also reduced operative time, screw placement time, blood loss, and intraoperative radiation exposure, compared to freehand fluoroscopic-assisted technique.9-11 With regard to the template-guided CBT technique, cadaveric and clinical studies have reported highly accurate screw placement ranging from 2.5% to 9.4% without any cortical breach.12-16 However, there is no study that can compare it to the standard technique, and little is known about its practical impact. It is expected to be particularly compatible with the template guide technology because of the anatomical specificity and unfamiliarity of CBT. In light of the widespread use of CBT technique, the present study compared the perioperative outcomes between patient-specific template-guided and fluoroscopic-assisted freehand techniques in posterior spinal fusion using the long CBT and provided objective evidence for surgical decision.
Materials and Methods
Study Population
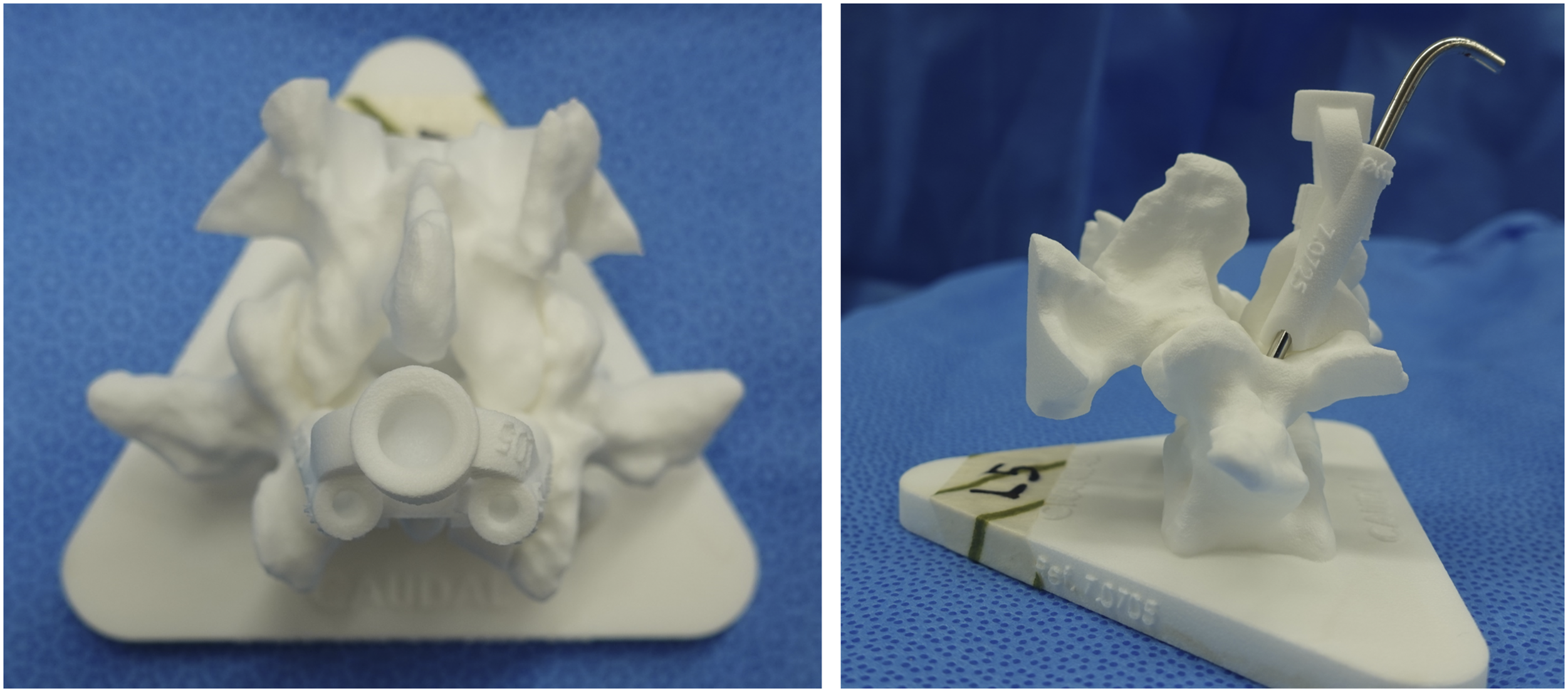
This was a non-randomized prospective controlled approved by the research ethics committee in our institute (Murayama Medical Center, ID:12-10). The written informed consent was not required in this study because all clinical and radiographic interventions followed routine protocols. The study included 94 consecutive patients (50 male and 44 female patients with a mean ± standard deviation [SD] age of 67.3 ± 10.8 years) who underwent single-level transforaminal lumbar interbody fusion (TLIF) using the long CBT technique between October 2017 and March 2022. Patients with previous lumbar surgery, spondylolysis, rheumatoid arthritis, and indication for lumbosacral fusion were excluded from the study. There were 88 patients with degenerative spondylolisthesis, 4 with disc herniation, and 2 with foraminal stenosis. Patient-specific template guide technique was performed in 66 patients (Guide group), and fluoroscopic-assisted freehand technique was performed in 28 patients (Freehand group). Patients were allocated to either group based on their available time (approximately 3 weeks) to produce and ship the guides prior to the scheduled surgery. To reduce bias, all surgeries were performed by a single surgeon who was familiar with the CBT technique since 2011. All patients underwent a routine CT scan with a slice thickness of < 1 mm preoperatively for surgical planning. In the Guide group, a 3D model of each vertebra was reconstructed from the CT data and a screw trajectory plan was developed using the MySpine MC® (Medacta International, Castel San Pietro, Switzerland) (Figure 1).12,14-16 Then, custom-made drill guides and 3D vertebral bone models that served as molds for the guides were manufactured using medical-grade polyamide and used after standard steam sterilization, similar to other implants (Figure 2). Example of preoperative planning for long cortical bone trajectory screw placement using MySpine MC® system at level L5. SAR/SAL: sagittal plane angle right/left with angulation of the screw shaft in relation to the pedicle center line, TAR/TAL: transverse plane angle right/left with angulation of the screw shaft in relation to the pedicle center line, HDL/HDR: horizontal distance left/right, VDL/VDR: vertical distance left/right. Design of the guide. A 3D-printed patient-specific template guide and lumbar mold that reproduces the posterior bone surface. The guide is equipped with tubular drill guides for creating screw holes.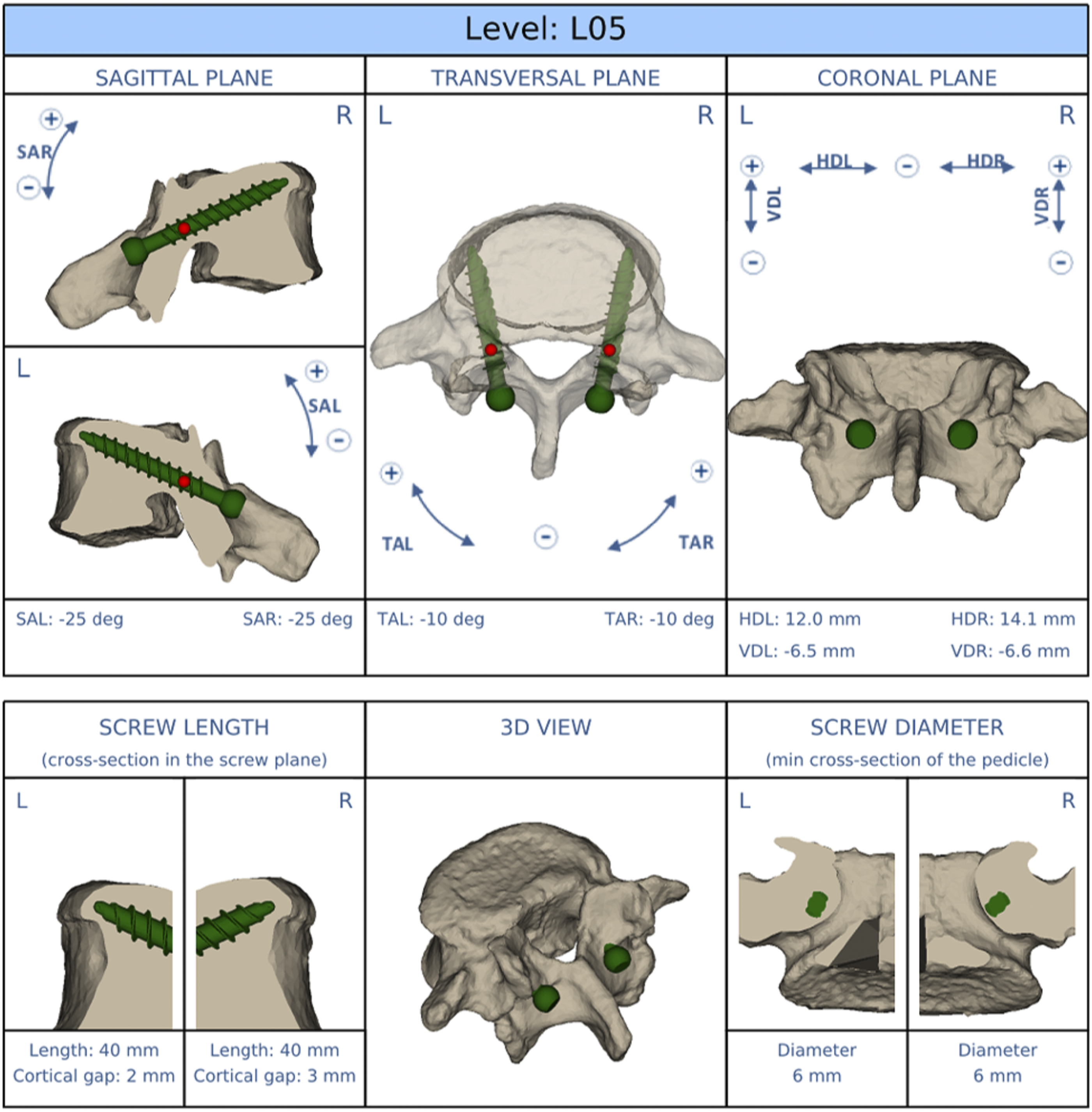
Surgical Procedure
The paraspinal muscles were dissected to expose the lateral borders of the pars interarticularis through a midline incision over the corresponding vertebrae. In this study, the standard trajectory was set so as to start from the pars interarticularis, pass the inferior border of the pedicle, and end around the middle of the vertebral endplate without bicortical penetration.4,5 In the Freehand group, the entry point and initial hole was created at the pars interarticularis using a 2-mm high-speed round burr drill. Then, the hole was dilated using a 3-mm-diameter bone probe, ending at the superior vertebral endplate. Intraoperative fluoroscopy was used during the procedure to check the trajectory. In the Guide group, after meticulous exposure of the posterior bone surface, the template guide was set on the lamina (Figure 3A). A suitable positioning of the guide was easily found by the specific fit with the bone surface and the appropriateness of the entry point position and trajectory direction by fluoroscopy. Once satisfactory fit was achieved, the surgeon held the guide firmly and drilled pilot holes of 2.7 mm in diameter along the planned trajectory to a depth 5 mm shorter than planned screw length, and then developed the rest of the screw path manually with a probe while palpating the bony integrity (Figure 3B). Intraoperative images of single-level transforaminal lumbar interbody fusion using patient-specific template guide for cortical bone trajectory screw placement. A. The guide on L5 laminar surface with L-shaped markers. B. Intraoperative radiograph showing the markers placed in the screw path.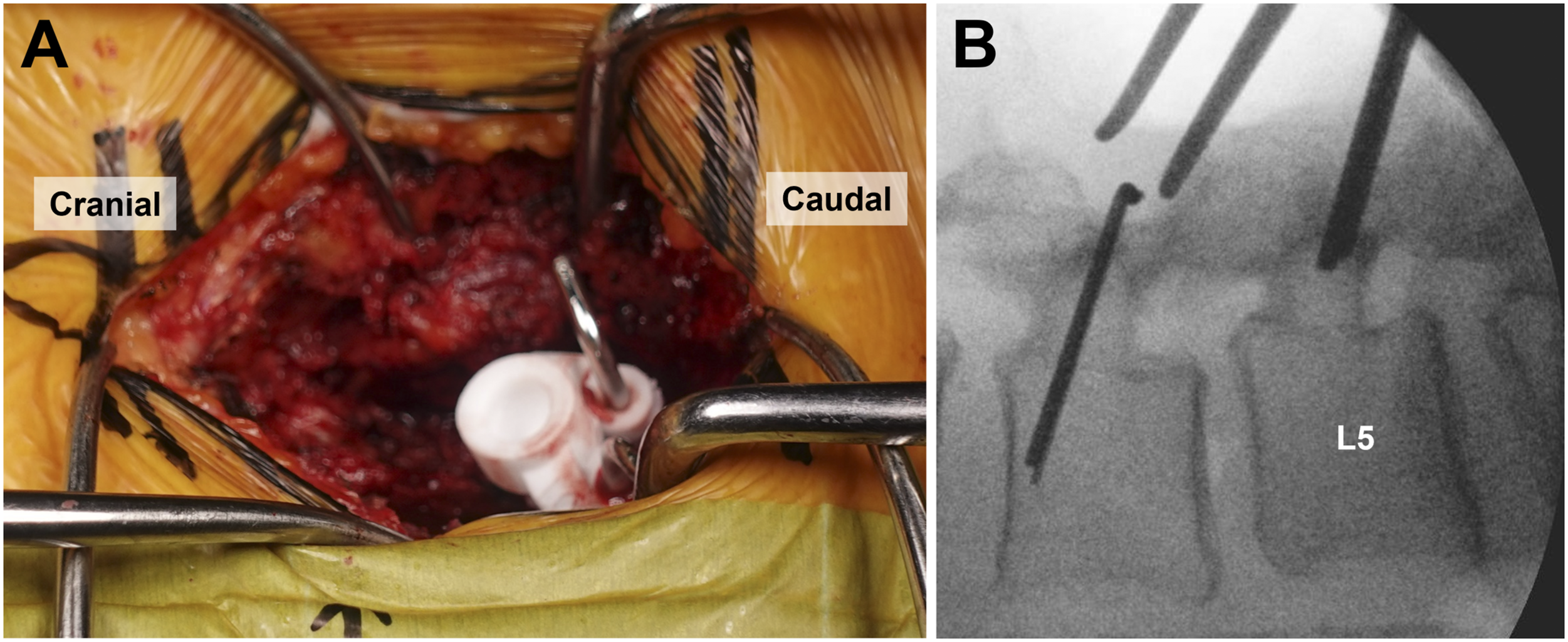
Following the creation of screw path, posterior decompression with unilateral facetectomy, interbody preparation, and insertion of a boomerang cage with local bone graft were performed. Lastly the screw paths were tapped to the size of the planned screw and screws were inserted. No cases required intraoperative screw replacement caused by malpositioning. The standard screw size in the present study was 5.5-6 mm in diameter and 35-45 mm in length.
Outcome Measures
The length of skin incision, operative time, intraoperative blood loss, intraoperative radiation exposure time, size of the screw used, depth of the screw in the vertebral body (%depth), the degree of facet joint violation (FJV) by the proximal screw at the adjacent cranial segment, accuracy of screw placement, and any complications occurred intraoperatively and within 6 months postoperatively were compared between the two groups. Screw positions were assessed from postoperative CT images obtained within a week after surgery. The %depth was defined as the ratio of screw length within the vertebral body to the anteroposterior length of the vertebral body in the axial plane. 5 The degree of FJV was evaluated according to the classification by Yson et al: grade 0 = no violation, grade 1 = screw or rod contacting with the facet joint, and grade 2 = screw penetrating the facet joint. 17 The accuracy of screw placement was graded based on the previously described classification: no perforation, grade A = < 2 mm perforation, grade B = 2-4 mm perforation, and grade C = > 4 mm perforation.8,12,16,18 A screw perforation was defined as any cortical breach outside the pedicle and vertebral body.
Statistical Analysis
Continuous and categorical variables were presented as the mean ± SD and number, respectively. The unpaired t-test and Mann-Whitney U-test were used for continuous variables, and the chi-square test and Fisher’s exact test were used for categorical variables to compare the differences between groups. JMP version 14 (SAS, Cary, NC) was used for all analyses, with the significance level set as P < .05.
Results
Comparison of Patient Characteristics.
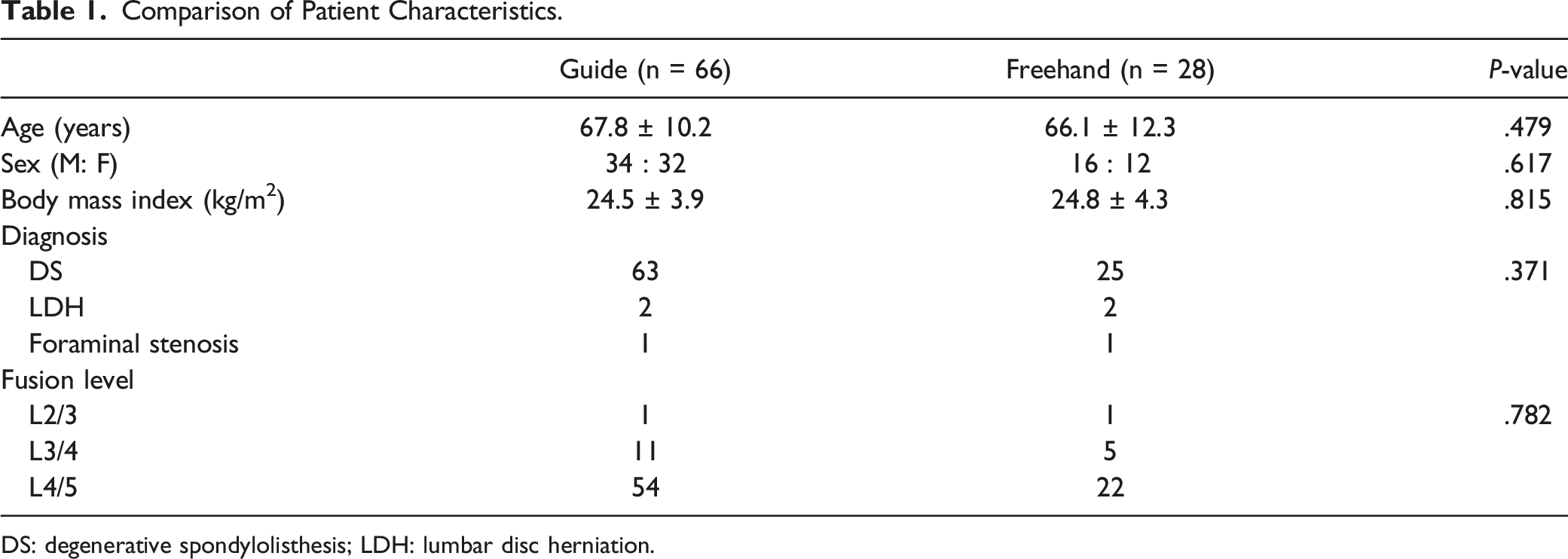
DS: degenerative spondylolisthesis; LDH: lumbar disc herniation.
Comparison of Surgical Outcomes.
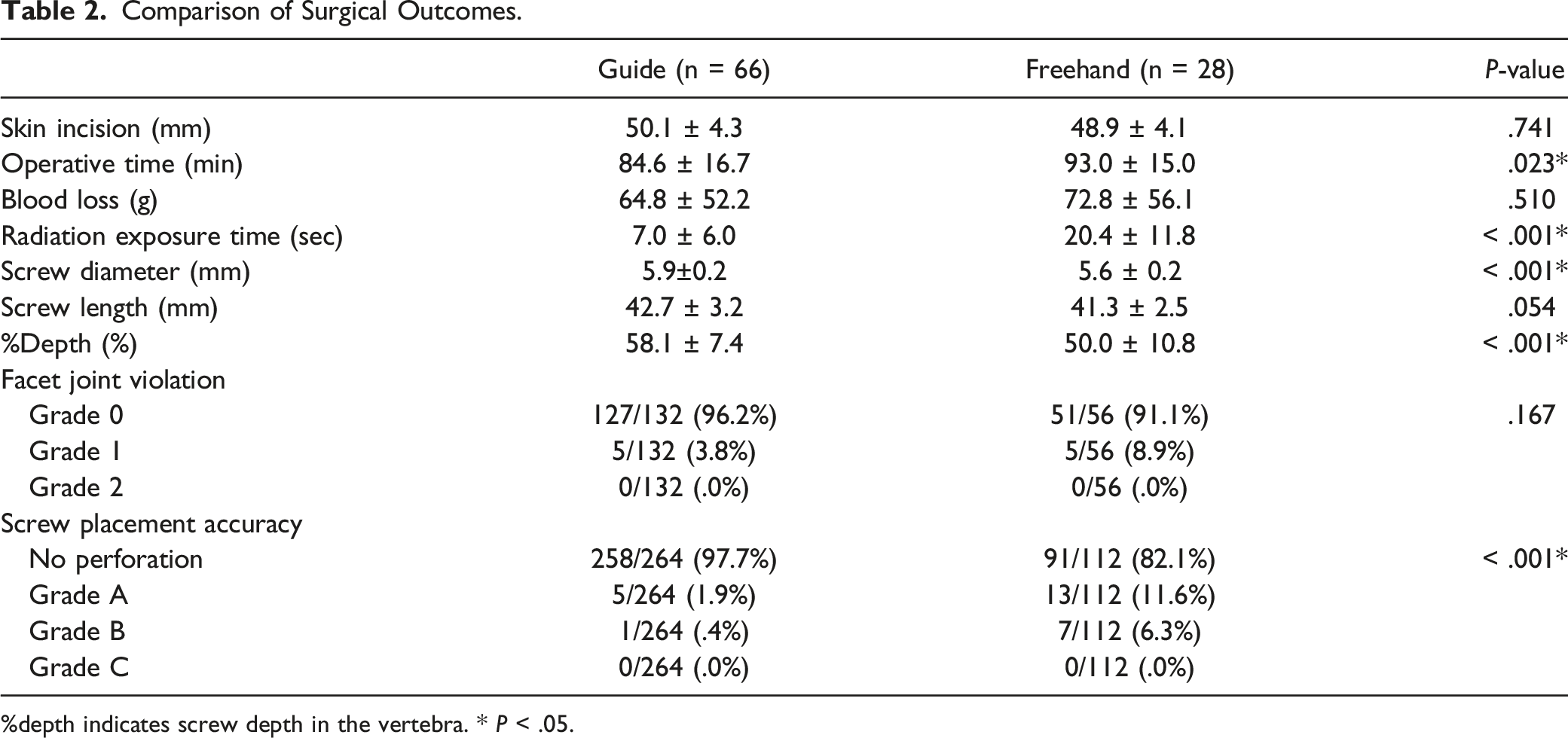
%depth indicates screw depth in the vertebra. * P < .05.
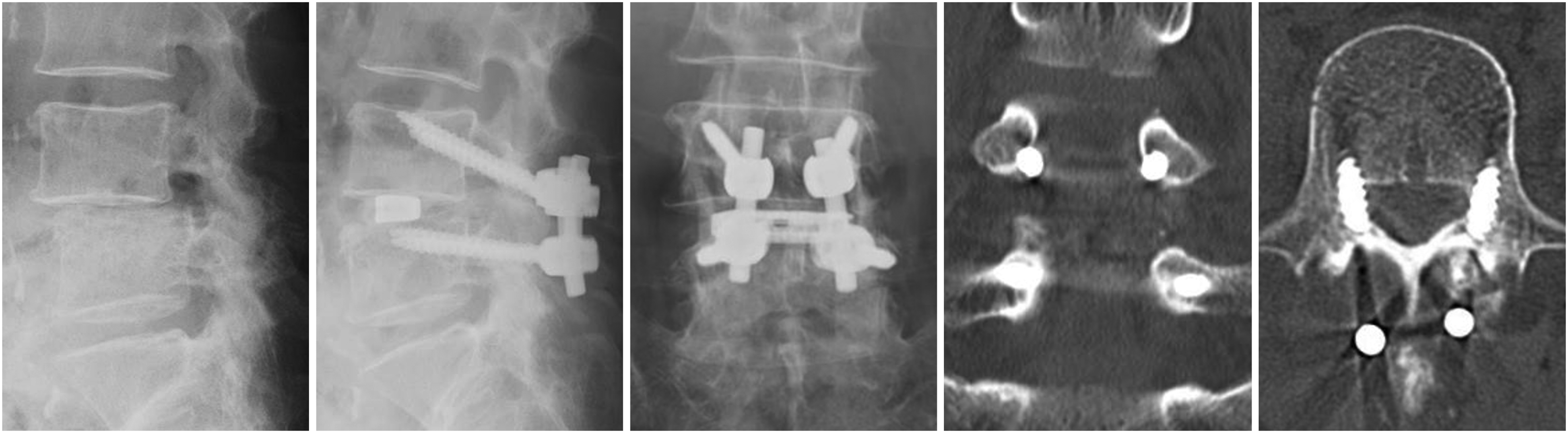
Illustrative case using freehand technique with grade B screw perforations.
Discussion
The present study was the first to compare the perioperative outcomes between patient-specific template-guided and fluoroscopic-assisted freehand techniques in spinal fusion using the CBT. The template-guided technique was highly accurate and safe, with shorter operative time and reduced intraoperative radiation exposure.
There are several clinical comparative studies on the effectiveness of the patient-specific template-guided pedicle screw placement. Recent meta-analysis by Liang et al has revealed that the template-guided technique significantly improved the accuracy of pedicle screw placements in spinal deformity surgery and reduced screw placement time and blood loss when compared to the freehand technique. 9 Li et al also reported that the template-guided atlantoaxial pedicle screw technique for odontoid fracture provided higher accuracy and reduced operative time, blood loss, and intraoperative radiation exposure than the freehand technique. 10 On the contrary, a randomized controlled study of 24 cases with lumbar pedicle screw implantation by Spirig et al reported that radiation exposure was 67% lower in the template-guided technique when compared with the freehand technique, with no significant difference in screw accuracy, operative time, and blood loss, which were inconsistent with the results of the present study. 11 This discrepancy might be due to two reasons as they mentioned: (1) the use of simple screw trajectory by highly experienced surgeons and (2) need for extensive dissection and meticulous removal of soft tissue to ensure proper fit of the template. In contrast to template guide for standard pedicle screw trajectory with convergent drill tubes, CBT template guide with divergent drill tubes is theoretically low profile and can be easily installed without additional surgical exposure. In the present study, the template was placed through a skin incision length equivalent to that of the freehand CBT technique, avoiding additional dissection of the posterior spinal elements. This could lead to different conclusions from the study by Spirig et al.
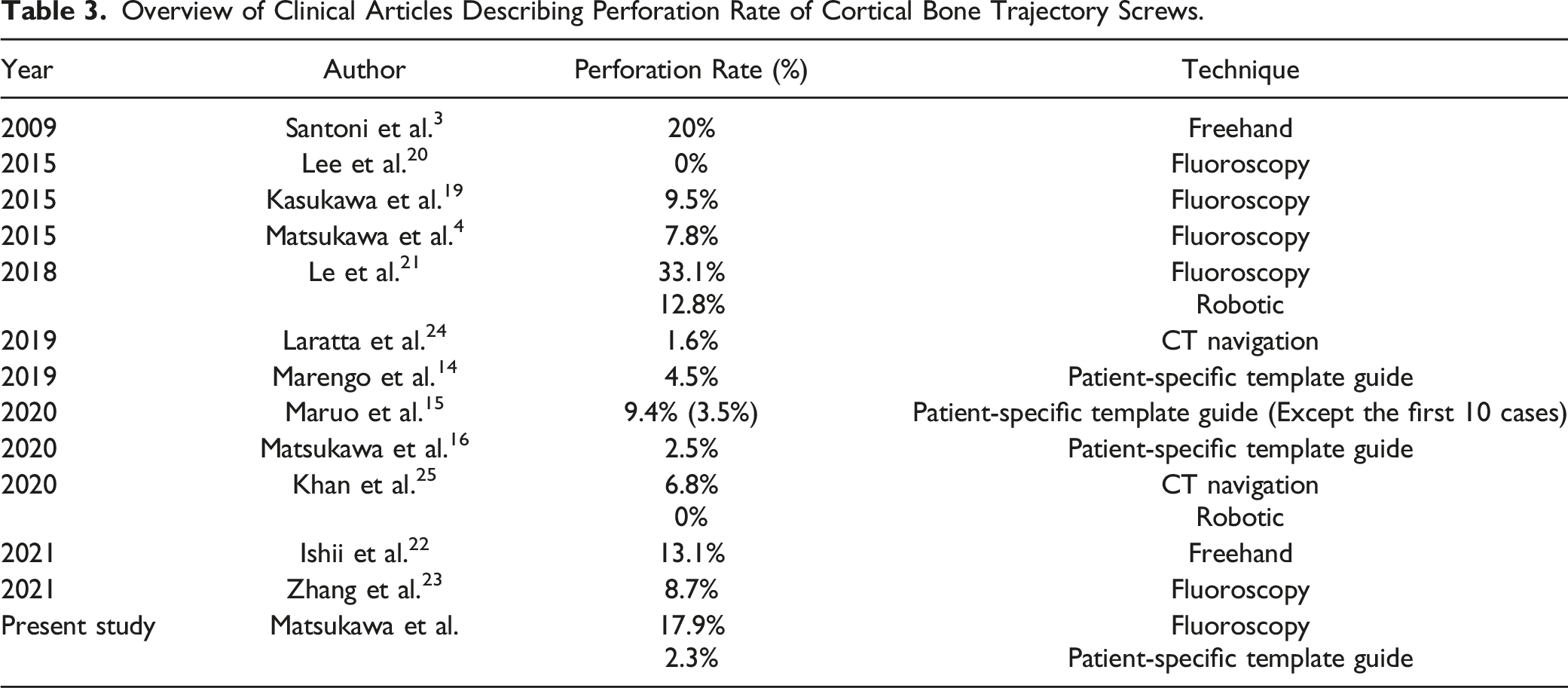
Overview of Clinical Articles Describing Perforation Rate of Cortical Bone Trajectory Screws.
In addition to the high accuracy, the template-guided technique has several other advantages. First, only CT data commonly taken prior to spinal instrumentation is required for surgical planning and production of 3D template guides, and no additional preoperative and intraoperative radiation exposure is needed just to use the guides. Second, preoperative simulation of screw placements allows surgeons to achieve optimal screw fixation by selecting optimal screw size and trajectory according to individual anatomy in advance, which may be useful for complicated trajectories such as CBT. Recent studies have shown that longer and deeper placement of CBT screws not only provides biomechanical advantages but also promotes bone fusion.2,4,5 Third, this technique is economically affordable and highly portable compared to various modern technologies, making it practically feasible in any facility. Fourth, while there is usually trade-off between exposure to radiation and accuracy of screw placement, the reduction of intraoperative radiation exposure and accuracy of screw placement is compatible with this technique. Intraoperative radiation exposure is still a critical problem for surgeons, medical staff and patients.
There are also drawbacks of this technique. First, surgeons need to meticulously remove the soft tissue to denude the bone with care not to damage the bone structures so that the template seats accurately. Next, because additional time (approximately 3-week period) and cost (approximately 200 USD for one vertebra) are needed for preoperative planning, production, and shipment, this guided technique is intended for scheduled surgeries, not applicable to emergent surgeries. A comparative cost-effectiveness analysis of the additional costs may be necessary in the future.
The present study has several limitations. First, all operations were performed by a single surgeon who was familiar with the CBT technique, including the initial experience using the template guide. Different conclusions may be drawn depending on the degree of the surgeon’s experience with the CBT technique and the use of guide system. 15 Second, clinical outcomes such as long-term functional and radiological results were not investigated. There was also an inequality in the number of patients between the two groups in this study. Therefore, additional studies with a large number of patients are necessary to elucidate the clinical impact using the template-guided technique. Third, the total intraoperative radiation exposure time was evaluated, not actual radiation dose, and the total operative time was recorded, not the time spent on individual procedures. Detailed investigation is needed to clarify the true benefits of the guide.
Conclusion
To the best of our knowledge, this study was the first to evaluate the usefulness of patient-specific template-guided screw placement using the CBT technique as compared to standard fluoroscopic-assisted freehand technique. The template-guided technique provided a safe and highly accurate option for CBT screw placement, with shorter operative and intraoperative radiation times.
Supplemental Material
Supplemental material - Comparison of Safety and Perioperative Outcomes Between Patient-specific Template-Guided and Fluoroscopic-Assisted Freehand Lumbar Screw Placement Using Cortical Bone Trajectory Technique
Supplemental material for Comparison of Safety and Perioperative Outcomes Between Patient-specific Template-Guided and Fluoroscopic-Assisted Freehand Lumbar Screw Placement Using Cortical Bone Trajectory Technique by Keitaro Matsukawa, Takashi Kaito, and Yuichiro Abe in Global Spine Journal
Footnotes
Author’s Contributions
All authors contributed to the study conception and design. Data collection and analysis were performed by Keitaro Matsukawa. The first draft of the manuscript was written by Keitaro Matsukawa and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflict of interest with respect to the research, authorship, and/or publication of this article: KM, KT, and YA have received speaker and consultant honoraria from Medacta International.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
IRB approval number: Murayama Medical Center 12-10.
Informed Consent
The written informed consent was not required in this retrospective study because all clinical and radiographic interventions followed routine assessment.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.