
Abstract
Study Design
Systematic Review.
Objectives
To systematically review the current literature and perform a meta-analysis on patients with cervical or lumbar spine Modic changes to determine if their baseline axial back pain and disability are comparable to patients without Modic changes.
Methods
A systematic review of the PubMed database was conducted in accordance with PRISMA guidelines. A meta-analysis was performed to compare the mean differences in back pain, leg pain, and disability based on the presence of cervical or lumbar spine Modic changes. A subgroup analysis of the different types of Modic changes was conducted to determine if Modic type affected back pain or disability.
Results
– After review of 259 articles, 17 studies were included for meta-analysis and ten studies were included for qualitative synthesis. In the lumbar spine, 10 high-quality studies analyzed Visual Analog Scale (VAS) back pain, 10 evaluated VAS leg pain, and 8 analyzed Oswestry Disability Index. VAS back pain (mean difference (MD), −.38; 95% CI, -.61 – .16) and Oswestry disability index (MD −2.52; 95% CI, −3.93 – −1.12) were significantly lower in patients without Modic changes. Modic change subtype was not associated with differences in patient-reported outcomes. Patients with cervical spine Modic changes did not experience more severe pain than those without MC.
Conclusions
Modic changes in the lumbar spine are not associated with clinically significant axial low back pain severity or patient disability. Similar to the lumbar spine, Modic changes in the cervical spine are not associated with symptom severity, but they are associated with pain duration.
Keywords
Introduction
Nearly 28% of US adults report back pain lasting more than 1 day during the last 3 months. 1 Neck pain, although less common, has a global age-standardized prevalence of 3.6%. 2 Both contribute significantly to global disability, poor quality of life, and significant economic costs.2-5 For most patients, the etiology of their spinal pain is undiagnosed. However, for those with a clear etiology of neck or back pain, treatment can provide significant improvement in quality of life.6-9 Vertebral end plate signal changes, specifically Modic changes (MC), are one frequently suggested cause of back and neck pain.
Modic elaborated on previous work by de Roos et al who first described subchondral vertebral body endplate signal changes in 1987. 10 The three classic MC subtypes were subsequently described by Modic as distinct magnetic resonance imaging (MRI) signaling phenotypes.11,12 Type I Modic changes (MC-I) are an inflammatory subtype that appear hypointense on T1-weighted MRI and hyperintense on T2-weighted MRI. Type II Modic changes (MC-II) represent fatty replacement of the bone marrow and appear hyperintense on T1-weighted MRI and either hyperintense or isointense on T2-weighted imaging. Type III Modic (MC-III) are the rarest subtype, representing sclerosis of the vertebral endplate. 13 MC-III appear hypointense on both T1- and T2-weighted MRI.
While the underlying cause of MCs are not fully elucidated, they are theorized to have one of the following etiologies: degenerative disc disease, infection, trauma and/or inflammation. 14 Moreover, the three primary subtypes of Modic changes appear to represent different phases of disease process. MC-I are evoked by inflammatory changes wherein vertebral endplates are disrupted and edematous changes are apparent in the bone. This hypothesis is supported by preclinical research, which has found that modulation of the local inflammatory environment occurs through cytokine signaling in the subchondral endplate.15,16 MC-I may progress to MC-II, MC-III, or resolve, although they do not always progress in a sequential order. 17 MC-II represents a more chronic disease phase highlighted by fatty replacement of subchondral bone, while MC-III are typically the final phase of MC disease. Although MC-II rarely progress to MC-III, MC-III are identified by continuous progression of the disease until subchondral bone marrow is absent and it is instead replaced by endplate sclerosis.11,17-19
While the exact etiology of MCs remains unclear, several studies have linked these lesions to both back and neck pain.20-24 These most frequently occur in the lumbar region. Studies evaluating cervical changes remain limited but have increased in recent years. 25 The literature has experienced significant growth in identifying the prevalence of and symptoms related to MCs. Therefore, the objective of this systematic review is to provide an overview of the literature evaluating the association of both lumbar and cervical MCs with patients’ baseline patient-reported outcome measures (PROMs) and to provide a meta-analysis evaluating how MCs affect PROMs.
Methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement. This study was deemed Institutional Review Board exempt since no identifiable health information was collected and only data from published studies were incorporated. We conducted a query of the PubMed database from inception until May 1, 2022, using combinations of the words “Modic changes,” “endplate signal changes,” and “outcomes.” We also conducted a reference review of included studies to identify additional studies that met inclusion criteria.
Study Eligibility
Studies were included if they described clinical pain or disability prior to any intervention in a population of patients with identifiable MCs or endplate defects in the lumbar or cervical spine on MRI. Studies were excluded if (1) a full text of the article could not be obtained, (2) the article was written in a language other than English, or (3) they were review papers. Two authors independently screened the abstracts and titles of identified articles. Disagreements on any articles at this stage were automatically included for full text review. At the full-text stage, articles were screened for inclusion based on the predetermined inclusion criteria. Discrepancies were reconciled by a more senior author.
Data Collection Quality Assessment
Authors extracted data from the included studies with a self-designed table. Contents of data selection included type and prevalence of Modic signal changes, baseline patient reported outcome measures, quality of life measures, and basic patient population statistics. A meta-analysis was conducted on any PROM that was compared by a minimum of 6 studies. This criterion was set to ensure adequate analysis of data heterogeneity. Meta-analyses were performed to compare the available PROMs among patients with and without Modic changes. Additionally, a subgroup analysis was done evaluating PROMs based on MC subtype (no-MC, MC-I, or MC-II). Due to the low number of studies evaluating cervical MCs, a meta-analysis of was not conducted.
Weighted means were evaluated for all continuous variables using a random effects model. Results are reported as weighted mean difference and 95% confidence interval. To assess the heterogeneity of studies (I2), comparisons were displayed in a forest plot. To examine publication bias, the existence of asymmetry between studies was verified and displayed in a funnel plot. Studies with data outside the funnel plot were considered biased and were removed from the meta-analysis. Studies were also assessed for bias using the validated Newcastle-Ottawa Score with a high-quality score defined as a greater than or equal to 6. 26 All statistical analyses were done using R Studio (Version 4.1.2, Vienna, Austria).
Results
Literature Search Results
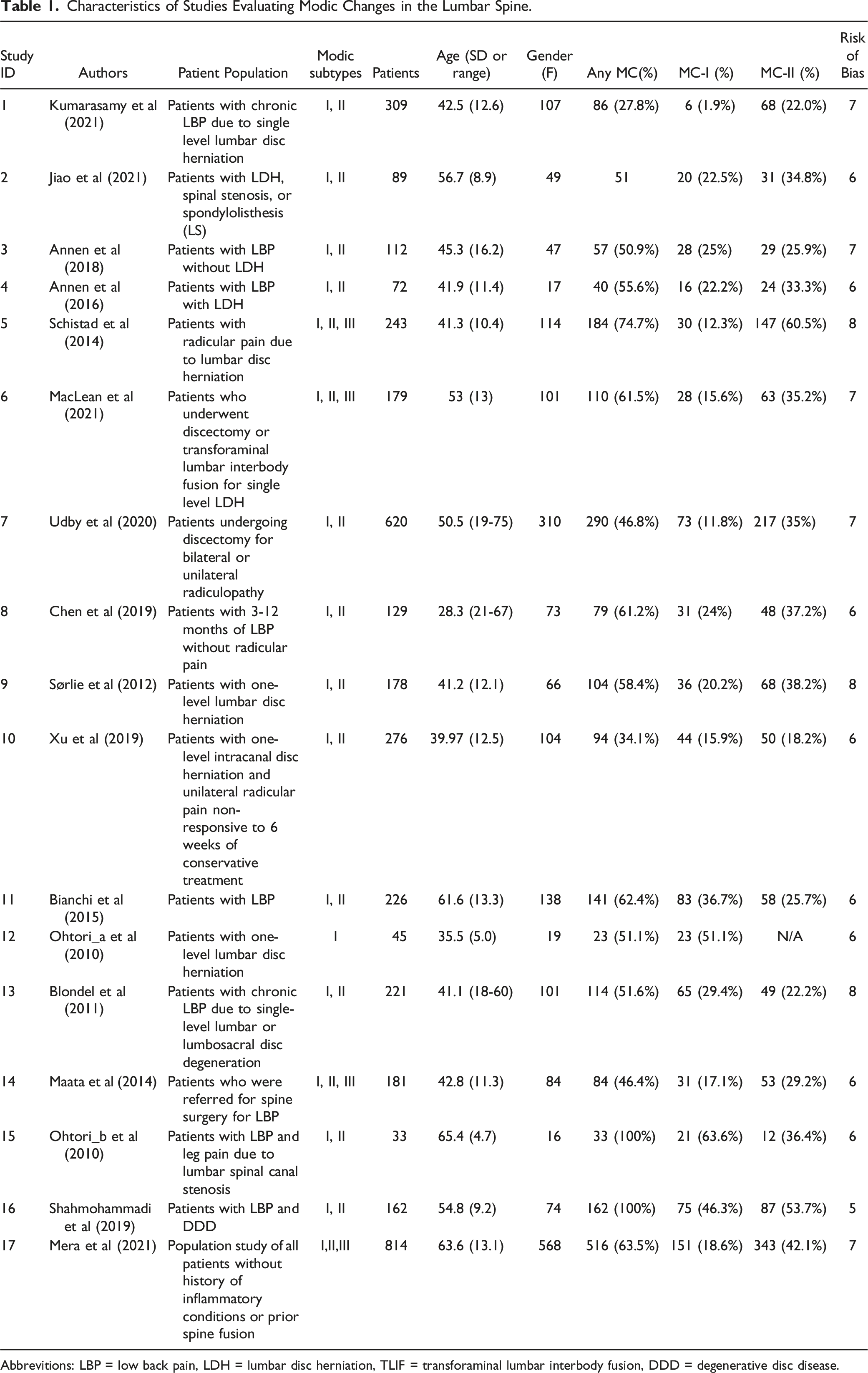
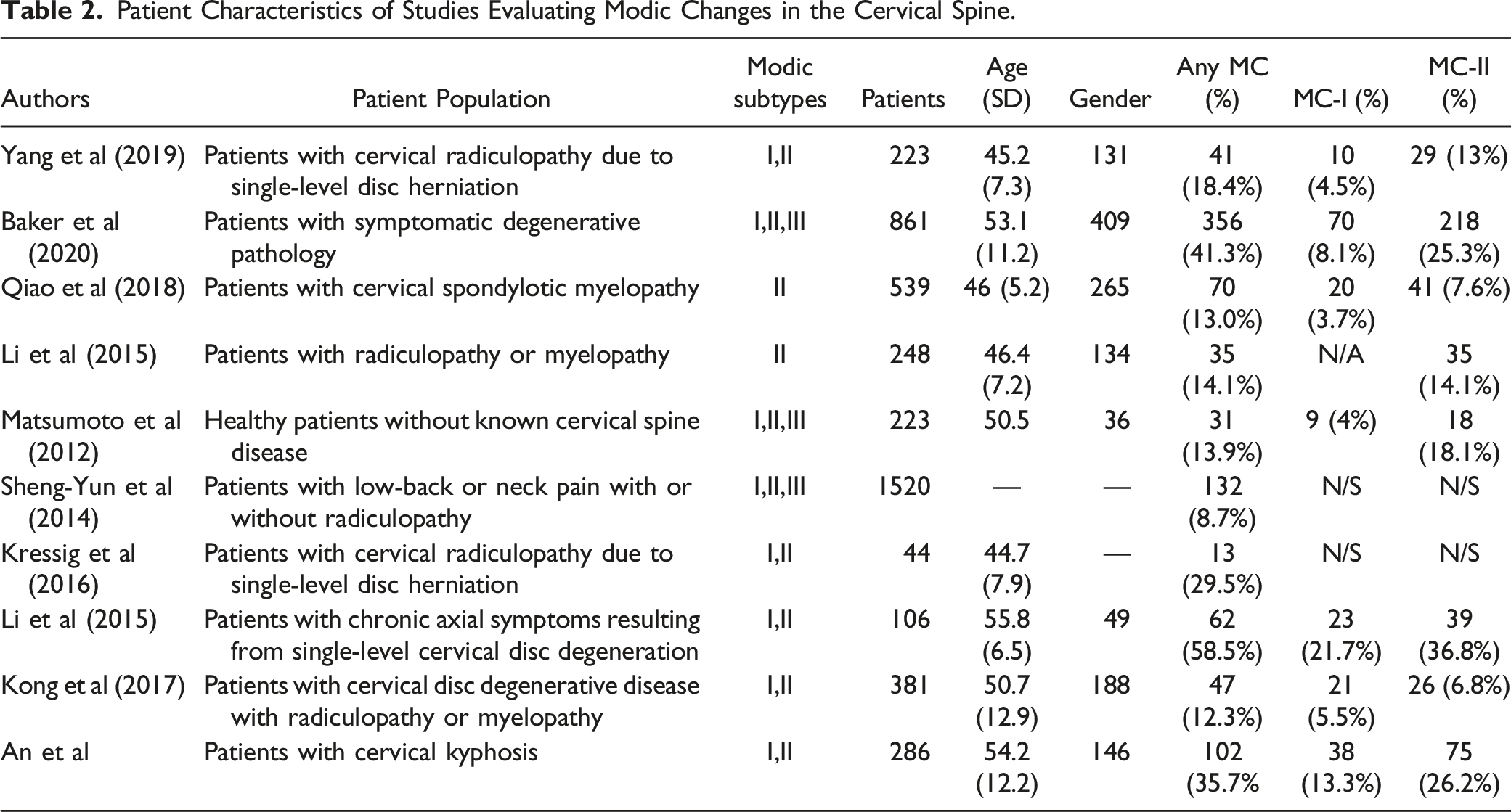
The initial literature review identified 259 articles meeting our search criteria. After title and abstract screen, 56 full text articles were reviewed. Four studies were included from citation review.22,24,27,28 Twenty-eight studies evaluated patients with MCs in the lumbar spine and ten studies evaluated patients with MCs in the cervical spine. The PRISMA search strategy is provided in (Figure 1). However, of the 28 lumbar spine studies meeting potential inclusion criteria, only 17 were included in our meta-analysis (since meta-analysis inclusion required a minimum of six studies to evaluate the same outcome measure). Thus, a total of 3889 patients were ultimately included (Table 1). No PROM in the cervical spine was evaluated by a minimum of 6 studies. Therefore, a meta-analysis was not performed, but an overview of the studies evaluating cervical spine MCs are described in Table 2. The majority (25 of 27) of studies included were considered high quality. Individual risk of bias scores are presented in Table 1 and Table 2. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram indicating study inclusion criteria and the reason for study exclusion. Characteristics of Studies Evaluating Modic Changes in the Lumbar Spine. Abbrevitions: LBP = low back pain, LDH = lumbar disc herniation, TLIF = transforaminal lumbar interbody fusion, DDD = degenerative disc disease. Patient Characteristics of Studies Evaluating Modic Changes in the Cervical Spine.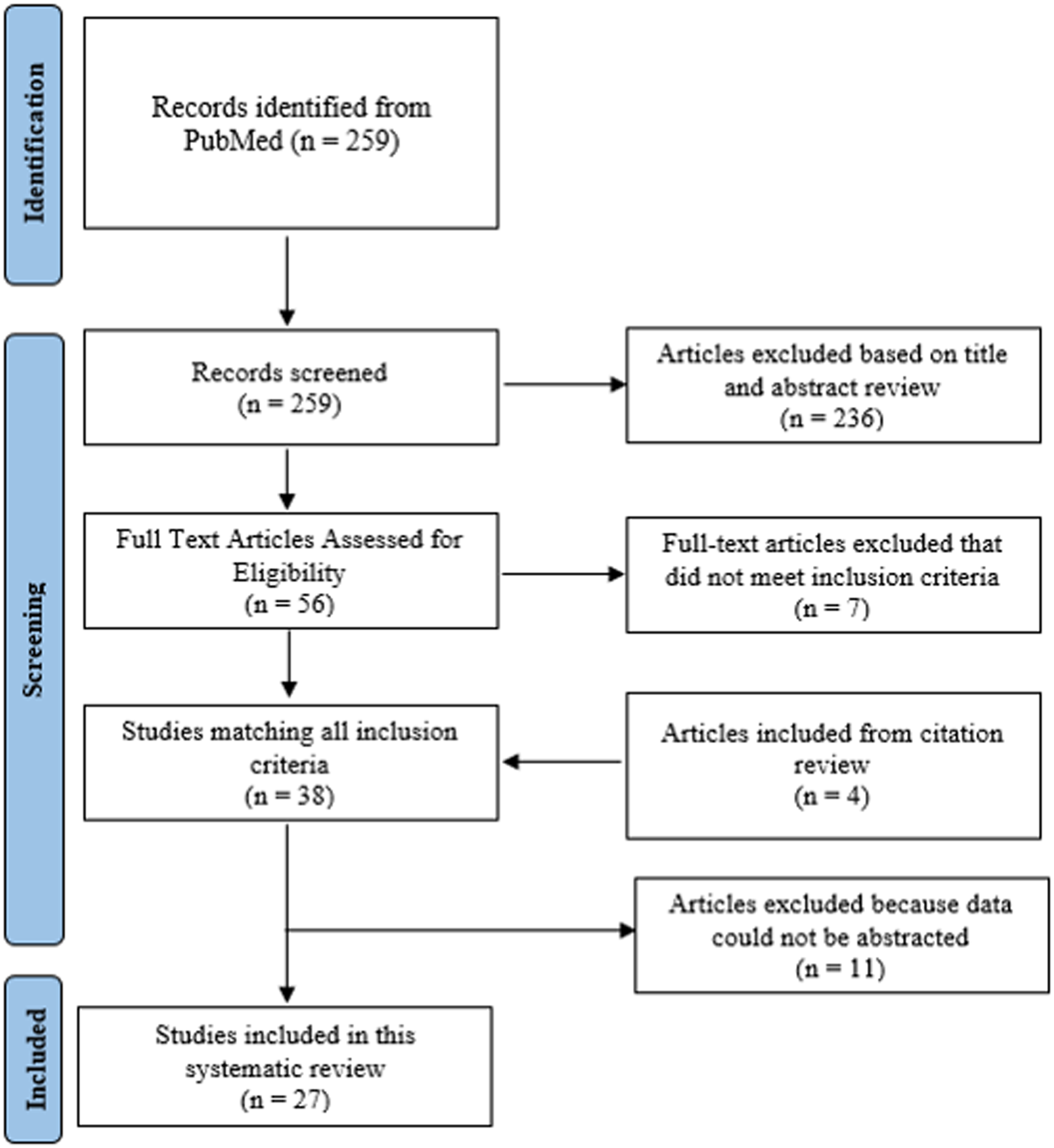
Visual Analogue Score Back Pain
Pooled reports of back pain intensity among patients with and without MC were reported in 10 studies.24,29-39 Low back pain intensity scores were standardized on a 0-10 scale. An initial funnel plot revealed possible publication bias in three studies15,29,30 After these studies were excluded, a forest plot revealed low data heterogeneity (I2 = 21%, P = .25) (Figure 2A). Publication bias was also deemed unlikely in the remaining studies (Figure 2B). When evaluating a random-effects model of the pooled studies, there was no significant difference in VAS back scores in patients with Modic changes vs those without MCs (weighted MD, −.38; 95% CI, −.61 – .16). A. Forest Plot of included studies evaluating VAS Back Pain, which are stratified based on the presence of Modic Changes. The Forest plot indicates the relative lack of back pain heterogeneity between patients with and without Modic changes. Although back pain is significantly lower in patients without MCs, the values do not meet clinical significance. 2B. Funnel plot indicates there is no obvious publication bias in any of the included studies.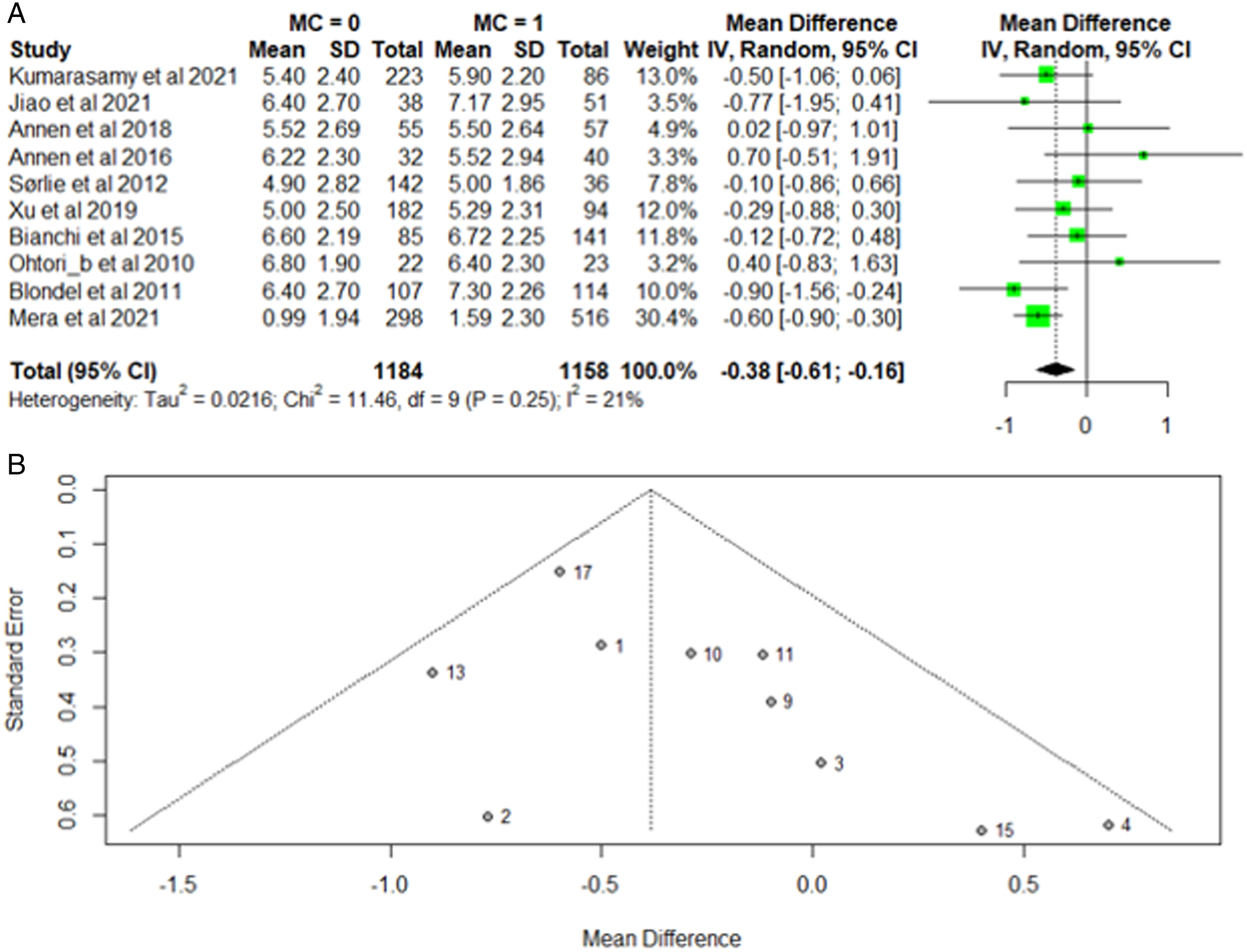
On MC subtype analysis, 12 studies specifically reported on back pain intensity in non-MC patients,15,24,29,30,32-39 14 studies were performed in patients with MC-I,15,24,29,30,32-41 and 12 were examined patients with MC-II.15,24,29,30,32-34,36,37,39-41 Subgroup analysis showed no significant differences in a weighted random-effects model for patients without MC (5.35; 95% CI: 4.43-6.27) vs patients with MC-I (5.73; 95% CI: 4.91-6.54) or MC-II (5.53; 95% CI: 4.45-6.54) (P = .83) (Supplemental Figure 2). However, there was high data heterogeneity among included studies (I2 = 99%).
Visual Analogue Score Leg Pain
Ten studies reported on leg pain scores in their analysis of patients with MCs compared to those without MCs.29-33,35,36,38,39,42 Random effects analysis of all studies demonstrated no significant association between baseline VAS leg pain score and Modic changes (MD .01, 95% CI: −.18 - .20; P = .68). Among these studies, low heterogeneity was observed (I2 = 0%). (Figure 3A). Among these studies, sensitivity analysis revealed no studies exhibiting publication bias (Figure 3B). A. Forest Plot of included studies evaluating VAS Leg Pain based on the presence of Modic Changes. The Forest plot indicates the relative lack of leg pain heterogeneity between patients with and without Modic changes. 3B. Funnel plot indicates there is no obvious publication bias in any of the included studies.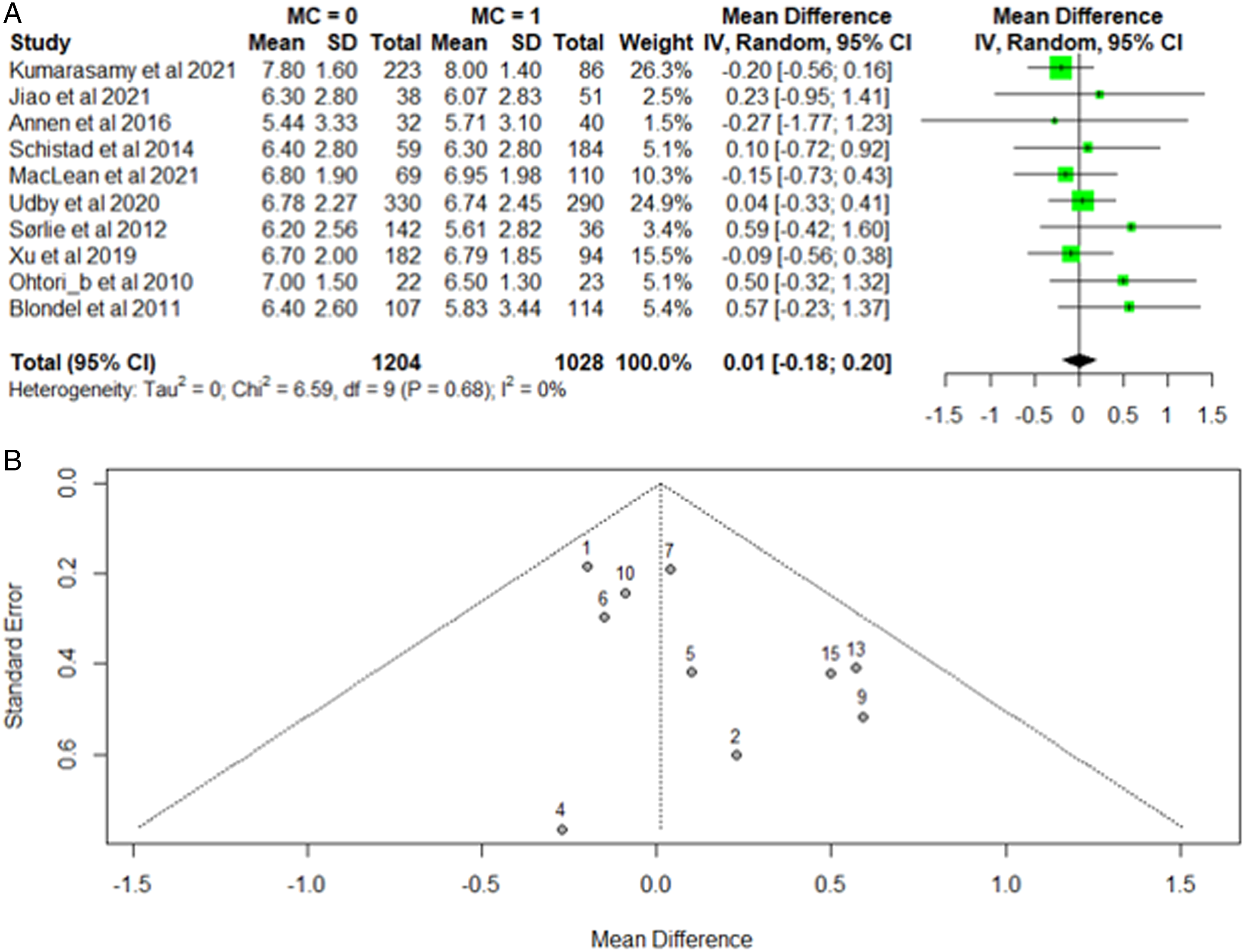
After stratification by MC subtype, nine studies were included that reported on leg pain in patients without Modic changes,29,30,32,33,35,36,38,39,42 ten examined patients with MC-I,29,30,32,33,35,36,38,39,41,42 and eight reported on leg pain in patients with MC-II.29,30,32,33,36,39,41,42 Forest plots revealed a high degree of data heterogeneity (I2 = 61%, P < .01). MC subtypes were not significantly associated with difference in VAS leg scores (P = .38) (Supplemental Figure 3).
Oswestry Disability Index
Twelve studies reported on Oswestry Disability Index (ODI) in patients with and without Modic changes.29,31-33,35,36,38,39,42,43 Two studies were at high risk of publication bias and were excluded38,42 Forest plot analysis of the eight included studies demonstrated low data heterogeneity when evaluating ODI scores between patients with Modic changes compared to those without Modic changes (I2 = 0%) (Figure 4A). A random effects comparison between patients with and without MCs demonstrated a significantly greater disability score in patients with MC (MD −2.52; 95% CI, −3.93 - −1.12) (Figure 4A). There was a low risk of publication bias among these studies (Figure 4B). Subgroup analysis was performed comparing ODI between patients with no-MC, MC-I, and MC-II, respectively. Weighted random effects modeling demonstrated no significant difference in ODI between groups (35.42 in no MC vs 36.80 in MC-I vs 34.82 in MC-II, P = .91). However, there was significant data heterogeneity between groups (I2 = 98%). A. Forest Plot of included studies evaluating Oswestry Disability Index (ODI) based on the presence of Modic Changes. The Forest plot indicates the relative lack of heterogeneity in disability between studies with Modic changes having a statitistically significant greater amount of disability. B. Funnel plot indicates there is no obvious publication bias in any of the included studies.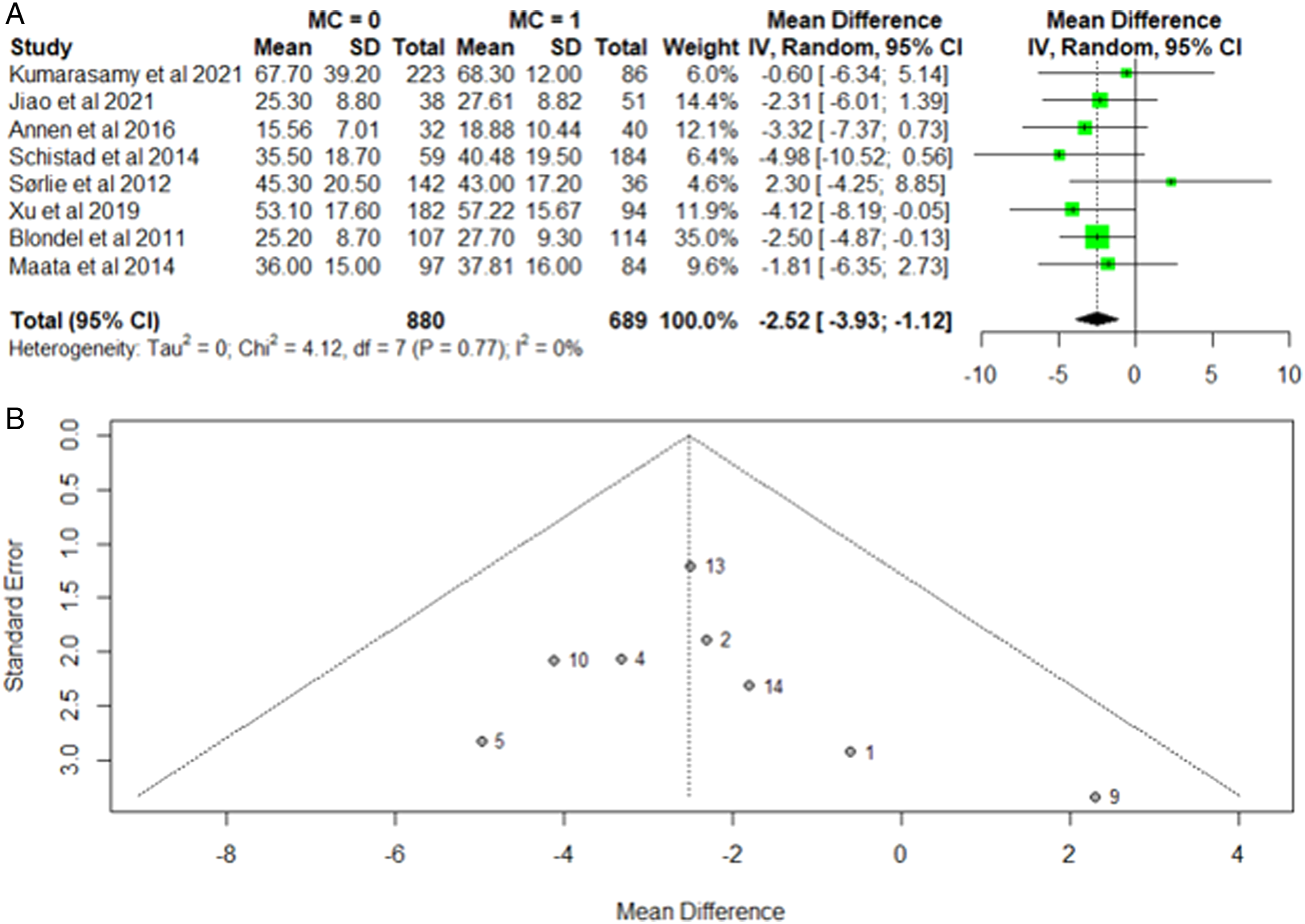
Cervical Modic Changes
Key Findings of Studies Evaluating Cervical Modic Changes.
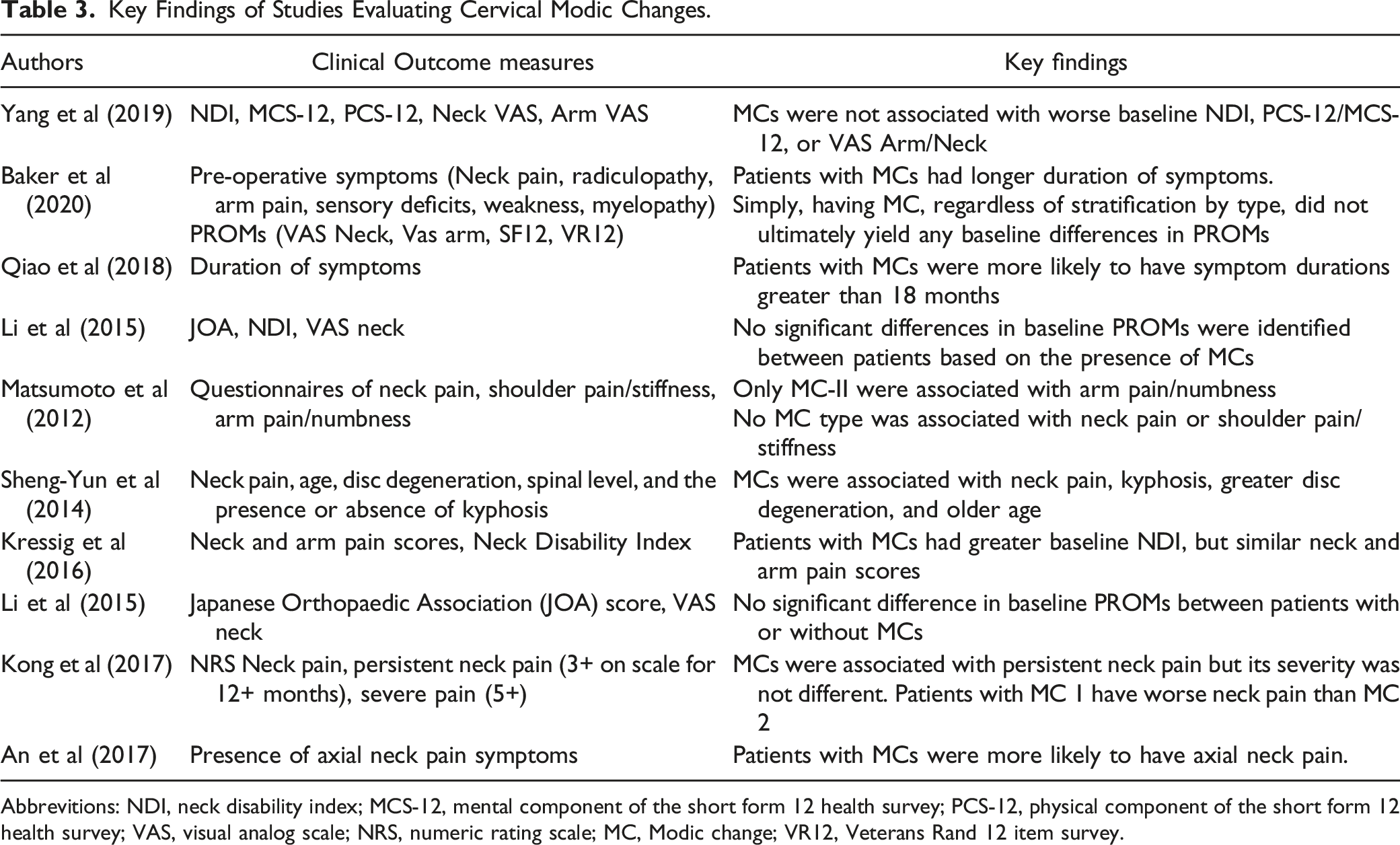
Abbrevitions: NDI, neck disability index; MCS-12, mental component of the short form 12 health survey; PCS-12, physical component of the short form 12 health survey; VAS, visual analog scale; NRS, numeric rating scale; MC, Modic change; VR12, Veterans Rand 12 item survey.
Matsumoto et al 44 identified a population of people without neck pain. Of the 223 study participants, 31 (13.9%) had Modic changes on MRI. Modic changes were not associated with neck or shoulder pain (given that the population was derived from asymptomatic patients), but MC-II lesions were associated with recent symptoms of arm pain/numbness.
Baker et al 45 identified 861 patients with symptomatic degenerative disc disease and found that 356 (41.3%) patients demonstrated some form of MCs. They found that MCs had no clear relationship with patient reported outcomes, although patients with MCs did have a longer duration of symptoms. Similarly, Kong et al 49 evaluated patients with degenerative disease causing radiculopathy and/or myelopathy and found no association between MCs and neck pain severity. However, patients with MCs were more likely to have persistent neck pain, defined as a score of at least 3/10 on neck pain score for at least 12 months. Li et al 48 similarly found no association between MCs and baseline pain or Japanese Orthopaedic Association score.
Of the two studies evaluating patients with radiculopathy due to disc herniation, Yang et al 25 included 223 patients, of whom 41 (18.4%) displayed MCs. They found no association between Modic changes and patient-reported disability, function or pain. Kressig et al 46 examined a smaller cohort of 44 patients, although they found that patients with MCs had worse baseline disability, they suggest they likely have similar pain scores compared to patients without MCs.
Qiao et al 28 evaluated 529 patients with cervical spondylotic myelopathy, 13% of whom displayed MCs. MCs were significantly associated with axial neck pain persisting greater than 18 months. However, they did not evaluate baseline differences in pain scores or PROMs between patients with and without MCs.
Sheng-Yun et al 22 identified 1520 patients with neck pain, regardless of etiology, and compared them to 120 asymptomatic patients with cervical spine MRI. Nine percent of symptomatic patients had MCs compared to only 3% of asymptomatic patients. Patients with MCs were also more likely to have concomitant disc degeneration and cervical kyphosis. Li et al 47 evaluated any patients with radiculopathy or myelopathy requiring anterior cervical discectomy and fusion (ACDF). They only evaluated patients with MC-II lesions; however, they found no significant association between baseline PROMs and the presence of MCs.
In one study evaluating patients with cervical kyphosis, An et al. 27 identified that patients with Modic changes were 5.4 times more likely to experience axial neck pain than patients with kyphosis and no MCs. However, they did not evaluate specific patient reported outcome measures or VAS scores.
Discussion
Low back pain is the leading cause of disability worldwide.3,50 Patients with identifiable sources of pain may benefit from targeted intervention, although unequivocally identifying spinal pain generators can be challenging since most asymptomatic patients have abnormalities on MRI including disc degeneration and central canal stenosis.51,52 If MCs are identified as a frequent source of pain across multiple studies, targeted treatment of these abnormalities may be one avenue to reduce patients’ time off work, while also lowering disability claims.24,53 This systematic review and meta-analysis evaluated the effects of Modic changes, a theorized etiology of axial pain, on the presence of patient reported disability and neck/low back pain. Our pooled analysis suggests that patients with MCs in the lumbar spine have significantly worse back pain and disability; however, these findings appear to be clinically insignificant based on previously established minimal clinically important differences (MCIDs). While the literature evaluating cervical spine MCs and their effect on baseline pain is limited, patients with cervical spine MCs tend to have longer symptom duration defined as persistent pain, but similar pain intensity and neck disability.
The most recent prior meta-analysis attempting to correlate MCs and low back pain found that MCs increased the likelihood of symptomatic back pain by a factor of 3.2-6.1. 54 However, that study only pooled patients undergoing provocative discography, which itself may be a significant pain generator and lead to significant long-term disc disease. 55 Further, while their question centered on identifying whether patients with MCs were more likely to have back pain, the question appears somewhat moot in a population of patients who required a lumbar spine MRI due to persistent lower back pain. Therefore, our study attempted to address a more prudent question, which is whether MCs may produce a significantly altered disease course defined by greater symptomatic back pain intensity or disability.
When aggregating all lumbar spine studies, regardless of MC subtype, Modic changes were associated with statistically worse back pain and disability, but the mean differences were small indicating they were clinically insignificant. This can easily be appreciated when evaluating well-established MCIDs for VAS back pain (1.2) and ODI (12.8), which serves as the threshold for the smallest change perceived to be important to patients.56,57 Our meta-analysis found that the weighted mean differences for VAS back pain (.38) and ODI (2.52) were substantially lower than the required threshold needed to be considered clinically important to patients. Therefore, the current literature shows, with some level of confidence, that Modic changes are not a clinically significant source of back pain severity or disability. This finding is strengthened by the low data heterogeneity present (I2 = 21%) indicating that this was a consistent finding across all studies evaluated. However, there is some evidence that MCs are linked to symptom chronicity as seen by studies suggesting that patients with MCs are more likely to have persistent symptoms.28,45,49
Since recent evidence supports MC-I phenotypes may be greater pain generators than MC-II or MC-III subtypes, we analyzed whether any correlation existed between back pain severity or disability across MC subtypes. 24 While this analysis was fraught with significant data heterogeneity (I2 = >97%, both), there was no clear evidence supporting different MC subtypes resulted in greater low back pain intensity or disability ([no MCs – VAS Back: 5.35; ODI: 35.4]; [MC-I – VAS Back: 5.73; ODI: 36.8] or [MC-II – VAS Back: 5.53; ODI: 34.8]).
When evaluating MCs’ effects on radicular leg pain, VAS Leg pain scores were not significantly different between groups with or without MCs. Since Modic changes represent inflammatory changes or endplate sclerosis confined to the vertebral body, nerve root compression and resultant radiculopathies are not an expected finding. Therefore, this finding may provide some additional validity to the data obtained from our meta-analysis. Although there was insufficient data to perform a meta-analysis evaluating a relationship between MCs and radiculopathy in the cervical spine, there were two studies that found no significant relationship.25,46
Literature evaluating Modic changes in the cervical spine remains limited with only ten studies meeting inclusion criteria. None of the included studies identified differences in axial neck pain severity based on the presence or absence of Modic changes. However, five studies demonstrated an association with the presence of pain,22,27 persistence of pain, 49 or symptom duration.28,45 Clinically, this may indicate that patients with Modic changes present similarly to other patients with neck pain, but they may have experienced a prolonged disease course. Qiao et al 28 identified MC-II as a primary cause of longer symptom duration, which supports the theory that MC-II is indicative of long-standing disease course compared to MC-I, which is more likely to be identified in the acute to subacute setting.
Vertebral end plate signal changes (VESCs) are another potential source of back pain, but they have only recently been recognized as a distinct phenomenon from Modic changes.58,59 VESCs include Schmorl’s nodes, insufficiency fractures, endplate erosions, and endplate calcifications, all of which display distinct phenotypes on imaging. 60 Historically, these lesions were thought to be a common finding in asymptomatic patients. 52 However, several recent studies suggest that the combined Modic-endplate disruption phenotype results in significantly greater back and neck pain compared to Modic changes independently.20,45,61 The literature on this phenotype remains extremely limited. However, the clinical impact of concomitant endplate defects and Modic changes may significantly impact patient presentation and serve as a prognostic factor for patient outcomes. 61 Future research should evaluate this phenotype and its potential impact on axial back pain and disability with a particular emphasis on whether any potential increase in pain or disability reaches the MCID threshold.
Patients with greater pain intensity or disability may be more likely to require additional treatment including non-operative or operative management. Several studies and reviews have evaluated both operative and non-operative treatment for Modic changes.62-65 A recent systematic review and meta-analysis of operative treatment for Modic changes demonstrated that surgical intervention for discal or vertebral pathologies successfully treat patient symptoms regardless of the presence of Modic changes. 63 Several non-surgical interventions have been evaluated in attempts to address discogenic back pain secondary to Modic changes including antibiotics, corticosteroids, basivertebral nerve ablation, physical therapy, and bisphosphonates.33,34,64-68 However, all of these therapies have varying levels of efficacy without conclusive evidence pointing towards superiority of a specific treatment. Based on the results of the current meta-analysis, the similar baseline PROMs between patients with or without Modic changes may add to the complexities of treatment algorithms for multifactorial discogenic back pain. Moreover, the various operative and non-operative interventions may be dependent on concomitant spinal pathologies and specific patient symptoms rather than Modic changes.
Several limitations of this systematic review and meta-analysis exist. Significant heterogeneity in studies reporting Modic subtypes made it inappropriate to draw strong conclusions regarding the impact of specific Modic subtypes, particularly differences between MC-I vs MC-II. However, our analysis is strengthened by the low differences in pain or disability between patients with or without Modic changes after they were aggregated irrespective of Modic type, something that has not been previously performed. While this may be subject to study bias, efforts to account for bias by excluding studies outside of our funnel plot further validate these findings. It should be noted that each author group may have defined and classified MCs differently. This may have accounted for some study heterogeneity, but this could not be accounted for or controlled for in our study. Additionally, we were unable to conduct a meta-analysis of axial neck pain or disability in patients with Modic changes of the cervical spine due to the limited literature evaluating these patients, but all available evidence suggests that Modic changes do not significantly increase neck pain intensity.22,28,44-49
Conclusion
Previously reported associations between Modic changes and axial back pain and patient disability do not meet clinical relevance in either the lumbar or cervical spine. Moreover, this review suggests that Modic changes do not serve as prognostic indicators of disease severity. Future studies evaluating the connections between VESCs and Modic changes are needed given emerging evidence linking the combined disease process with greater back pain severity. Despite the expanding literature on Modic changes and PROMs, additional studies should evaluate the impact of MC size and duration on symptom intensity and disability.
Supplemental Material
Supplemental material - Modic Changes of the Cervical and Lumbar Spine and Their Effect on Neck and Back Pain: A Systematic Review and Meta-Analysis
Supplemental material for Modic Changes of the Cervical and Lumbar Spine and Their Effect on Neck and Back Pain: A Systematic Review and Meta-Analysis by Mark J. Lambrechts, Tariq Z. Issa, Gregory R. Toci, Meghan Schilken, Jose A. Canseco, Alan S. Hilibrand, Gregory D. Schroeder, Alexander R. Vaccaro, and Christopher K. Kepler in Global Spine Journal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.