
Abstract
Study Design
Retrospective cohort study.
Objective
To explore the association between craniocervical sagittal balance and clinical and radiological outcomes of cervical disc replacement (CDR).
Methods
Patients who underwent 1-level and 2-level CDR were retrospectively analyzed. Clinical outcomes were evaluated using scores on the Japanese Orthopaedic Association (JOA), Visual Analogue Scale (VAS), and Neck Disability Index (NDI). The craniocervical sagittal alignment parameters, including the C0-C2 Cobb angle, C2-C7 Cobb angle, C2 slope, T1 slope, C2-C7 sagittal vertical axis (SVA), C1-C7 SVA, the center of gravity of the head (CGH)-C7 SVA, and range of motion (ROM) at the surgical segments were measured.
Results
A total of 169 patients were involved. Significantly lower pre- and postoperative C2 slope and CGH-C7 SVA were found in arthroplasty levels with better ROMs. Patients with a higher preoperative C2 slope and CGH-C7 SVA had lower cervical lordosis and ROM after surgery. There were no significant differences in the clinical outcomes between patients with different sagittal balance statuses. C2-C7 SVA and CGH-C7 SVA were significantly associated with radiographic adjacent segment pathology (rASP).
Conclusion
Craniocervical sagittal balance is associated with cervical lordosis and ROM at the index level after CDR. A higher preoperative SVA is related to the presence and progression of rASP. A relationship between sagittal alignment and clinical outcomes was not observed.
Keywords
Introduction
The cervical spine is a highly intricate segment and is responsible for supporting the weight of the head as well as maintaining horizontal gaze. 1 Cervical sagittal alignment plays a crucial role in transmitting mechanical loads and maintaining the physiological function of the cervical spine, which is considered one of the most critical factors affecting the outcomes of surgery and health-related quality of life.2,3 Deviations from normal sagittal balance are associated with neck pain, cervical spondylosis, and disability.4,5
Cervical disc replacement (CDR) is an effective procedure for the treatment of cervical radiculopathy and myelopathy, as it boasts the advantage of preserving motion. CDR has been demonstrated to have at least equivalent clinical effectiveness compared with anterior cervical discectomy and fusion (ACDF) through several randomized controlled studies with long-term results.6-8 Several studies have investigated the relationship between cervical sagittal alignment parameters and clinical and radiological outcomes after CDR and suggested that imbalanced global and regional cervical sagittal alignment is associated with heterotopic ossification (HO) and radiographic adjacent segment pathology (rASP).9-12 However, the sagittal parameters concentrated on the subaxial sagittal parameters and the cervicothoracic junction parameters. The influence of craniocervical sagittal balance has rarely been reported.
As one of the most important functions of the cervical spine is to support the mass of the head, the cranial position in the sagittal plane may play an essential role in cervical sagittal balance and surgical outcomes. Previous studies have shown the significance of indices evaluating the balance of the gravity of the head in patients who underwent ACDF and laminoplasty.13-15 However, the effect of craniocervical sagittal balance on the patient-reported outcomes and radiological results of CDR has been poorly studied. Therefore, this study aimed to evaluate the craniocervical sagittal alignment parameters in patients who underwent CDR to determine whether preoperative and postoperative craniocervical sagittal alignment affects the clinical and radiological outcomes after CDR.
Methods
Study Population
The Ethics Committee of West China Hospital of Sichuan University approved the current retrospective study (Project License Number 20190946). All patients provided written informed consent. From January 2009 to December 2019, patients who underwent 1-level or 2-level CDR with Prestige-LP (Medtronic, Dublin, Ireland) in our institution were retrospectively identified. The inclusion criteria were as follows: (1) 18-65 years old; (2) 1-level or 2-level cervical degenerative disc disease causing symptomatic radiculopathy or myelopathy between C3 and C7; and (3) failure of strict conservative therapy for at least 12 weeks. The exclusion criteria were as follows: (1) a follow-up period of less than 2 years; (2) instability, irreducible kyphosis, or severe spondylosis at the index level; (3) previous history of cervical spine surgery; and (4) nondegenerative cervical spine diseases.
Surgical Procedure
All surgeries were performed by the same senior surgeon using a standard Smith-Robinson approach. Discectomy and thorough decompression were performed and the endplate was carefully prepared with a high-speed burr. A rail cutter guide and bit were then used to drill the fixation channels in the endplates. Then, the Prestige-LP disc of the most suitable size was implanted into the intervertebral space. The same procedure was performed at the other segment in patients with 2-level lesions.
Clinical and Radiographic Evaluations
Clinical outcomes were evaluated preoperatively and at the last follow-up postoperatively using scores on the Japanese Orthopaedic Association (JOA), Neck Disability Index (NDI), and Visual Analogue Scale (VAS) for the neck. Lateral radiographs of the cervical spine were obtained with the patients in a standing position and maintaining horizontal gaze, with the hips and knees extended. The C0-C2 angle was defined as the angle between McGregor’s line and the line parallel to the inferior endplate of C2. Cervical lordosis (CL) was quantified through the C2-C7 Cobb angle, namely, the angle formed between the caudal endplate of the C2 and C7 vertebrae. The functional spinal unit (FSU) angle was defined as the angle between the lines from the superior endplate of the cranial vertebra and the inferior endplate of the caudal vertebra at the index level. The range of motion (ROM) of the index level was calculated as the difference in the FSU angle between flexion and extension radiographs. The C2 slope and T1 slope were measured by the angle between the horizontal line and the inferior endplate of the C2 vertebra and superior endplate of the T1 vertebra, respectively. The center of gravity of the head (CGH)-C7 sagittal vertical axis (SVA) was measured by the distance from the posterosuperior corner of C7 and the plumb line from the anterior margin of the external auditory canal shade. If there were two shades owing to the oblique view of the cranium, the middle of the two anterior margins was considered the starting point of the plumb line.
16
C1-C7 SVA was defined as the distance from the posterosuperior corner of C7 and the plumb line from the center of the anterior margin of the C1 body. C2-C7 SVA was the distance between the posterosuperior corner of C7 and the plumb line from the center of the C2 vertebra (Figure 1). Radiographic measurement of the sagittal parameters. (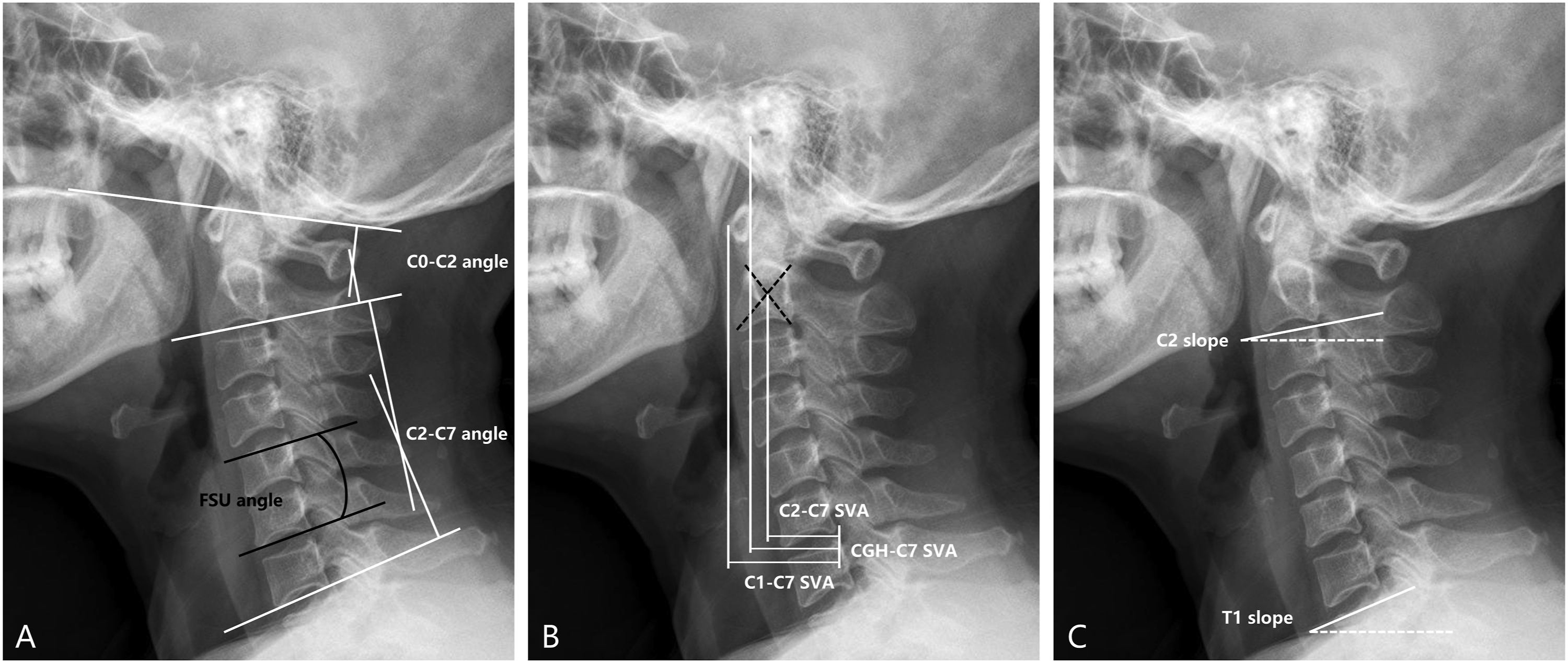
rASP was defined with the Kellgren-Lawrence scale 17 on X-rays preoperatively and at the last follow-up postoperatively. The progression of rASP was marked as an increase in the Kellgren-Lawrence score during follow-up. 18
Statistical Analysis
Continuous variables are presented as the mean±standard deviation (SD), and categorical variables are presented as the number of cases. A paired t-test was used to compare the clinical outcomes and sagittal alignment parameters between pre- and post-operation. Student’s t-test or the Mann‒Whitney U test was used to compare continuous variables depending on the normality of the data. The correlations between sagittal alignment parameters were analyzed using the Pearson correlation coefficient. A 2-tailed P value < .05 was considered statistically significant. All statistical analyses were performed using SPSS 25.0 software (IBM Corp., Armonk, New York, USA).
Results
Demographics
Demographic Data.
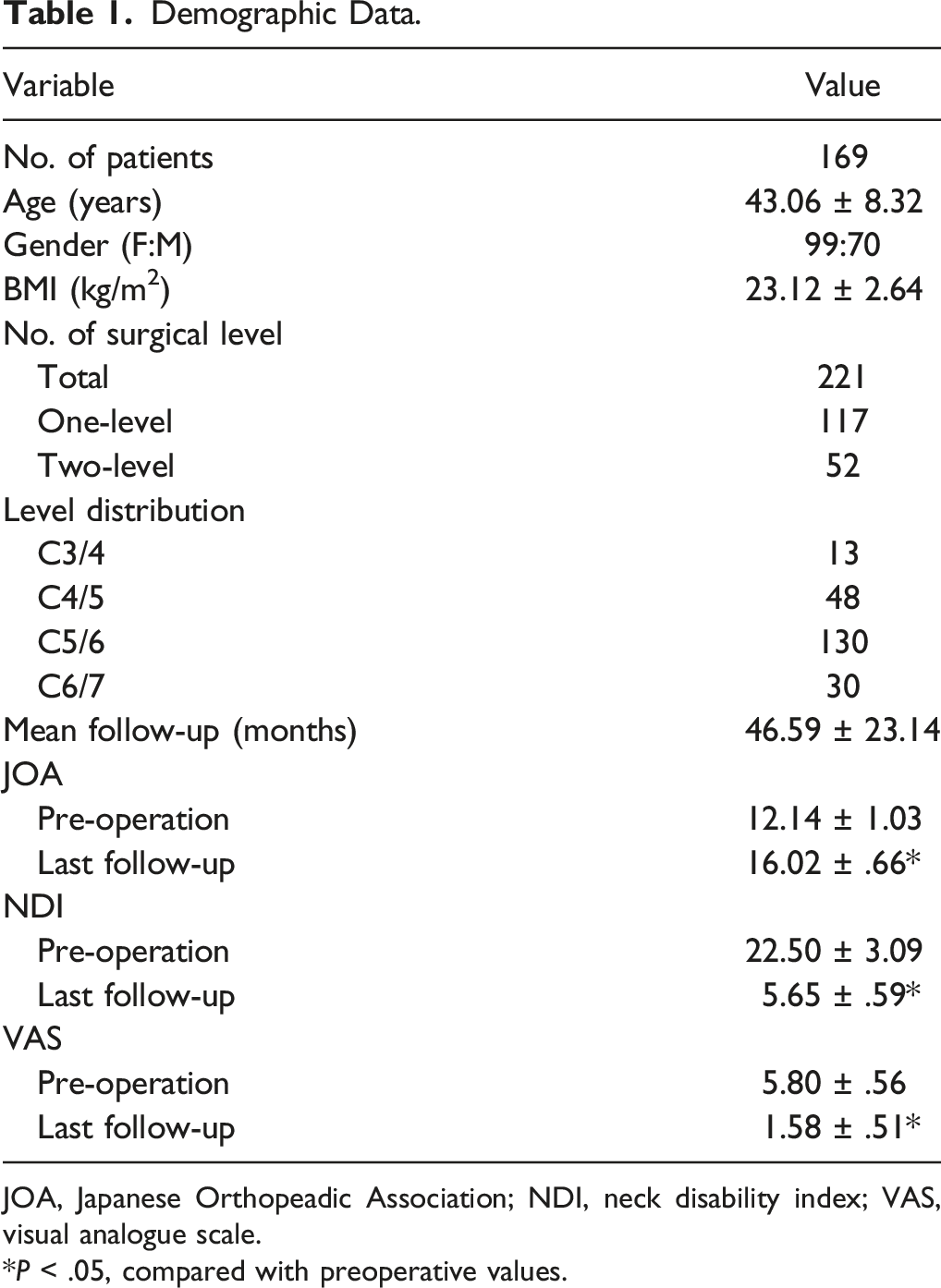
JOA, Japanese Orthopeadic Association; NDI, neck disability index; VAS, visual analogue scale.
*P < .05, compared with preoperative values.
Radiological and Clinical Differences
The pre- and postoperative sagittal alignment parameters in the entire cohort and 1-level and 2-level CDR subgroups are presented in Figure 2. There were no significant differences in the C0-C2 angle, FSU angle, T1 slope, or SVA before and after the operation. The C2-C7 angle showed a significant improvement after surgery in the entire cohort (from 8.48 ± 10.24° to 12.03 ± 9.08°, P < .001) and the 1-level CDR subgroup (from 8.04 ± 10.48° to 12.78 ± 9.12°, P < .001), while there were few differences in the 2-level subgroup. The values of the C2 slope decreased significantly compared to preoperative values in the entire cohort (from 11.98 ± 7.19° to 10.01 ± 6.39°, P < .001) and the 1-level CDR subgroup (from 12.36 ± 6.71° to 9.75 ± 5.71°, P < .001) but did not change significantly in the 2-level subgroup. T1 slope-CL had an analogous trend with C2 slope during follow-up, as the values in the entire group (from 11.13 ± 8.08° to 8.52 ± 7.41°, P < .001) and 1-level subgroup (from 11.38 ± 7.72° to 7.84 ± 7.56°, P < .001) decreased significantly after surgery while showing fewer changes in the 2-level CDR subgroup. Changes of cervical sagittal alignment parameters between pre-operation and last follow-up in the entire cohort, 1-level CDR group, and 2-level CDR group. An asterisk represents a significant difference compared with preoperative values. Abbreviations: FSU, functional spinal unit; CL, cervical lordosis; CGH, center of gravity of the head; SVA, sagittal vertical axis; CDR, cervical disc replacement.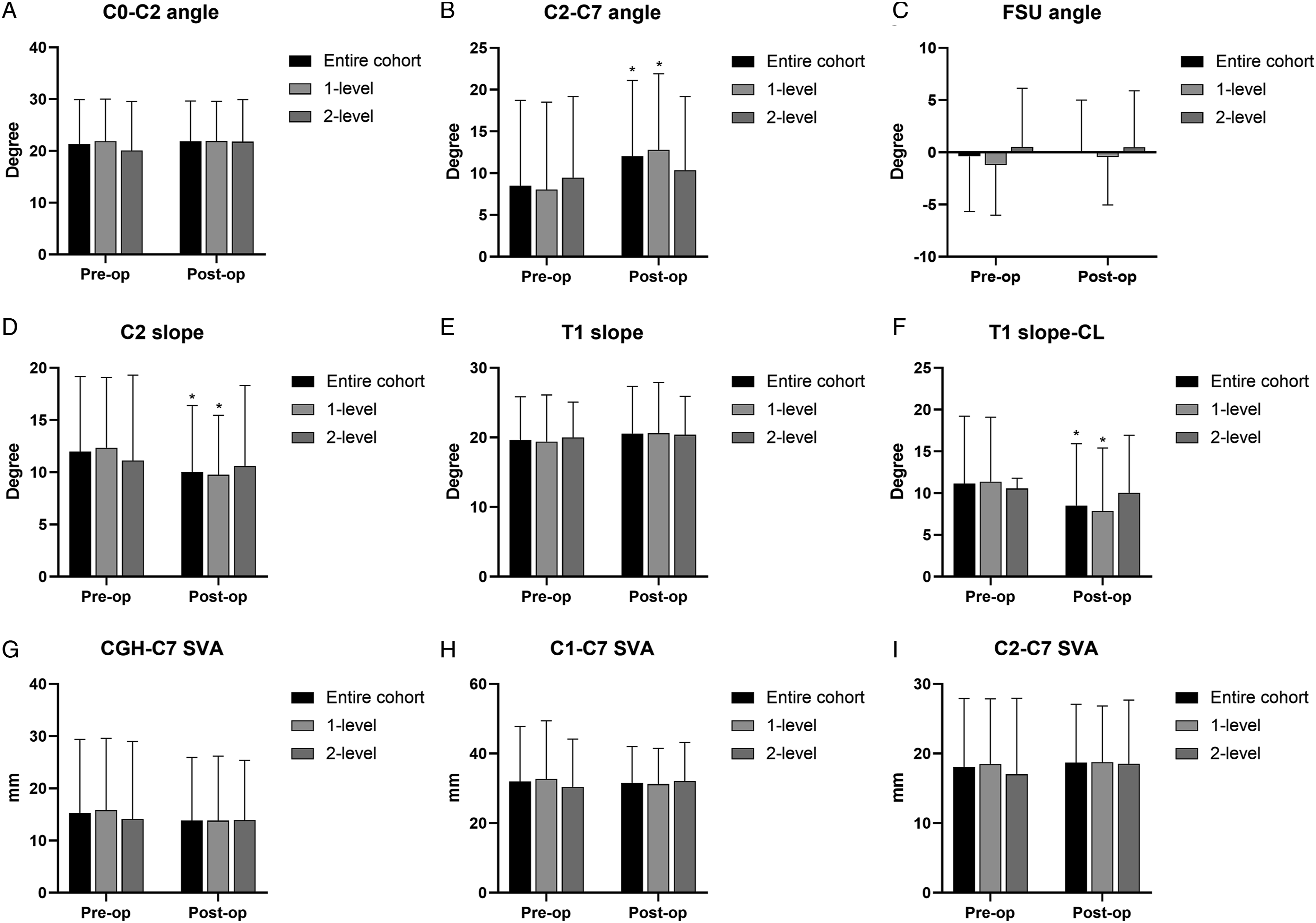
Comparison of Sagittal Parameters Between Less Mobile and More Mobile Levels.
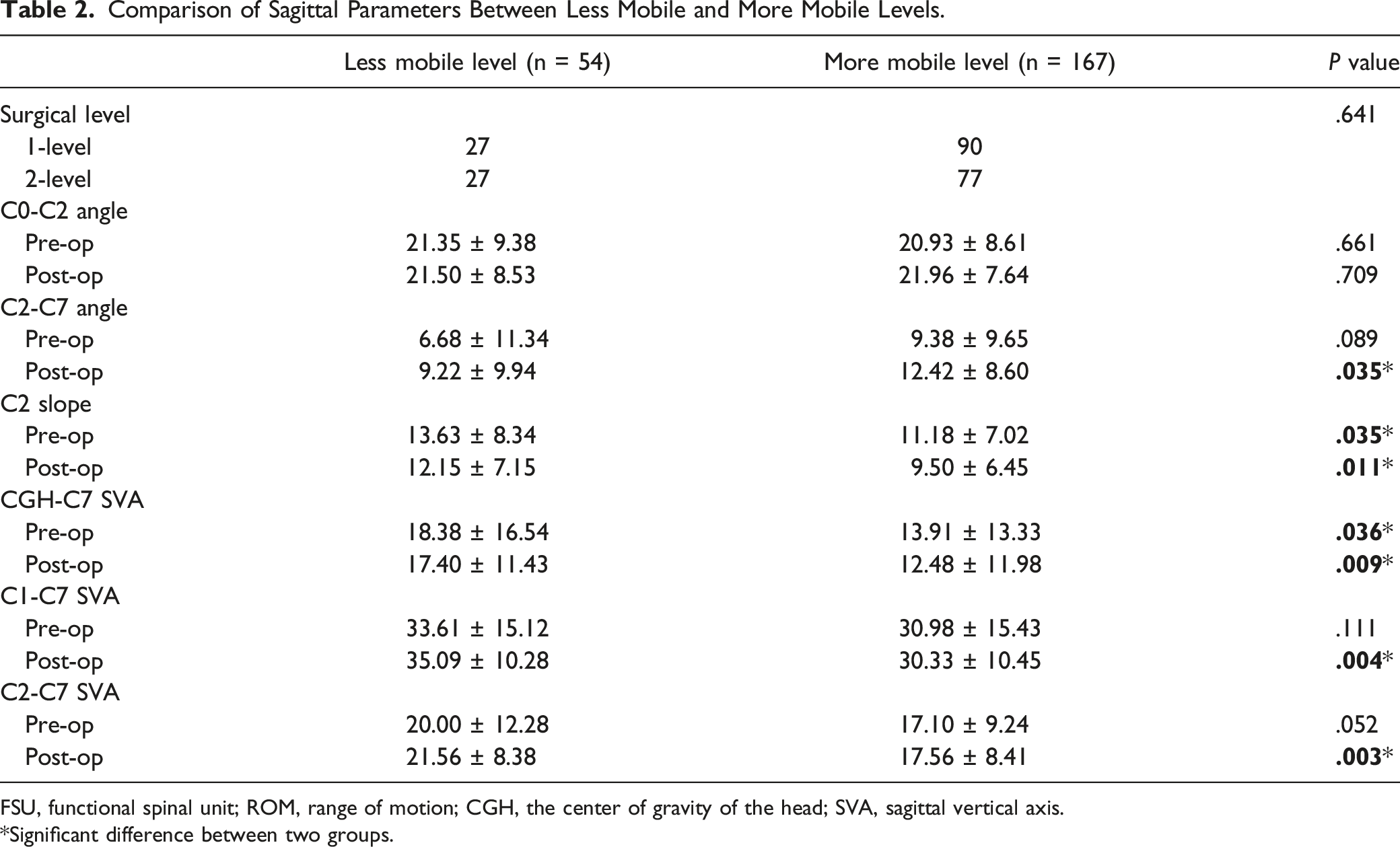
FSU, functional spinal unit; ROM, range of motion; CGH, the center of gravity of the head; SVA, sagittal vertical axis.
*Significant difference between two groups.
Comparison Between the Groups of High and Low C2 slope in 1- and 2-Level Cervical Disc Replacement.
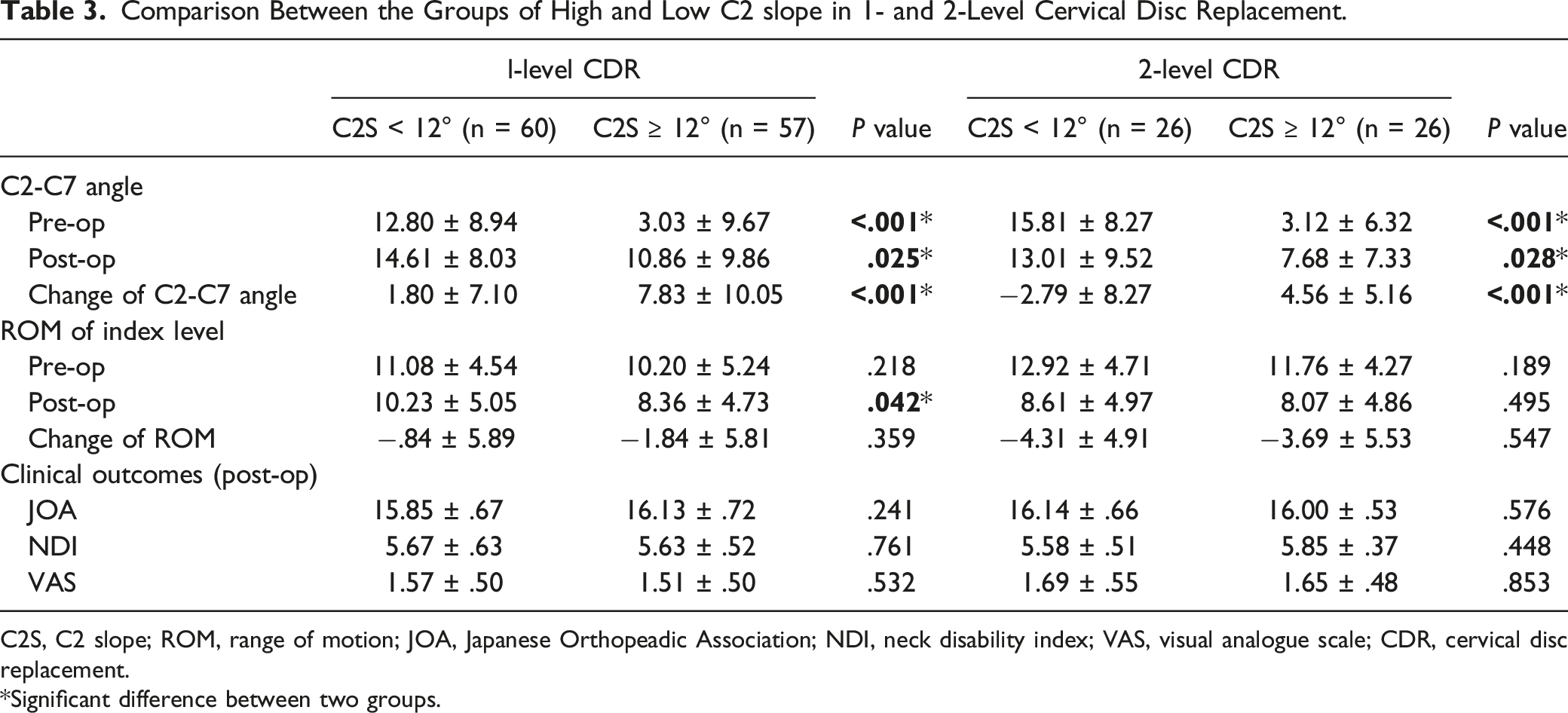
C2S, C2 slope; ROM, range of motion; JOA, Japanese Orthopeadic Association; NDI, neck disability index; VAS, visual analogue scale; CDR, cervical disc replacement.
*Significant difference between two groups.
Comparison Between the Groups of High and Low Center of Gravity of the Head-C7 Sagittal Vertical Axis in 1- and 2-Level Cervical Disc Replacement.
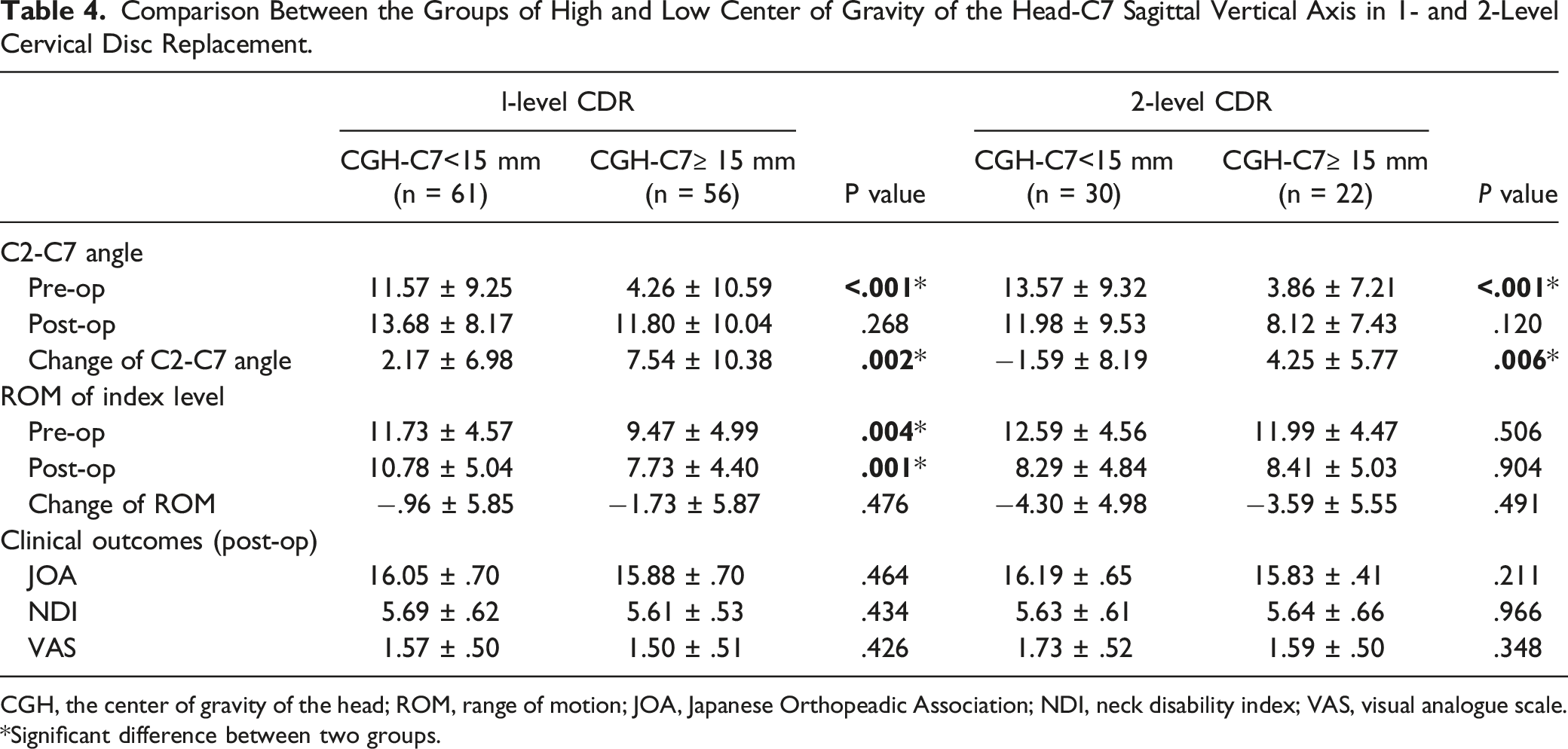
CGH, the center of gravity of the head; ROM, range of motion; JOA, Japanese Orthopeadic Association; NDI, neck disability index; VAS, visual analogue scale.
*Significant difference between two groups.
Relationship Between Sagittal Alignment Parameters and rASP
Cervical Sagittal Parameters With the Presence and Progression of Radiographic Adjacent Segment Pathology.
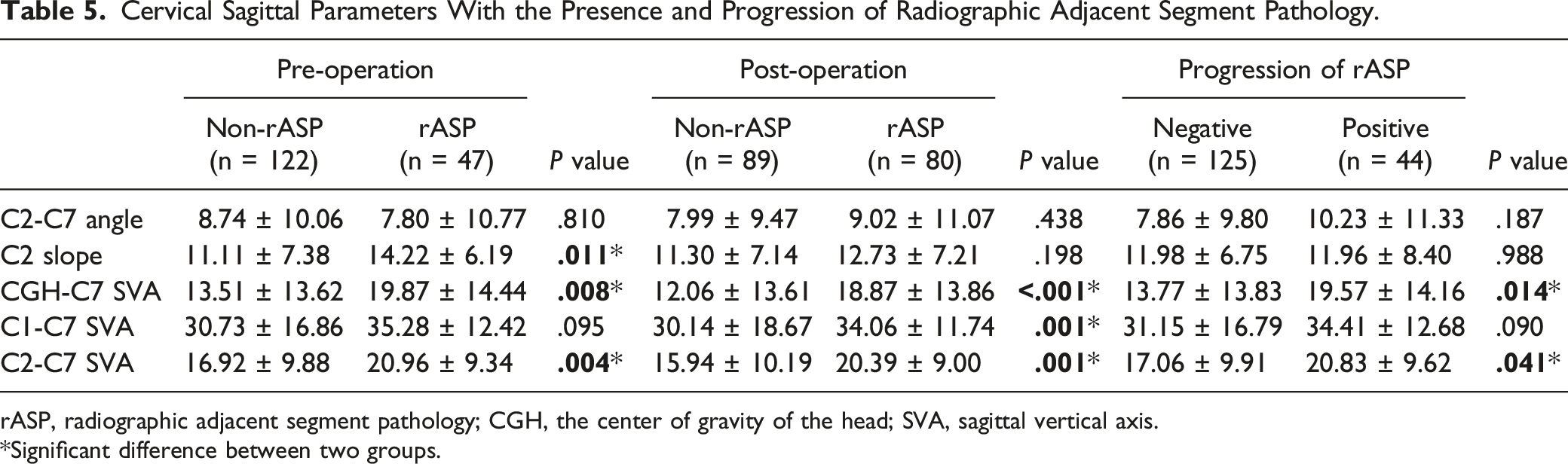
rASP, radiographic adjacent segment pathology; CGH, the center of gravity of the head; SVA, sagittal vertical axis.
*Significant difference between two groups.
Relationship Between Sagittal Alignment Parameters
Correlation Between Sagittal Alignment Parameters.
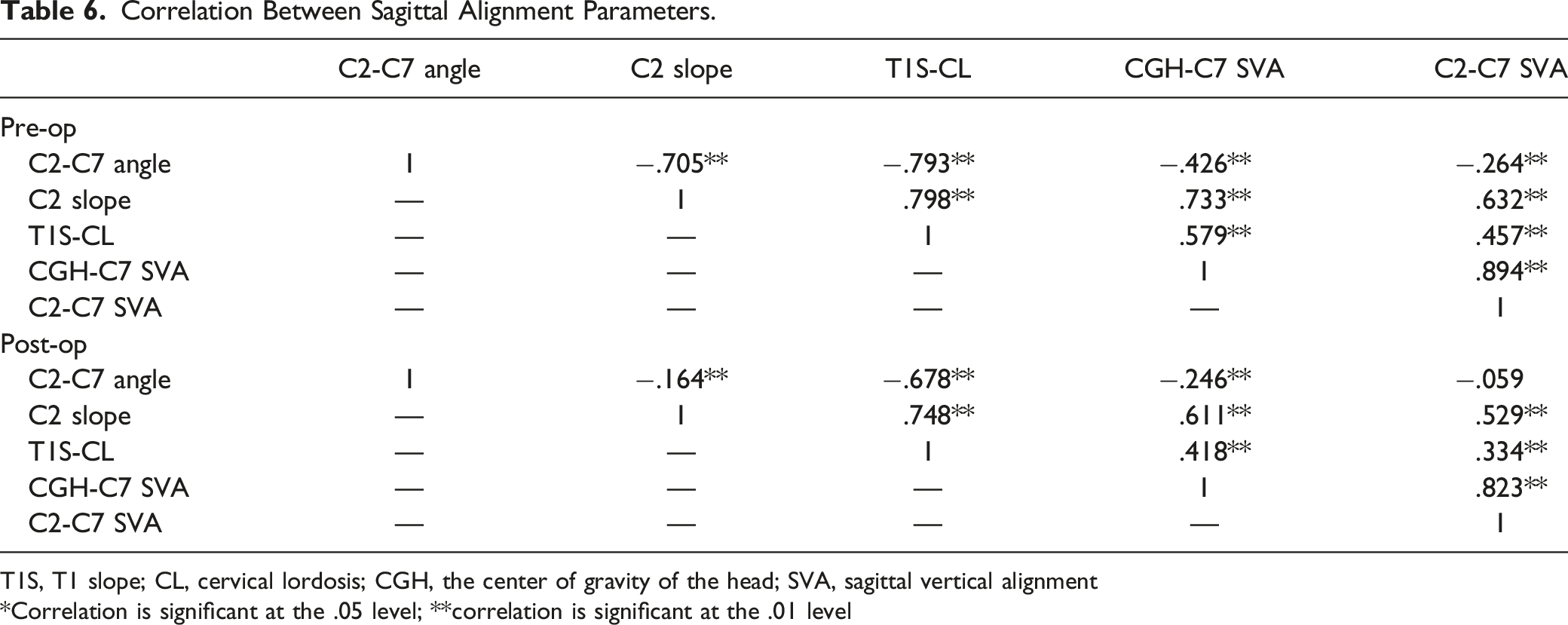
T1S, T1 slope; CL, cervical lordosis; CGH, the center of gravity of the head; SVA, sagittal vertical alignment
*Correlation is significant at the .05 level; **correlation is significant at the .01 level
Discussion
The cervical spine is the most mobile segment of the spinal column with the main responsibility for supporting the weight of the head over the body. 1 Previous studies have demonstrated the relationship between cervical sagittal alignment and cervicothoracic junction parameters in the sagittal plane.20,21 As the superior structure that the cervical spine connects and supports, the balance of the cranial position in the sagittal plane is also associated with cervical sagittal alignment. Lee et al 22 analyzed craniocervical sagittal alignment parameters in 77 asymptomatic adult volunteers and found that cranial offset and cranial tilting were significantly correlated with cervical sagittal curvature. Zhu et al 23 redefined the occipital parameters and explored the correlations among occipitocervical parameters. They found that occipital orientation was a significant factor affecting cervical sagittal alignment. It has been reported that the majority of cervical lordosis is localized at the C1-C2 segments, while the lower cervical spine contributes to relatively little lordosis.24,25 This is probably because the center of gravity of the head lies directly above the C1 and C2 vertebrae, emphasizing the unique role of craniocervical sagittal balance. 4 Therefore, in the present study, we explored the relationship between craniocervical sagittal alignment and the outcomes of CDR. The results suggested that craniocervical sagittal balance was associated with ROMs of arthroplasty levels and cervical lordosis but not with patient-reported outcomes.
The present study found significant lordotic changes in cervical curvature after 1-level CDR, which is concordant with prior reports.26-28 There was an increasing trend in cervical lordosis in patients who underwent 2-level CDR, but the differences did not reach statistical significance, probably because of the limited sample size. The design philosophy of CDR is to preserve segmental mobility. In this study, lower preoperative and postoperative CGH-C7 SVA and C2 slope were observed in the more mobile group. At the last follow-up, the less mobile group had less lordotic sagittal alignment and significantly higher SVA. Previous studies have suggested that patients with a higher T1 slope tended to have higher cervical lordosis, which may contribute to better segmental lordosis and consequently affect ROM.9,12 The T1 slope functions as the abutment of the cervical spine, allowing the cervical spine to play a role in the support of head weight. 29 Thus, the cranial position in the sagittal plane and T1 slope may jointly affect the cervical curvature and should both be evaluated before surgery. In addition, Kuo et al 12 found a clear correlation between the change in ROM and the change in cervical lordosis, which indicated that increased segmental ROM might be related to the improvement in cervical curvature. Our findings suggested that although patients with a higher C2 slope and CGH-C7 SVA had lower ROM and cervical lordosis after surgery, they had a greater chance for improvement in cervical lordosis and may benefit from CDR.
The balance of sagittal alignment is considered an important factor affecting patient-reported outcomes. Xu et al 13 evaluated the relationship between preoperative cervical sagittal balance and outcomes among 181 patients who underwent laminoplasty. They found that a larger preoperative CGH-C7 SVA was significantly associated with postoperative lordotic decreases and poor JOA scores, which indicated the distinctive role of the status of the gravity center of the head in sagittal balance. Wang et al 15 retrospectively analyzed 72 patients after laminoplasty and revealed that patients with a higher spino-cranial angle had worse NDI scores. However, in the current study, there were no differences in the clinical outcomes after CDR between patients with different craniocervical sagittal parameters, which is consistent with previous studies of CDR.9,12,26 Similarly, Evaniew et al 30 found that preoperative increased SVA and T1 slope were associated with poor health-related quality of life in patients with cervical spondylotic myelopathy, while significant associations were not observed after surgery. This discrepancy may be due to the differences in surgical methods as well as the sample size of the study.
C2 slope is a recently proposed sagittal parameter that can briefly measure cervical deformity because of its mathematical approximation to T1 slope-CL, which was considered a quantitative measurement of the mismatch between the degree of cervical lordosis and T1 slope. 31 Due to its close relationship with both the occipitocervical and cervicothoracic spine, the C2 slope can adequately describe the imbalance of upper-cervical and subaxial alignment. 32 However, the C2 slope has rarely been reported in CDR. In this study, we found that the C2 slope was strongly correlated with the T1 slope-CL before and after surgery and had a similar decreasing trend with the T1 slope-CL during follow-up. The correlation analysis also suggested that the C2 slope was positively correlated with the SVA parameters. Patients with a higher C2 slope had lower pre- and postoperative lordosis and lower postoperative ROM but larger lordotic change after CDR. In addition, a higher C2 slope was also found to be associated with the presence of preoperative rASP. Protopsaltis et al 31 retrospectively analyzed 104 patients with cervical deformities and found that a higher postoperative C2 slope was correlated with worse health outcomes. A relationship between C2 slope and clinical outcomes was not observed in the current study; this was most likely due to the overall mild cervical sagittal imbalance in CDR patients. Nonetheless, C2 slope remains a simplified and useful indicator for evaluating the craniocervical sagittal balance and predicting sagittal alignment outcomes after CDR.
The imbalance of craniocervical sagittal alignment may be associated with the presence of degenerative diseases. 33 This study found that higher preoperative CGH-C7 SVA and C2-C7 SVA were related to the presence of pre- and postoperative rASP and positive progression of rASP. The increased SVA could cause an abnormal load transmission pattern and increase the axial load through the adjacent levels. 34 In an in vitro biomechanical study, Patwardhan et el. 35 found that the adjacent segment mechanical burden due to fusion increased when the SVA increased. Yang et al 18 investigated the relationship between cervical sagittal alignment and rASP. They found that the occipito-cervical angle, which is an important factor in maintaining horizontal gaze, was associated with the presence and positive progression of rASP. Thus, craniocervical sagittal imbalance might be an independent risk factor for rASP, and further long-term studies are needed to explore whether such radiographic changes lead to adverse clinical results.
Limitations
There were several limitations to the present study. First, this was a retrospective, single-center study that may have introduced some bias and limited the generalizability of the results. Second, the duration of the follow-up was relatively short in this study, and the rASP and clinical outcomes may be more accurate in the long-term study. Third, only the best-validated sagittal parameters were involved in the analysis. 32 Other craniocervical parameters, such as cervical tilting and cranial tilting, were not investigated in the present study, and their effects need to be researched further. 22 Fourth, there were some differences in sagittal parameters that were significant in 1-level CDR but not in 2-level CDR, which was probably due to the small sample sizes of patients who underwent 2-level CDR. The results should be interpreted with caution. Thus, large-sample, prospective, multicenter studies with long-term follow-up are warranted.
Conclusions
Craniocervical sagittal balance is associated with cervical lordosis and ROM at the index level after CDR. Patients with preoperative sagittal imbalance had less postoperative cervical lordosis and ROM yet could experience more improvement in cervical curvature after surgery. Increased preoperative SVA is an important factor related to rASP. An association between sagittal alignment parameters and clinical outcomes was not found.
Footnotes
Authors’ contributions
Yi-Wei Shen and Yi Yang provided equal contribution to this study and should be considered co-first authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by the Science and Technology Project of the Health Planning Committee of Sichuan Province (21PJ037), the Sichuan Province Science and Technology Support Program (2019YFQ0002), the National Natural Science Foundation of China (81902190), and the Science and Technology Project of the Health Planning Committee of Sichuan Province (21PJ039).